
Abstract
Study Design
Retrospective cohort study.
Objectives
The risk factors for proximal junctional kyphosis (PJK) in adult spinal deformity (ASD) are well established, but their association with onset timing remains unclear. This study aims to identify distinct risk factors for early-onset and late-onset PJK.
Methods
This study included 96 ASD patients who underwent corrective surgery (fusion ≥5 levels, UIV: T1–L1, LIV: L5/S1) with ≥2 years of follow-up. Patients were categorized into Non-PJK, Early-Onset PJK (≤6 months), and Late-Onset PJK (>6 months) groups. Clinical characteristics were compared to identify potential risk factors (P < .10). Multinomial logistic regression was used to evaluate the independent effects of these variables on early-onset and late-onset PJK.
Results
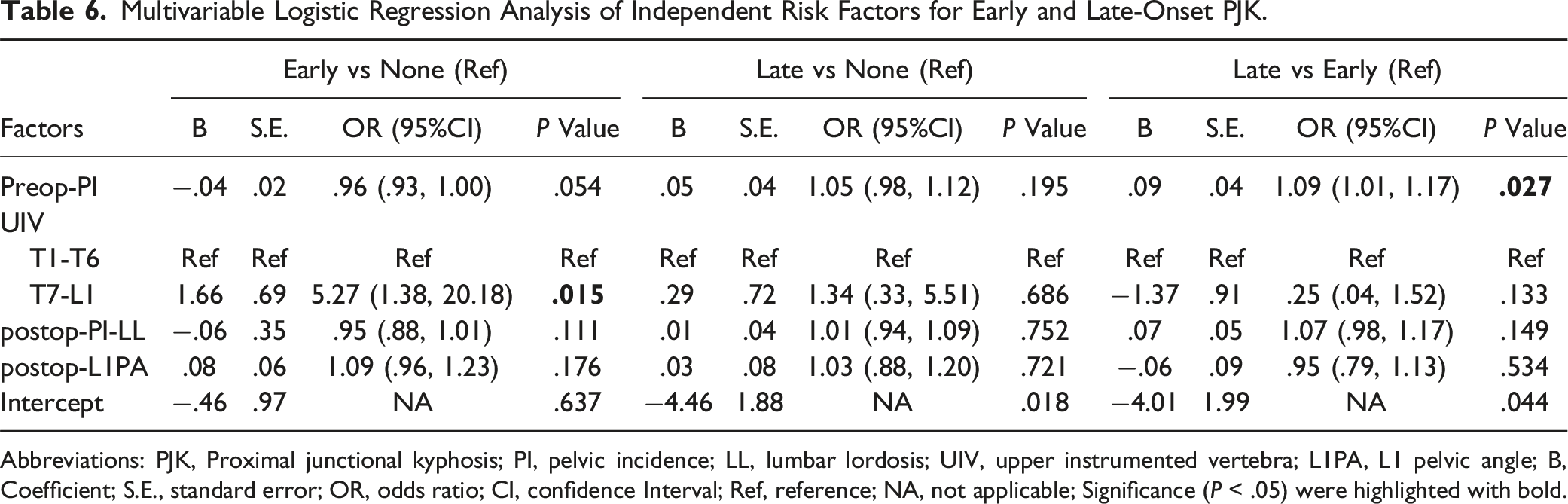
Among 96 patients, 44 (45.8%) developed PJK (31 early-onset, 13 late-onset), and 7 (7.3%) developed PJF, including 6 cases in the Early-Onset group (19.4%, P = .005). After initial screening and addressing multicollinearity, preoperative PI, UIV location, and postoperative PI-LL and L1PA were finally included in regression analysis. Lower thoracic UIV (T7–L1) increased the risk of Early-Onset PJK (OR = 5.27, P = .015). Higher preoperative PI was associated with Late-Onset PJK, with a 9% increased risk per degree (OR = 1.09, P = .027).
Conclusions
Most PJK cases occur within 6 months and have a higher risk of PJF. Lower thoracic UIV increases Early-Onset PJK risk, while higher preoperative PI predisposes to Late-Onset PJK. Strategies should focus on preventing Early-Onset PJK in lower thoracic UIV cases and long-term monitoring for Late-Onset PJK in high-PI patients.
Introduction
Proximal junctional kyphosis (PJK) is one of the most common mechanical complications after long segment spinal fusion for adult spinal deformity (ASD). 1 It can lead to adverse clinical consequences, including functional impairment,2,3 reduced quality of life,4,5 and the potential need for revision surgery. 6 Identifying risk factors for PJK is important for targeted management, reducing its incidence and improving patient outcomes. Recently, a variety of PJK risk factors have been widely identified, broadly categorized into demographic, tissue-related, and mechanical factors.7,8 While these factors provide valuable insights into the overall risk of developing PJK, they fail to explain the differences in the timing of PJK onset among patients.
