
Abstract
Study Design
Retrospective cohort.
Objective
Determine effects of bracing on proximal junctional kyphosis (PJK) after adult deformity correction.
Methods
Patients were identified from a single-surgeon dataset of posterior-only fusions for ASD (pelvis to UIV of T9-12) with a minimum of 1-year follow up. Starting in 2021, all lower thoracic fusions were braced using a hyperextension brace. Patients wore the brace at all times (unless in bed) for the first 6 weeks after surgery. A 1:1 propensity-match was performed based on age, number of levels, 3 column osteotomies, and magnitude of correction to identify a comparative non-braced cohort.
Results
141 patients (113 non-brace, 28 brace) were evaluated. After matching, 56 patients were identified to form similar cohorts. Non-matched and matched groups had no statistically significant differences in demographics, comorbid conditions, surgical characteristics (except shorter operative time and lower EBL in the braced group), and preoperative radiographic parameters. For the overall cohort, the change in proximal junctional angle at 1-year was higher in the non-braced group (7.6° vs 8.1°, P = .047), and non-braced patients had a higher incidence of PJK at 1-year in both the overall cohort (36% vs 14%, P = .045) and matched cohort (43% vs 14%, P = .038). There was no difference in proximal junctional failure between groups.
Conclusion
This pilot study shows that our protocol for extension bracing may reduce rates of PJK. These findings can form the basis for future multi-center trials examining the effect of extension bracing on junctional complications.
Introduction
Proximal junctional kyphosis (PJK) is a known mechanical complication of adult spinal deformity (ASD) surgery. Its incidence has been reported to be in the range of 17 to 62%, with about 1%–11% of patients requiring revision surgery because of symptoms.1–4 The etiology of PJK is multifactorial with the involvement of various surgical, radiographic, and patient factors. 5
Various techniques have been described for the prevention of PJK following ASD surgery. These include avoiding over- or under-correction, prophylactic vertebroplasty, junctional tethers, transverse process hooks, novel pedicle screw insertion techniques, reduced stiffness of the construct, and preoperative optimization of the bone density. 6 However, there is contrasting evidence on the efficacy of these techniques with no consensus on a definitive preventive method.
To date, only 3 studies have been conducted assessing the utility of postoperative extension bracing to prevent PJK.7–9 Hence, there is very limited evidence on this topic in the literature. In addition, these studies have heterogeneous patient populations and bracing strategies, raising questions about the validity of their findings. The objective of this study was to assess whether hyperextension bracing reduces the incidence of PJK after ASD surgery at a single center, with patients from a single surgeon in order to minimize systematic variables. In addition, we only included lower thoracic to pelvis posterior-only fusion patients to maintain the homogeneity of the cohort and minimize confounding variables when analyzing the role of bracing.
Methods
Study Design and Patient Population
This was a retrospective cohort study approved by the Institutional Review Board (eCAP, IRB #2014-357), and informed consent was obtained for all patients. Patients who underwent a posterior-only fusion (pelvis to UIV T9-12) for ASD by a single surgeon between 2017 and 2021 and had a minimum of 1-year follow-up were included. Starting in 2021, all lower thoracic fusions were braced using a Jewett hyperextension brace. Patients were stratified into 2 cohorts: braced and non-braced. The surgeon routinely preserves the midline ligamentous structures from the UIV-2 and proximally. Other PJK prophylactic techniques, such as posterior ligamentous reinforcement or vertebroplasty were not used.
Brace Application and Postoperative Protocol
The Jewett hyperextension brace is designed for resisting motion primarily in flexion. It is a three-point orthosis having 3 distinct areas of contact with the trunk – superior and inferior anterior pads contacting the manubrio-sternal area and pubis, respectively, and a posterior pad contacting the middle of the back. The superior and inferior anterior pads apply pressure forcing the patient backwards and the posterior pad pushes the spine forward maintaining a hyperextension posture. The brace was fitted with the patient in a supine position using a log roll technique. Patients wore the brace at all times (unless in bed) for the first 6 weeks after surgery. Various manufacturers were used. The Jewett brace was used because it has a “three-point” loading design where it pushes on the upper thoracic region to support extension and protect the junction. Other thoraco-lumbo-sacral orthoses (TLSOs) do not support extension in the same manner.
