
Abstract
Study Design
Case-based survey.
Objectives
This study aims to investigate what a group of surgeons learned from their own revisions, and what they would do differently today.
Methods
A multi-center database of ASD surgical patients was queried to identify those with at least 2 surgical procedures performed by the same surgeon between 2009 and 2019. A clinical vignette was created for each case including demographics, a timeline of events, radiographs/measurements, patient-reported outcomes, complications, and surgical strategies used for the index and revision surgeries. The operative surgeon was then asked to fill out a five-question survey aimed at determining factors that contribute to operative decision-making and planning.
Results
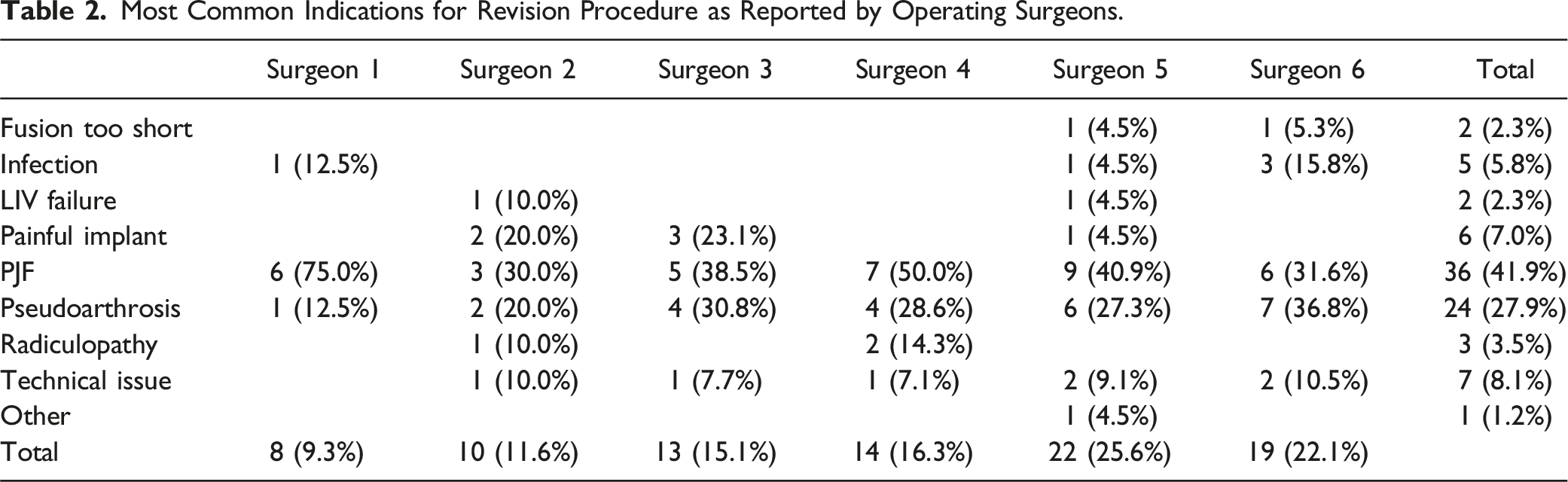
86 patients were operated on by 6 participating surgeons for both index and revision ASD surgery. The revised patients had similar follow-up compared to the non-revised group (P = 0.73), with the most common complications indicating a need for revision surgery being proximal junctional failure (42%) and pseudoarthrosis (28%). Surgeons reported that they would not change their surgical strategy in 52.3% of the cases. The leading cause for revision was hardware/instrumentation issues (24.4%). Learning points included rod-related choice (23.3%), level selection (19.8), PJF prophylactic strategy (15.1%), and sagittal alignment objective (11.6%).
Conclusions
Surgeons saw opportunity in nearly half of the cases to improve outcomes by changing something in the original surgery. While 40% of the failures remained unexplained from the surgeons’ perspective, this study highlights the capacity for adopting changes in adult spinal deformity surgery and illuminates the reasoning behind certain surgical decisions.
