
Abstract
Study Design
Retrospective review of prospective multicenter data.
Objectives
This study aimed to investigate the shape of TK before and after fusion in ASD patients treated with long fusion.
Methods
ASD patients undergoing posterior spinal fusions including at least T5 to L1 without prior fusion extending to the thoracic spine were included. Patients were categorized based on the preoperative T1-T12 kyphosis into: Hypo-TK (if < 30°), Normal-TK, and Hyper-TK (if > 70°). Regional kyphosis at T10-L1 (Distal), T5-T10 (Middle), and T1-T5 (Proximal) and their relative contributions to total kyphosis were compared between groups, and the pre-to postoperative changes were investigated using paired t test.
Results
In total, 329 patients were included in this analysis (mean age: 57 ± 16 years, 79.6% female). Preoperative T1-T12 TK for the entire cohort was 40.9 ± 2° (32% Hypo-TK, 11% Hyper-TK, 57% Normal-TK). The Hypo-TK group had the smallest distal TK (5.9 vs 17.1 & 26.0), and middle TK (8.0 vs 25.3 & 45.4), but the percentage of contribution to total kyphosis was not significantly different (Distal: 24.1% vs 34.1% vs 32.8%; Middle: 46.6% vs 53.9% vs 56.8%, all P > .1). Postoperatively, T1-12 TK increased significantly (40.9 ± 2.0° vs 57.8 ± 17.6°). Each group had a decrease in distal kyphosis (Hypo-TK 2.6 ± 10.4°; Normal-TK 8.9 ± 11.5°; Hyper-TK 14.9 ± 12°, all P < .05). The middle kyphosis significantly decreased for Hyper-TK (11.8 ± 12.4) and increased for both Normal-TK and Hypo-TK (3.8 ± 11° and 14.2 ± 11°). Proximal TK increased significantly for all groups by 14-18°. Deterioration from Normal-TK to Hyper-TK postoperatively was associated with lower rate of patient satisfaction (59.6% vs 77.3%, P = .032).
Conclusions
Posterior spinal fusion for ASD alters the magnitude and shape of thoracic kyphosis. While 60% of patients had a normal TK at baseline, 30% of those patients developed iatrogenic hyperkyphosis postoperatively. Patients with baseline hypokyphosis were more likely to be corrected to normal TK than hyperkyphotic patients. Future research should investigate TK restoration in ASD and its impact on clinical outcomes and complications.
Keywords
Introduction
Adult spinal deformity (ASD) encompasses a broad range of radiographic patterns and clinical presentations but often leads to detrimental effects on function and quality of life.1,2 Precise estimation of the prevalence of ASD is challenging, but it has been reported to be over 60% in the elderly population. 3 With the increasing life expectancy in the United States, 4 ASD prevalence can be expected to continually rise, and further investigations focused on ASD are warranted.
Spinopelvic sagittal alignment is an important predictor of clinical outcomes following surgical treatment of ASD.5-7 Prior studies on sagittal alignment have placed significant emphasis on understanding and analyzing the loss of lumbar lordosis (LL), which is observed in both simple degenerative and complex deformity patient populations. 8 Loss of lordosis has been well-quantified9,10 and shown to be a primary contributor to pain and disability in ASD patients.11-14 Subsequent studies have also focused on describing the distribution, segmental angles, and apex of lumbar lordosis.15,16
Contrary to the abundance of studies on LL shape and morphology, current literature regarding thoracic kyphosis (TK) remains sparse. In patients with flatback deformity, flattening of TK may be observed as a compensatory mechanism for the loss of lumbar lordosis.17-19 Following surgical correction of ASD, increased TK has been reported as a reciprocal change and has been correlated with the development of proximal junctional kyphosis (PJK).20-22 However, little is known about the baseline shape of TK in ASD patients and the iatrogenic impact of long fusions on this curvature. It is critical to pursue a deeper understanding of TK given the potential for providing greater insight into ASD pathophysiology and improving surgical outcomes. Therefore, we examined the shape and distribution of TK before and after surgery in ASD patients undergoing long thoracic fusion.
Methods
Patient Population
This was a retrospective review of a prospective multicenter database of ASD patients. Institutional review board (IRB) approval was obtained at each site prior to study initiation. We included patients above 18 years of age who underwent posterior spinal fusion from at least T5 to L1 and met the radiological criteria of ASD (coronal Cobb angle >20°, sagittal vertical axis [SVA] >5 cm, pelvic tilt [PT] >25°, or TK >60°). Exclusion criteria included previous fusion involving any thoracic level (T1-T12) and less than 2 years of follow-up.
