
Abstract
Objectives:
This systematic review examines advancements in computed tomography imaging-based classification systems and their implications for surgical decision-making in managing cervical ossification of the posterior longitudinal ligament.
Methods:
This study is a systematic review. A comprehensive search of PubMed, MEDLINE, and Scopus databases identified relevant studies published from January 2010 to July 2024. The search utilized keywords including “ossification of the posterior longitudinal ligament,” “cervical,” “spine,” “computed tomography,” and “classification.” Studies meeting predefined inclusion criteria focused on computed tomography imaging for diagnosing and surgically managing cervical ossification of the posterior longitudinal ligament. The study adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and the ROBINS-I tool was used for risk of bias assessment.
Results:
Sixteen studies were included, demonstrating that computed tomography imaging enhances diagnostic precision and classification reliability for cervical ossification of the posterior longitudinal ligament. Comparative analysis across studies revealed consistent trends in computed tomography-based classification improving surgical decision-making, particularly influencing anterior approaches such as anterior controllable antedisplacement and fusion. However, moderate to severe risks of bias were identified in some studies, primarily due to confounding variables and deviations from intended interventions. Additionally, computed tomography imaging’s role in prevalence studies has been expanded by incorporating, which highlights its epidemiological significance. The review also discusses the disadvantages of computed tomography, including radiation exposure and cost implications.
Conclusions:
Computed tomography imaging is a crucial modality for diagnosing and managing cervical ossification of the posterior longitudinal ligament, offering superior lesion classification and guiding surgical decision-making. Future research should refine classification systems and integrate multimodal imaging approaches to enhance diagnostic and therapeutic precision.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a pathological condition characterized by abnormal calcification of the posterior longitudinal ligament within the spinal column, predominantly affecting the cervical region.1 –4 This disorder often leads to severe clinical manifestations, including myelopathy and radiculopathy, which arises due to compression of the spinal cord and nerve roots. Consequently, the accurate diagnosis and effective management of OPLL are critical in preventing neurological deterioration and improving patient outcomes.1,4
Historically, the classification of OPLL has relied heavily on plain radiographic methods, particularly lateral radiographs.1,2 However, the intricate three-dimensional architecture of OPLL frequently renders radiographs insufficient for a thorough evaluation.2,3 The advent of advanced imaging modalities, especially computed tomography (CT), has instigated a significant shift in the diagnostic approach to OPLL. CT imaging surpasses traditional methods by offering superior visualization of the ossified lesions’ extent and morphology, enabling more precise classification and facilitating customized surgical planning.1,2,4
Surgical intervention remains a cornerstone in the treatment of OPLL, particularly for patients presenting with significant neurological deficits. The complexity of OPLL demands a meticulous approach to spinal surgery, where the choice of surgical techniques, whether anterior, posterior, or a combined approach, is informed by the precise characterization of the ossified lesion. Recent studies have introduced various CT-based classification systems that provide a more nuanced assessment of OPLL.1,2,5,6 These systems have been pivotal in guiding surgical decision-making and tailoring the surgical approach to achieve optimal decompression and stabilization of the cervical spine.1,2,5,6 Despite these advancements, there remains an unmet need for a standardized classification system that is universally applicable across diverse patient populations and adaptable to various surgical contexts.
This systematic review endeavors to critically analyze the extant literature on CT imaging-based classification systems for cervical OPLL and their implications for surgical strategy formulation and treatment outcomes. By synthesizing evidence from multiple studies, this review seeks to elucidate the progress achieved in this domain, identify persisting gaps in knowledge, and suggest avenues for future research that could further refine surgical techniques and improve patient care.
Methods
This study is a systematic review conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, focusing on advancements in CT imaging and its implications on surgical strategies for managing cervical OPLL. 7
Literature search strategy
A literature search was conducted using PubMed, MEDLINE, and Scopus databases to identify relevant studies published between January 1, 2010, and July 31, 2024. The search strategy employed a combination of Medical Subject Headings (MeSH) terms and keywords, including “OPLL,” “Cervical,” “Spine,” “CT,” and “Classification.” This systematic review adhered to the PRISMA guidelines 7 to ensure a comprehensive and unbiased search. Additionally, reference lists of relevant articles were manually screened to capture any studies that might have been missed during the database search.
