
Abstract
Study Design
Retrospective observation study.
Objectives
Despite pelvic incidence (PI)-lumbar lordosis (LL) overcorrection, some patients exhibit residual pelvic tilt (PT) malalignment, termed pelvic non-responders (PNRs). We aimed to identify risk factors for PNRS after PI-LL overcorrection and its impact on surgical outcomes.
Methods
A retrospective analysis of 181 adult spinal deformity (ASD) patients who underwent fusion of ≥ five levels. PNRs were defined as postoperative PT ≥ 20° despite PI-LL overcorrection. Patient-reported outcomes (PROMs) and mechanical complications, such as proximal junctional failure (PJF), were documented. Logistic regression identified significant risk factors for PNRs.
Results
Among the 181 patients, 30 (16.6%) were classified as having PNRs. Preoperative PI and postoperative PI-LL mismatch were significantly higher in PNRs than in PRs. Multivariate analysis identified higher preoperative PI, postoperative PI-LL ≥ −2°, lordosis distribution index (LDI) < 53%, and increased postoperative thoracic kyphosis as significant risk factors for pelvic non-response. PJF was significantly higher in PNRs (30.0% vs 10.6%, P < 0.01). At 1 year postoperatively, PNRs had lower SRS-22 scores in activity, pain, appearance, and mental health (P < 0.05), but MCID analysis indicated these differences may not be clinically meaningful.
Conclusions
Larger preoperative PI, lower postoperative LDI, and higher postoperative PI-LL are significant risk factors for pelvic non-response in ASD patients with PI-LL overcorrection. PNRs are at increased risk of higher rates of PJF. Surgical strategies should prioritize achieving the target PI-LL and an LDI of ≥53% to optimize alignment and reduce the risk of PNRs and associated mechanical complications.
Keywords
Introduction
Adult spinal deformity (ASD) commonly involves spinopelvic malalignment, resulting in severe pain and functional limitations.1-5 Correcting sagittal malalignment is crucial for successful ASD surgery.6,7 Among the key sagittal parameters, pelvic tilt (PT) is of paramount importance, alongside pelvic incidence (PI)–lumbar lordosis (LL) mismatch, in surgical correction.7-12 Increased PT is closely associated with poor clinical outcomes in ASD patients, regardless of whether they undergo surgery.1,6,13,14 Therefore, achieving appropriate restoration of PT is crucial in ASD surgery.8-11 Despite adequate PI-LL correction or overcorrection, PT undercorrection persists in some patients, termed pelvic non-responders (PNRs). Passias et al found PT undercorrection in 32.6% of ASD patients with matched PI-LL correction and 6.4% with overcorrection.9
PT adjusts passively to LL correction, making PI-LL overcorrection beneficial for preventing PT undercorrection.9,10 However, it may increase the risk of proximal junctional kyphosis (PJK) or proximal junctional failure (PJF).7,9,12,15-17 Although some studies associate PI-LL overcorrection with increased PJK or PJF risk,12,18 others have reported acceptable or even favorable outcomes in patients with PI-LL overcorrection, 19 suggesting that not all overcorrected patients experience complications.
Given the variability in outcomes after PI-LL overcorrection and limited knowledge of PT undercorrection, we hypothesize that PNRs have worse clinical outcomes than pelvic responders (PRs). We also propose that postoperative factors, such as lordosis distribution index (LDI), play a significant role in increasing the risk of pelvic non-response, beyond the amount of PI-LL correction. Existing literature on specific surgical outcomes and risk factors for PT undercorrection in the context of PI-LL overcorrection is limited. Therefore, this study aimed to identify the incidence and risk factors of PT undercorrection in patients with PI-LL overcorrection and compare the radiological outcomes, clinical outcomes, and mechanical complications between PNRs and PRs.
Materials and Methods
This study was approved by our institutional review board, with informed consent waived due to its retrospective design. This study included only patients with PI-LL overcorrection to ensure a amount of correction universally considered sufficient by all experts and to allow postoperative PT to adequately respond to the degree of PI-LL correction.
Study Population
This retrospective case series analyzed consecutive patients from our prospective ASD database who underwent degenerative-type ASD surgery (2011-2023). Inclusion criteria: (1) ASD defined by C7 sagittal vertical axis (SVA) ≥ 50 mm, PI-LL mismatch ≥10°, PT ≥ 25°, or coronal Cobb ≥30°; (2) fusion of ≥ five levels, including sacrum/pelvis; (3) PI-LL overcorrection, defined as achieving an age-adjusted PI-LL target (PI-LL = (age – 55)/2 + 3)20,21 and falling below its lower limit. 21 Exclusion: (1) <1-year follow-up, (2) incomplete radiographic data, (3) congenital hip dysplasia, degenerative hip disease, malignancy, inflammatory diseases, or infections. Pelvic fixation was used in all cases unless L5–S1 had been previously fused during lumbosacral surgery.
Demographic and Operative Data Collection
Demographic data, such as sex, age, body mass index (BMI), bone mineral density, osteoporosis status, and follow-up duration, were collected. Operative data, including fusion techniques, osteotomies, and pelvic fixation methods, augmentation in the upper instrumented vertebra were collected.
Radiographic Data Collection
Preoperative and 6-week postoperative measurements included PI, LL, PI-LL, sacral slope (SS), PT, thoracic kyphosis (TK), T1-pelvic angle (TPA), and SVA. Postoperative lower lumbar lordosis (LLL) was measured from L4 to S1, and LDI was calculated as LLL/LL × 100. Postoperative sagittal alignment, was assessed using the global alignment and proportionality (GAP) and sagittal age-adjusted scores (SAAS).22,23 If PJK developed within 6 weeks postoperatively, immediate postoperative radiographs were obtained.