Data Collection
Demographic information collected included age, sex, and body mass index (BMI). Surgical data collected included locations of the posterior instrumentation upper-most instrumented vertebra (UIV) and lower-most instrumented vertebra (LIV), procedure details (interbody fusion [IBF], osteotomy, direct decompression), intensive care unit (ICU) stay, and length of postoperative hospital stay (LOS). Revision data including date of revision surgery and associated complications were also collected, when applicable. Health-related quality of life (HRQOL) outcomes, including Oswestry Disability Index (ODI) and Scoliosis Research Society-22 (SRS-22) questionnaire, were collected preoperatively and 2 years postoperatively.23,24 SRS-22 Satisfaction domain scores were analyzed, with specific focus on questions 21 and 22 (“Are you satisfied with the results of your back management?” and “Would you have the same management again if you had the same condition?”).
Preoperative and 2-year follow-up free-standing full-length spine radiographs were collected and analyzed by 2 trained independent observers using a dedicated software (Spineview, ENSAM Laboratory of Biomechanics, Paris, France).
25
Radiographic parameters were extracted and calculated using Matlab (MathWork, Natick, Massachusetts). The collected radiographic parameters included PT, pelvic incidence (PI), LL, T1 pelvic angle (TPA), SVA, and thoracic and lumbar Cobb angles (Figure 1). In addition, TK was analyzed by measuring global TK (angle between superior endplate of T1 and inferior endplate of T12), proximal TK (angle between superior endplate of T1 and superior endplate of T5), middle TK (angle between superior endplate of T5 and superior endplate of T10), and distal TK (angle between superior endplate of T10 and superior endplate of L1) (Figure 1). Segmental kyphosis was measured at each level between T1 and T12 (angle between the superior endplate of one level with the superior endplate of one level above). By convention, a lordotic angle was positive, while a kyphotic angle was negative. Radiographic parameters collected: Pelvic Incidence (PI), Pelvic Tilt (PT) T1-Pelvic Angle (TPA), Thoracic Kyphosis (TK), as well as Regional Kyphosis (Proximal, Middle, and Distal) and Segmental Kyphosis.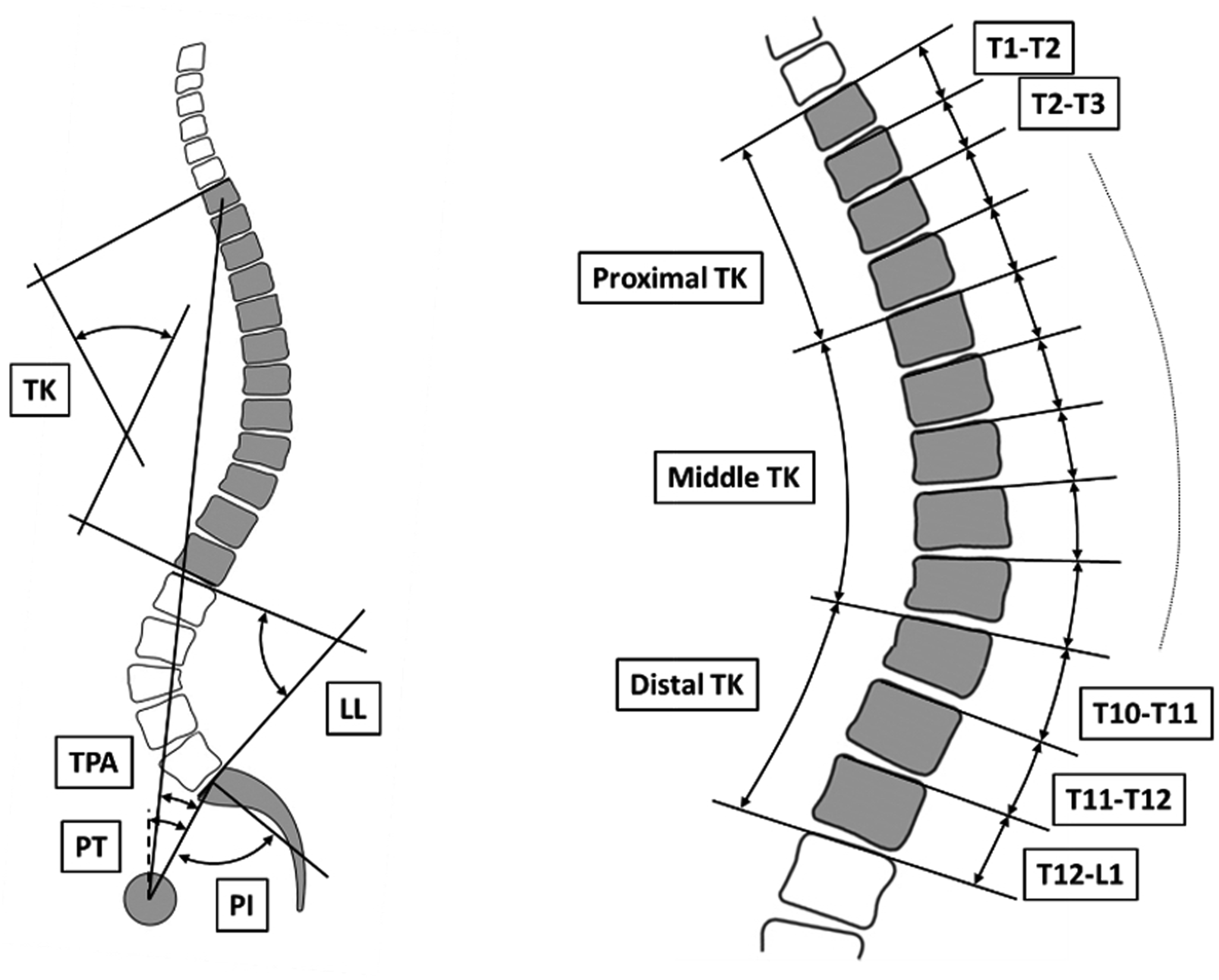
Composite imaging methods were applied to provide visualization of TK shape analysis. The TK sagittal length and orientation were normalized by setting the T7 vertebra as horizontal. TK shapes were superimposed on top of each other to create the “average” shape of TK. Whiter areas represent higher probability of presence of the spine, while black represents no spine detected in this area. Isoline with color code was then generated for more distinct visualization.