Inclusion and exclusion criteria
The inclusion criteria for the review encompassed randomized controlled trials (RCTs) and observational cohort studies, without limitations on study design, and including both retrospective and prospective studies. Only articles written in English with accessible abstracts and full texts were considered. Studies excluded from the review were case reports, reviews, meta-analyses, and studies without available abstracts or full texts. Non-English language articles were also excluded. Two reviewers conducted the study selection process independently, with discrepancies resolved through discussion and, if necessary, by consultation with a third reviewer.
Data extraction
Data extraction was performed using a standardized data extraction form, recording details such as authors, year of publication, journal, study title, objectives, specific patient groups, methods, sample size, nationality, type of study, classification systems used, measurement parameters, statistical tools, performance, accuracy, results, and outcomes. To ensure data accuracy, a second independent reviewer cross-verified all extracted data, resolving any inconsistencies through discussion or, if required, consultation with a third reviewer.
Risk of bias assessment
The risk of bias in nonrandomized studies was assessed using the ROBINS-I tool (Cochrane, London, UK, Risk Of Bias In Non-randomized Studies – of Interventions), 8 which evaluates biases across domains such as confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. For RCTs, the Cochrane Risk of Bias Assessment Tool (RoB 2) 9 was employed, evaluating domains including the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was rated as having a low, moderate, serious, or critical risk of bias. The risk of bias assessment was conducted independently by two reviewers, with discrepancies resolved through discussion or, when necessary, by involving a third reviewer.
Data synthesis