Definition of PNRs and PRs
Postoperative PT was assessed using SRS-Schwab classification: zero (<20°), + (20°–30°), and ++ (>30°). 24 Patients with PI-LL overcorrection and PT ≥ 20° (+/++) were classified as PNRs, while others were PRs.
Mechanical Complications
Mechanical complications included PJK (Proximal junctional angle >20°)25,26 and PJF (requiring revision for proximal junctional complications). Rod fractures were assessed at or above L5-S1, excluding those between the S1 pedicle and iliac screws. 27 The date of mechanical failure was recorded.
Patient-Reported Outcome Measures (PROMs) Data Collection
PROMs were evaluated using the visual analog scale for back and leg pain, Oswestry Disability Index (ODI), and Scoliosis Research Society-22 (SRS-22) questionnaire. The SRS-22 assessed activity, pain, appearance, mental health, and satisfaction. PROMs were collected preoperatively, at 1 year postoperatively, and at the final follow-up, with changes analyzed over time. We assessed the proportion of patients achieving the minimal clinically important difference (MCID) for VAS, ODI, and SRS-22 in PROMs with significant group differences. The MCID thresholds were 1.2 (VAS), 12.8 (ODI), and for SRS-22: 1.05 (activity, appearance, subtotal), 0.85 (pain), and 0.70 (mental health). 28
Statistical Analysis
Categorical variables were presented as frequencies (%) and compared using the chi-square test. Continuous variables were expressed as means ± SD and analyzed with the t test or Kruskal–Wallis test. Kaplan-Meier analysis with log-rank tests evaluated PJK/PJF incidence. Receiver operating characteristic (ROC) curve analysis was used to determine cutoff values for surgically modifiable associated factors, such as PI-LL and LDI, in relation to PT undercorrection. Logistic regression identified risk factors for PT undercorrection, with multicollinearity assessed using correlation coefficients (r < 0.80) and variance inflation factors <10. Variables with P < 0.20 in univariable analysis entered the multivariable model, followed by backward stepwise elimination. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Analyses were performed in SPSS (v27.0, IBM), with significance set at P < 0.05.
Results
This study included 181 patients (mean age: 71.8 years, 84% women). Mean BMI was 25.9 kg/m2, and T-score was −1.4. Most surgeries used a front-back approach, with pedicle subtraction osteotomy in 5.5%. Prior spine surgery was noted in 31.5% (57 cases). Mean fused levels were 6.6, with pelvic fixation in 82.3% (149 cases). Mean follow-up was 38.9 months. The mean preoperative PI-LL and PT values were 25.4° and 29.9°, respectively. Among the patients, 30 were PNRs and 151 were PRs.
Baseline Data of Included Patients and Comparison of Baseline Data Between Pelvic Responder (PR) and Pelvic Non-responder (PNR).
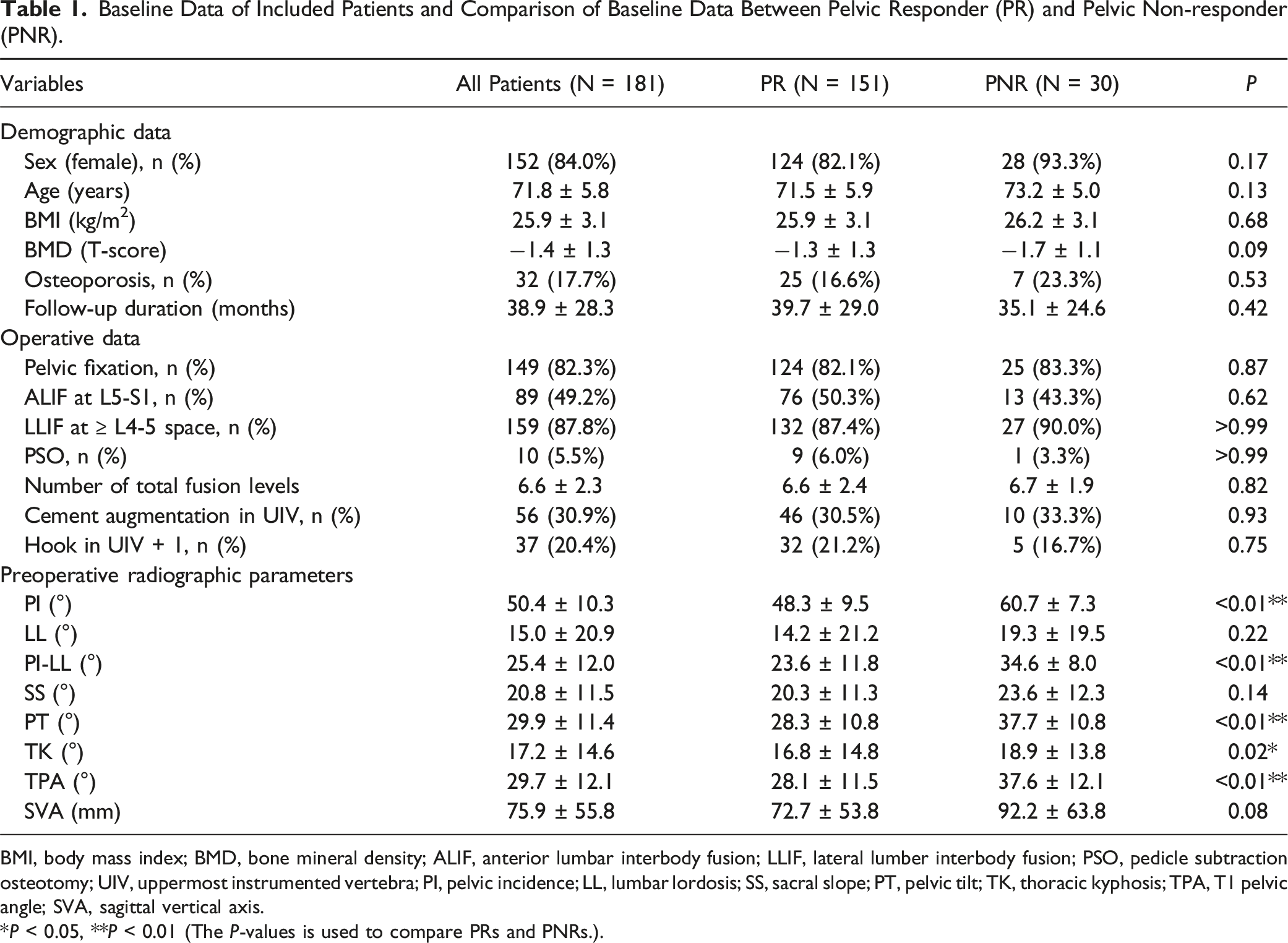
BMI, body mass index; BMD, bone mineral density; ALIF, anterior lumbar interbody fusion; LLIF, lateral lumber interbody fusion; PSO, pedicle subtraction osteotomy; UIV, uppermost instrumented vertebra; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis.