Statistical Analysis
Descriptive statistics were provided for demographic, clinical, and radiographic data. Mean and standard deviation (StD) were recorded for continuous variables, and frequencies were recorded for categorical variables. For surgical data, median number of fusion levels and frequencies of extension to pelvis, direct decompression, osteotomy, and IBF were analyzed.
For the total cohort, preoperative total and regional TK mean values were analyzed. Patients were then subcategorized into three cohorts based on their preoperative T1-T12 kyphosis using previously defined normative values. 26 Hyper-TK was defined as normative mean +1.5 StD, equating to greater than 70° global TK. Hypo-TK was defined as normative mean - 1.5 StD, equating to less than 30° global TK. Normal-TK was defined as global TK between 30° and 70°. Mean values for regional and segmental kyphosis, as well as their relative contributions to the total kyphosis, were compared among the TK groups. ANOVA or Kruskal-Wallis test was applied as appropriate for comparisons across TK groups, and post-hoc analysis with Bonferroni correction was performed for multiple comparison.
The change in TK shape from preoperative to postoperative was also analyzed; total, regional, and segmental TK were compared using either t test or Wilcoxon test, as appropriate. For each preoperative TK group, proportions of patients whose TK improved vs deteriorated vs remained the same postoperatively were recorded. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY). The level of statistical significance was set at P < .05 a priori.
Results
Cohort Description
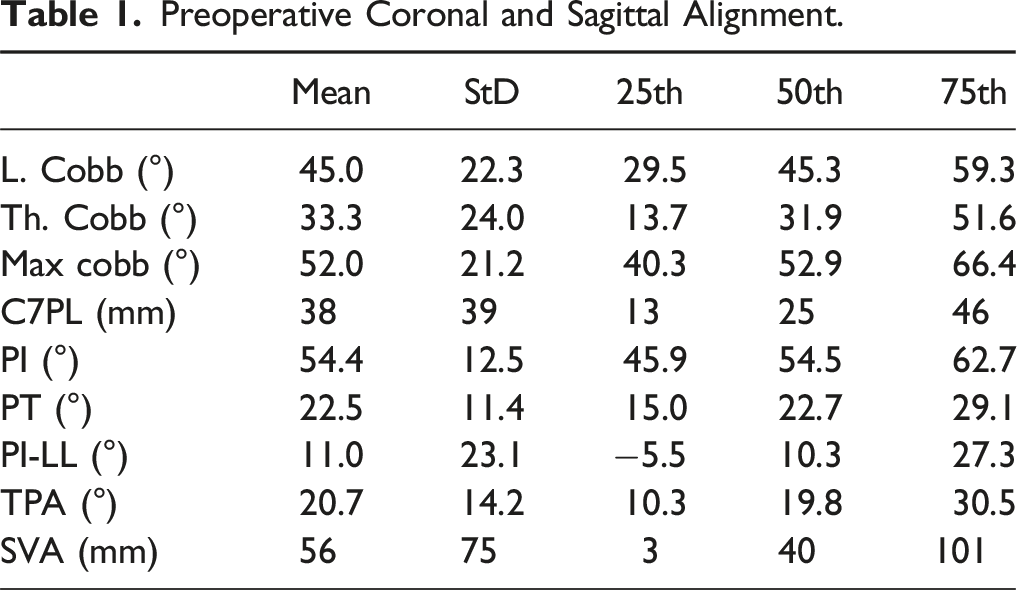
Preoperative Coronal and Sagittal Alignment.
The median number of levels fused was 15 (interquartile range [IQR] 14-16), 68.4% of cases extended to the pelvis, breakdown of UIV position: T4 (44.4%) T3 (28.6%) and T2 (16.8%). 44.8% of cases involved some direct decompression, 81.0% of cases involved some osteotomy (15.2% received a 3-column osteotomy), and 51.9% of cases involved IBF. The median EBL was 1500 cc (IQR 900-2500 cc). 78.7% of patients required some ICU stay, and 20.2% of patients required ICU stay for more than 48 h. The median LOS was 7 days (IQR 6-10 days).