Data Collection
The following data were collected and managed using REDCap (Research Electronic Data Capture) 10,11 hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384: 1. Demographics and Comorbid Conditions: age, gender, body mass index (BMI), race, ethnicity, comorbid conditions, age-adjusted Charlson Comorbidity Index (CCI), American Society of Anesthesiologists (ASA) class, osteoporosis, opioid use, smoking status, insurance type. 2. Operative: primary/revision surgery, estimated blood loss (EBL), operative time, number of levels, upper instrumented level and instrumentation used, rod configuration, rod material, rod diameter, graft type, posterior column osteotomy, 3 column osteotomy, interbody fusion. 3. Radiographic: pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), PI-LL, thoracic kyphosis (TK), T1 pelvic angle (TPA), L1 pelvic angle (L1PA), maximum Cobb angle, proximal junctional angle (PJA), proximal junctional kyphosis (PJK). PJK was defined as a proximal junction sagittal Cobb angle (a) 4. Primary outcomes of interest included: PJK angle, PJK incidence and proximal junctional failure (PJF - PJK requiring revision surgery) within 1 year of surgery.
Statistical Analysis
All statistical analyses were performed using Posit team (2023). RStudio: Integrated Development Environment for R. Posit Software, PBC, Boston, MA. URL https://www.posit.co/. A 1:1 propensity match was performed identify comparative braced and non-braced cohorts. The parameters for matching were age, number of levels, 3 column osteotomies, and magnitude of correction as determined by change in PI-LL mismatch from preoperative to immediate postoperative x-rays. The above-listed variables were analyzed for differences between the braced and non-braced cohorts (both matched and unmatched) with unpaired t, Mann Whitney, and Chi-square tests, when appropriate. Significance was defined at P ≤ .05. All analyses were performed using.
Results