*P < 0.05, **P < 0.01 (The P-values is used to compare PRs and PNRs.).
Comparison of Postoperative Radiographic Parameters and Their Changes Between Pelvic Non-responder (PNR) and Pelvic Responder (PR).
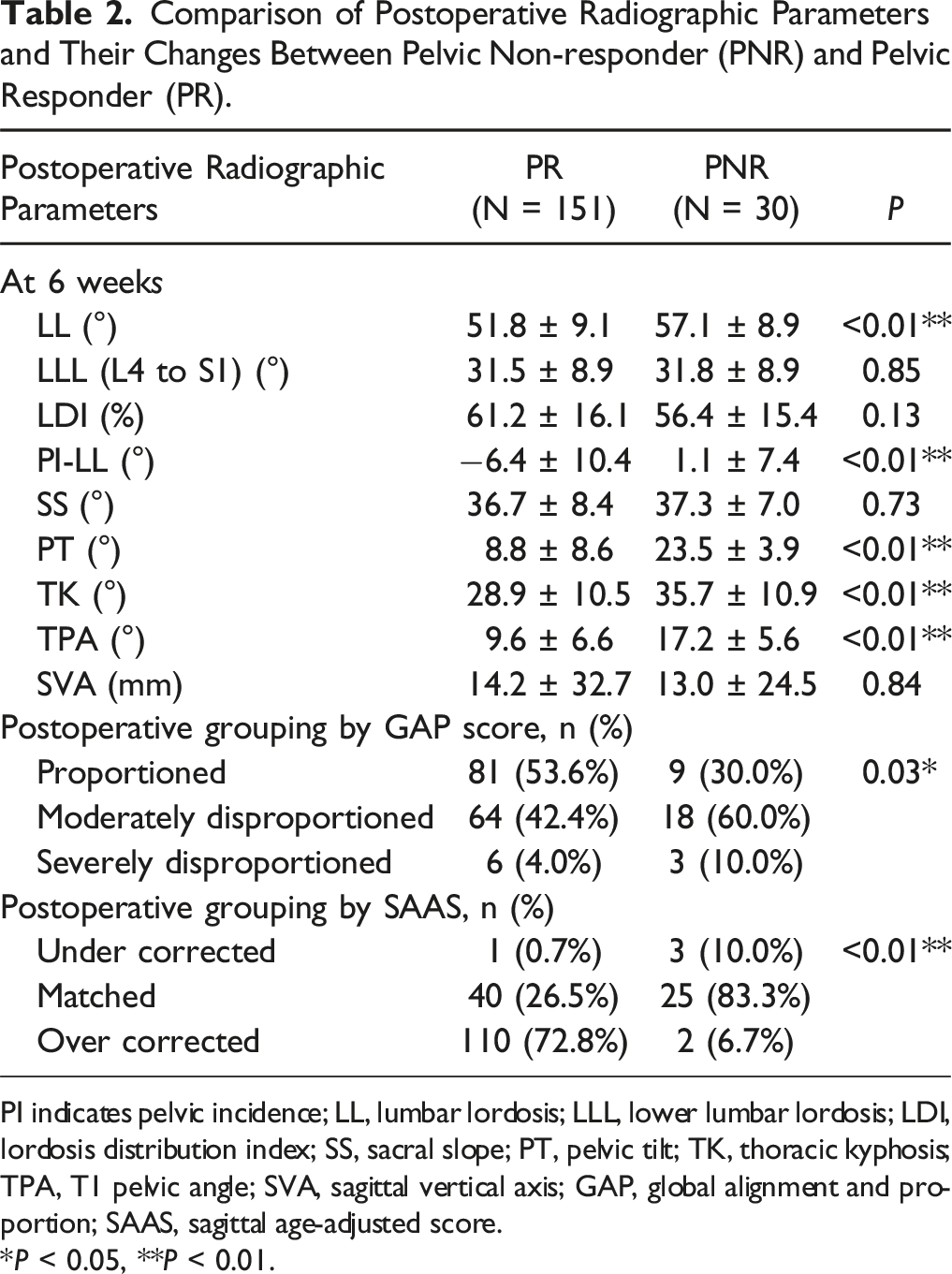
PI indicates pelvic incidence; LL, lumbar lordosis; LLL, lower lumbar lordosis; LDI, lordosis distribution index; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis; GAP, global alignment and proportion; SAAS, sagittal age-adjusted score.