Introduction
Adult spinal deformity (ASD) is a spectrum of local, regional, and global three-dimensional abnormalities in the thoracic and lumbar spine that can result from degenerative changes, idiopathic scoliosis, trauma, or iatrogenic causes such as flatback syndrome.1–4 ASD can exist across multiple age groups, however, it is closely linked with increased age and has a prevalence as high as 68% in subjects older than 60 years of age as determined by imaging studies, with a large proportion of those patients never seeking treatment.4,5 Surgical treatment strategies for ASD vary based on the extent of deformity and are associated with substantial clinical benefit with regards to pain and disability in all health-related quality of life measures (HRQoL) compared with patients undergoing nonoperative treatment.6,7 Despite these significant clinical benefits, ASD surgery is associated with high complication rates and rates of revision surgery at approximately 20% within 2 years.8–10
According to the literature, revision surgery following adult spinal deformity surgery is often due to complications such as proximal junction failure, pseudoarthrosis, implant breakage, malalignment, and infection. With the recent expansion of ASD literature - 279 publications before 2015 compared to 1757 publications before 2022 (as per PubMed results for “Adult Spinal Deformity”) - and the use of a multidisciplinary team approach, there have been significant advancements in the treatment of these patients. The recent focus on optimizing preoperative modifiable risk factors has been shown to reduce postoperative complications and improve ASD surgery outcomes. 11 Additionally, reliable preoperative planning strategies, including patient-specific alignment targets and precise level selection, have been associated with fewer functional complications and better outcomes following ASD surgery. 12 However, there is still a discrepancy between research and clinical practice, possibly due to factors such as resistance to change, limited access to educational resources, the challenge of establishing new techniques, and the capacity and motivation for change. 13