141 patients were included. Out of 141, 113 (80.1%) were not braced and 28 (19.9%) were braced.
Non-Matched Analysis
Comparison of Demographics, Comorbid Conditions, Surgical Characteristics, and Preoperative Radiographic Parameters Between the Non-matched Braced and Non-braced Cohorts.
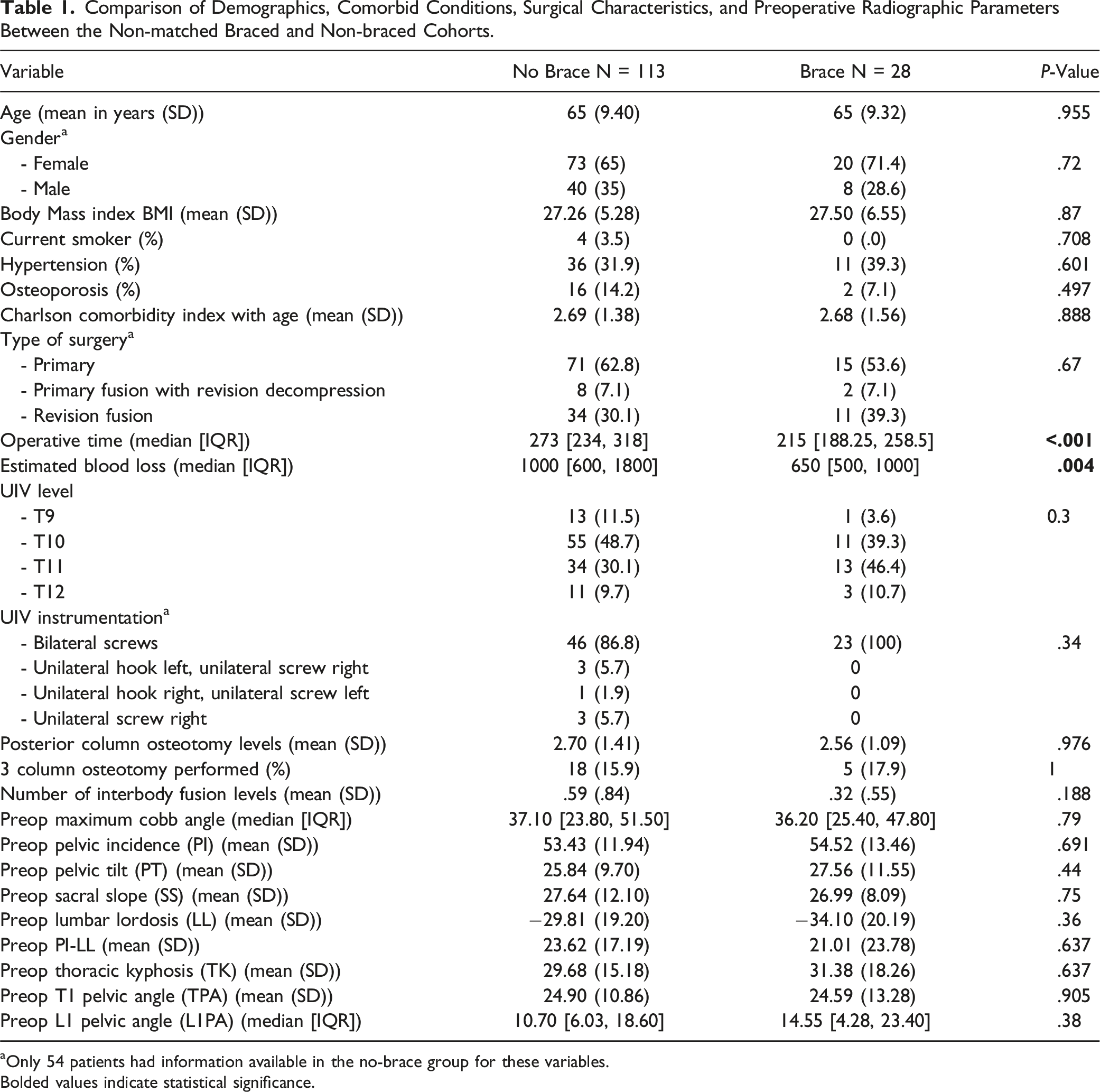
aOnly 54 patients had information available in the no-brace group for these variables.
Bolded values indicate statistical significance.
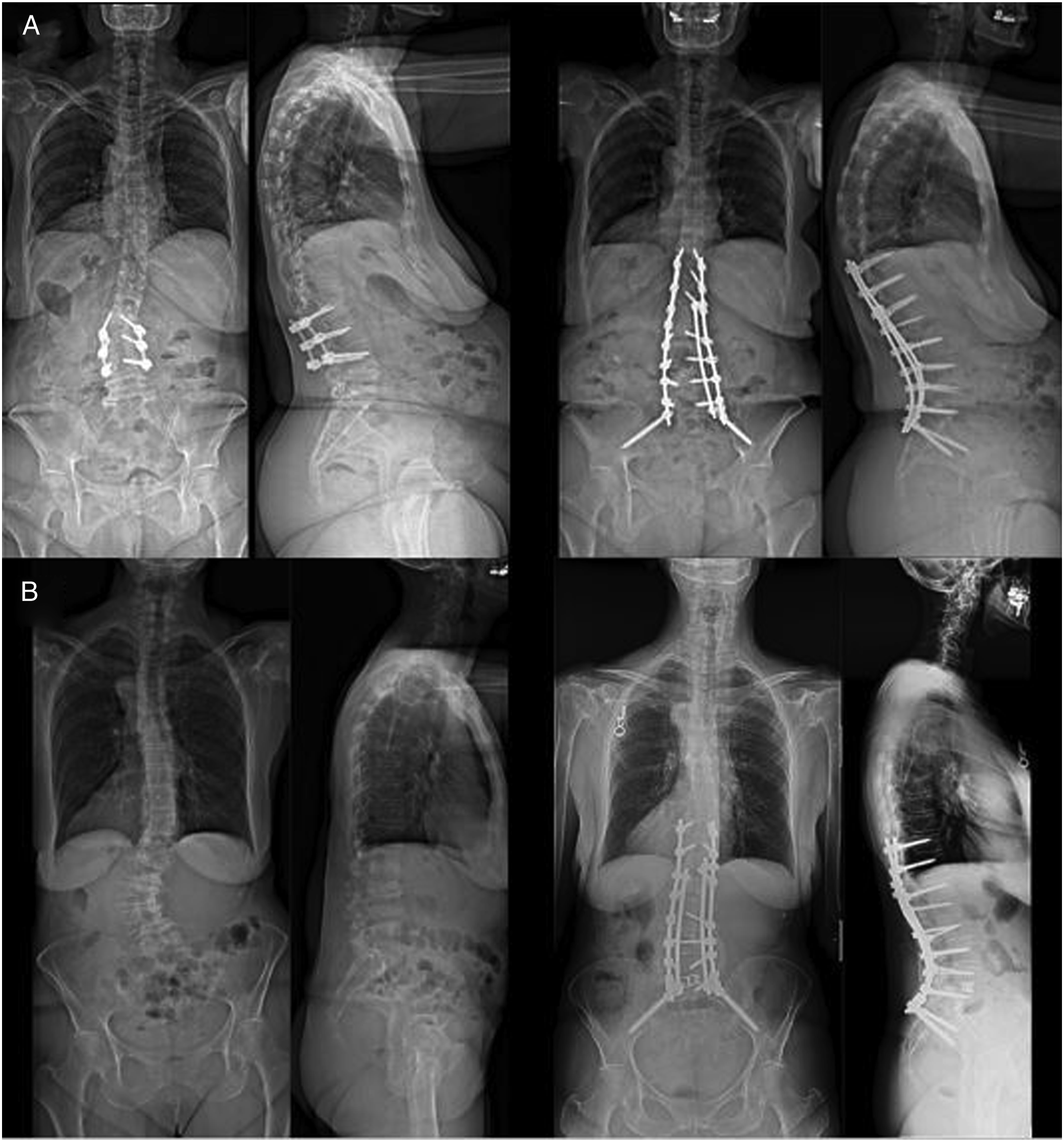
Standing AP and lateral pre and 1-year postoperative scoliosis x-rays of representative patient in the non-brace (A) and brace (B) cohorts.
Comparison of Changes in Radiographic Parameters Between the Non-matched Braced and Non-braced Cohorts.