The extracted data were synthesized and analyzed to compare the outcomes of the various studies. A systematic synthesis was performed due to the heterogeneity of the study designs, patient populations, and outcome measures. The findings were then categorized based on the primary focus of the studies, including the classification systems used, imaging modalities evaluated, surgical strategies, and surgical outcomes reported.
Results
Literature search results
The systematic literature search identified a total of 630 records from the MeSH, MEDLINE, and Scopus databases after duplicate records and the article Language in non-English were removed. Titles were reviewed, leading to the exclusion of 365 records that were deemed irrelevant to the study’s focus. Abstract assessments excluded 283 reports, including 157 review articles, 32 meta-analyses, 5 letters to the editor, and 89 case reports. During the full-text assessment, an additional 108 reports were excluded due to various reasons, such as not being related to cervical spine studies, not involving CT-scan studies, or focusing on artificial intelligence, expert opinions, or consensus studies. Ultimately, 16 studies were selected as the best match for inclusion in the review. These studies were chosen based on their relevance to clinical practices, CT imaging, and surgical strategies for managing cervical OPLL in spine surgery. The study selection process is summarized in the PRISMA flow diagram (Figure 1), which includes the reasons for exclusions at each stage.

PRISMA flow diagram in this systematic study.
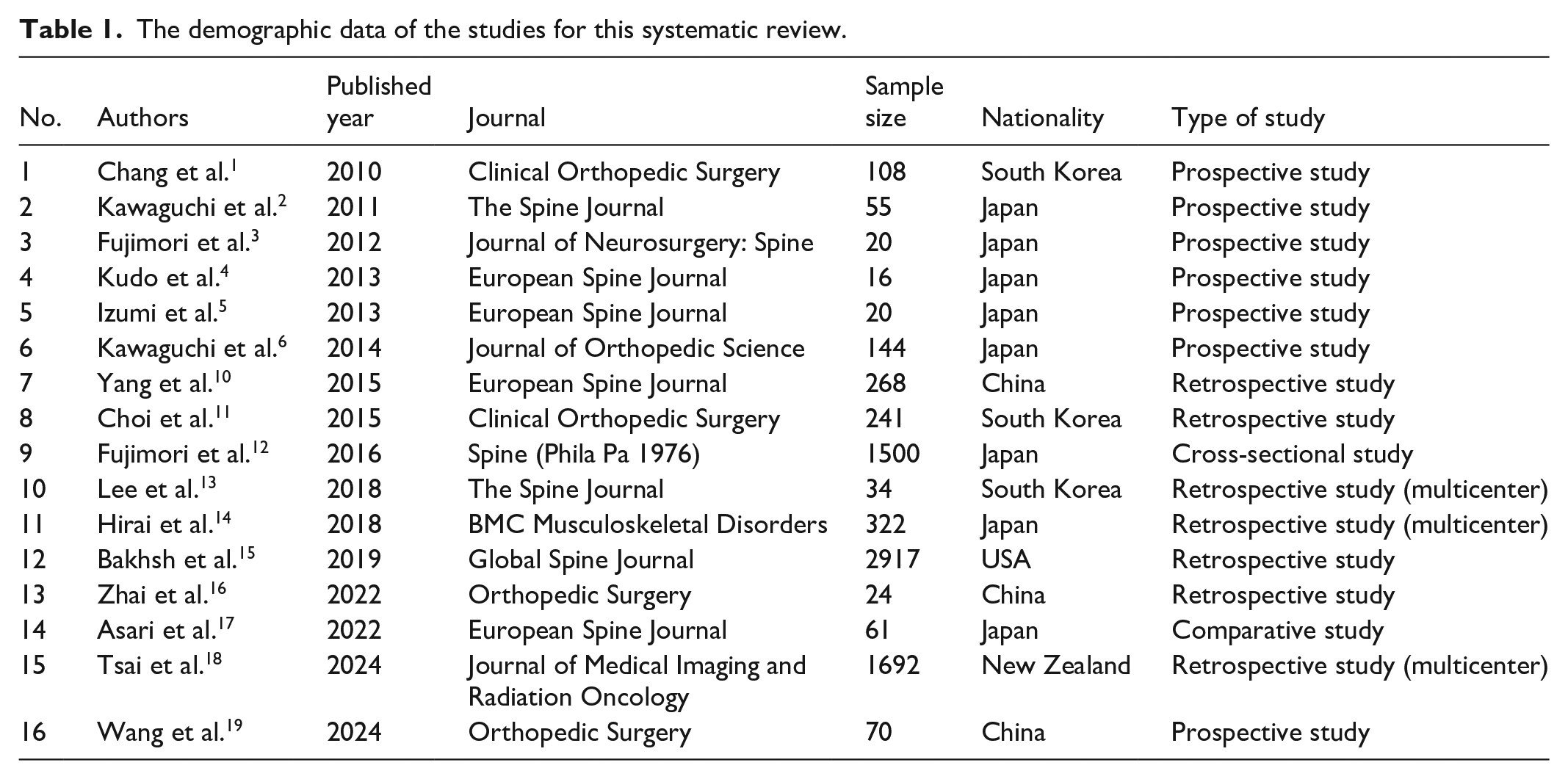
The demographic data of this systematic review
This systematic review included 16 studies focusing on the advancements in CT imaging-based classification systems for cervical OPLL and their implications for surgical strategies. The studies were conducted across various countries, with a majority from Asia, particularly Japan and South Korea. The study designs included prospective case studies, retrospective reviews, and comparative analyses. The sample sizes ranged from 16 to 2917 patients, highlighting the study scope, and design diversity. The demographic data of the studies are included in this review (Table 1).