Tactics for productive conversations around changes rely on reception to constructive feedback, which is more readily accepted by surgeons in the setting of a discussion concerning problems encountered during surgery, while holding a follow-up discussion of specific errors is a necessary exercise that may be interpreted in a more threatening manner.14,15 Moreover, studies have shown that people tend to exaggerate the subjective magnitude of their personal contributions when those actions are being observed, 16 which may be insightful when surgeons are asked to comment on their own performance during an initially unsuccessful procedure. There has been research in general and colorectal surgery showing that surgeon self-review protocols led to constructive discussion, practice improvement, and a potential for large cost savings.17,18 This process of self-review is important to discerning perception vs reality, with a prior investigation among gynecologic surgeons revealing an association between individuals that underestimated their own complication rate actually having a higher true complication rate as compared to their peers. 19 To better understand the relationship between new practice guidelines, clinical outcomes, and surgeon feedback, a survey was generated to evaluate possible opportunities in the primary surgical treatment of ASD after surgeons were asked to analyze their own operations that required subsequent revision procedures.
Methods
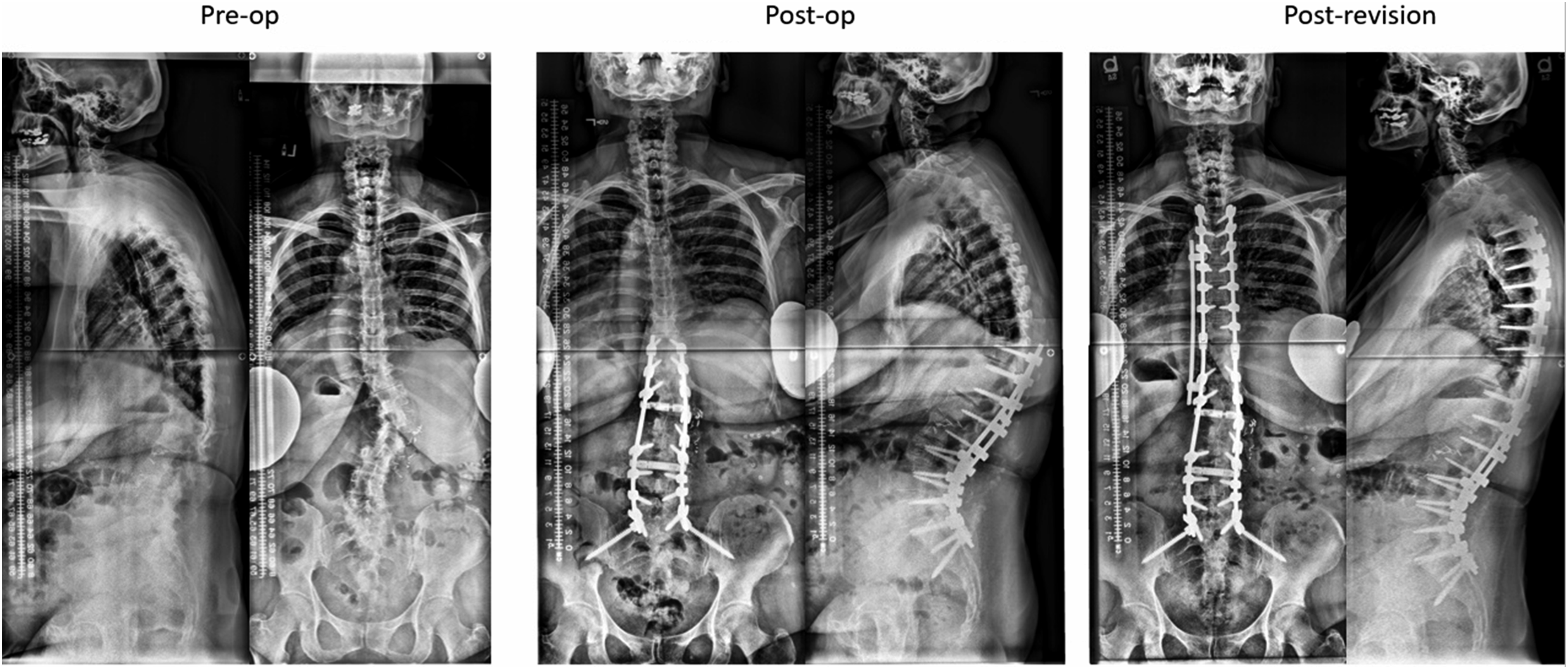
The study population was selected from a prospective multi-center adult spinal deformity registry treated between 2009 and 2019. The database included data on baseline demographics, scoliosis films, and complications (ClinicalTrials.gov identifier: NCT00738439). IRB approvals were obtained from all collaborating institutions prior to subject enrollment, and informed consent was sought from all