*P < 0.05, **P < 0.01.
In the ROC curve analysis for determining the cutoff values of surgically modifiable factors, PI-LL demonstrated an AUC of 0.77 (95% CI: 0.69-0.86) with a cutoff value of −2° (P < 0.01) (Figure 1a), and LDI had an AUC of 0.59 (95% CI: 0.48-0.70) with a cutoff value of 53% (P < 0.01) (Figure 1b). Receiver operating characteristic (ROC) curves showing the calculated cutoff values for (a) pelvic incidence-lumbar lordosis (PI-LL) and (b) lordosis distribution index (LDI) in predicting pelvic non-responders. AUC, area under the curve; Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value.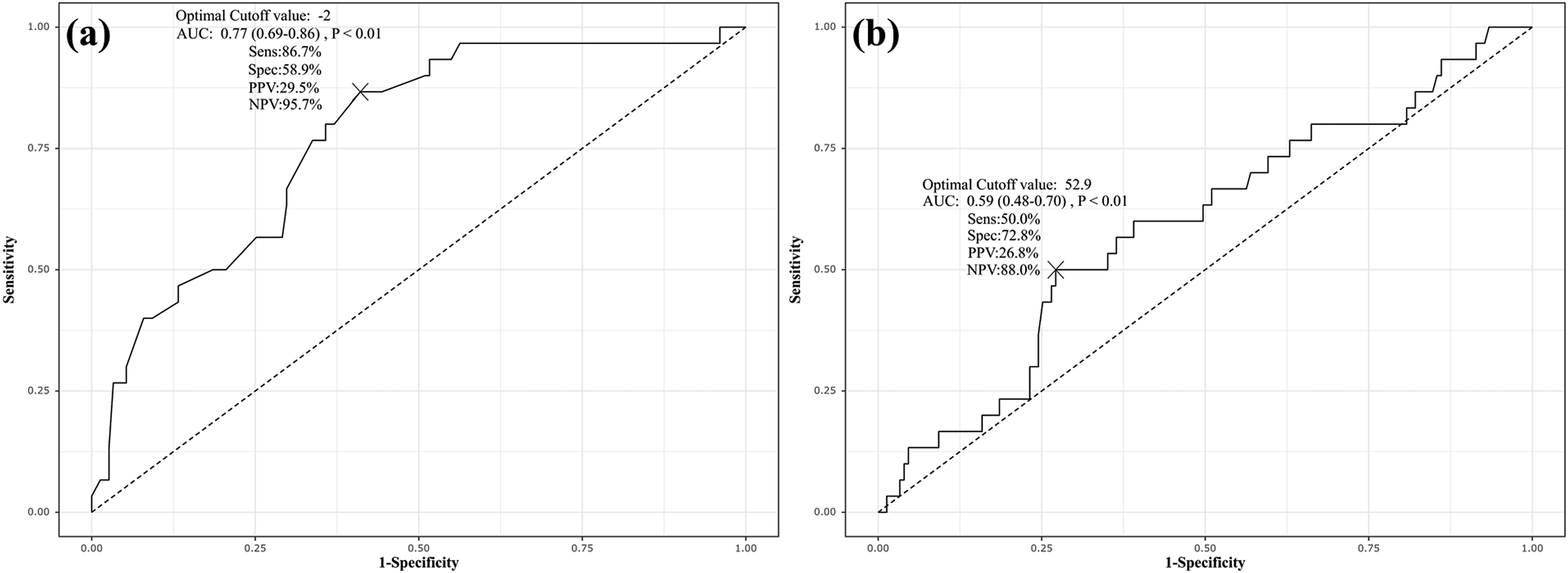
Univariate and Multivariate Logistic Regression Analyses for Postoperative Pelvic Non-response in Patients With Postoperative PI-LL Overcorrection.