The demographic data of the studies for this systematic review.
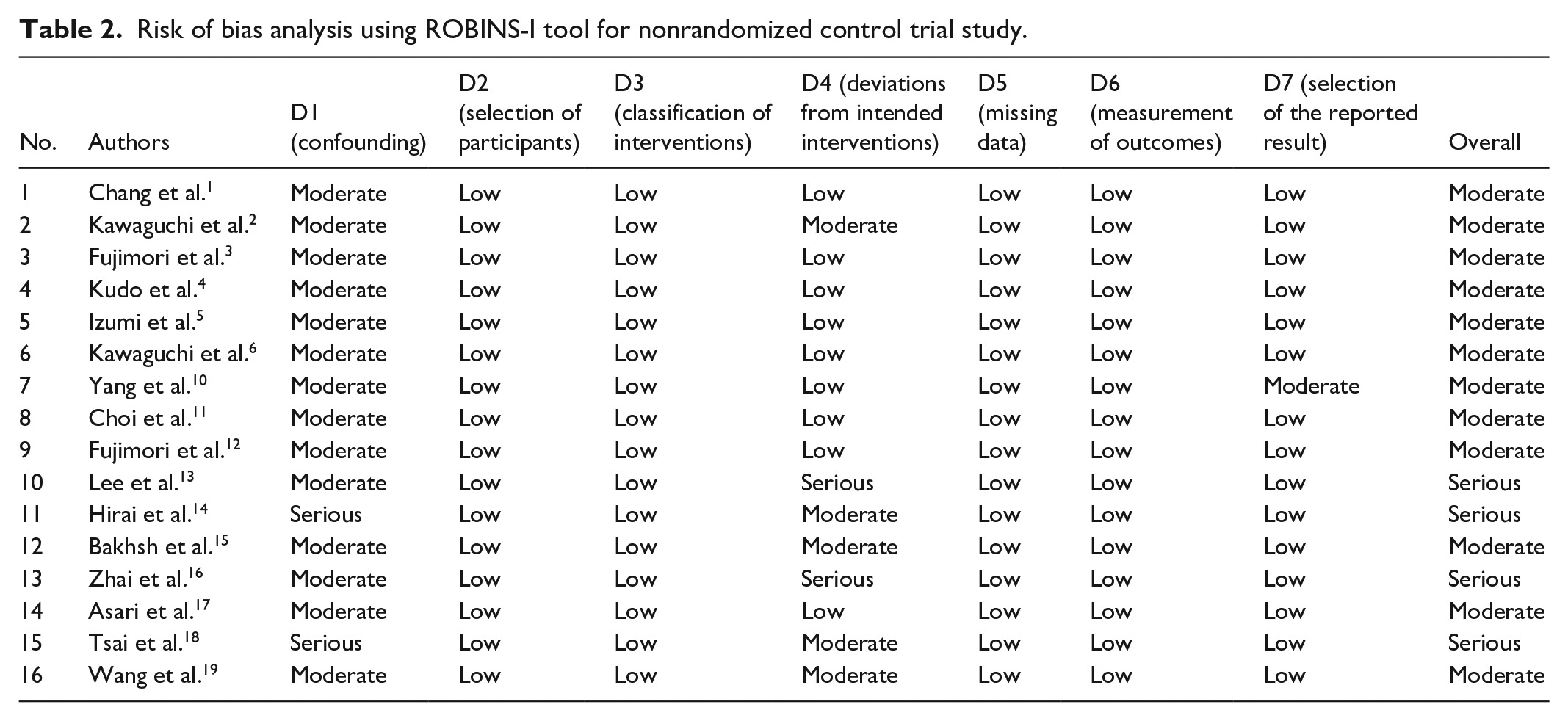
Risk of bias analysis
All 16 studies were nonrandomized studies. Therefore, risk of bias was evaluated and analyzed by the ROBINS-I tool. 8 The risk of bias analysis for the included studies revealed that the majority of studies, such as those by Chang et al., 1 Kawaguchi et al., 2 Fujimori et al., 3 Kudo et al., 4 Izumi et al., 5 Kawaguchi et al., 6 Yang et al., 10 Choi et al., 11 Fujimori et al., 12 Bakhsh et al., 15 Asari et al., 17 and Wang et al., 19 were found to have a moderate overall risk of bias. However, a few studies, including those by Lee et al., 13 Hirai et al., 14 Zhai et al., 16 and Tsai et al. 18 exhibited an overall severe risk of bias, primarily due to issues such as deviations from intended interventions or confounding factors. These findings underscore the need for careful interpretation of the results, especially in studies with a higher risk of bias (Table 2 and Figure 2).
Risk of bias analysis using ROBINS-I tool for nonrandomized control trial study.

Risk of bias summary for nonrandomized controlled trials, assessed using the risk of bias in nonrandomized studies of interventions ROBINS-I tool (Cochrane, London, UK).
Clinical practices of CT imaging and surgical strategies
The results of this systematic review included 16 studies that focused on various aspects of using CT imaging to classify, diagnose, and manage cervical OPLL. The studies assessed the reliability of different imaging modalities, the development and validation of classification systems, and the implications for surgical decision-making and outcomes (Table 3).
The summary of clinical practices of CT imaging and surgical strategies in cervical OPLL for this systematic review.