Among ASD patients who develop PJK, some experience it within 6 months postoperatively (early-onset), while others may develop it for years (late-onset). 9 Elucidating distinct risk factors for early- and late-onset PJK, relative to non-PJK, provides a basis for improving clinical decision-making. Specifically, for those at higher risk of early-onset PJK, targeted interventions (such as reinforcing postoperative bracing, optimizing alignment intraoperatively, or initiating early rehabilitation) may be considered during the immediate postoperative period. In contrast, patients at risk for late-onset PJK may benefit from extended follow-up schedules, long-term radiographic surveillance, and interventions aimed at maintaining spinal stability and muscular function over time. However, few studies to date have systematically investigated the distinct risk factors associated with early-onset and late-onset PJK.
This study aims to address this understudied area by identifying and comparing the distinct risk factors for early-onset and late-onset PJK in ASD patients. The findings could serve as a foundation for personalized postoperative care strategies, ultimately improving patient outcomes.
Methods
Patient Sample
This retrospective study included patients diagnosed with ASD who underwent corrective surgery at our institution between May 2013 and September 2022, with a minimum follow-up period of 2 years. Surgical parameters included a fusion segment of ≥5 levels, an upper instrumented vertebra (UIV) ranging from T1 to L1, and a lower instrumented vertebra (LIV) at L5 or S1. All patients received instrumentation with 2 screws per vertebral level, and the correction goals were determined according to age-adjusted PI–LL targets.6,7 Regarding rehabilitation protocols, all patients participated in physical therapy twice daily starting on postoperative day 1 (POD1). Patients were excluded from the database if: (1) their spinal deformities were attributable to neuromuscular conditions, post-traumatic events, neoplastic processes, rheumatologic diseases, and/or infectious etiologies; (2) they underwent revision surgery for any reason after correction surgery; (3) Follow-up less than 2 years; (4) missing any of the required demographic, tissue-related, or mechanical data.
Data Collection
Clinical characteristics, including the demographic, tissue-related, and mechanical factors, were collected for analysis.
Demographic Factors
Demographic data and comorbidities were retrospectively retrieved from electronic medical records. These included age, gender, body mass index (BMI), smoking status, and the presence of conditions such as diabetes, hypertension, osteoporosis, dyslipidemia, coronary artery disease, peripheral neuropathy, autoimmune diseases, and anxiety.
Tissue-Related Factors
The cross-sectional area (CSA) of the psoas, paralumbar muscles (erector spinae and multifidus), and the L4 vertebral body were measured using a single T2-weighted MRI axial slice at the level of the L4 pedicles.10,11 The psoas vertebral body index (PVBI) and paralumbar vertebral body index (PLVBI) were both calculated by dividing the sum of the left and right muscle CSA (psoas or paralumbar, respectively) by the CSA of the L4 vertebral body. PVBI and PLVBI were chosen as representatives of muscle quantity for subsequent analysis.
Mechanical Factors
Mechanical factors were obtained from surgical records and radiographic images conducted preoperatively and at discharge.
Preoperative and postoperative spinopelvic parameters were assessed using standing lateral and posteroanterior (PA) full-length radiographs. These parameters included: (1) Proximal Junctional Angle (PJA); (2) maximum Cobb angle, (3) thoracic kyphosis (TK; T4-T12), (4) lumbar lordosis (LL; L1-S1), (5) sacral slope (SS), (6) pelvic incidence (PI), (7) pelvic tilt (PT), (8) PI-LL mismatch, (9) sagittal vertical axis (SVA), (10) L1 pelvic angle (L1PA), (11) T4 pelvic angle (T4PA), (12) L1PA deviation (L1PA – normal L1PA, where normal L1PA is defined as 0.5 × PI – 21° 12 ), and (13) T4-L1PA mismatch (T4PA – L1PA).
Intraoperative factors included the upper instrumented vertebra (UIV), categorized as either the upper thoracic region (T1–T6) or the lower thoracic region (T7–L1), based on the most widely accepted criteria13-18; the lower instrumented vertebra (LIV), defined as either L5 or S1; and the configuration of upper instrumented level instrumentation, involving hooks, screws, or a combination of both. Besides, the extent of PI-LL correction was calculated using the formula: (age-adjusted ideal PI - LL) - (discharge PI - LL).19,20 Patients were classified into 3 types based on the extent of correction: undercorrection (<−10°), ideal correction (−10° to 10°), and overcorrection (>10°).
In addition, we calculated the change in spinal alignment (postoperative minus preoperative) for the following parameters: Max Cobb angle, PI–LL mismatch, PT, L1PA offset, and T4–L1PA mismatch.