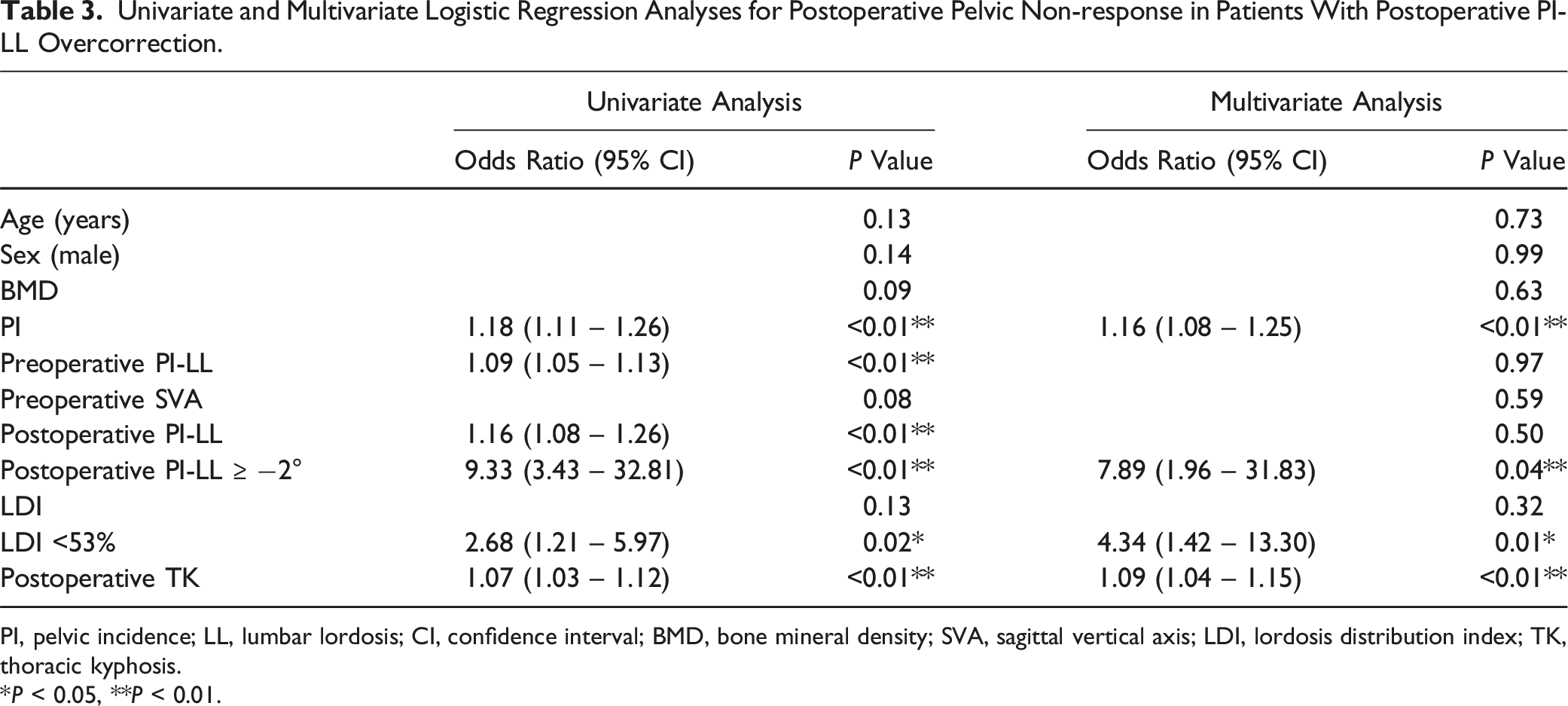
PI, pelvic incidence; LL, lumbar lordosis; CI, confidence interval; BMD, bone mineral density; SVA, sagittal vertical axis; LDI, lordosis distribution index; TK, thoracic kyphosis.
*P < 0.05, **P < 0.01.
Comparison of the Mechanical Failures Between Pelvic Responder (PR) and Pelvic Non-responder (PNR).
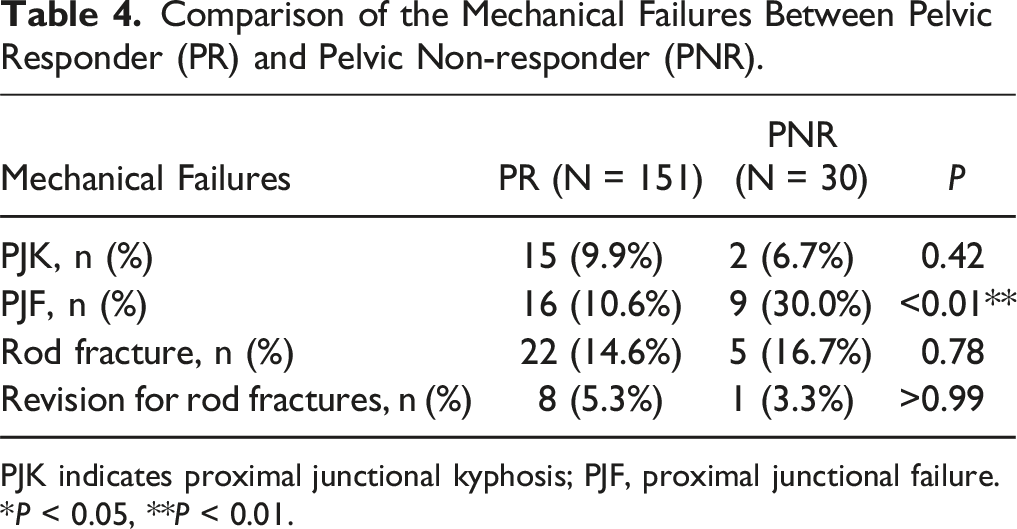
PJK indicates proximal junctional kyphosis; PJF, proximal junctional failure.
*P < 0.05, **P < 0.01.
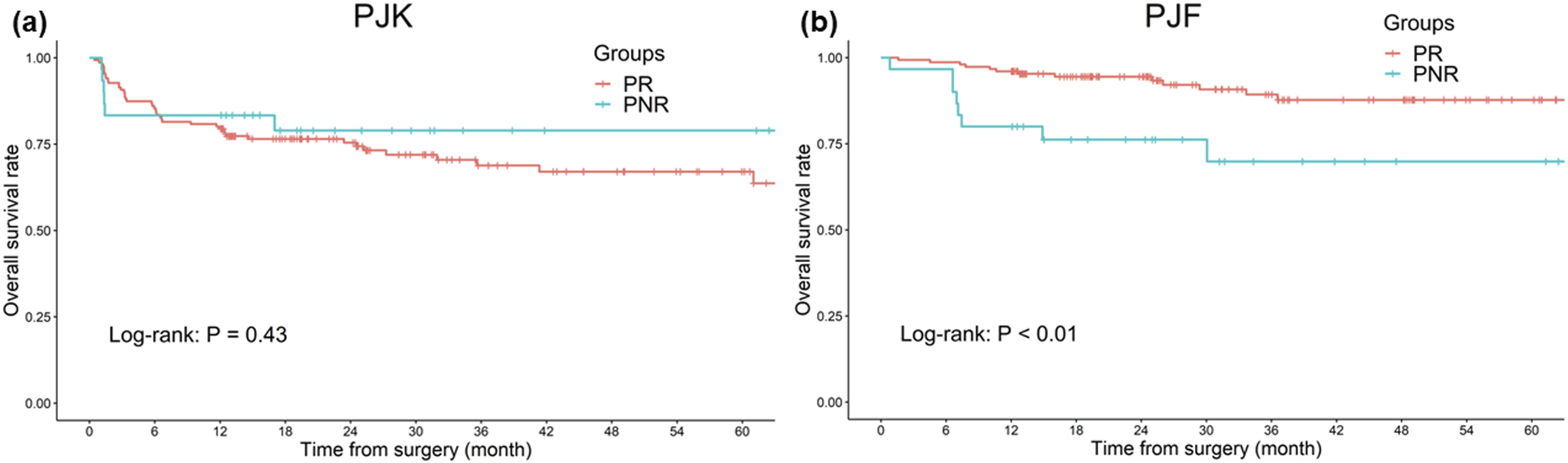
Kaplan–Meier curve for (a) proximal junctional kyphosis (PJK) and (b) proximal junctional failure (PJF) in pelvic non-responders (PNRs) and pelvic responders (PRs).