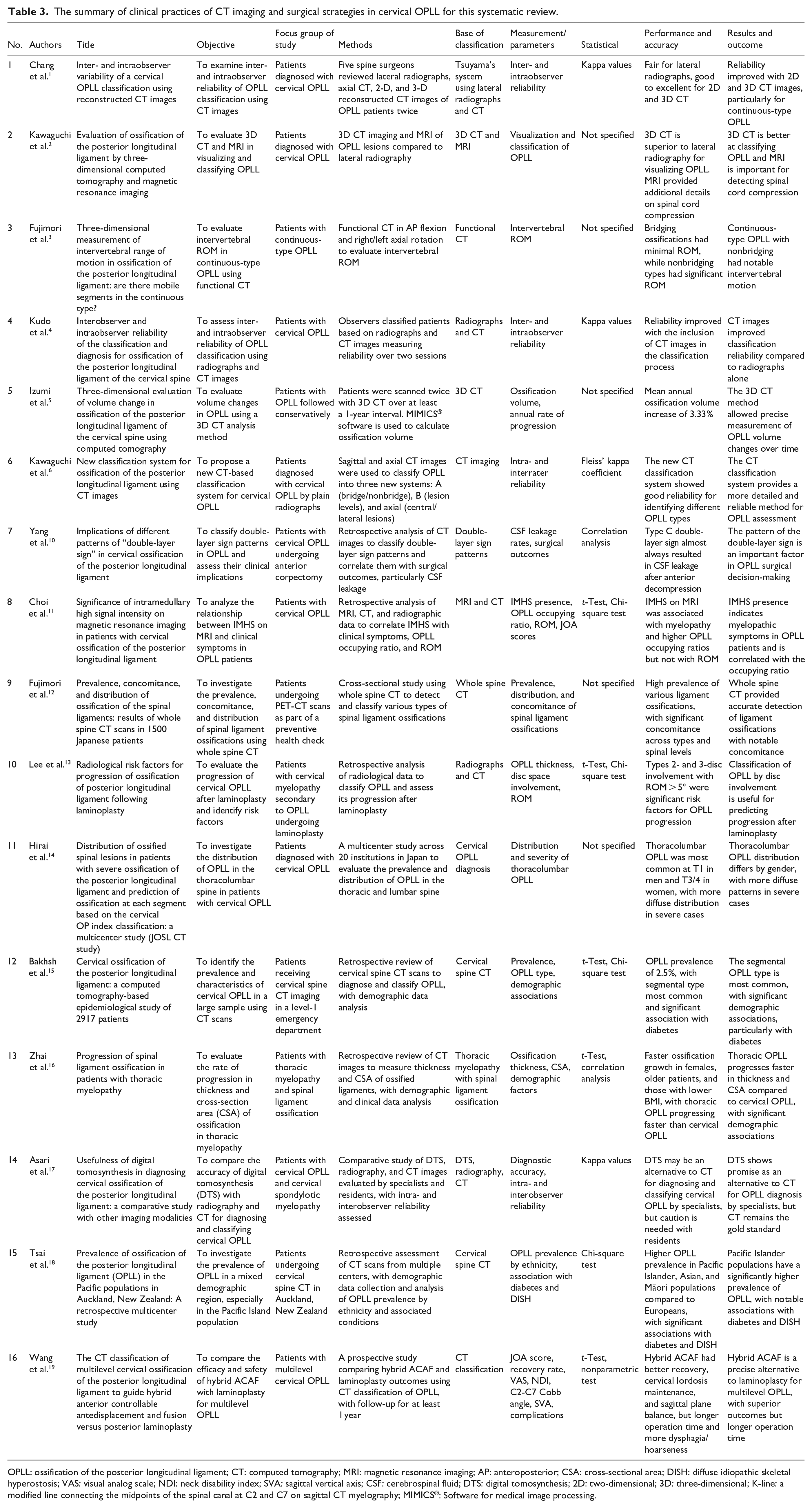
OPLL: ossification of the posterior longitudinal ligament; CT: computed tomography; MRI: magnetic resonance imaging; AP: anteroposterior; CSA: cross-sectional area; DISH: diffuse idiopathic skeletal hyperostosis; VAS: visual analog scale; NDI: neck disability index; SVA: sagittal vertical axis; CSF: cerebrospinal fluid; DTS: digital tomosynthesis; 2D: two-dimensional; 3D: three-dimensional; K-line: a modified line connecting the midpoints of the spinal canal at C2 and C7 on sagittal CT myelography; MIMICS®: Software for medical image processing.
Inter- and intraobserver reliability
Chang et al. 1 examined the inter- and intraobserver reliability of OPLL classification using different imaging techniques. The study found that while lateral radiographs showed fair reliability, the use of 2D and 3D CT significantly improved reliability, particularly for continuous-type OPLL. Similarly, Kudo et al. 4 reported that including CT images enhanced the reliability of OPLL classification compared to radiographs alone.
