
Abstract
Study Design
Retrospective multi-institutional study.
Objectives
Although previous studies have evaluated the surgical outcomes of laminoplasty in patients with cervical ossification of the posterior longitudinal ligament (OPLL), the long-term results remain unclear. The purpose of this study is to assess outcomes more than 10 years post-surgery and identify to identify factors that affect the long-term prognosis.
Methods
Eighty-four OPLL patients with more than a minimum of 10-year follow-up after surgery were divided into a good group with more than 50% improvement of the recovery rate of the cervical Japanese Orthopaedic Association (JOA) score, and a poor group with less than 50% improvement. The demographic data and radiographic parameters of cervical spinal alignment were compared, and significant poor prognostic factors were evaluated by multivariate logistic regression.
Results
Four preoperative factors showed significant differences between 2 groups: the presence of type 2 diabetes (P = 0.012), the baseline JOA scores (P = 0.001), the narrowest segment in the cervical (P < 0.001) and the presence of T2-weighted high signal on MRI (P = 0.030). Logistic regression analysis identified 3 of 4 factors were significantly associated with postoperative poor outcomes: the presence of type 2 diabetes (P = 0.011), the baseline JOA scores (P = 0.022), and the presence of T2-weighted high signal on MRI (P = 0.035).
Conclusion
This study identified three risk factors associated with poor long-term surgical outcomes following laminoplasty for cervical OPLL. These findings could be significant indicators for predicting long-term outcomes in cervical OPLL patients.
Keywords
Introduction
Cervical ossification of the posterior longitudinal ligament (OPLL) is a major disease of spinal ligament ossification, predominantly affecting individuals in Asian countries.1,2 About half of the patients with cervical OPLL experience progressive ossification, leading to symptomatic myelopathy. Surgical decompression is often employed to prevent further neurological decline, and the clinical outcomes following these procedures are generally stable. 3
Numerous studies evaluated the surgical outcomes of laminoplasty for cervical OPLL.4-9 A recent study demonstrated the comparable efficacy of both open-door and double-door laminoplasties from prospectively registered OPLL databases. 6 However, most studies assessed the outcomes at short to mid-term follow-up periods, and there are few reports evaluating long-term surgical results for more than 10 years.10-12 Among these studies, Iwasaki et al. purely registered OPLL patients from cervical myelopathy cases and reported slight but significant functional deterioration over 10 years after surgery with the postoperative development of ossification. 10 There was, however, a lack of precise imaging evaluation including radiographic parameters or magnetic resonance imaging (MRI), and a relatively small number of patients enrolled from 2 institutions.
We hypothesize that specific preoperative factors, such as comorbidities and imaging findings, predict long-term functional outcomes following laminoplasty for cervical OPLL. We conducted a multicenter study and performed a comprehensive analysis to identify factors affecting therapeutic outcomes.
Method
Patients
This study was performed as a multi-institutional study including 8 collaborated institutions. Overall, 104 cervical OPLL subjects took posterior cervical laminoplasty, and a minimum of 10 years of follow-up were included. Of these, 84 patients with complete data were finally registered. None of OPLL subjects who underwent surgery of laminectomy, PSF, anterior or combined approaches surgeries in this study. The choice of surgical technique was at the discretion of the surgeon. The patients were excluded if they had an infection or spondylosis. The patients were divided into a good group (GG) which presented more than 50% improvement in the recovery rate of the cervical Japanese Orthopaedic Association (JOA) score, and a poor group (PG) which showed less than 50% improvement, based on previous studies.13-15 The recovery rate was evaluated using the following formula reported by the previous study: (postoperative JOA-preoperative JOA)/(17-preoperative JOA)×100%. 16
Data Collection
Demographic information, medical history, imaging findings, and surgical outcomes were collected. Clinical and surgical outcomes were assessed before surgery, at 2 and 10 years after surgery using the cervical JOA. Those data were measured and evaluated by board-certified spine surgeons in each participating institution.
Imaging
Preoperative radiological examinations were performed using plane radiography, computed tomography, and MRI in all the patients. The types of OPLL were categorized as localized, segmental, continuous, and mixed. 17 The occupying ratio of OPLL and the OPLL’s narrowest segment were evaluated as previously reported. 18 The Cobb angle between C2 and C7, C7 slope, C2-C7 sagittal vertical axis (SVA), and the cervical range of motion (ROM) calculated by subtracting the flexion from the extension C2 to C7 angles were evaluated using plain radiography at preoperative, at 2 years and 10 years after surgery, respectively. Preoperative MRI was used to evaluate the high signal intensity area on the T2-weighted images.
Statistical Analysis
Continuous variables and frequencies are presented as means ± standard deviations and categorical variables as percentages. The baseline demographics, imaging characteristics and cervical JOA scores in the 2 groups were compared using the Wilcoxon signed-rank test for continuous variables and Fisher’s exact tests for the categorical variables. The Wilcoxon signed-rank test was applied for the changes in cervical spinal angles before and after surgery. To remove type-Ⅰ error, false discovery rate (FDR) control based on Benjamini-Hochberg method was applied. Adjusted P-value by FDR <0.05 was considered statistically significant in this stage.