Comparison of PROMs and Their Changes at Preoperative, One-Year Postoperative, and Final Follow-up Between Pelvic Responder (PR) and Pelvic Non-responder (PNR).
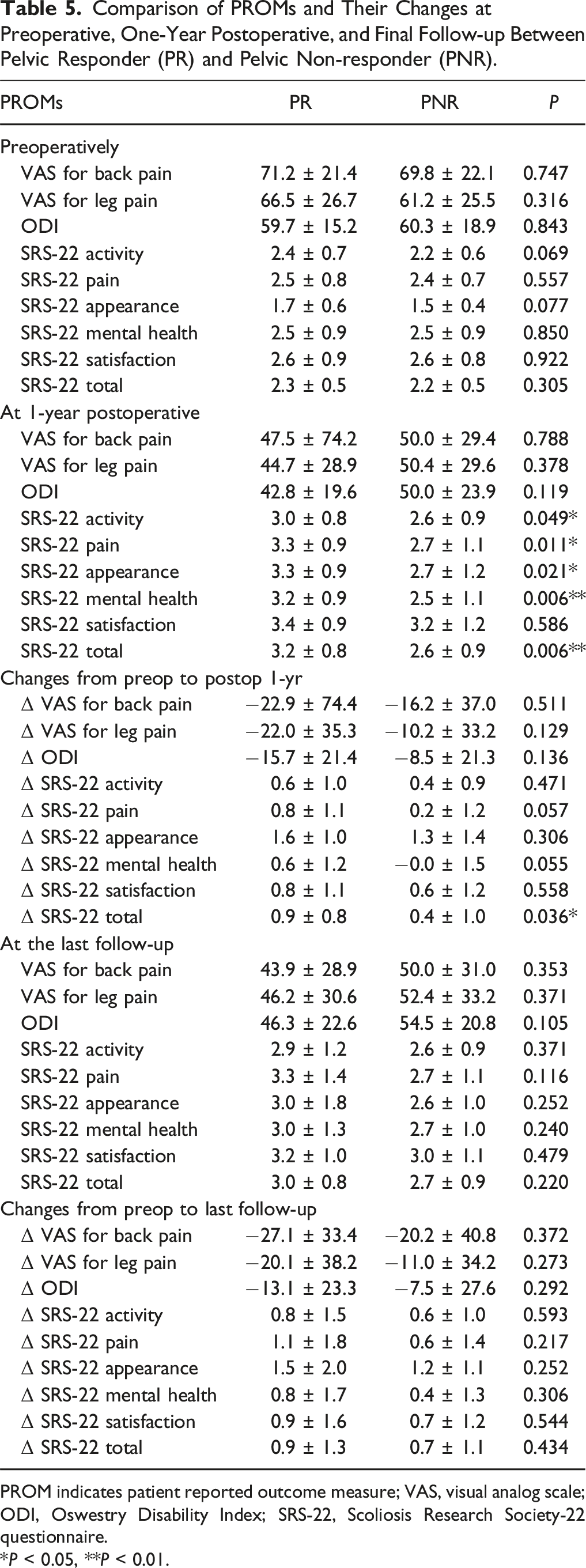
PROM indicates patient reported outcome measure; VAS, visual analog scale; ODI, Oswestry Disability Index; SRS-22, Scoliosis Research Society-22 questionnaire.
*P < 0.05, **P < 0.01.