Classification and visualization
Both of Kawaguchi et al.2,6 studies reported the classification and visualization of OPLL using CT imaging. Kawaguchi et al. 2 highlighted the superiority of 3D CT over lateral radiography in visualizing OPLL and emphasized the importance of MRI in detecting spinal cord compression. Kawaguchi et al. 6 proposed a new CT-based classification system that demonstrated good reliability for identifying different OPLL types, offering a more detailed and accurate method for OPLL assessment.
Surgical decision-making
Several studies explored the impact of imaging and classification on surgical strategies. Yang et al. 10 classified different patterns of the “double-layer sign” in OPLL and found that certain patterns were strongly associated with cerebrospinal fluid (CSF) leakage after anterior decompression surgery. These findings suggest that the “Double-Layer Sign” is a crucial factor in surgical decision-making. Wang et al. 19 compared the outcomes of Hybrid anterior controllable antedisplacement and fusion (ACAF) and laminoplasty in patients with multilevel cervical OPLL, finding that Hybrid ACAF provided better recovery and maintenance of cervical lordosis and sagittal plane balance, albeit with longer operation times and higher rates of dysphagia and hoarseness.
Progression and risk factors
Studies by Lee et al. 13 and Zhai et al. 16 examined the progression of cervical OPLL and its associated risk factors. Lee et al. 13 identified that disc involvement and segmental range of motion (ROM) were significant risk factors for cervical OPLL progression after laminoplasty. Zhai et al. 16 found that thoracic OPLL progressed faster in thickness and cross-sectional area (CSA) compared to cervical OPLL, with notable demographic associations, such as age, gender, and BMI.
Epidemiology and prevalence
The prevalence and characteristics of cervical OPLL in various populations were studied by Fujimori et al., 12 Bakhsh et al., 15 and Tsai et al. 18 Fujimori et al. 12 reported a high prevalence and significant concomitance of various ligament ossifications in Japanese patients. Bakhsh et al. 15 observed a prevalence of 2.5% in a large cohort of patients in the USA, with the segmental type being most common and significantly associated with diabetes. Tsai and Doyle 18 found that the Pacific Islander population in Auckland, New Zealand, had a significantly higher prevalence of cervical OPLL, with strong associations with diabetes and diffuse idiopathic skeletal hyperostosis (DISH).
Discussion
CT imaging has emerged as the preferred modality due to its ability to provide high-resolution assessments of ossified lesions, leading to enhanced classification accuracy and surgical planning. Recent advances in CT-based classification systems have significantly impacted on surgical decision-making. Particularly, ACAF and laminoplasty strategies have been influenced by CT-based classifications, improving surgical outcomes. This systematic review aims to synthesize current literature regarding CT imaging-based classification systems for cervical OPLL, discussing their clinical implications and surgical strategies. According to the studies reviewed, it is evident that while traditional radiographic methods provide some insights into cervical OPLL, they often fall short of capturing the complexity and variability of the ossified lesions. The introduction and validation of 2D and 3D CT imaging has addressed these limitations, offering clinicians a more nuanced understanding of cervical OPLL morphology, which is crucial for diagnosis and surgical planning. One of the significant contributions of this review is the emphasis on the reliability of cervical OPLL classification systems when enhanced by CT imaging. Studies such as those by Chang et al. 1 and Kudo et al. 4 demonstrated that the inter- and intraobserver reliability significantly improves with CT imaging compared to lateral radiographs alone. This improvement is particularly noteworthy for continuous-type OPLL, where traditional imaging modalities often struggle to provide consistent and reliable results. These findings highlight the necessity of incorporating CT imaging into routine clinical practice for a more accurate and reproducible OPLL classification, which can ultimately guide better patient management.
Integrated findings and comparative analysis across studies that are one of the key strengths of this systematic review. While each study individually assessed different aspects of CT imaging in OPLL, a consistent trend emerged wherein CT-based classifications led to improved inter- and intraobserver reliability. For instance, Chang et al. 1 and Kudo et al. 4 demonstrated enhanced classification reliability with 3D CT compared to lateral radiographs. Similarly, Kawaguchi et al. 6 proposed a CT-based classification system that better characterized different OPLL types, improving clinical decision-making. These findings emphasize the importance of integrating multiple study outcomes to provide a holistic understanding of CT imaging’s role in OPLL management.