Statistical Analysis
PJK was defined based on the following criteria: a proximal junction angle (PJA) of ≥10° with an increase of ≥10° compared to the preoperative measurement. 21 Patients were categorized into Non-PJK, Early-Onset PJK (≤6 months), and Late-Onset PJK (>6 months) groups. Proximal junctional failure (PJF) was defined as a proximal junctional angle (PJA) of ≥28°, an increase of ≥22° from the preoperative measurement, or the need for revision surgery due to PJK. Intraoperative complications included anesthesia-related events, neurologic injury, dural tears, blood loss >4 liters, vascular, or visceral injuries. Postoperative complications were classified as surgical (implant-related, radiographic, neurologic, or wound problems) or medical (cardiopulmonary, central nervous system, gastrointestinal, musculoskeletal, renal disorders, or infections unrelated to the spine).
The Kolmogorov-Smirnov test was used to assess the normality of distributions for samples larger than 50, while the Shapiro-Wilk test was applied for samples of 50 or fewer. Continuous variables were reported as mean and standard deviation (SD) or median and interquartile range (IQR), depending on the data distribution.
ANOVA, the Kruskal-Wallis test, Fisher’s exact test, and Chi-square tests were performed to evaluate differences in clinical characteristics among the 3 groups and to identify potential risk factors (P < .10). Post hoc analysis was conducted using the Bonferroni test and Mann–Whitney test. Multicollinearity among independent variables was assessed using the Pearson correlation analysis (also includes Point-Biserial correlations for dichotomous variables) and the variance inflation factor (VIF), with correlation coefficients between variable pairs >0.7 or VIF >10 indicating the presence of multicollinearity.22,23 Multinomial logistic regression was performed to assess the independent effects of selected potential risk factors on the development of Early-Onset and Late-Onset PJK. All statistical analyses were carried out using IBM SPSS Statistics (version 22.0; IBM). A P value of < .05 was considered statistically significant in all analyses, except potential risk factors identification.
Results
Clinical Data
Clinical Characteristics for the 96 Patients With Adult Spinal Deformity.
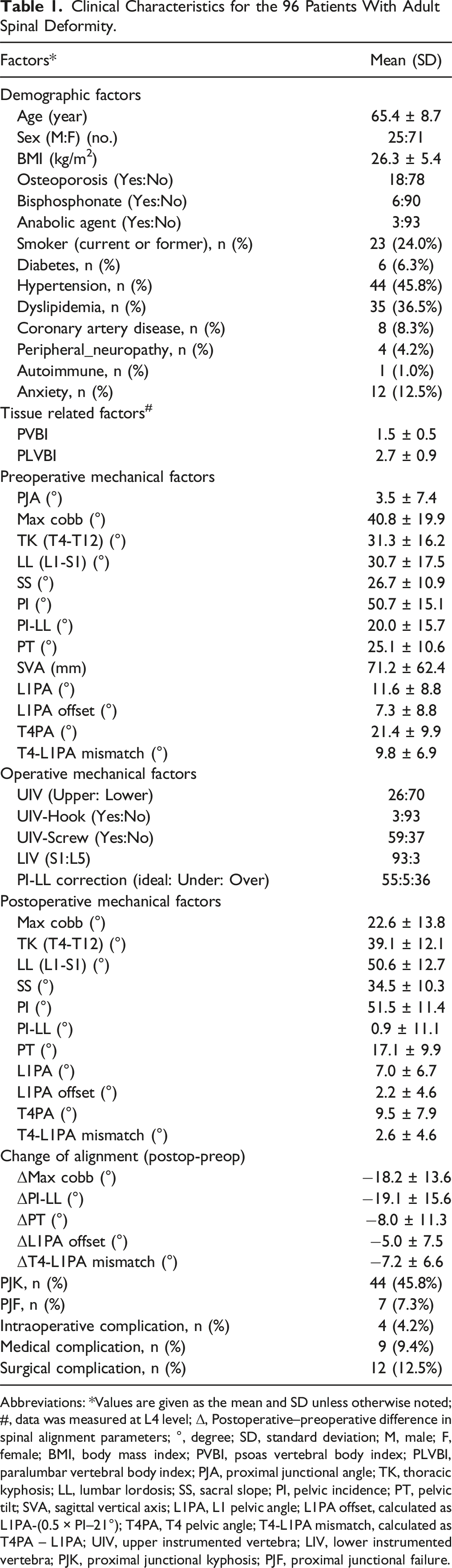
Abbreviations: *Values are given as the mean and SD unless otherwise noted; #, data was measured at L4 level; Δ, Postoperative–preoperative difference in spinal alignment parameters; °, degree; SD, standard deviation; M, male; F, female; BMI, body mass index; PVBI, psoas vertebral body index; PLVBI, paralumbar vertebral body index; PJA, proximal junctional angle; TK, thoracic kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt; SVA, sagittal vertical axis; L1PA, L1 pelvic angle; L1PA offset, calculated as L1PA-(0.5 × PI–21°); T4PA, T4 pelvic angle; T4-L1PA mismatch, calculated as T4PA – L1PA; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra; PJK, proximal junctional kyphosis; PJF, proximal junctional failure.