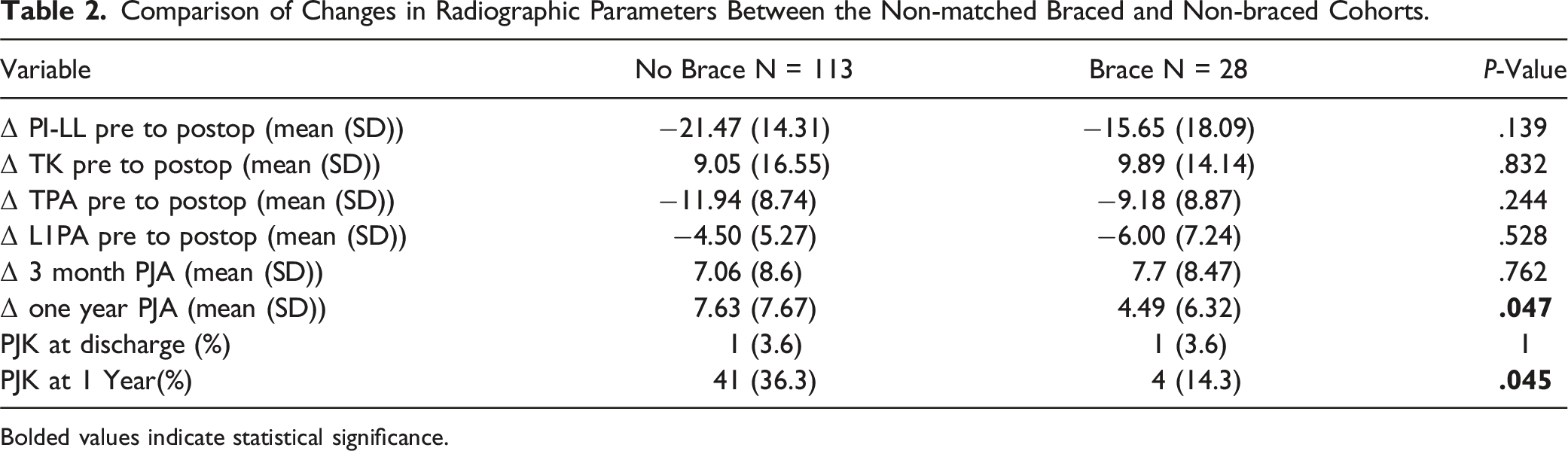
Bolded values indicate statistical significance.
Propensity-Matched Cohort Analysis
Comparison of Demographics, Comorbid Conditions, Surgical Characteristics, and Preoperative Radiographic Parameters Between the Matched Braced and Non-braced Cohorts.
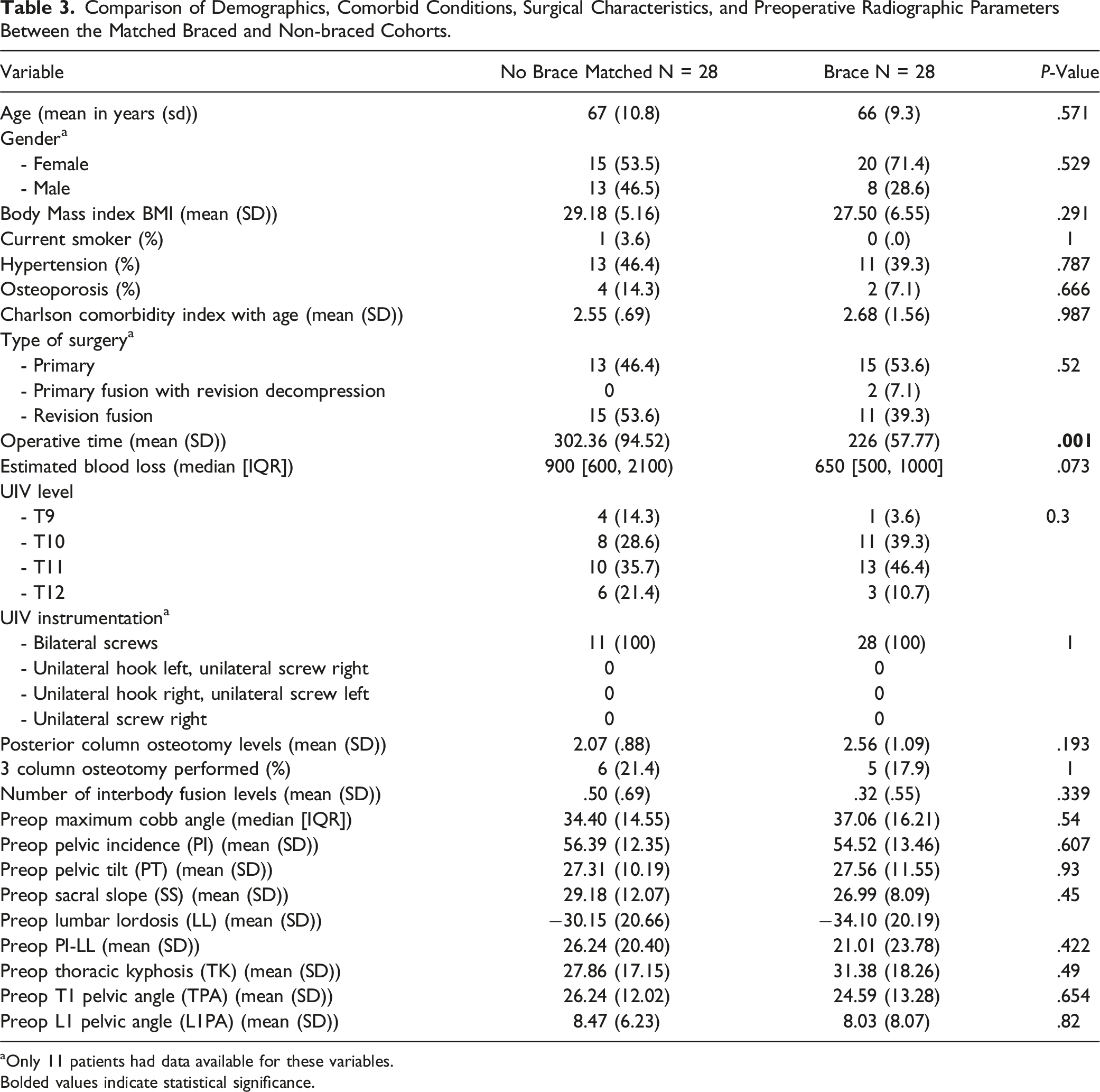
aOnly 11 patients had data available for these variables.
Bolded values indicate statistical significance.
Comparison of Changes in Radiographic Parameters Between the Matched Braced and Non-braced Cohorts.
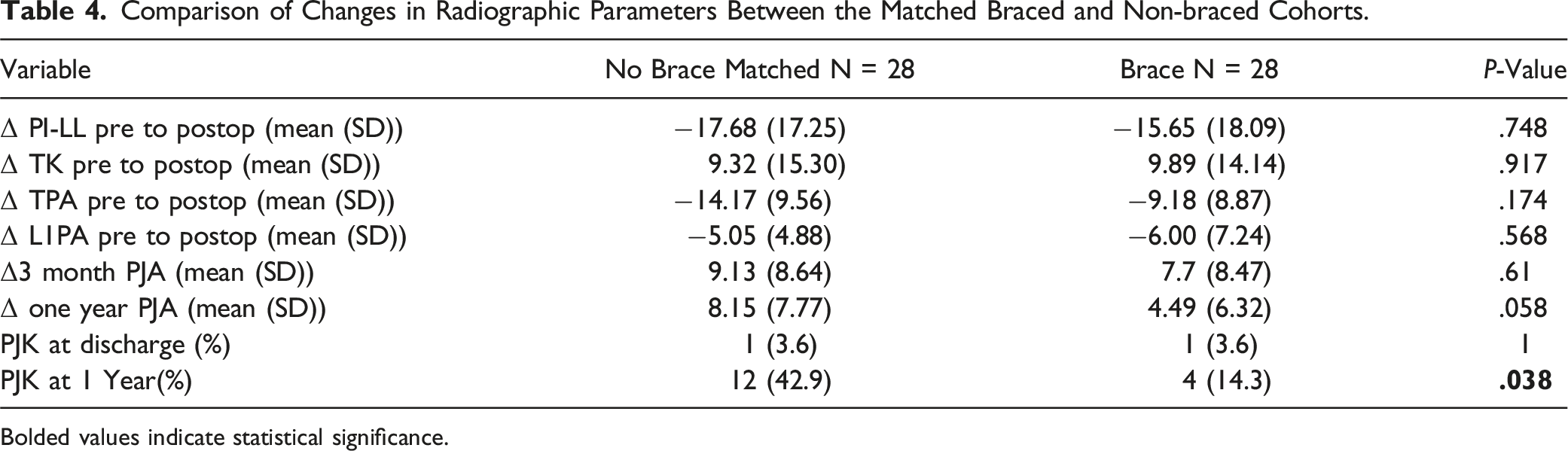
Bolded values indicate statistical significance.