The development of new classification systems based on CT imaging, as proposed by Kawaguchi et al.,2,6 further illustrates the potential of CT imaging in refining our understanding of cervical OPLL. These classification systems not only offer a more detailed characterization of the lesion but also provide a framework for assessing the severity and progression of the disease. This level of detail is indispensable for tailoring surgical interventions to individual patient needs, which is critical given the varying patterns and clinical implications of cervical OPLL.
Impact of CT imaging on surgical decision-making are critical gap in previous reviews was the explicit discussion of how CT imaging classification directly influences surgical approaches, such as ACAF. In this review, we address this issue by integrating findings from Yang et al. 10 and Wang et al., 19 which revealed that certain CT-based classifications correlate with CSF leakage risks in anterior decompression surgeries. Surgical decision-making is another area where CT imaging has been shown to be particularly beneficial.1,20 The classification of double-layer signs by Yang et al. 10 is a prime example of how CT imaging can inform surgical approaches, particularly in predicting the risk of complications such as CSF leakage. This predictive capability underscores the importance of detailed preoperative imaging in optimizing surgical outcomes and minimizing complications. This highlights the necessity of preoperative CT assessments in selecting the most appropriate surgical approach.
Risk factor of cervical OPLL of this review also sheds light on the progression of cervical OPLL and the factors that influence its development. Studies by Lee et al. 13 and Zhai et al. 16 suggest that factors such as disc involvement, ROM, and demographic variables like age, gender, and BMI play significant roles in the progression of cervical OPLL. The ability to identify these risk factors through detailed imaging and classification allows for more proactive management strategies, potentially slowing the progression of the disease and improving long-term outcomes.
Epidemiological insights and prevalence studies that strengthen the epidemiological aspect of OPLL, we have now included Singh et al., 21 which reported the prevalence and demographic associations of OPLL based on 2500 CT scans. Their findings contribute to a broader understanding of regional variations and associated comorbidities, such as diabetes and DISH. Moreover, the epidemiological studies included in this review, such as those by Fujimori et al.3,12 and Tsai and Doyle, 18 highlight the varying prevalence of OPLL across different populations and the associated demographic and health factors, such as diabetes and DISH. These findings contribute to a broader understanding of cervical OPLL and emphasize the need for targeted screening and management strategies in populations at higher risk. This addition improves the review’s comprehensiveness in discussing both diagnostic and prevalence aspects of CT imaging. We comprehensively summarize advancements in CT imaging, surgical strategy, and decision-making for cervical OPLL in Table 4.