recruited patients for long-term follow-up. Inclusion criteria for the registry consisted of patients aged 18 or greater at the time of enrollment with a diagnosis of adult degenerative or idiopathic scoliosis meeting at least 1 of the following radiographic criteria of spinal deformity: coronal curvature of the spine greater than 20°, Sagittal Vertical Axis (SVA) > 5 cm, Pelvic Tilt >25°, and/or Thoracic kyphosis >60°. The current investigation only retained surgeons who contributed at least 50 cases and patients who sustained at least 2 consecutive spinal procedures while captured by the registry. For each of these patients, a detailed vignette was created and shared with the operating surgeons. These vignettes included patient demographics, all the relevant dates (inclusion, index surgery, revision surgery, and follow-up visits), dates and descriptions of all complications, detailed description of surgical procedures for the index and revision surgery, as well as coronal/sagittal scoliosis films, radiographic measurements, and PROMs for all visits from pre-op to post-revision surgery (Figures 1 and 2). Example of patient demographics and surgical data for primary and revision surgery sent to each surgeon for review of their own case. Example of pre-operative, post-operative, and post-revision radiographic data sent to surgeon for review.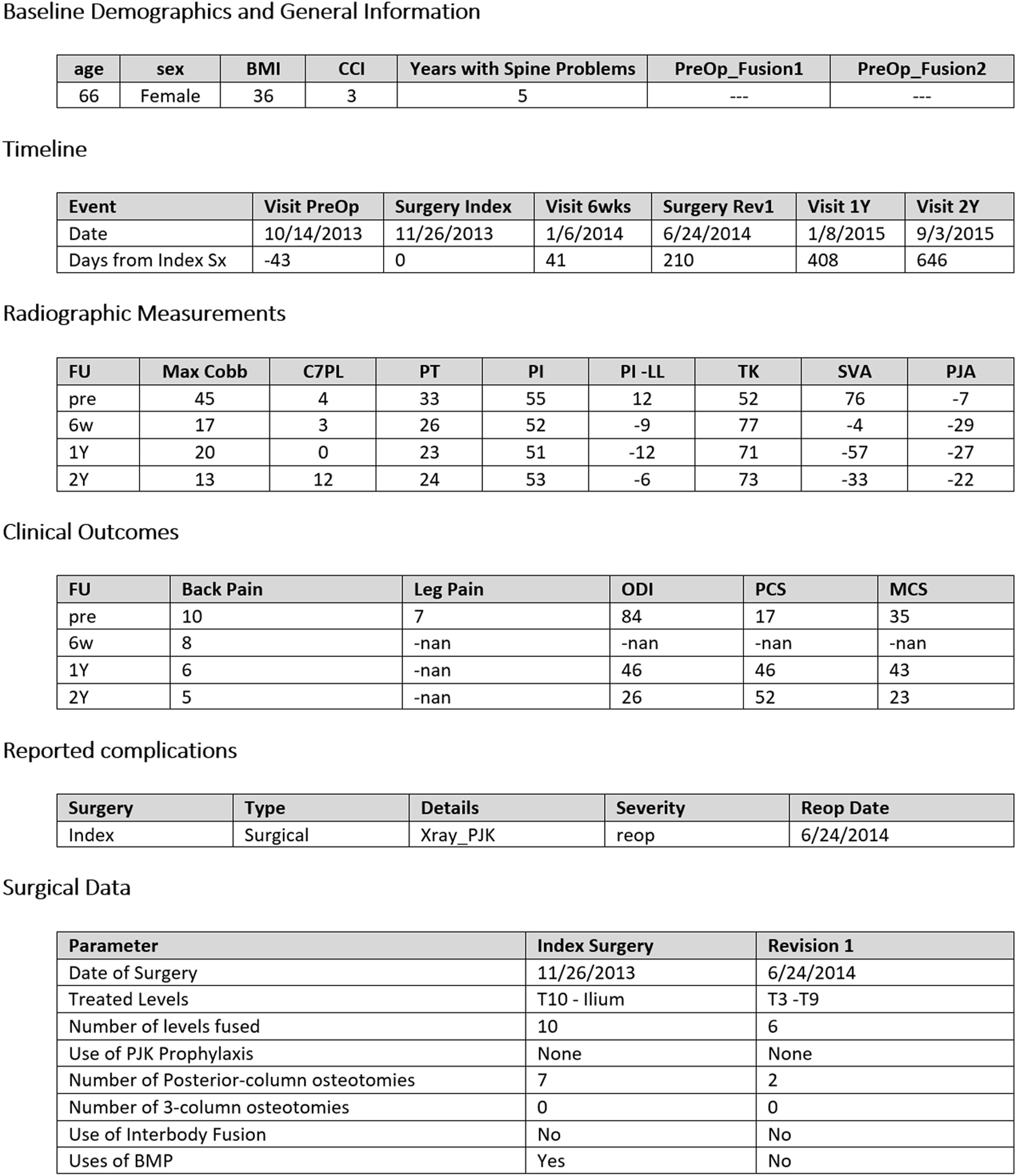
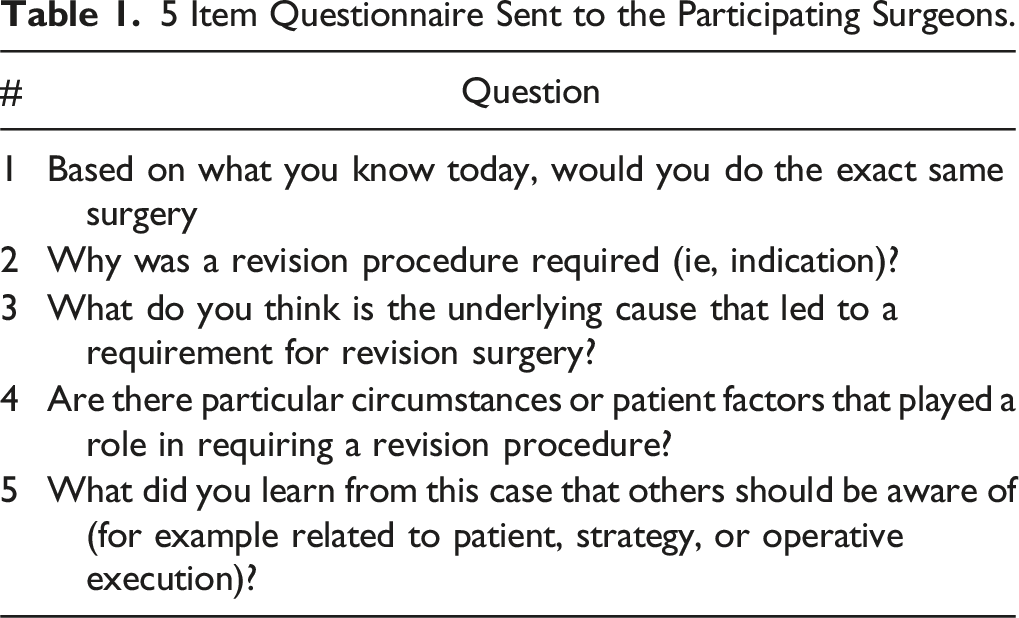
5 Item Questionnaire Sent to the Participating Surgeons.
Results
Cohort Description
The registry query identified 6 surgeons with 437 patients enrolled in the database between 2009 and 2019. Of these, 90 patients (20.6%) sustained a revision surgery, 4 by a different surgeon, and 86 by the same surgeon. The total follow-up period between the no revision group (9.3 months to 9.8 years) and the revision group (9.1 months to 9.1 years) showed no significant difference (P = 0.73). On average, the revision procedure occurred 429 days after the index procedure, ranging from zero days to 5.4 years.