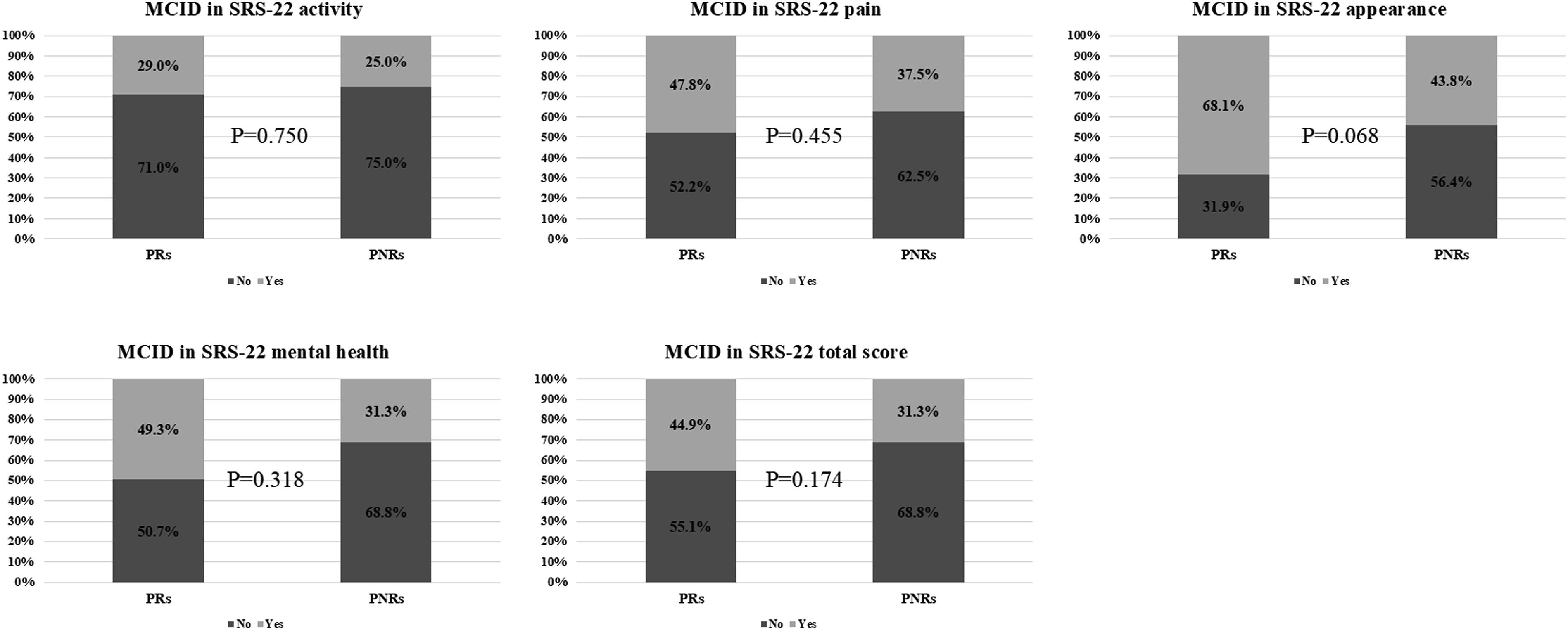
The proportion of pelvic non-responders (PNRs) and pelvic responders (PRs) achieving minimal clinically important difference (MCID) thresholds for SRS-22 at 1 year postoperatively.
Discussion
Our findings highlight that despite PI-LL overcorrection, pelvic non-response was observed in a substantial proportion of patients, mainly because of a larger PI and lower LDI. Specifically, our findings indicated that higher preoperative PI, postoperative PI-LL ≥ −2°, LDI <53%, and increased postoperative TK were independently associated with PT undercorrection. These PNRs had a greater risk of PJF.
Definition of PNRs
Our study defines PNRs using a postoperative PT threshold of ≥20°. While some studies suggest PT normalization based on PI-adjusted equations, prior research has demonstrated that PT >20° is independently associated with higher ODI scores, regardless of PI. 1 Moreover, our findings demonstrate that PNRs had a significantly higher incidence of PJF compared to PRs, further validating the clinical relevance of the PT >20° threshold. The strong association between PNR status and increased mechanical complications underscores the importance of addressing residual PT postoperatively. Furthermore, our multivariate regression analysis identified high PI, lower LDI, and increased thoracic kyphosis as independent risk factors for pelvic non-response, reinforcing the validity of our PT-based definition. Notably, these findings indicate that pelvic non-response is influenced by multiple factors beyond PI alone. The presence of additional independent risk factors suggests that PT >20° is not an arbitrary threshold but rather a clinically meaningful marker of suboptimal spinopelvic alignment and functional impairment. Additionally, considering that the cohort included in our study consists exclusively of patients with PI-LL overcorrection, PT >20° alone can serves as an appropriate threshold for distinguishing between PRs and PNRs. The overcorrection itself ensures that any residual PT represents a clinically meaningful deviation rather than a result of inadequate correction.
Radiographic Characteristics of PNRs
PNRs had higher PI values and more severe preoperative deformity, indicated by greater PI-LL mismatch and SVA (Table 1). Despite greater LL correction, PNRs exhibited higher postoperative PI-LL than PRs, suggesting difficulty in fully correcting their deformity (Table 2). Interestingly, Postoperative SVA did not differ significantly, implying adequate global alignment; however, PT remained undercorrected. This may explain why larger postoperative TK emerged as a significant risk factor, as PT undercorrection and substantial LL correction can cause a posterior SVA shift and compensatory TK increase.
Impact of Postoperative PI-LL
Our finding that postoperative PI-LL ≥ −2° strongly predicts PNR status corroborated the findings of previous studies demonstrating a close relationship between PT and the extent of LL or PI-LL correction. Passias et al reported that postoperative PI-LL values were higher in PNRs than in those with adequate PT correction (17° vs 3°) in patients with severe ASD. 29 They concluded that a more aggressive correction exceeding the ideal age-adjusted PI-LL target is required to minimize PT undercorrection. Dave et al similarly found PT normalization was more common with PI-LL overcorrection. 10 Therefore, a greater degree of LL correction is directly associated with improved PT normalization. However, these two studies did not report the PI of PNRs and PRs, overlooking the possibility of a difference in the PI between PNRs and PRs. Kim et al analyzed the relationship between PT changes and both upper and lower LL corrections. Their regression analysis revealed that the postoperative PT change was influenced by corrections in both the upper and lower LL, with coefficients of −0.250 and −0.238, respectively (all P < 0.05). 30 They found that a 10° increase in lordosis from L4-S1 led to a 2.4° PT correction, whereas a 10° increase from L1-L4 resulted in a 1.6° PT correction. These findings highlight that PT correction is influenced by the sum of the total LL, including the contributions of both the upper and lower LL.