Comparisons of Clinical Characteristics and Complications Among None, Early, and Late-Onset PJK Groups.
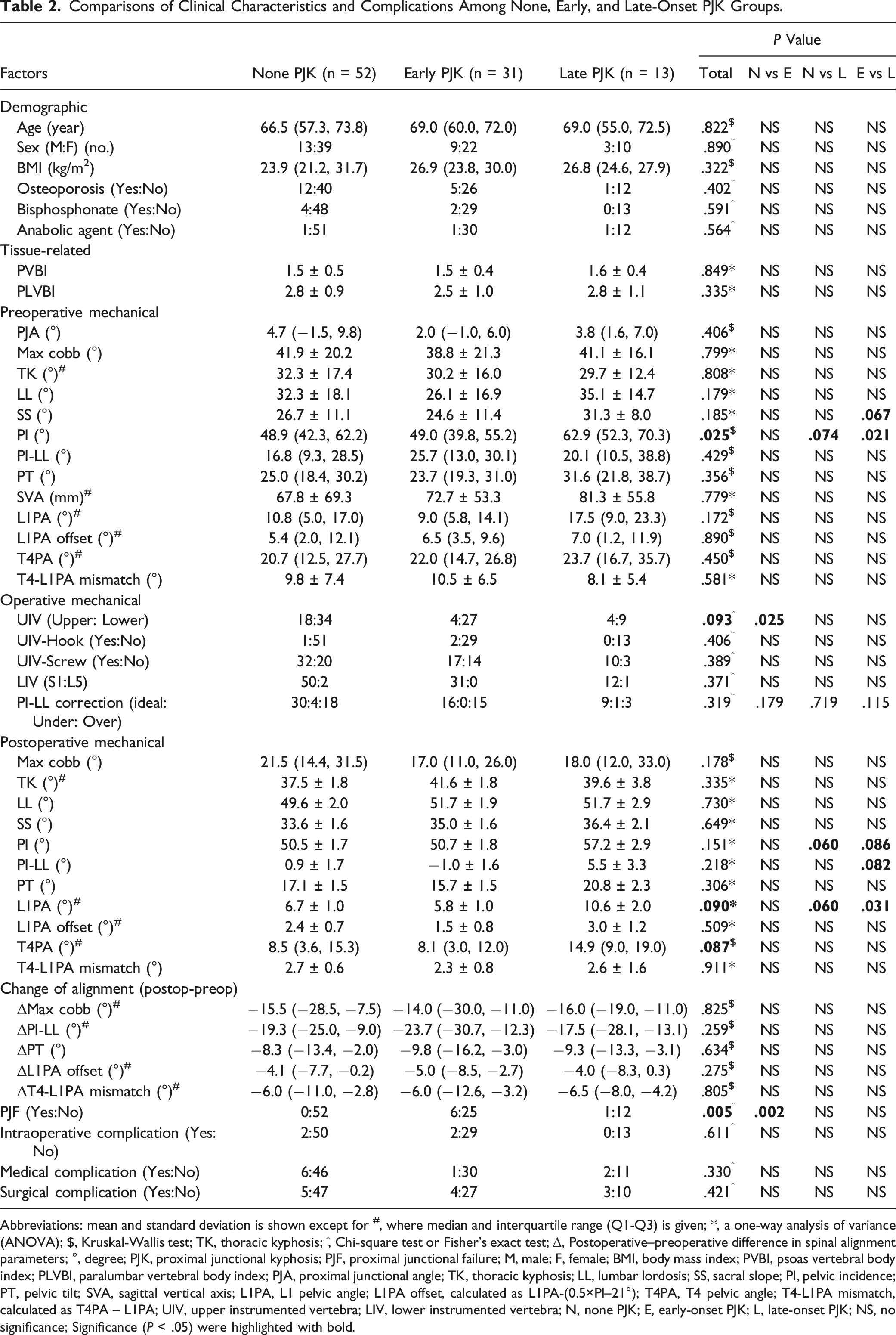
Abbreviations: mean and standard deviation is shown except for #, where median and interquartile range (Q1-Q3) is given; *, a one-way analysis of variance (ANOVA); $, Kruskal-Wallis test; TK, thoracic kyphosis; ^, Chi-square test or Fisher’s exact test; Δ, Postoperative–preoperative difference in spinal alignment parameters; °, degree; PJK, proximal junctional kyphosis; PJF, proximal junctional failure; M, male; F, female; BMI, body mass index; PVBI, psoas vertebral body index; PLVBI, paralumbar vertebral body index; PJA, proximal junctional angle; TK, thoracic kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt; SVA, sagittal vertical axis; L1PA, L1 pelvic angle; L1PA offset, calculated as L1PA-(0.5×PI–21°); T4PA, T4 pelvic angle; T4-L1PA mismatch, calculated as T4PA – L1PA; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra; N, none PJK; E, early-onset PJK; L, late-onset PJK; NS, no significance; Significance (P < .05) were highlighted with bold.