The variables showing significance in the above are evaluated in association with the poor clinical outcome using multivariate logistic regression. Logistic regression analysis was also applied for continuous variables to evaluate appropriate cut-off values. A P value <0.05 was considered statistically significant. All the statistical analyses were performed using R software version 4.4.0.
Result
Demographics
Demographics of the OPLL Subjects Who Underwent Laminoplasty.
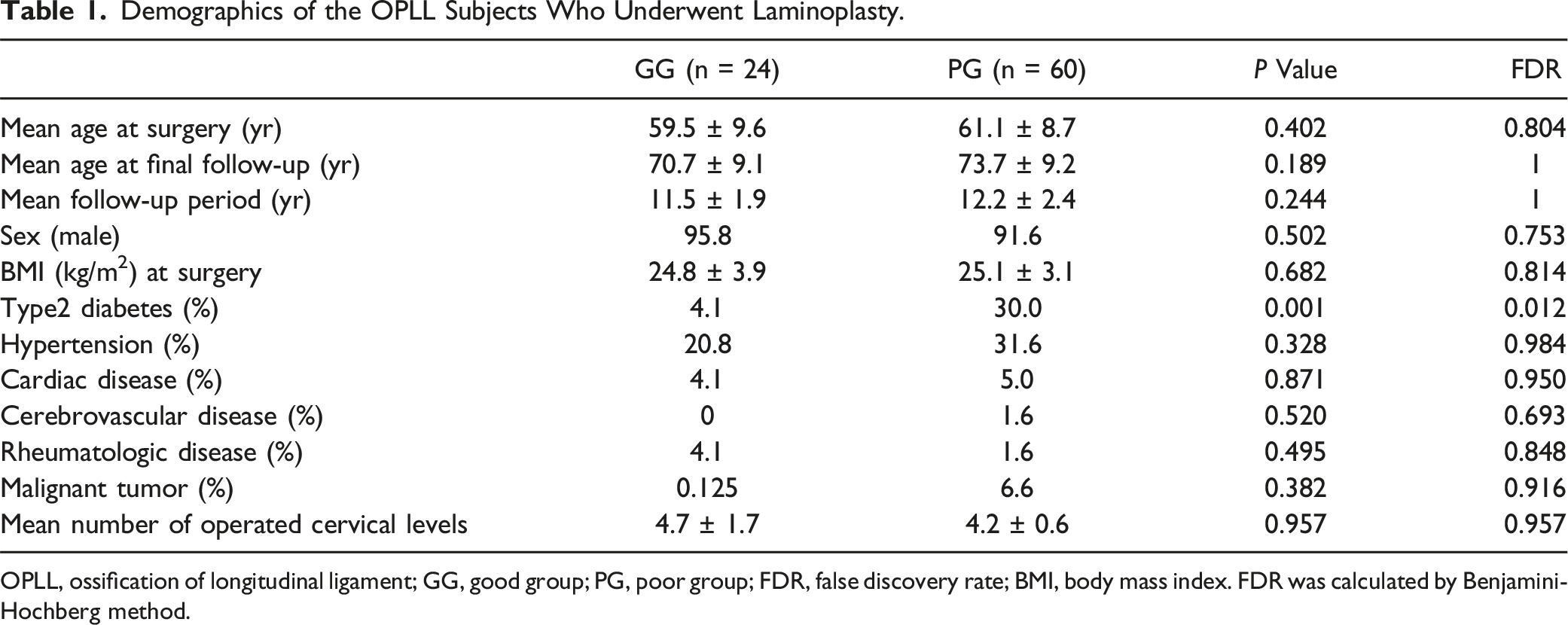
OPLL, ossification of longitudinal ligament; GG, good group; PG, poor group; FDR, false discovery rate; BMI, body mass index. FDR was calculated by Benjamini-Hochberg method.
Imaging Characteristics
Imaging Characteristics.