A comprehensive summary of advancements in CT imaging to manage cervical OPLL.
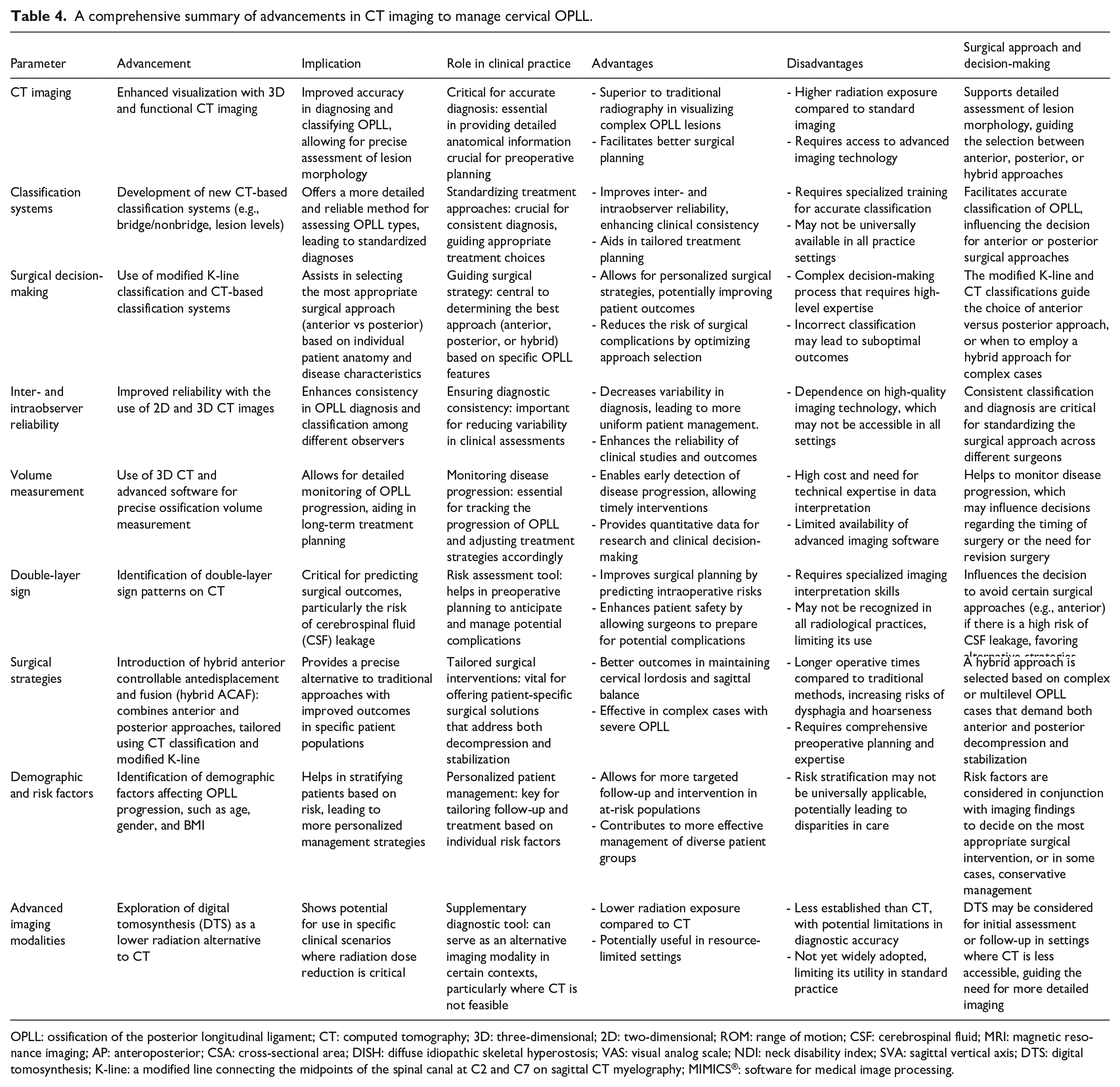
OPLL: ossification of the posterior longitudinal ligament; CT: computed tomography; 3D: three-dimensional; 2D: two-dimensional; ROM: range of motion; CSF: cerebrospinal fluid; MRI: magnetic resonance imaging; AP: anteroposterior; CSA: cross-sectional area; DISH: diffuse idiopathic skeletal hyperostosis; VAS: visual analog scale; NDI: neck disability index; SVA: sagittal vertical axis; DTS: digital tomosynthesis; K-line: a modified line connecting the midpoints of the spinal canal at C2 and C7 on sagittal CT myelography; MIMICS®: software for medical image processing.
This study’s limitation is its reliance on imaging modalities, particularly CT scans, as the primary diagnostic tool for cervical OPLL classification and surgical planning. While CT imaging offers enhanced accuracy and reliability, it also exposes patients to higher radiation levels than other imaging techniques, such as MRI. The potential risks associated with repeated radiation exposure, especially in populations requiring frequent imaging, are a concern that warrants careful consideration. Furthermore, this review primarily focuses on studies that used CT imaging to classify and manage cervical OPLL, which may have excluded relevant studies utilizing other imaging modalities or approaches. As a result, the conclusions drawn may not fully encompass the broader spectrum of diagnostic and treatment strategies available for cervical OPLL. Finally, the review is limited by potential bias as studies with negative or nonsignificant findings are less likely to be published and, consequently, included in the analysis. This bias can skew the overall interpretation of the effectiveness and reliability of CT scan in managing cervical OPLL. Lastly, future studies should investigate the cost-effectiveness of different imaging and treatment strategies for OPLL. As healthcare resources are finite, understanding the economic implications of various approaches is essential for ensuring that the most effective and efficient strategies are adopted in clinical practice.
Conclusion
This systematic review highlights the transformative impact of CT imaging in the diagnosis, classification, and surgical management of cervical OPLL. The integration of study findings reinforces the advantages of CT-based classifications in guiding surgical decision-making. Additionally, epidemiological insights provide a broader understanding of OPLL prevalence and risk factors. However, the limitations of CT imaging, including radiation exposure and cost, must be considered when implementing it as a primary diagnostic tool. Future research should focus on refining classification systems, integrating multimodal imaging approaches, and evaluating the cost-effectiveness of different imaging strategies to optimize patient outcomes.