Discussion
Our data demonstrate that patients who underwent hyperextension bracing for 6 weeks after corrective surgery for adult spinal deformity had a statistically significant smaller change in proximal junctional angle at 1 year postoperatively. Additionally, patients who were braced had a lower incidence of proximal junctional kyphosis at 1 year postoperatively. Despite these findings, no difference in proximal junctional failure was observed between braced and non-braced cohorts at 1 year.
There is very limited evidence in the literature, with only 3 studies to our knowledge addressing this topic. Pizones et al. recently conducted a retrospective matched cohort study of 359 patients analyzing the utility of bracing in preventing mechanical complications (screw failure, rod breakage, PJK) following ASD surgery . 7 The non-braced group showed significantly higher rates of mechanical complications (40% vs 27%, P = .014) and reinterventions (27% vs 17%, P = .037) compared to the braced group on univariate analysis in their study. However, PJK rates specifically did not show a significant difference between the 2 groups (braced 50%, non-braced 47%). Additionally, the significant difference seen on univariate analysis was not seen on multivariate analysis and the use of multiple rods was found to be the only independent predictor of decreased mechanical complications. Although this study had a large sample size, it had the following drawbacks that question the validity of the findings: a) matching only controlled for age, gender, and frailty. The braced and non-braced groups had significant differences in UIV, use of multiple rods, extent of correction, and surgical approaches, suggesting the groups may have been quite different, selection bias as brace prescription was at surgeon’s discretion, and assessment methodology of PJK was not defined.
In another study, Lord et al. conducted a retrospective review of 81 patients and found no significant difference between the braced and non-braced groups in terms of PJK rates. 8 However, the focus of their study was to examine the relationship between global alignment and proportion (GAP) score. The effect of bracing on PJK was only a secondary objective. They provided no information regarding the type of brace utilized or the treatment protocol. Lastly, Crawford et al, in their retrospective cohort study of 112 patients, reported no significant difference in PJK rates between the braced and non-braced groups, but interestingly found significantly less thoracolumbar kyphosis in patients who were braced. 9 However, this study has been published only as an abstract, so further information on the methodology is unavailable for comparisons. The current study is the first to show a significant reduction in PJK rates with postoperative extension bracing following ASD surgery. We believe that the strengths of this study over the previous studies are: (a) homogeneous ASD patient population undergoing lower thoracic to pelvis posterior-only fusion, (b) propensity matching based on age, number of levels, 3 column osteotomies, and magnitude of correction (all factors shown to influence the rate of PJK),12,13 and (c) similar braced and non-braced groups in terms of demographics, comorbid conditions, surgical characteristics, and preoperative radiographic parameters. In terms of PJF, although the difference in rates did not reach statistical significance, there was a trend of higher incidence seen in the matched non-braced vs braced cohort (11% and 7%, respectively). Given the PJK rate in the non-braced cohort was thrice that of the braced cohort (43% vs 14%), we believe that the failure to observe statistically significant differences in PJF rates is likely due to a lack of sufficient numbers. Future studies with larger sample size and adequate statistical power are required to demonstrate the role of bracing in reducing PJF rates.
One of the demonstrated risk factors for PJK after ASD surgery is a lower thoracic UIV.14,15 Lafage et al. recently developed a scoring system to estimate PJK risk after ASD surgery. 16 They found a higher odds ratio (OR) and attributed more points for lower thoracic UIV (OR 8.24, 2 points) than upper thoracic UIV (OR 6.63, 1 point). In their retrospective analysis of 58 patients, O’Shaughnessy et al. similarly reported higher rates of PJK in the lower thoracic UIV group compared to upper thoracic UIV (18% vs 10%). 17 These reports provide even more impetus for larger investigations designed to study whether bracing helps prevent PJK after thoracolumbar fusions.