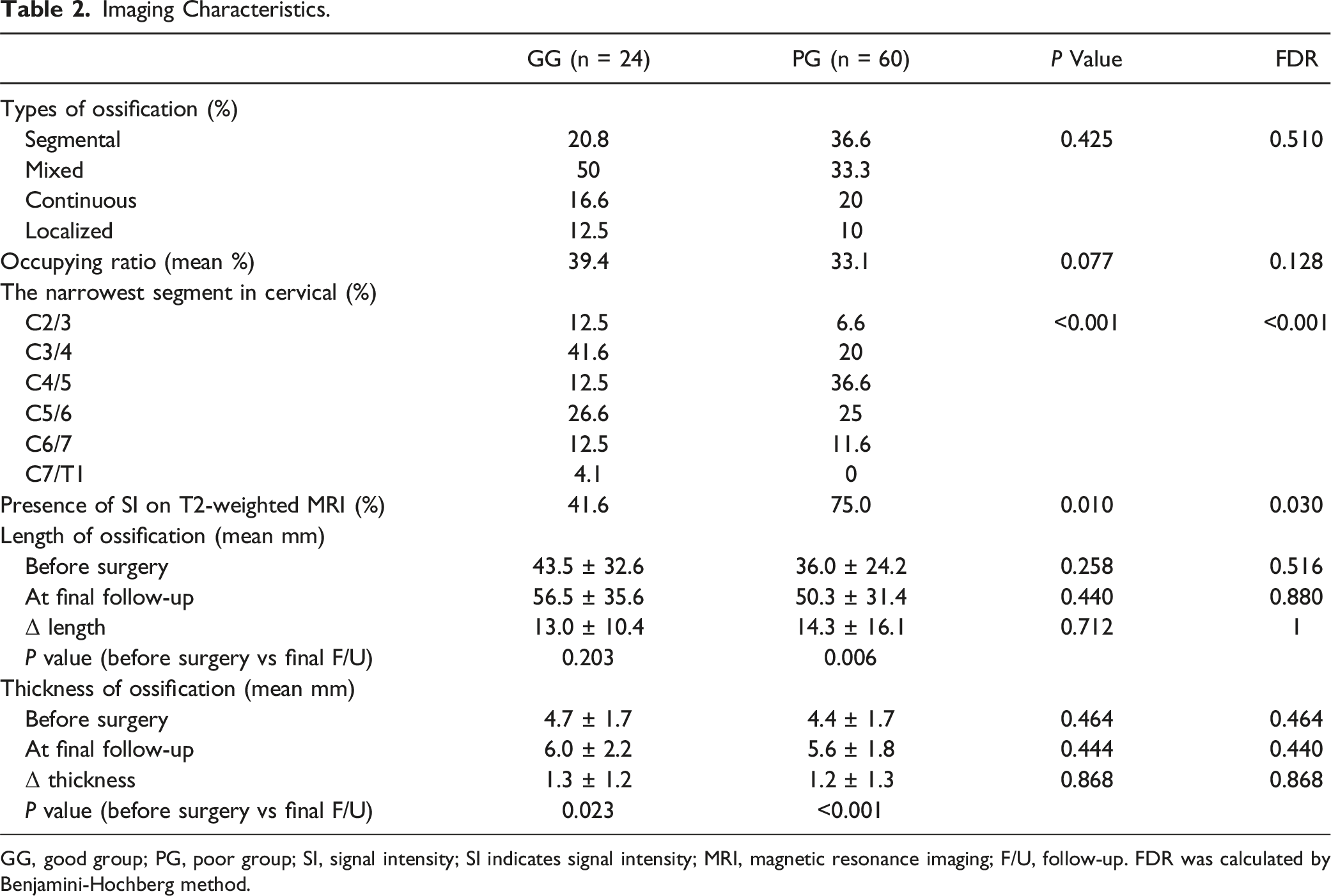
GG, good group; PG, poor group; SI, signal intensity; SI indicates signal intensity; MRI, magnetic resonance imaging; F/U, follow-up. FDR was calculated by Benjamini-Hochberg method.
The intermediate C2 to C7 angles were 14.3 ± 9.26° in the GG and 12.6 ± 12.9° in the PG before surgery (P = 0.741), 10.5 ± 7.67° in the GG and 9.68 ± 12.3° in the PG (P = 1) at the 2-year follow-up, and 13.2° ± 8.58° in the GG and 11.1 ± 15.2° in the PG (P = 1) at final follow-up. From the preoperative period to 2 years and 10 years after surgery, there were no statistically significant differences in the temporal changes of these angles (Figure 1A, Table 3). The C7 slope angle was 23.7 ± 8.8° in the GG and 25.0 ± 8.7° in the PG before surgery (P = 1), 27.7 ± 9.9° in the GG and 26.3 ± 10.3° in the PG (P = 1) at the 2-year follow-up, and 29.9 ± 9.5° in the GG and 29.4 ± 10.6° in the PG (P = 0.893) at final follow-up. Both groups showed significant increases in the C7 slope from the period before surgery to the final follow-up (GG, P = 0.032; PG, P = 0.016) (Figure 