Preoperative Thoracic Kyphosis
Median and Interquartile Value for the Total, Regional and Segmental Kyphosis. Values Are Reported for Overall Cohort as Well as by Preoperative TK Group. Comparison Performed Using Kruskal-Wallis Test.
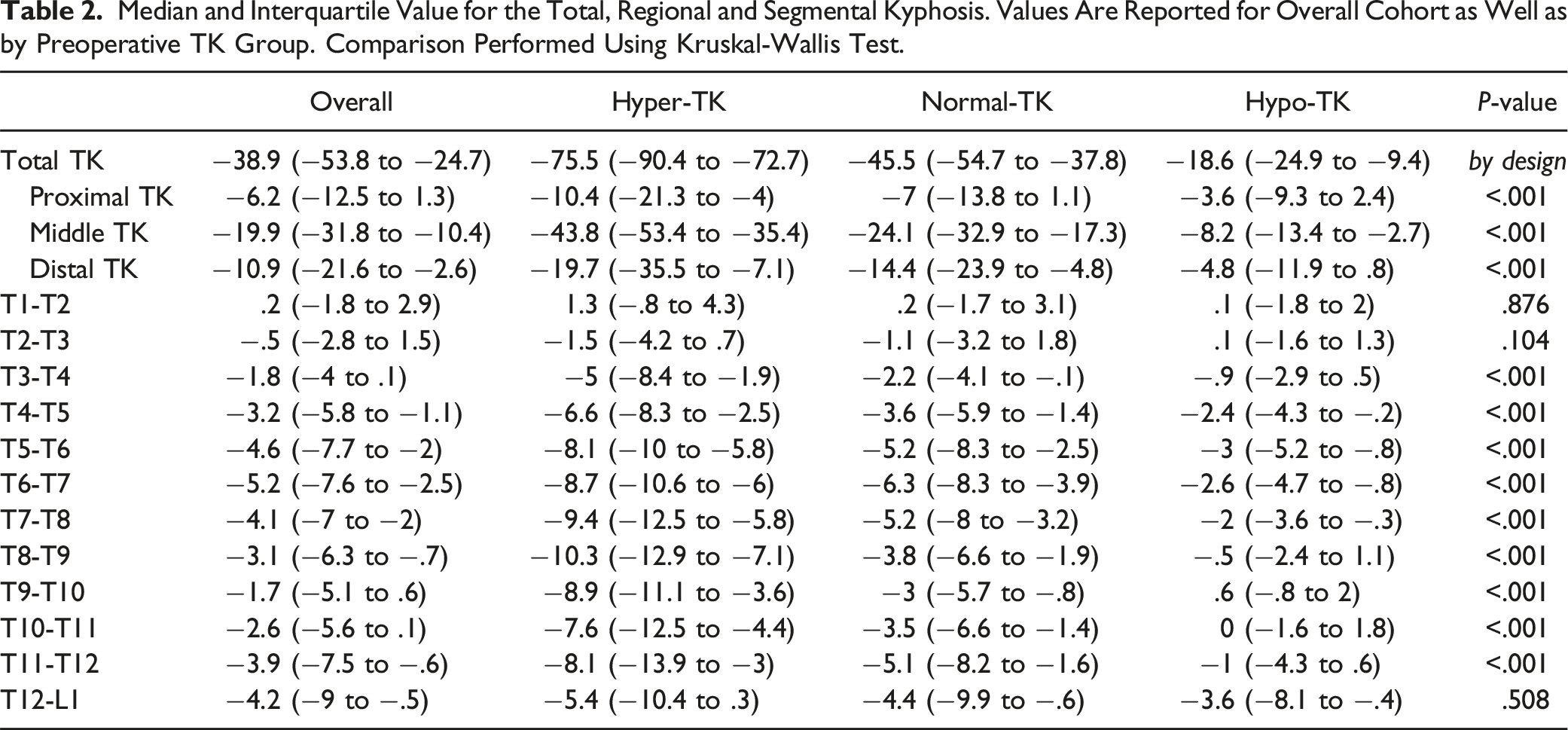
When stratifying into preoperative total TK cohorts, 31 (9.8%) patients were categorized as Hyper-TK (mean TK -83.1° ± 15°), 176 (55.7%) patients as Normal-TK (mean TK -46.9° ± 11°), and 108 (34.3%) patients as Hypo-TK (mean TK -16.1° ± 11°). Post-hoc analysis revealed no significant difference in proximal nor distal TK between Hyper-TK and Normal-TK (P = .157 and P = .291, respectively). However, all other comparisons of regional kyphosis were significant (all P < .05) (Table 2).