There are multiple possible explanations for the benefit of postoperative bracing shown in our study. A hyperextension brace prevents the spine from excessive mechanical loads by enforcing a more erect posture and shifting the center of gravity of the upper body more posteriorly, thereby reducing the load on the implant. 18 It also restrains flexion of the upper body – a motion involving the generation of high spinal forces. 19 Lastly, due to its contact with the upper body, the hyperextension brace transfers part of the load to the lower parts of the body, thus reducing spinal loads at the implant level. 20 Implant loading, spinal forces, and other biomechanical factors can play a critical role in the development of PJK especially during the early postoperative period, hence rationalizing the use of hyperextension bracing during this period. Apart from the biomechanical advantages, braces may also help as a psychological device. Patients wearing a brace postoperatively are more likely to avoid mechanical overloads and be more compliant with the surgeon’s recommendations. 7 At the same time, it is important to address the potential drawbacks of bracing including an increase in costs and complications such as muscle atrophy and skin maceration. 21
In our protocol, patients were advised to wear the brace at all times (unless in bed) for the first 6 weeks. The previous 2 studies examining the utility of postoperative bracing in reducing PJK had slightly different protocols. In the study by Pizones et al, patients wore a thermoplastic rigid TLSO during daytime for 3 months and were then weaned over the next 4 weeks. 7 Crawford et al. also followed the protocol of bracing for 3 months postoperatively. 9 Since there is very limited evidence in the literature with only 2 prior studies reporting their protocol, it is not possible to have a consensus on the duration of postoperative bracing when it is being investigated for the likelihood of reducing PJK after ASD surgery. We recommend wearing the brace for 6 weeks as advising it for a shorter period is likely to maintain patient compliance and keep brace-related complications to a minimum. Six weeks also seems to be significant enough time for bracing to play a role in preventing junctional complications given that PJK is often an early postoperative phenomenon, occurring within 6-8 weeks in up to 62% of cases.22,23 Although PJK can still occur thereafter, we recommend wearing the brace for 6 weeks as it provides a fine balance between brace-related benefits, patient compliance, and complications.
There are several limitations of this study. This was a retrospective study and has a limited level of evidence. The data was single-center and single-surgeon making the findings less generalizable. However, this also minimizes difference in surgical techniques and allows for more accurate estimates of singular interventions. Although postoperative radiographic parameters and incidence of PJK/PJF were analyzed, clinical outcomes were not compared between the braced and non-braced groups. Additionally, brace-related complications were not analyzed. The minimum follow-up required for inclusion in the study was short (1 year). In our defense, although PJK can have a progressive component for up to 2 years after surgery, it is usually recognized in the early postoperative period.22,23 Only 28 patients were included in the braced cohort of this study, reducing the statistical power. Although results in terms of PJF rates and change in PJA at 3 months and 1 year trended to be favorable in the braced group, statistical significance could not be attained possibly due to the low sample size. The matched non-braced cohort had more patients who had osteoporosis (4 vs 2 in braced cohort) and were currently smoking (1 vs zero in braced cohort). These differences, although not statistically significant, could have confounded the results. While the difference in osteoporosis was significant, the clinical difference was not enough to support this being solely responsible for the relatively large increase in PJK. For this reason, we present this as a pilot trial and cannot conclude that bracing was the sole reason for the reduction in PJK. This will certainly be tested in future randomized controlled trials (RCTs). Variations in rod contouring can also impact rates of PJK. However, this was not analyzed in this study and could have been another confounding factor. Lastly, there is a temporal bias in the patient cohort. Bracing was performed on patients who more recently underwent surgery. Surgeon technique may have therefore become more proficient, which could have an effect on patient outcome. This may have also been the likely cause of significantly less operative time and EBL in the braced cohort.
In conclusion, this pilot study shows that our protocol for extension bracing may reduce rates of PJK following ASD surgery. These findings can form the basis to power future multi-center trials examining the effect of extension bracing on rates of junctional complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.