1B, Table 3). The C2-C7 SVA was 26.8 ± 13.6 mm in the GG and 27.5 ± 19.6 mm in the PG before surgery (P = 0.859), 29.7 ± 14.4 mm in the GG and 28.9 ± 17.2 mm in the PG (P = 0.844) at the 2-year follow-up, and 38.9 ± 14.3 mm in the GG and 37.3 ± 15.6 mm in the PG (P = 0.901) at final follow-up. Both groups exhibited significant increases in C2-C7 SVA from the time at preoperation to final follow-up (GG, P = 0.004; PG, P = 0.022), as well as from the 2-year to final follow-up (GG, P = 0.034; PG, P = 0.008) (Figure 1C, Table 3). Changes of cervical alignment parameters and cervical JOA score before surgery, at 2-year follow-up and at final follow-up. (A)Intermediate C2 –C7 angle, (B) C7 slope, (C) C2 –C7 SVA, (D) Cervical ROM. * represents the significance between before surgery and 2-year follow-up scores, before surgery and final follow-up scores and 2-year and final follow-up scores in GG and PG, respectively. # represents the significance between GG and PG before surgery, at 2-year follow-up and final follow-up, respectively; SVA, sagittal vertical axis; ROM, range of motion; *, P < 0.05. Imaging Characteristics of Cervical Alignment. GG, good group; PG, poor group; F/U, follow-up; SVA, sagittal vertical axis; ROM, range of motion. FDR was calculated by Benjamini-Hochberg method.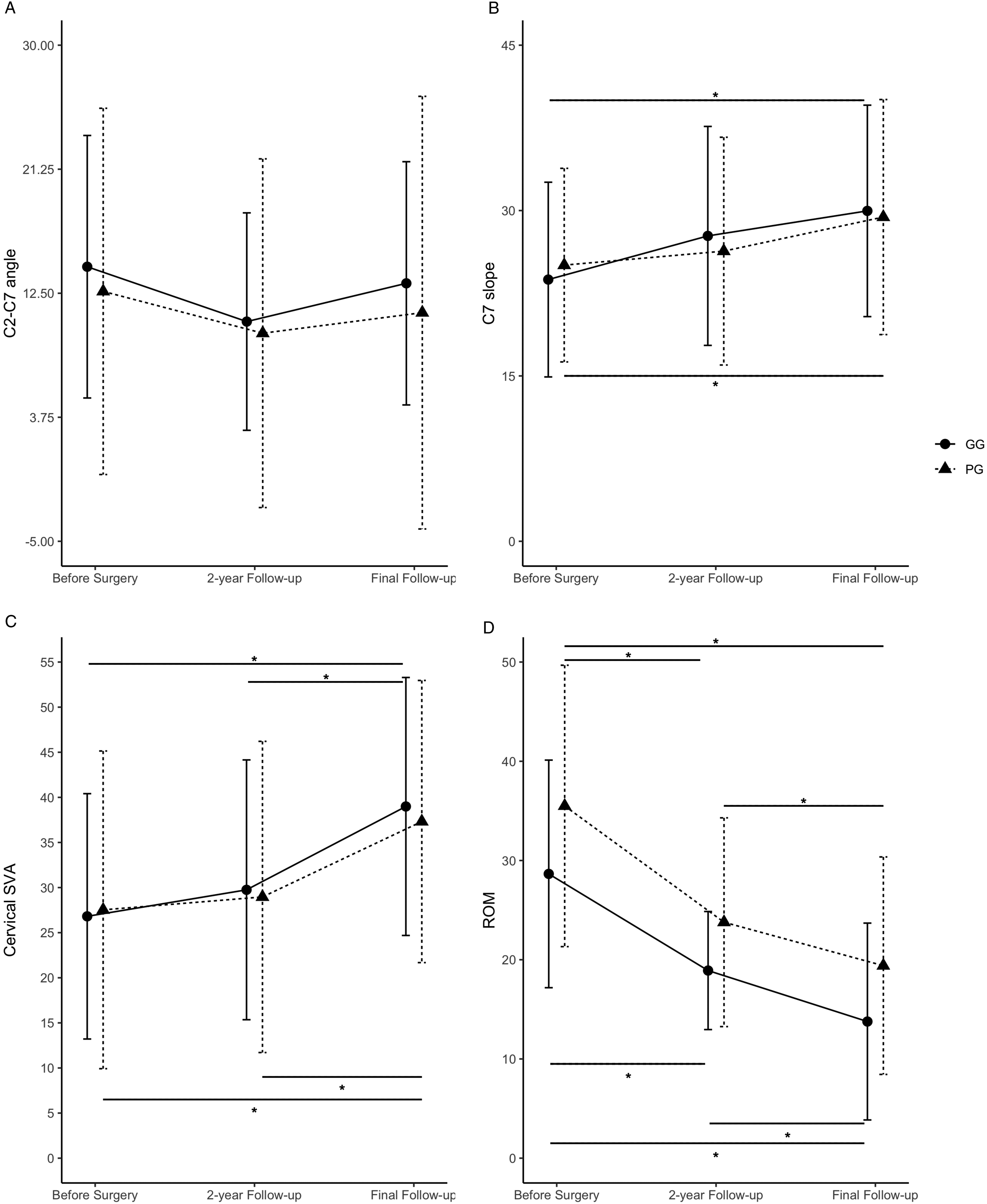
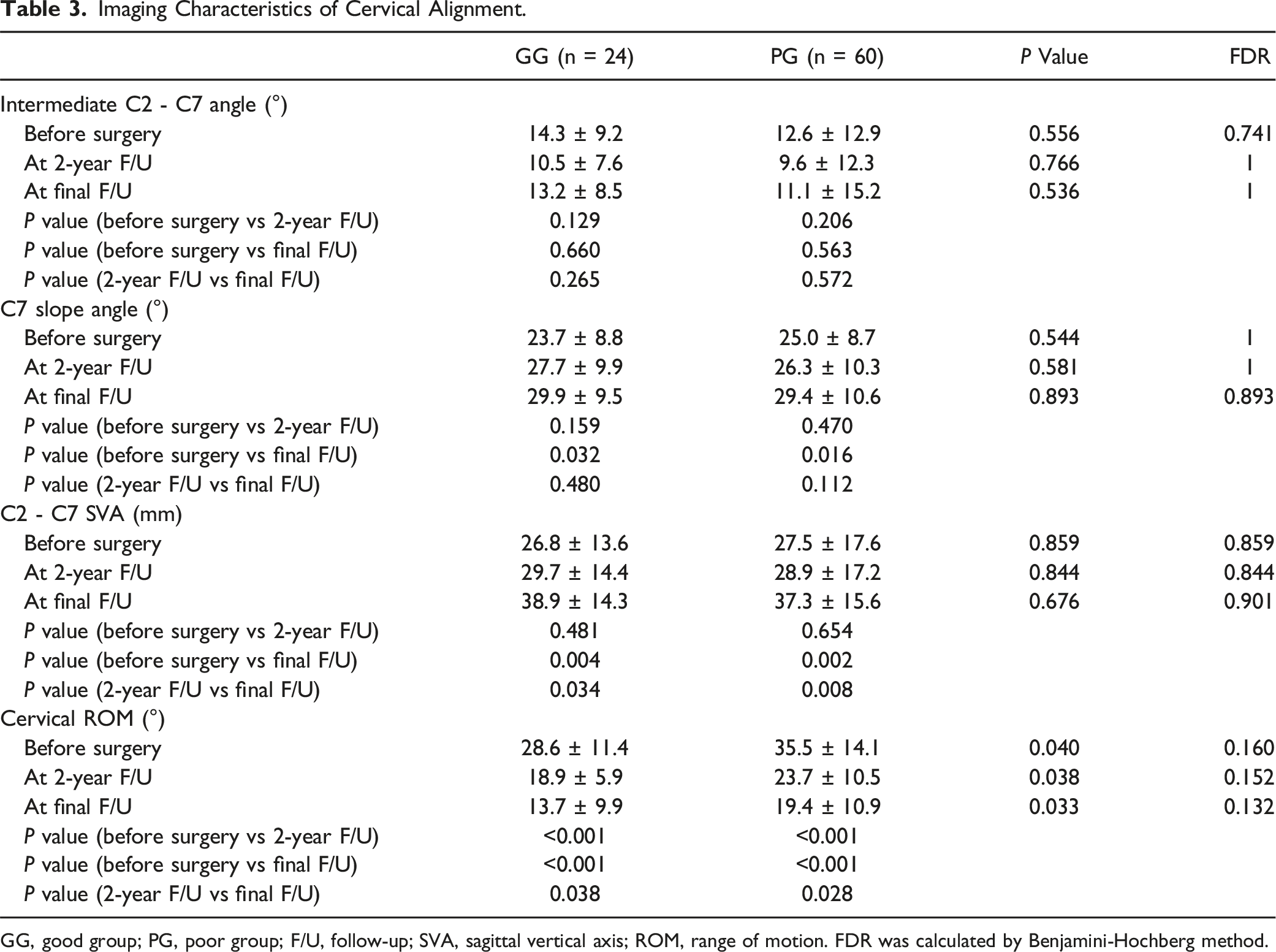
Before surgery, the ROM was 28.6 ± 11.4° in the GG and 35.5 ± 14.1° in the PG (P = 0.160). At the 2-year follow-up, it was 18.9 ± 8.9° in the GG and 23.7 ± 10.5° in the PG (P = 0.152), and 13.7 ± 9.9° in the GG and 19.4 ± 10.9° in the PG (P = 0.132) at the final follow-up. The 2 groups showed significant decreases in ROM between the preoperation and at 2-year follow-up (GG, P < 0.001; PG, P < 0.001), preoperation and final follow-up (GG, P < 0.001; PG, P < 0.001), and at 2-year and final follow-ups (GG, P = 0.038; PG, P = 0.028) (Figure 1D, Table 3). Changes in signal intensity in the spinal cord were observed on preoperative T2-weighted MRI in both groups (GG, 41.6; PG, 75.0%; P = 0.030), with a significantly higher frequency in the PG (Table 2). There were no cases showing instability in this study.