Why was a revision procedure required?
Most Common Indications for Revision Procedure as Reported by Operating Surgeons.
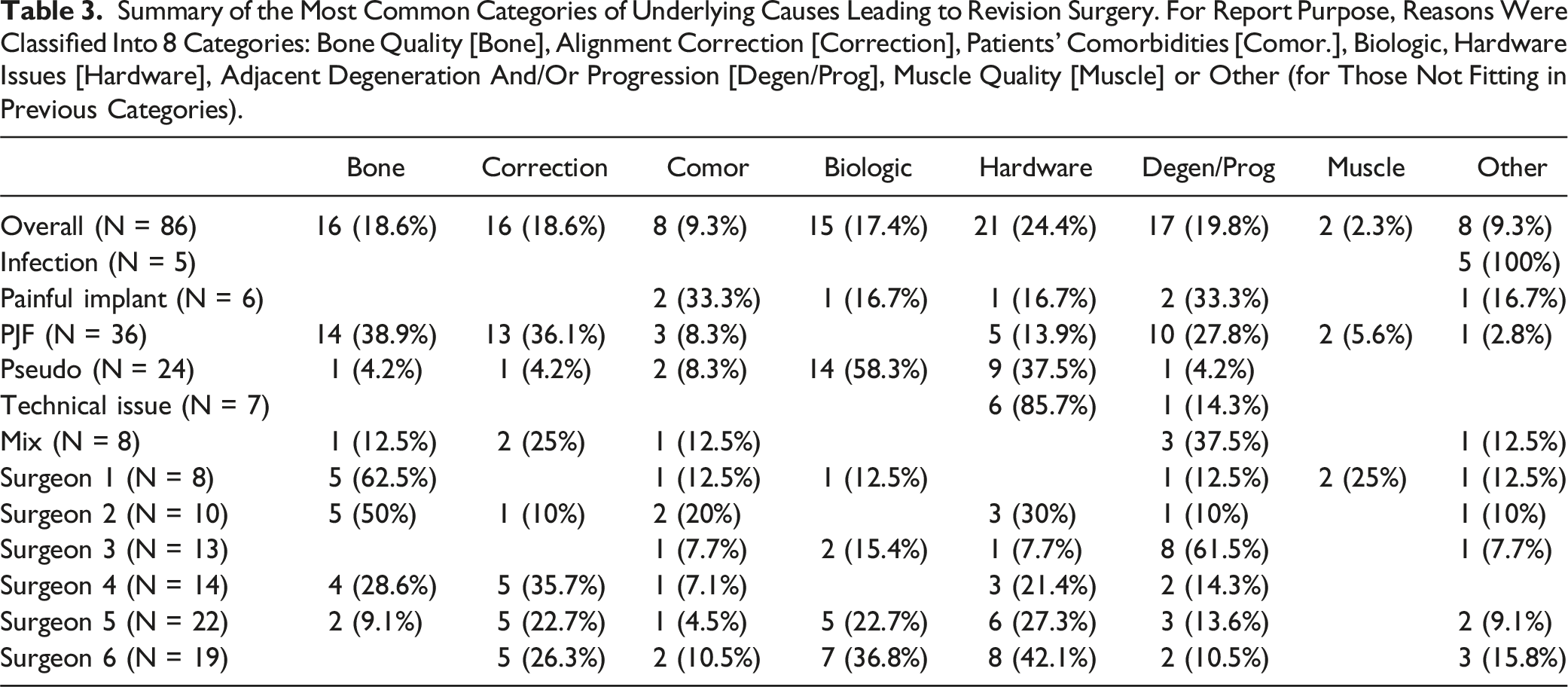
Underlying Cause Leading to Revision
Summary of the Most Common Categories of Underlying Causes Leading to Revision Surgery. For Report Purpose, Reasons Were Classified Into 8 Categories: Bone Quality [Bone], Alignment Correction [Correction], Patients’ Comorbidities [Comor.], Biologic, Hardware Issues [Hardware], Adjacent Degeneration And/Or Progression [Degen/Prog], Muscle Quality [Muscle] or Other (for Those Not Fitting in Previous Categories).