Comparison of the Demographic, Tissue-Related, and Mechanical Factors Among Groups
As shown in Table 2, no significant differences were observed among the 3 groups in terms of demographic and tissue-related factors.
For mechanical factors, significant differences in preoperative PI were identified among the Non-PJK, Early-Onset PJK, and Late-Onset PJK groups (P = .025). Specifically, the median (IQR) PI was notably lower in the Non-PJK group (48.9 [42.3, 62.2]) and the Early-Onset PJK group (49.0 [39.8, 55.2]) compared to the Late-Onset PJK group (62.9 [52.3, 70.3]). Additionally, some radiographic factors such as preoperative SS, UIV, and postoperative PI, PI-LL, L1PA, and T4PA demonstrated trends of differences between at least 2 of the 3 groups (P < 0.10). There were no differences in the change of spinal alignment (postoperative minus preoperative) among the 3 groups.
Based on these observations, preoperative SS and PI, UIV, as well as postoperative PI, PI-LL, L1PA, and T4PA were initially selected as potential risk factors for further analysis.
Independent Influence of Risk Factors on Early-Onset and Late-Onset PJK
Multicollinearity Judgement Before Variable Elimination.
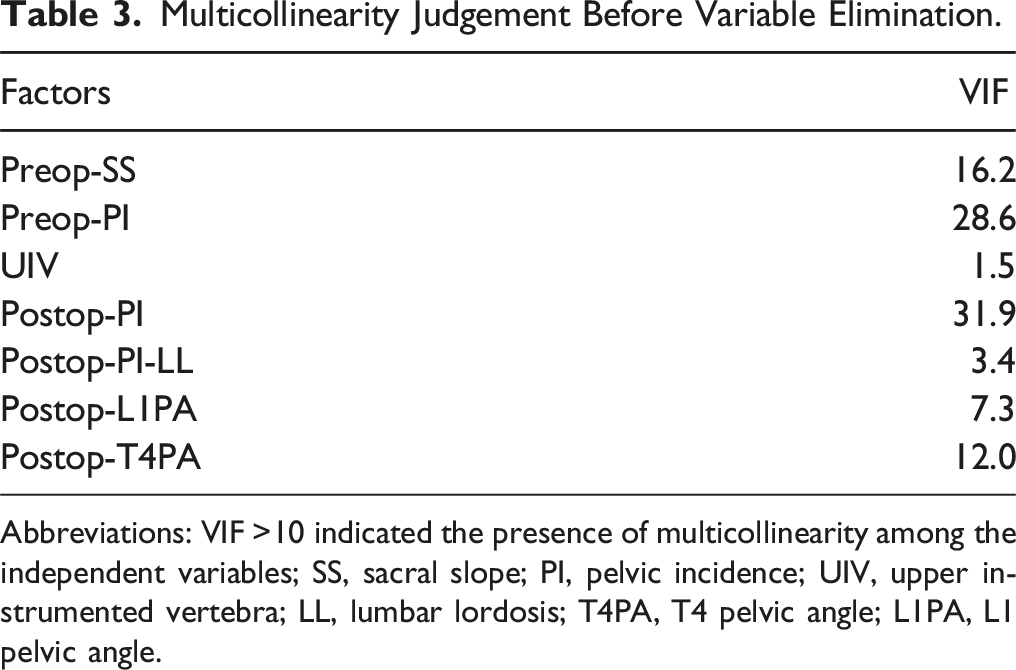
Abbreviations: VIF >10 indicated the presence of multicollinearity among the independent variables; SS, sacral slope; PI, pelvic incidence; UIV, upper instrumented vertebra; LL, lumbar lordosis; T4PA, T4 pelvic angle; L1PA, L1 pelvic angle.
Pearson or Point-Biserial Correlations of the Potential Risk Factors.