Clinical Outcomes
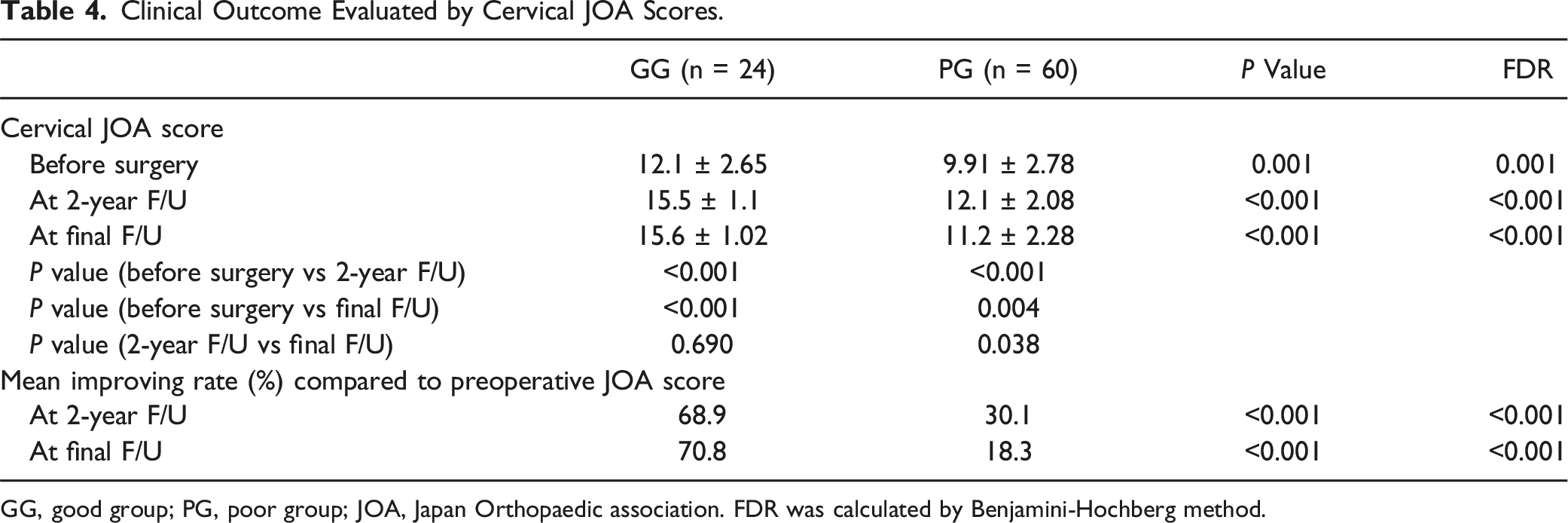
The baseline severity assessed using the cervical JOA score was 12.1 ± 2.6 in the GG and 9.9 ± 2.7 in the PG (P = 0.001) before surgery, 15.5 ± 1.0 in the GG and 12.1 ± 2.0 in the PG (P < 0.001) at the 2-year follow-up, and 15.6 ± 1.0 in the GG and 11.2 ± 2.2 in the PG (P < 0.001) at final follow-up. Both groups demonstrated a statistically significant improvement in JOA score from preoperation to the 2-year follow-up (GG, P < 0.001; PG, P < 0.001), as well as from preoperation to the final follow-up (GG, P < 0.001; PG, P = 0.004). In the GG, there was no significant improvement between the 2-year and final follow-ups (P = 0.690). On the other hand, in the PG, a significant decrease in JOA score was observed between at 2-year and final follow-ups (P = 0.038) (Figure 2, Table 4). The improving rate was 68.9% in the GG and 30.1% in the PG (P < 0.001) at the 2-year follow-up, and 70.8% in the GG and 18.3% in the PG (P < 0.001) at the final follow-up (Table 4). In terms of C5 palsy after laminoplasty, 3 patients in GG showed C5 palsy but the incidence of C5 palsy showed no significant differences between PG and GG (P = 0.55). Changes of cervical JOA score before surgery, at 2-year follow-up and at final follow-up. * represents the significance between before surgery and 2-year follow-up scores, before surgery and final follow-up scores and 2-year and final follow-up scores in GG and PG, respectively. # represents the significance between GG and PG before surgery, at 2-year follow-up and final