Patient Factors and Circumstances Associated with Revision
The most common circumstances or patient factors determined by the operating surgeon to contribute to an increased likelihood of revision surgery was bone quality (16 patients, 18.6%) defined as osteoporosis and/or osteopenia. The next most common patient factor was pre-operative alignment defined as fixed cervical kyphosis, coronal malalignment, and sagittal imbalance (13 patients, 15.1%). Out of the entire cohort, 12 patients (14.0%) were thought to have comorbidities such as high BMI, frailty, and history of prior fusion that contributed to revision surgery. Technical decision-making such as the use of pedicle subtracting osteotomies (PSO), iliac fixation, screw diameter was thought to contribute to revision surgery in 12 patients (14.0%). Among this cohort of 86 patients, 35 (40.7%) had no specific factors associated with the need for revision procedure according to the operating surgeon.
Would You do the Exact Same Surgery?
Rate of “Yes” to the Question “Would You do the Exact Same Surgery?” Despite Knowing the Patient Underwent Reoperation. Rates Reported Overall, as Well as by Surgeon, Stratified by Reason for Revision, Underlying Cause Leading to Revision, and by Patient Factors or Circumstances Leading to Revision.
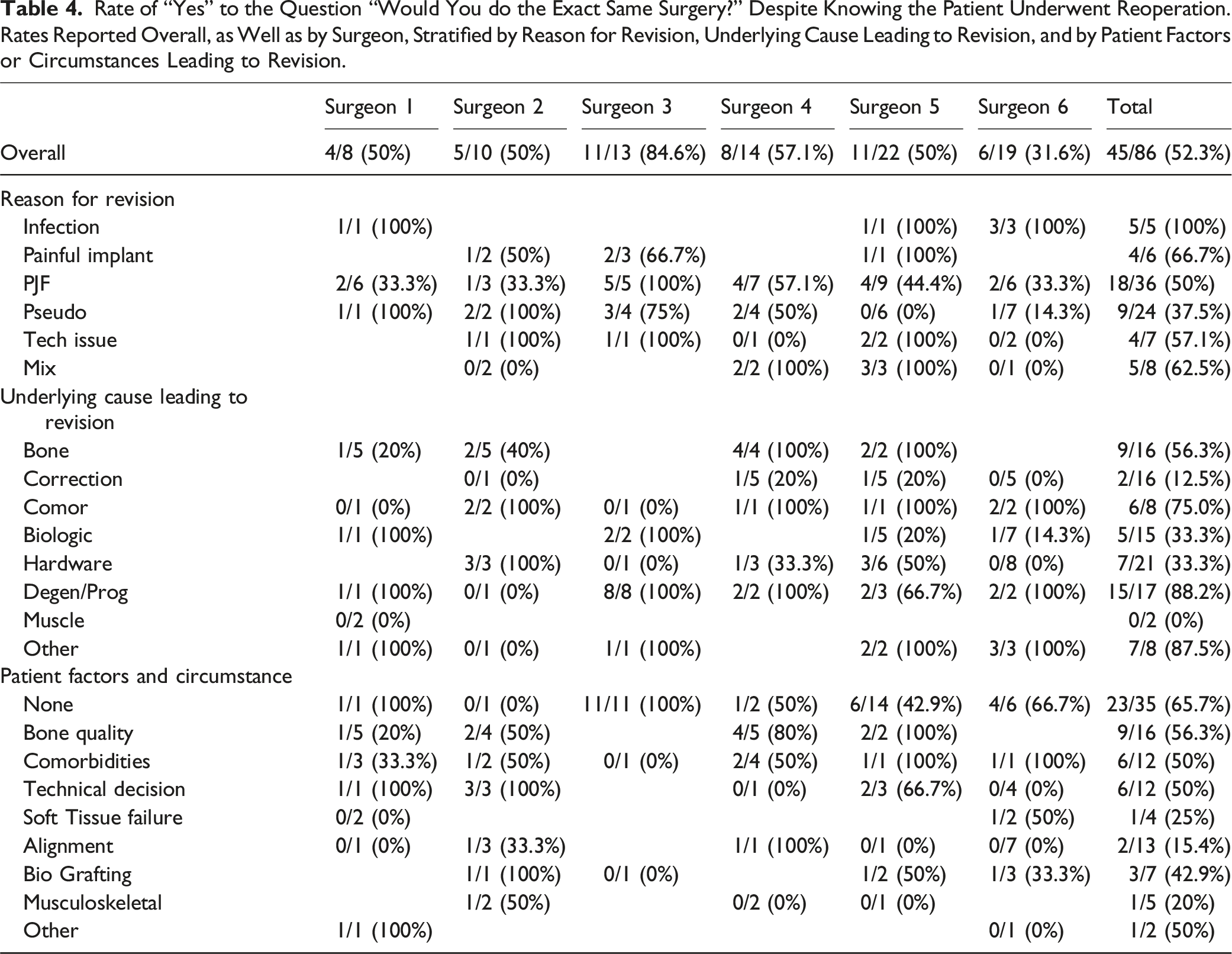
With respect to the main underlying cause leading to revision, the operating surgeons surveyed would perform the exact same surgery for 88.2% of patients having a degeneration and/or progression of the disease, 33.3% of patients revised due to biologic, 33.3% of patients revised due to hardware/instrumentation reasons, and 12.5% of the patients revised due to alignment issue. 65.7% of patients with no particular factor or circumstance playing a role in revision would be treated using the exact same surgery. Alignment factor was found to have the smallest rate (15.4%) of surgeons answering yes to the question “Would you do the same surgery”. Half of the cases presenting risk factor or circumstance related to bone quality (56.3%), comorbidities (50%), technical decision (50%) and biologic/Grafting (42.9%) would receive the same surgery today. A large proportion of patients for whom surgeons would do the same surgery have no particular circumstances/factor playing a role (51.1%). (Table 4).
Learning Points
According to the operating surgeon, most cases (91.9%) led to a learning opportunity including rod related choice (23.3%: contouring, multi-rod construct for PSO or obesity, kickstand rod), level selection (19.8%: extended fusion to thoracic, choice of UIV, extension to cervical spine), PJF prevention (15.1%: tether, cement, thoracic rod contouring), correction related choice (11.6%: use of appropriate goal, transitional anatomy, correction and flexibility), patient selection (10.5%: patient optimization, frail patient and surgical treatment), bone quality (9.3%: osteoporosis, osteopenic), interbody fusion (9.3%: use of interbody lumbar expandable device in lower levels of fusion, IBF and PSO, cage material) and biologic (8.1%: use of BMP).