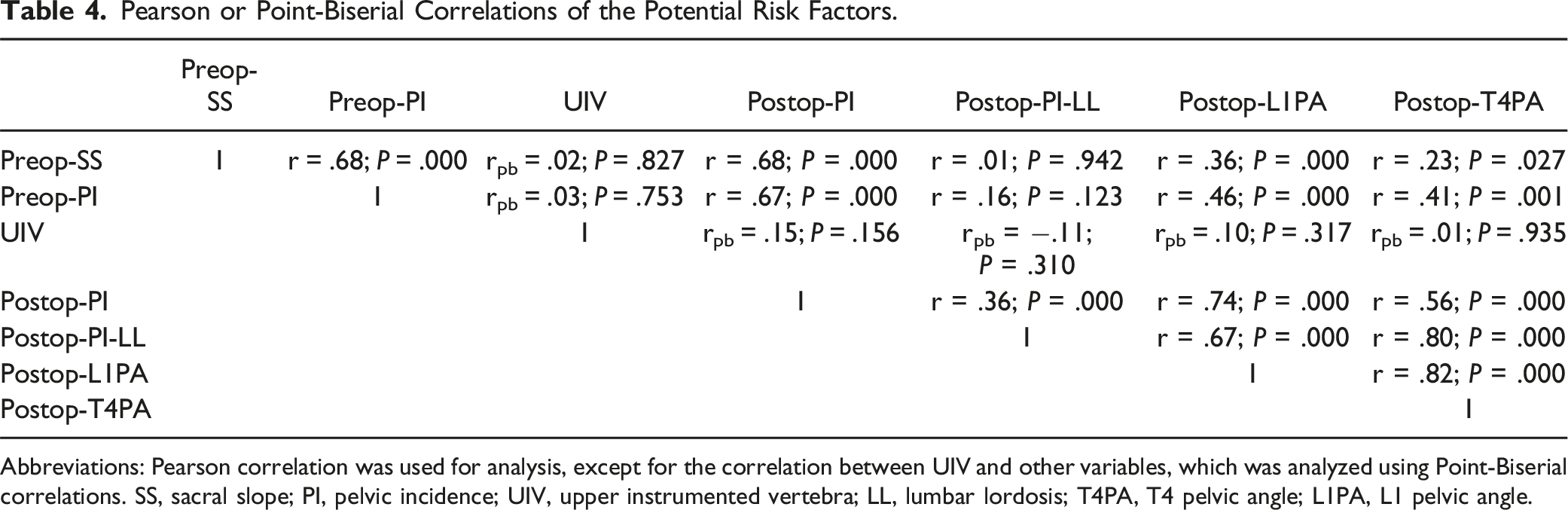
Abbreviations: Pearson correlation was used for analysis, except for the correlation between UIV and other variables, which was analyzed using Point-Biserial correlations. SS, sacral slope; PI, pelvic incidence; UIV, upper instrumented vertebra; LL, lumbar lordosis; T4PA, T4 pelvic angle; L1PA, L1 pelvic angle.
Clinically, PI is an inherent parameter determined by an individual’s pelvic anatomy 24 and remains constant regardless of surgical intervention, leading to strong collinearity between preoperative and postoperative PI. Preoperative SS is intrinsically correlated with PI, as larger PI values are typically associated with higher SS.24,25 Additionally, T4PA reflects standing global sagittal alignment but overlaps substantially with L1PA and PI-LL. 12 Based on these considerations, preoperative PI was retained because it is an individually anatomic constant, while other variables with VIF >10, including preoperative SS, postoperative PI, and postoperative T4PA, were excluded to reduce collinearity and redundancy.
Multicollinearity Judgement After Variable Elimination.
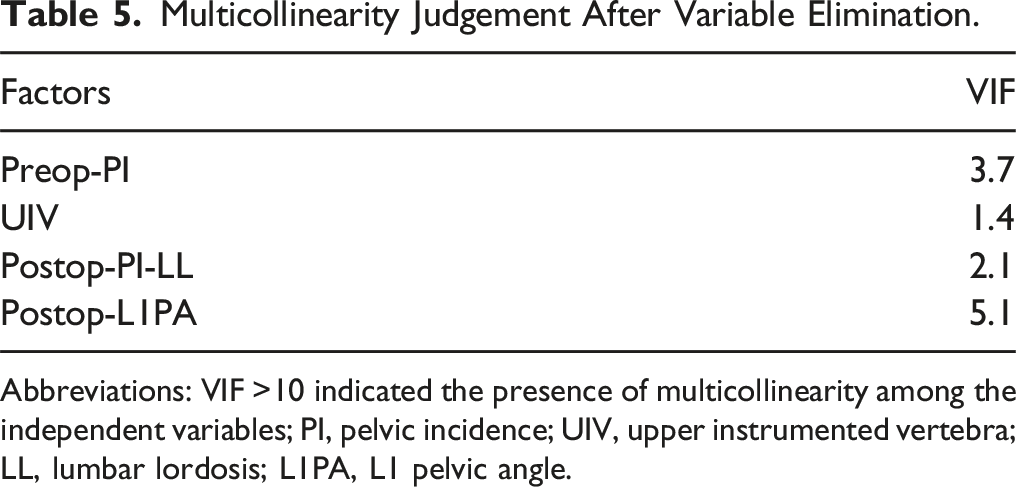
Abbreviations: VIF >10 indicated the presence of multicollinearity among the independent variables; PI, pelvic incidence; UIV, upper instrumented vertebra; LL, lumbar lordosis; L1PA, L1 pelvic angle.