follow-up, respectively. JOA indicates Japan Orthopaedic Association; *, P < 0.05; #, P < 0.05. Clinical Outcome Evaluated by Cervical JOA Scores. GG, good group; PG, poor group; JOA, Japan Orthopaedic association. FDR was calculated by Benjamini-Hochberg method.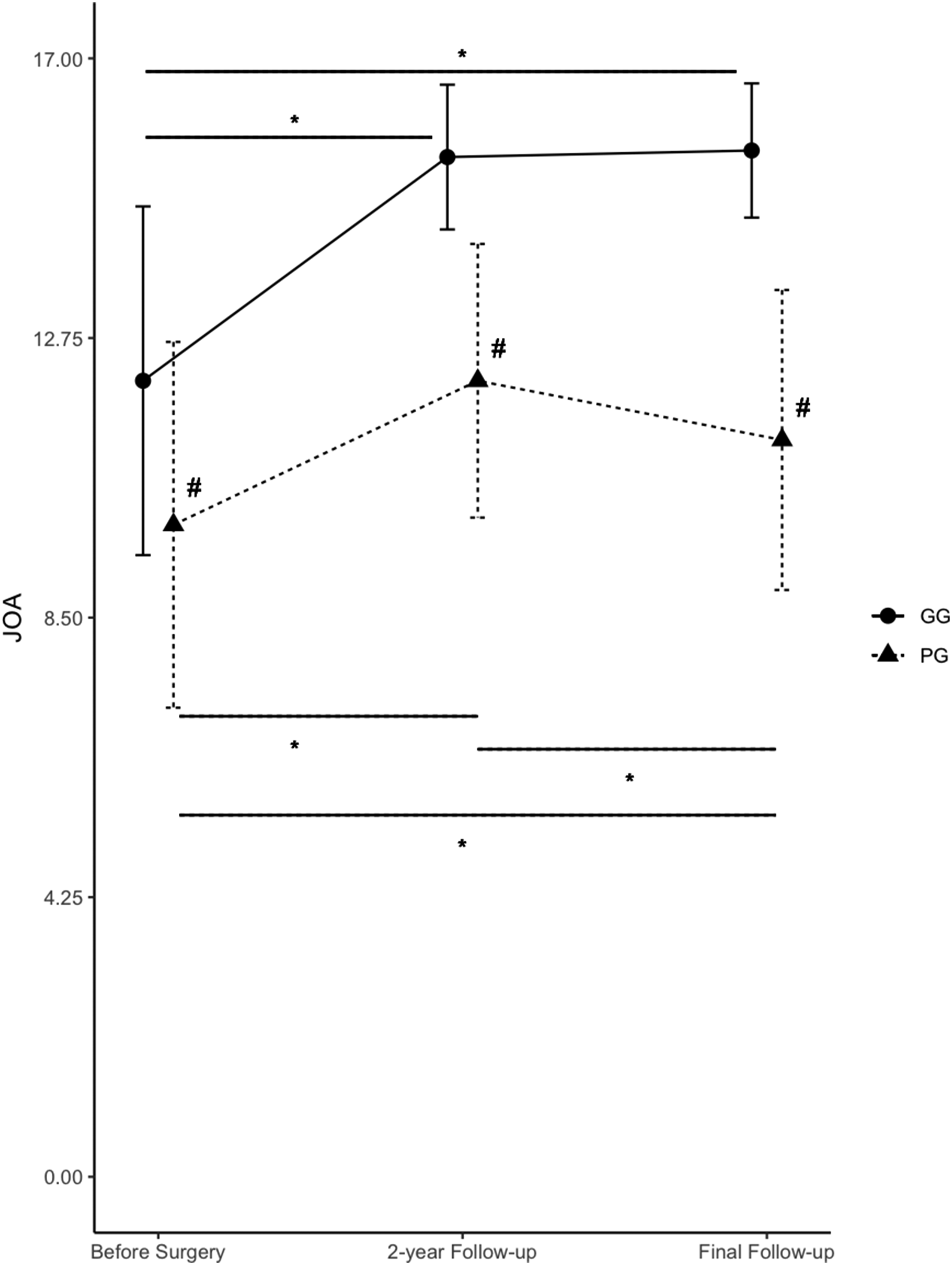
Evaluation of Risk Factors
Evaluation of Susceptible Predictive Factors by Multivariate Logistic Regression.
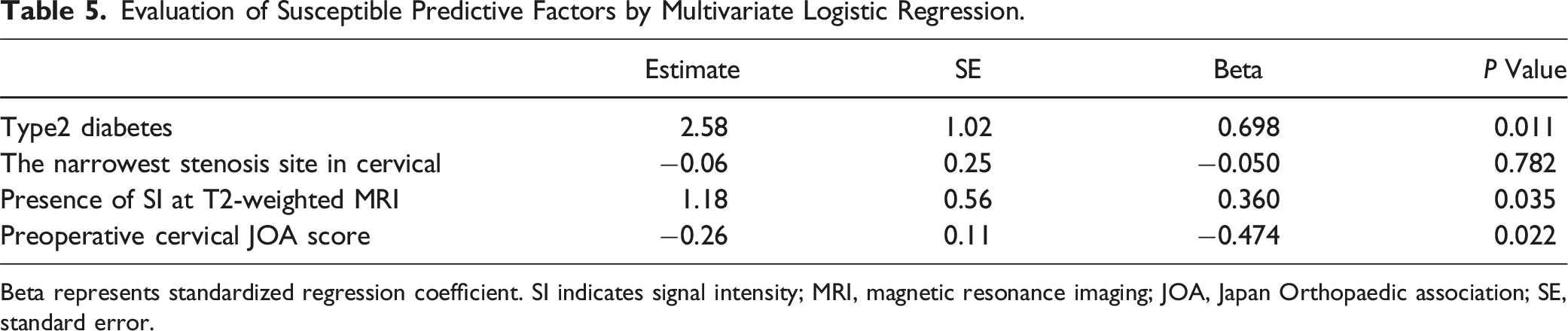
Beta represents standardized regression coefficient. SI indicates signal intensity; MRI, magnetic resonance imaging; JOA, Japan Orthopaedic association; SE, standard error.
Discussion
In this study, we evaluated the demographics, ossification status, radiographic parameters, and clinical outcomes in OPLL patients who underwent laminoplasty and were followed up for more than 10 years. Although both the good and poor recovery groups showed significant functional improvement at 2 years postoperatively, the good recovery group maintained this improvement during the long follow-up period, whereas the poor recovery group experienced significant deterioration from 2 years to the final follow-up. These poor clinical outcomes were significantly associated with 3 independent preoperative factors: comorbidity of type 2 diabetes, high signal intensity on T2-weighted MRI. This study is the first to identify factors influencing long-term surgical outcomes in cervical OPLL. Previous study demonstrated that JOA scores have dropped in OPLL group after long-term follow up compared to CSM. 11 The same effect has been observed in this study.