Role of Preoperative PI and LDI in PNRs
Patients with larger PI are more likely to be PNRs, as PT remains undercorrected despite adequate or overcorrected PI-LL. Kim’s study identified preoperative PI as a strong predictor of PT change (standardized coefficient: 0.289, P < 0.01).28 In their analysis, patients with a low PI showed a stronger association between preoperative PT and postoperative PT response, as a larger portion of the PI was already used to compensate for sagittal imbalance, resulting in more significant PT changes after lumbar lordosis correction. In contrast, patients with a high PI have more compensatory reserves, leading to less dramatic PT correction. Our multivariate analysis identified LDI <53% as a significant predictor of PNRs. This result aligns with Pesenti’s finding that a normal LDI of 54% was observed in asymptomatic adults with high PI, matching our LDI cutoff. 31 Furthermore, Kim et al emphasized lower lumbar LL (L4-S1) as crucial for pelvic compensation, observing greater PT correction per 10° lordosis in L4-S1 (2.4°) vs L1-L4 (1.6°).28 They also found stronger correlations between segmental lordosis (L4-S1) and PT changes in the high PI group (r = −0.42) than in the low PI group (r = −0.31).28 In their study, although LDI was not directly analyzed, the predicted postoperative LDI based on mean PI and LLL values was 56% and 74.5% in the high and low PI groups, respectively. Given the limited LL correction possible per level, the LDI is likely to vary with PI. For patients with a low PI, reaching the target PI-LL typically involves maximizing LLL, which reduces the reliance on upper LL and tends to yield a higher LDI. In contrast, patients with a high PI often require additional upper LL correction, even after optimizing LLL, resulting in a lower LDI owing to the need for greater involvement of the upper lumbar segments. Therefore, in patients with a high PI, balancing the PI-LL correction while maintaining an LDI of at least 53% may be challenging but crucial.
Mechanical Complications, PROMs, and Clinical Implications
PNRs had significantly higher PJF rates than PRs (30.0% vs 10.6%) (Table 4). These findings align with prior studies linking inadequate pelvic compensation to increased mechanical stress at the proximal junction.9,13 Passias et al found that normalizing pelvic compensation reduced PJF risk (OR [95% CI]: 0.6 [0.3-1.0]; P = 0.04).13 Persistent PT undercorrection despite LL correction may cause posterior SVA shift and compensatory TK increase, elevating proximal junctional stress. Regarding PROMs, PNRs showed significantly worse SRS-22 scores at 1 year postoperatively and consistently demonstrated inferior trends across multiple PROMs, including VAS and ODI (Table 5). Although these differences did not consistently exceed MCID thresholds, the overall pattern suggests that pelvic non-response may be associated with unfavorable clinical outcomes, possibly due to the higher incidence of PJF. These findings imply that not all overcorrected patients are at high PJK risk, and that PRs with favorable PI or LDI may achieve more favorable outcomes. A larger sample may clarify these trends, and further studies are warranted to validate these observations.
Surgical Planning and Patient Stratification
In practice, stratifying patients based on both PI and LDI can lead to more targeted and effective interventions, ultimately optimizing alignment and minimizing the risk of mechanical complications, such as PJK. Specifically, in patients with high PI, focusing on both PI-LL and LDI to achieve the target PI-LL and maintain an LDI of at least 53% is crucial to prevent PNRs. To achieve an LDI of ≥53%, surgeons should aim to maximize segmental lordosis at L4-5 and L5-S1, typically using anterior techniques such as OLIF. When this alone is not sufficient, surgeons may consider ACR or posterior osteotomies to further increase lower lumbar lordosis and optimize distribution.
Limitations
Our study had certain limitations. First, this was a retrospective analysis conducted at a single institution despite using a consecutively selected cohort from a prospectively collected database. This may limit the generalizability of our findings to other populations, health care settings, or surgical techniques that differ from those used in our institution. Second, the study primarily involved patients with the uppermost instrumented vertebra in the lower thoracic spine, which may restrict the generalizability of the findings to cases in which the fusion extends to the upper thoracic spine. Lastly, PT >20° is not a universally accepted threshold for pelvic non-response, but prior studies have shown its independent association with high ODI scores, regardless of PI. 1 Given that our cohort exclusively included PI-LL overcorrected patients, PT >20° can effectively differentiate PRs from PNRs, as residual PT reflects a clinically meaningful deviation rather than undercorrection. Therefore, our study’s conclusions can remain valid under the PT >20° criterion. However, we acknowledge that this fixed threshold may not fully reflect the spectrum of pelvic malalignment across diverse patients. To improve clinical applicability, future studies should investigate alternative thresholds or models for defining PT normalization, potentially incorporating PI-adjusted targets. Large-scale, multicenter prospective trials are also warranted to validate LDI and PI-LL mismatch as predictors of pelvic non-response.
Conclusion
Patients with higher preoperative PI, postoperative PI-LL ≥ −2°, and LDI <53% are more likely to be PNRs despite sufficient LL correction, leading to higher rates of PJF. We propose that, especially in patients with high PI, achieving optimal outcomes requires not only reaching the target PI-LL but also ensuring that at least 53% of LL is concentrated in the lower lumbar segments. Incorporating LDI into surgical planning may reduce the risk of pelvic non-response and associated mechanical complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets used and analyzed in this study are available from the corresponding author upon reasonable request, in accordance with institutional and ethical regulations.