Despite the significant differences in the magnitude of curvature, relative contributions of the middle and distal TK to overall TK were not significantly different between TK groups (P = .216 and P = .329, respectively). The proximal TK contribution was only significantly different between Normal-TK and Hypo-TK groups (15.0% [IQR -2.2% to 30.0%] vs 30.8% [IQR -7.7% to 52.0%], P = .026).
Postoperative Outcomes
From preoperative to 2-year follow-up, there were significant improvements in both ODI (Δ −15.5 ± 18.8, P < .001) and SRS-22 (Δ .93 ± .7, P < .001). The median SRS-22 Satisfaction score was 4.5 (IQR 3.5 to 5). 73.2% of patients responded either “satisfied” or “very satisfied” to the question: “Are you satisfied with the results of your back management?” 80.4% of patients responded either “probably yes” or “definitely yes” to the question: “Would you have the same management again if you had the same condition?” Following the index procedure, 58 (18.4%) patients underwent some revision surgery before the 2-year postoperative visit. The mean time to revision surgery was 11.4 ± 7.5 months from index surgery. The 2 main reasons for revision were implant failure (screw/rod breakage, N = 20) and X-ray imbalance (PJK/distal junctional kyphosis [DJK], N = 16). At 2-year follow-up, PI-LL decreased by 10.1° ± 19°, and TPA decreased by 6.2° ± 11.1°. Mean postoperative SVA was 13 ± 53 mm, and mean postoperative PT was 19.8° ± 11°. Patient with a fusion extended to pelvis had a significantly more anterior alignment (PI-LL: −2.6 + 13.5 vs 2.4 ± 15.8; TPA: 10.2 ± 13.3 vs 16.5 ± 11.3; SVA: 1 ± 46 vs 19 ± 55, all P < .005).
2-Year Follow-up Thoracic Kyphosis
From preoperative to 2-year follow-up, the mean overall TK for the total cohort increased significantly (2-year TK: −56.8° ± 18.0°, P < .001). Proximal TK (−15.5° ± 12.7°) and middle TK (−5.7° ± 13.0°) both increased significantly, while distal TK decreased (eg, flattened) by 7.3° ± 11.1° (all P < .001). Segmental kyphosis changed significantly at each individual level (Figure 2). Rate of radiographic PJK at 2-year was 40.6%. Comparison of regional change between patient without and without radiographic PJK demonstrated a significantly larger kyphotic proximal change for PJK (−23.2° ± 12.5 vs −10.3° ± 9.2, P < .001) and a significantly larger lordotic distal correction for PJK patients (9.6° ± 12.1 vs 5.5° ± 10.2, P < .001) without significant change in middle TK (P = .99). Boxplot of the change in segmental kyphosis for the entire cohort. Wilcoxon paired test p-value reported for each individual level.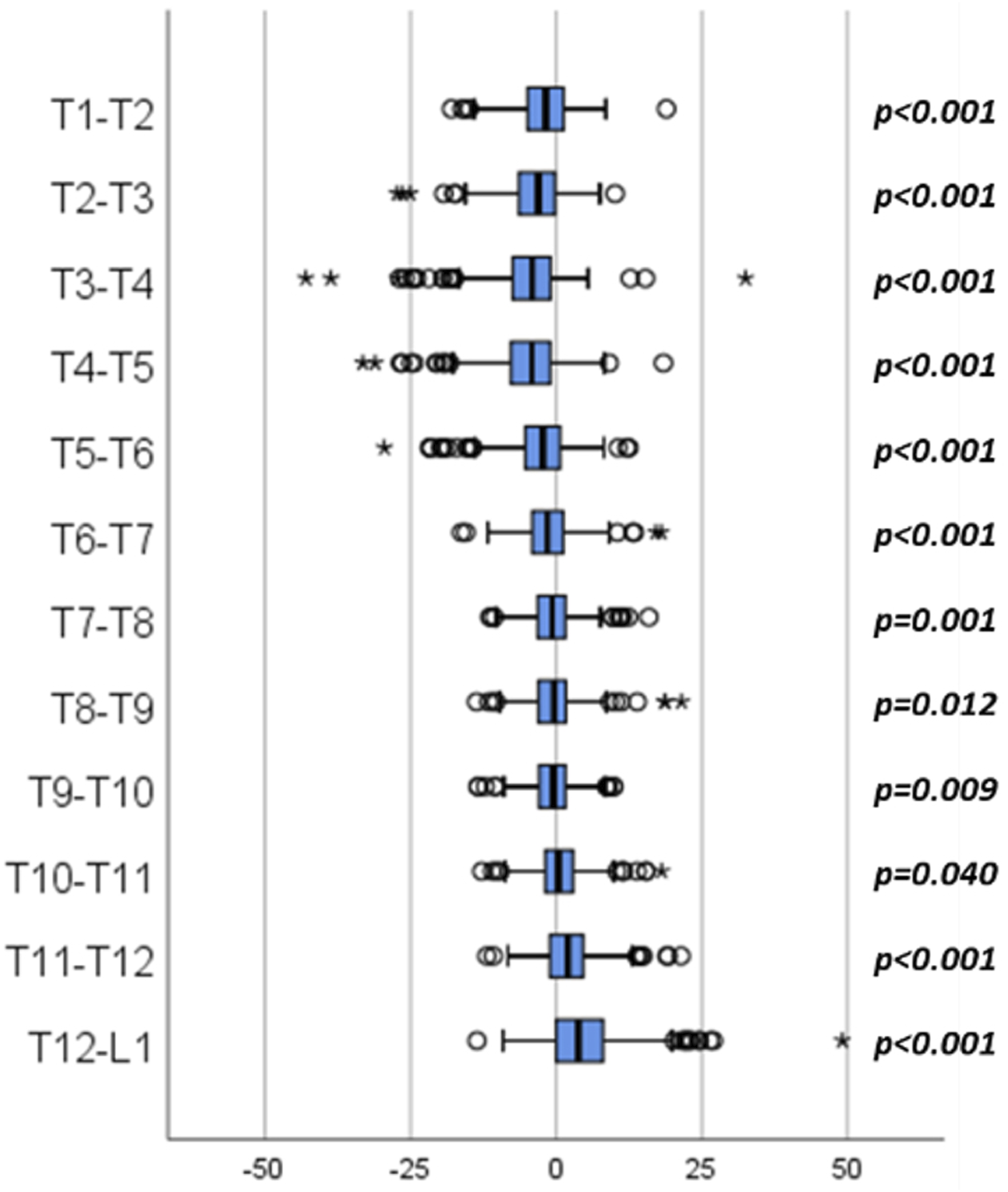