Multivariable Logistic Regression Analysis of Independent Risk Factors for Early and Late-Onset PJK.
Abbreviations: PJK, Proximal junctional kyphosis; PI, pelvic incidence; LL, lumbar lordosis; UIV, upper instrumented vertebra; L1PA, L1 pelvic angle; B, Coefficient; S.E., standard error; OR, odds ratio; CI, confidence Interval; Ref, reference; NA, not applicable; Significance (P < .05) were highlighted with bold.
Discussions
To our knowledge, few studies have specifically investigated the distinct risk factors associated with early-onset and late-onset PJK. In this study, our findings demonstrate that the location of the UIV in the lower thoracic region is an independent risk factor for Early-Onset PJK or PJF at any time, while higher preoperative PI increases the risk of Late-Onset PJK.
PJK is among the most common mechanical complication following long-segment spinal fusion for ASD. 1 In our study, with a minimum follow-up of 2 years, we observed a PJK incidence rate of 45.8%, which is consistent closely with previously reported rates of approximately 40%.8,26 In addition, the majority of PJK cases occurred within 6 months after surgery, with Early-Onset PJK accounting for 31 out of the 44 cases (70.5%). This finding supports prior observations that PJK frequently manifests shortly after surgery, with approximately 66% of cases identified within 3 months postoperatively. 3 Notably, the incidence of PJF was significantly higher in patients with Early-Onset PJK compared to those in the other groups (Table 2). This might suggest that early-onset PJK is more likely to progress to PJF, while late-onset PJK represents radiographic finding that does not necessarily progress to a severe clinical complication.
The timing of PJK onset might have different clinical implications due to variations in pathogenesis and contributing factors. Early-Onset PJK is a more acute problem that may require intervention, as it often indicates an underlying structural issue that the body cannot immediately compensate for. In contrast, we hypothesize that late PJK typically arises from gradual biomechanical changes and decompensation over time. Thus, identifying the distinct risk factors for early- and late-onset PJK is crucial for optimizing patient-specific management strategies. A prior study defined Early-Onset PJK as occurring within 1-2 months postoperatively and compared patients with and without PJK at this time point. 27 Their findings associated Early-Onset PJK with older age, hypolordosis, and increased T1PA. In contrast, our study defined Early-Onset PJK as occurring within 6 months postoperatively, based on previous research. 9 Additionally, the grouping criteria was different. The prior study classified patients without PJK at 1-2 months as Non-PJK, even though some may have developed PJK later in the follow-up period. In our study, only patients who remained free of PJK throughout a minimum 2-year follow-up were categorized as Non-PJK. This distinction prevents direct comparisons between our study and the previous study.
For long-segment fusion surgery in ASD, the incidence rates of PJK in the upper vs lower thoracic regions remain a topic of debate. A meta-analysis included these controversial studies and demonstrated significantly higher PJK rates in the lower thoracic regions compared to the upper thoracic regions. 28 However, it did not take the timing of PJK onset into account. Notably, our findings further clarify this distinction, as we identified that UIV in the lower thoracic region was independently associated with a higher likelihood of Early-Onset PJK, but not Late-Onset PJK (Table 6). Supporting our findings, studies also observed that acute proximal junctional failure (PJF), defined as occurring within approximately 6 months postoperatively, was significantly more frequent in the lower thoracic region.16,29,30 Although this study did not specifically analyze PJK incidence, it is clinically relevant because PJK is more likely to progress to PJF within the first 3 to 6 months postoperatively.31,32 A possible explanation for this association lies in biomechanical differences between the upper and lower thoracic regions. The rib cage and stronger posterior tension band in the upper thoracic spine provided better axial support and stability,33,34 thereby reducing stress at the junctional segment. In contrast, the lower thoracic spine lacks the stabilizing support provided by the rib cage. 34 Constructs terminating in this region experience immediate stress concentration after surgery, leading to rapid early-stage mechanical failure. Moreover, previous finite element analysis has indicated that the thoracolumbar spine undergoes significantly greater compressive loading than the upper thoracic spine. 35
On the contrary, larger preoperative PI was independently associated with a higher likelihood of Late-Onset PJK (Table 6). PI is a constant, individual-specific pelvic parameter that plays a crucial role in determining sagittal spinal alignment.36,37 A larger PI, particularly exceeding 50°, 38 has been widely reported to increase the risk of PJK.36,37 In our study, the median (IQR) PI in the Late-Onset group was 62.9 (52.3-70.3), significantly higher than that in both the Early-Onset and Non-PJK groups (Table 2). The potential mechanism through which high PI contributes to Late-Onset PJK likely involves prolonged biomechanical adaptations through reciprocal changes rather than acute postoperative changes. With restoration of lumbar lordosis, thoracic compensatory mechanisms can relax, leading to an initial reciprocal change. 38 Over time, these reciprocal changes may increase, and the thoracic arc adjusts to match the upper arc lumbar lordosis, which is physiologically higher in patients with high PI. 37 Over time, this kyphotic increase may manifest as “PJK”, though it may be physiologically representative of normal kyphosis in a high-PI patient. More refined definitions of “pathologic” vs “physiologic” kyphotic change are needed.