Discussion
In the cohort of patients included in this study, revision rates were found to be approximately 20%, a high rate consistent with the literature.8-10 The most common indications for revision surgery were PJF and pseudoarthrosis at 41.9% and 27.9% respectively, with underlying causes of revisions determined to be instrumentation failure, degenerative or progression of deformity, and biologics. These underlying factors were further broken down into categories such as bone quality, alignment correction, comorbidities, and technical decisions (PSO, iliac fixation, screw, etc.…). Although revision rates were high, over half of the surgeons were congruent with the original choice of surgery, and reviewing their own cases provided a large opportunity for learning for almost every surgeon surveyed. To our knowledge, this is the first study investigating surgeons’ self-review of adult spinal deformity corrective surgery that required subsequent revision.
Research has shown that two-thirds of PJF occurs within 3 months after the initial surgery and around 80% of PJF presents within a year and a half, 20 with the median time to revision in ASD cases occurring at 308 days. 9 Given this short timeframe, it is likely that the same surgeon will perform the revision procedure and will have the opportunity to adjust the approach. It is important to understand why 52% of surveyed surgeons maintain confidence in their choice of primary procedure, particularly because in 40% of cases, the reason for revision surgery remains unexplained. However, this confidence may not always reflect objective reality, as surgeons’ responses could be influenced by subjective perceptions and biases present at the time of the survey, leading to potential inaccuracies in reporting. Changing a surgeon’s behavior or thought process is inherently challenging and typically requires very significant circumstances to prompt a shift. 21 Spinal alignment issues represented the smallest percentage of underlying cause for maintaining the original surgical strategy, while reasons such as bone degeneration, hardware failure, and biologics were cited as common indications. One area of justification for repeating the original procedure that was unanimously agreed upon was the treatment of infection. ASD specific research regarding technical aspects of ASD surgery such as multiple rod construct or the use of bone morphogenetic protein impact the risk of adverse outcomes and alter the quality of life of patients after surgery,22,23 but infection itself is not an ASD-specific problem and thus is not wholly dependent on the particular technical approach utilized. Although there are high failure rates of primary ASD procedures, surgeons with access to updated guidelines are able to carefully evaluate options for treating patients, and new technologies are yet to be developed that may reduce the risks.