There were significant differences in the magnitude of change in regional kyphosis among the preoperative TK groups. The overall TK increased for the Normal-TK group (Δ −14.4° ± 14°) and Hypo-TK group (Δ −27.9° ± 15°), while it flattened for the Hyper-TK group (Δ 7.3° ± 15°) (all pairwise comparison P < .001). There was no significant difference in the increase in proximal TK between groups (Hyper: −14.8° ± 17° vs Normal: −16.7° ± 12° vs Hypo: −13.7° ± 12°, P = .206). Middle TK flattened significantly for Hyper-TK patients while it increased for Hypo-TK group (Hyper: 11.4° ± 12° vs Normal: −3.6° ± 11 vs Hypo −14.1° ± 11, all pairwise P < .001). Lastly, the distal TK flattened on average for Hyper- and Normal-TK groups while it significantly increased for Hypo-TK patients (Hyper: 3.6° ± 10° vs Normal: 8.7° ± 11° vs Hypo: −13.1° ± 11°, both P < .001).
Median and Interquartile Segmental Change for Hyper-, Normal-, and Hypo-TK. Comparison Pre-to-post (Paired) Within Each Group and Kruskal-Wallis Test (K-W) Across Group. Orange Represents a Significant Increase in Kyphosis, Blue Represents a Significant Decrease in Kyphosis.
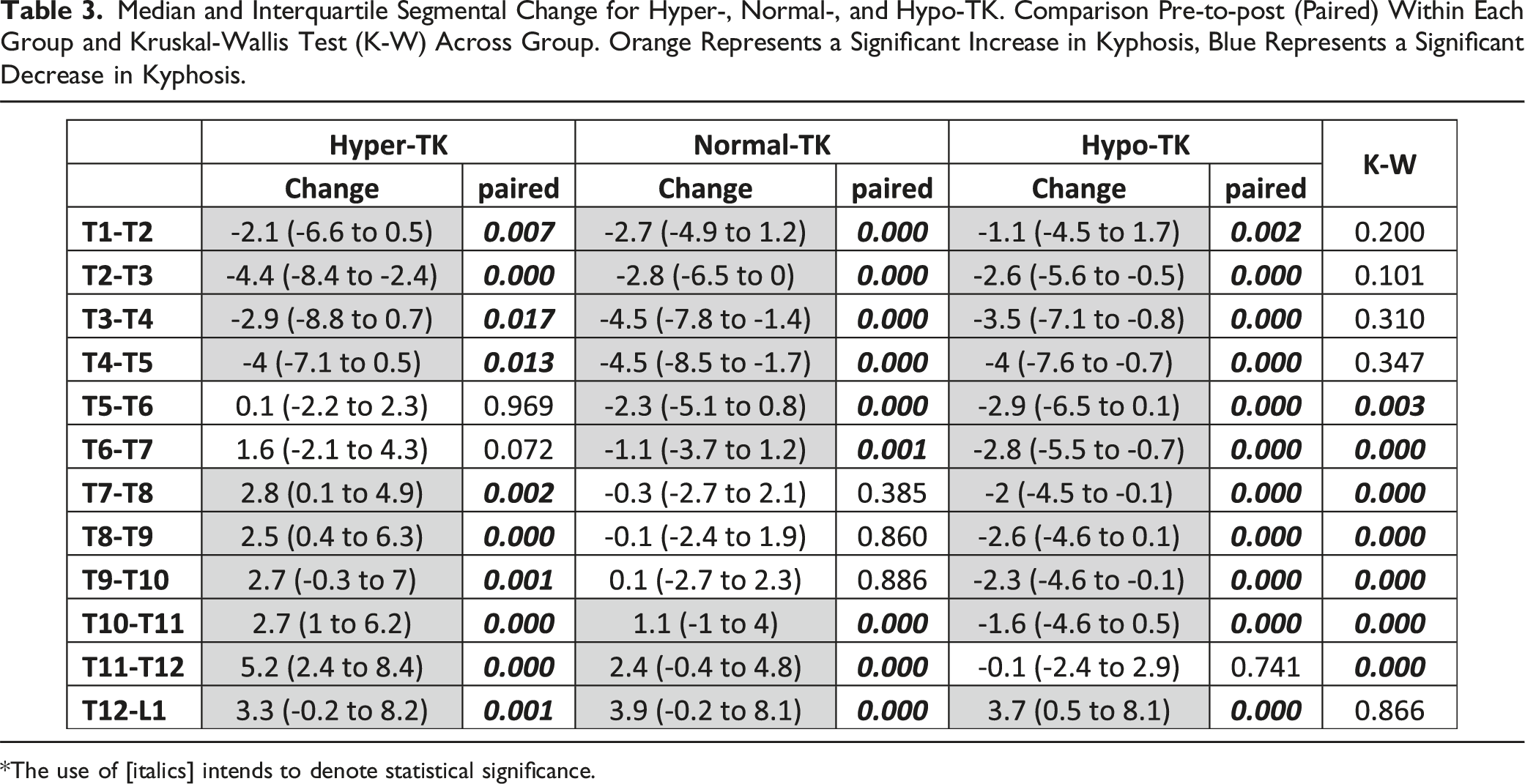
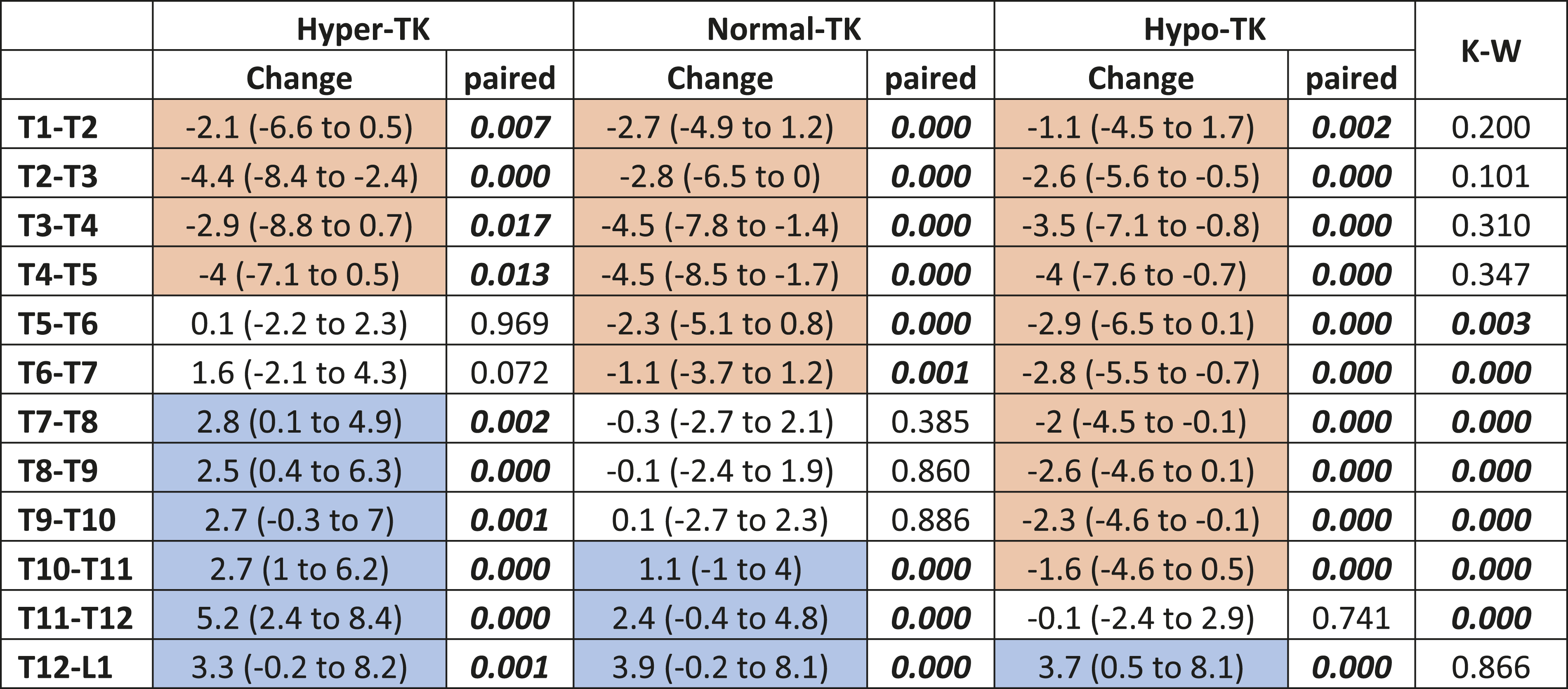
*The use of [italics] intends to denote statistical significance.