Diabetes has been reported to affect the treatment outcomes of laminoplasty for OPLL negatively. Kimura et al. reported that in their prospective study of 402 cervical OPLL cases, postoperative functional and QOL-related improvements were significantly worse in patients with diabetes. 17 While their follow-up period was 2 years postoperatively, our long-term follow-up also revealed that diabetes adversely affects functional improvement. Although preoperative HgbA1c levels were not examined in this study, previous research has reported that it does not impact surgical outcomes.17,18 Therefore, regardless of the severity of diabetes, careful attention is required when performing cervical posterior decompression surgery in diabetic patients, considering their long-term prognosis.
Previous studies have shown that changes in intramedullary signal intensity on T2-weighted MRI are associated with poor clinical results. Wang et al. reported that higher signal intensity combined with positive pyramidal signs indicated a poor surgical outcome due to the reduced recuperative potential of the spinal cord in OPLL patients. 19 Similarly, Ito et al. demonstrated that high signal intensity in the compressed spinal cord was strongly associated with surgical outcomes for cervical OPLL. 20 The current study extends their findings, showing poor functional recovery even more than 10 years after laminoplasty. Because the signal changes are not only a sign of poor long-term prognosis but also correlate with the severity of preoperative neurological symptoms, 20 surgical decompression should be performed promptly before the spinal cord undergoes degeneration. Other study suggested that factors such as the presence of T1 low signal intensity or the extent of the T2 high signal intensity suggested indicative of irreversible changes. 21 In this study, we could investigate only the presence or absence of T2 high signal intensity, and no follow-up MRI imaging was performed. Therefore, based on our result, it is not possible to determine whether the observed signal changes reflect irreversible spinal cord damage or ongoing demyelination. Further studies are demanded to investigate association preoperative comprehensive MRI assessments with postoperative imaging follow-up. Regarding dynamic positional changes, previous study demonstrated that dynamic positional changes of the cervical spine affected the degree of spinal cord compression, and those changes are associated with the presence of signal intensity. 22 This suggests that spinal cord signal changes are influenced not only by static compression but also by dynamic mechanical factors. It is possible that increased compression of the spinal cord due to both OPLL and dynamic factors leads to ischemic changes, thereby contributing to the observed MRI signal changes.
In cervical OPLL, the narrowest stenosis site showed significance in comparative analysis but was not significant in multivariate analysis. And incidence of C5 palsy after laminoplasty between 2 groups. This suggested that the location of the narrowest stenosis site does not have a significant effect on the pathophysiology. In PG group, the length of OPLL at final follow-up was significantly longer than preoperative length. However, change of length was not significance between GG and PG, which indicated that rate of change had no effect on surgical outcome. In this study, changes in OPLL progression have not affected postoperative outcomes.
There have been numerous studies that preoperative baseline function affects surgical outcomes in patients with compressive cervical myelopathy.23,24 However, many of these reports focus on the association between clinical outcomes and short-term follow-up periods of about 2 years postoperatively. In contrast, Iwasaki et al. reported that preoperative neurological function was a prognostic predictor for postoperative outcomes in cervical OPLL patients over an observation period of more than 10 years. 10 In term of preoperative JOA score, our result replicated their research and showed that moderate to severe myelopathy needs surgical treatment.25-27 Together, these findings and ours suggest that even considering long-term outcomes, early surgical intervention before significant functional deterioration is crucial for managing OPLL.
This study has several limitations. First, the retrospective design inherently introduces bias, resulting in a lower level of evidence. In fact, our presented scoring system only includes patients who survived more than 10 years postoperatively, excluding those who required reoperation or died. Second, the sample size is still not large, so higher-evidence studies are needed to validate our findings. Third, lack of adequate follow-up of type 2 diabetes history and treatment. The severity of type 2 diabetes might affect the result. Fourth, the measurement of OPLL was performed by board-certified spine surgeons in each participating hospital. Ideally, such measurements should be conducted independently by multiple physicians including radiologists. Finally, the surgical indications, techniques, and postoperative therapies, such as medication and rehabilitation, were left to the discretion of the operating surgeons, which may have influenced the surgical outcomes. Despite these limitations, this study is the first to collect and evaluate long-term (over 10 years) surgical outcomes in cervical OPLL patients and prognostic factors. Given the advancing age of the population, we believe these findings will become increasingly important in the future.
In conclusion, we evaluated clinical outcomes for patients with cervical OPLL who underwent laminoplasty and were followed up for more than 10 years. Three poor prognostic factors were identified. These findings could serve as significant indicators for predicting long-term outcomes in cervical OPLL patients.
Footnotes
Author Contributions
Nao Otomo: conceptualization, methodology, data analysis, data collection, writing original draft, reviewing and editing, figure conceptualization and design. Narihito Nagoshi: conceptualization, data collection, reviewing, editing draft and supervision. Hitoshi Kono, Azusa Miyamoto, Reo Shibata, Soraya Nishimura, Yasuhiro Kamata, Kenshi Daimon, Toshiki Okubo, Yoshiomi Kobayashi, Takahito Iga, Satoshi Suzuki and Masahiro Ozaki: data collection. Junichi Yamane, Morio Matsumoto, Masaya Nakamura, Kota Watanabe: reviewing draft. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.