As our study showed, when surgeons were given another opportunity to critically review their own cases in a structured way, more than 90% of cases demonstrated a learning point for future implementation. The formula for making change in ASD surgery is clear, but it requires a multi-pronged approach; knowledge of new techniques, capacity for training and implementation of better solutions, demonstrated improvements in patient reported outcomes measurements, working within a well-resourced health system, and positive interpersonal interactions all lead to faster and more widespread uptake of a new practice24–26. Even with a clear formula, strategies that have been implemented thus far have mixed opinions. Public outcome reporting has been shown in survey studies to be opposed by surgeons due to concerns of mistaking the context of information revealed during a review of cases. 27 Newer standardized education programs for both surgeons and patients have been created in accordance with national physician organizations like the American Orthopaedic Association (AOA) and are expanding to more clinic sites nationwide but are not yet widely implemented for adult spinal deformity. It may be the case that the learning curve for new concept integration is too steep to expect practicing surgeons to adapt in their already limited time.
The revision rates found in our study are in line with those found in literature over 10 year follow up periods,8–10,28 and other investigations also observed PJF as the most common complication.29,30 These complication rates further increase as more osteotomies are needed for correction, 31 especially with confounding poor bone quality, osteoporosis, and other comorbidities.10,32 In an attempt to mitigate the risk of instrumentation complications, recent research has focused on multi-rods techniques across three-column osteotomy sites, use of patient-specific alignment targets based on age, PI, and lordosis distribution, contouring the proximal extremity of the rod, and/or to create semi-rigid junctional fixation through the use of tethers and cement33–38. Despite these complications and attempts at solutions, surgery remains the cornerstone of ASD management despite the increased risk for very sick patients.12,39
The major limitations of this survey-based study include variance in surgical practice at the multiple institutions, the small sample size, and as such the limited statistical analysis. Survey questions were limited to objective findings unless necessary, but inherent recall or response biases may have been present. Although gathering responses from the same surgeons who performed the primary procedure allowed for continuity of responses and self-reflection, the sample size was only able to capture the cases of the 6 participating surgeons. Each of the 6 surgeons may be operating under differing circumstances with regards to patient population and institution policies as well, with variance not entirely represented by the data. Another challenge in collecting responses was the discrepancy in the time elapsed since the revision cases were completed and subsequently reviewed in this study. Some surgeons might have benefitted from being able to better recall a surgery that happened recently as opposed to those who performed revisions close to a decade ago. Additionally, there was no method of external validation for determining whether the reported indications for revision surgery by the performing surgeon were agreed upon by third parties, which limits the generalizability of the results. The majority support of the primary surgical approach in the majority of cases was perhaps due to the paucity of literature available for revision techniques, or similarities in the practice of surgeons operating to standards set by their shared institution, which may be a strength as the results could be focused into tangible points.
Future studies should focus on understanding the clinical reasons behind the failure of primary ASD surgery. Given that learning points were identified, this survey offers a useful exercise for health systems to adopt as they pursue quality improvement measures. Surgical decision making may be influenced in a positive manner via self-review if repeat surveys are administered to an individual surgeon in a private or deidentified manner and correctable patterns are identified. Surgeon behavior is not standardized across health systems and is dependent on training and experience, but this study emphasizes the need for continuous education and access to the latest information after fellowship to ensure the most up-to-date and effective care.
Conclusions
From this study we gained valuable key insights into the decision-making process for spine surgery to treat adult spinal deformity and factors that can influence the decision on revising the initial procedure. In this survey, the most common indications for revision surgery were PJF and pseudoarthrosis (42% and 28%, respectively). Surgeons most common evolving strategies were rod-related techniques, upper and lower instrumented vertebrae, PJF prophylactic strategy and better understanding of sagittal alignment objectives. Despite the large variability in their retrospective opinions about their own revisions, nearly 50% of cases saw opportunities for improvement. This learning potential will hopefully translate to better patient outcomes, and we need ongoing surgeon feedback loops to drive incremental change. ASD surgical treatment is continually evolving, and we must also ensure that surgeons are actively learning and training to adopt newer approaches to mitigate the need for revision surgery. Further research is needed to explore the clinical explanation as to why revision surgeries occurred in this patient population, specifically if no particular factors were identified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
IRB approvals were obtained from all collaborating institutions (ClinicalTrials.gov identifier: NCT00738439).