The impact of the extent of PI-LL correction on PJK occurrence remains controversial. Though we acknowledge the limitations of PI-LL in its inability to address the shape and distribution of lumbar alignment,12,39-41 we included it in this analysis compare to prior literature. Some studies have reported that overcorrection of LL relative to PI increases the incidence of PJK compared to ideal correction. 19 Others suggest that both overcorrection and undercorrection are linked to a higher frequency of PJK.42-44 However, some research indicates that overcorrection may yield favorable surgical outcomes, including a lower Oswestry Disability Index and reduced back pain, without necessarily increasing PJK prevalence. 21 In our study, a potential trend of difference was observed regarding the distribution of PI-LL correction (ideal: under: over) between the early-onset (16:0:15) and late-onset (9:1:3) PJK groups, respectively, although no statistical significance reached (P = .115) (Table 2). Specifically, the proportion of overcorrection was higher in the early-onset group compared to the late-onset group, and no undercorrection cases were noted in the early-onset group. Consistent with our findings, one previous study identified overcorrection of PI-LL as a significant risk factor for acute PJF. 45 Although the study focused on PJF rather than PJK, the tendency of early-onset PJK to progress to PJF provides potential support to our observations. We hypothesize that this difference may be attributed to heterogenous etiologies of PJK associated with overcorrection and undercorrection. Overcorrection may lead to early-onset PJK by imposing increased kyphotic stresses on the proximal junction due to abrupt anterior shift of the center of gravity of the proximal junction, 19 while undercorrection may contribute to PJK through a slower progression, as insufficient correction of LL leads to increased compensatory pelvic retroversion to maintain sagittal balance over time. 21 Finally, the differing results on PI-LL also support that this measure may be insufficient in evaluating spinal alignment as this parameter does not evaluate spinal shape. As surgical targets are refined, new alignment targets can be used to judge corrections. 12
Limitations
This study has several limitations. First, the retrospective design of this study carries a risk of sampling bias. Second, the late-onset PJK group was relatively small (n = 13), which limited the statistical power and may have prevented the detection of subtle risk factors. As a result, negative findings, such as BMI or osteoporosis, should be interpreted with caution, as they may not accurately reflect the absence of association. Third, although we identified distinct risk factors associated with Early-Onset and Late-Onset PJK, the limited number of these factors constrains us to further develop predictive models, such as ROC curve analyses.
Conclusion
In conclusion, this study highlights distinct risk factors for early-onset and late-onset PJK following long-segment spinal fusion in ASD patients. Specifically, a lower thoracic UIV location was independently associated with a higher risk of early-onset PJK, while higher preoperative PI significantly increased the likelihood of late-onset PJK. Individualized postoperative management strategies were recommended, including close monitoring of lower thoracic UIV patients for early-onset PJK and long-term follow-up for high PI patients to detect late-onset PJK. Future research should focus on developing risk probability prediction models for early-onset and late-onset PJK to enhance postoperative management.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Donghua Huang, Zhan Wang, Mihir Dekhne, Robert Uzzo, Atahan Durbas, Gabrielle Dykhouse, Tejas Subramanian, Andrea Pezzi, Luis Felipe Colon and Stephane Owusu-Sarpong declare no potential conflicts of interest with respects to research, authorship and/or publication of this article. Han Jo Kim has the following disclosures: Grant: ISSGF; Royalties: Zimmerbiomet, K2M Stryker, Acuity Surgical; Consulting: Nuvasive; Scientific Advisory Board/ Other Office, Vivex Biology, Aspen Medical; Fellowship Support: AO Spine. Francis Lovecchio has the following disclosures: Consultant: SeaSpine; Consultant: SI-Bone.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: However, data was collected and managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.
IRB Approval
This study protocol was conducted in accordance with the Declaration of Helsinki and received approval from the local institutional review board (Approval No: 2018-1599) with an exemption from requiring informed consent owing to the retrospective observational design of the study.