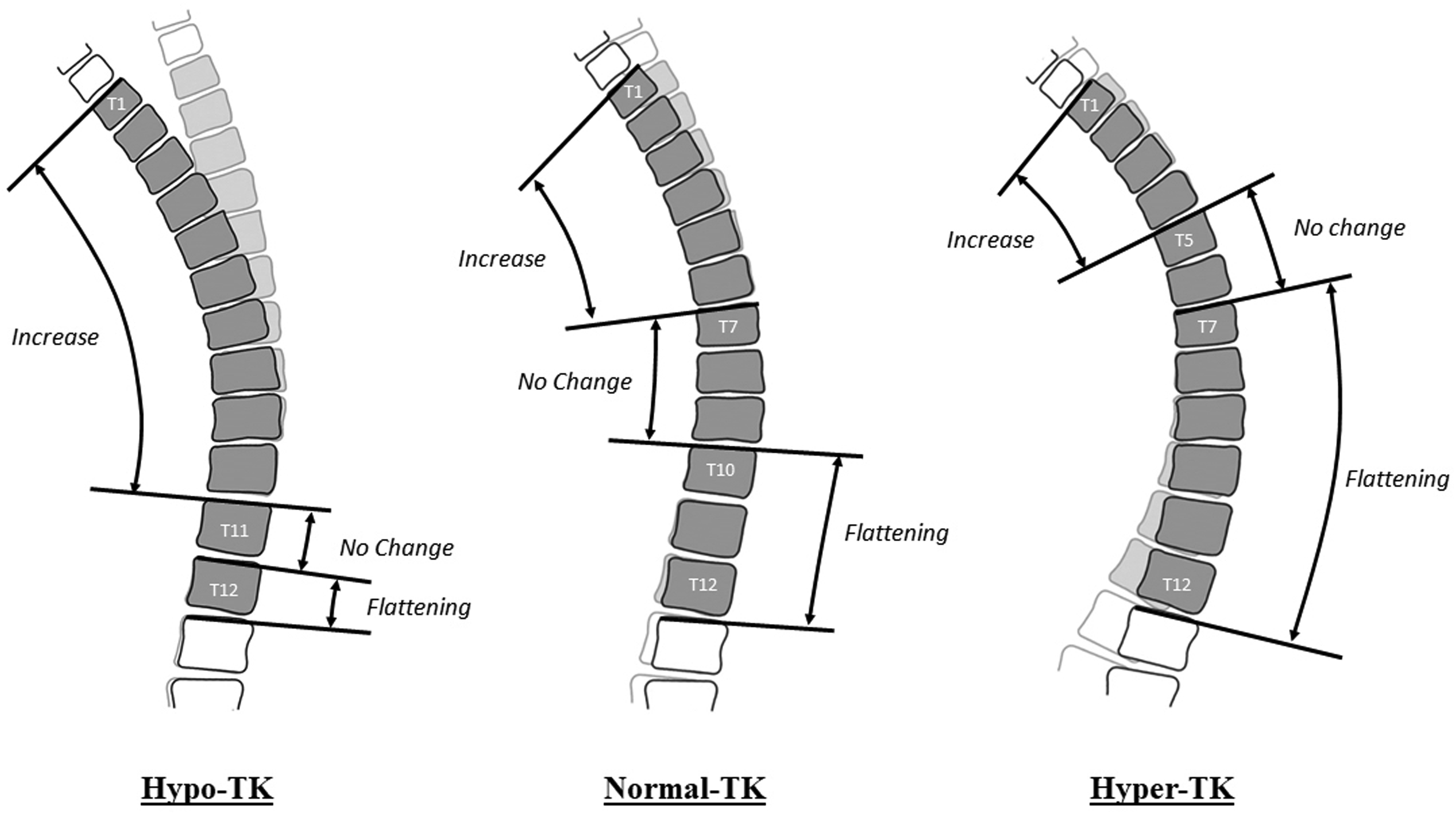
Schematic representation of the segmental change between pre (transparent) and post (bold) for the 3 types of pre-operative kyphosis (Hypo-TK: left, Normal-TK: middle, Hyper TK: right).
Postoperative global TK measurements were categorized as Hyper-, Normal-, and Hypo-TK based on the same criteria used for preoperative grouping (Figure 4). Postoperatively, 71 (22.5%) patients were categorized as Hyper-TK, 217 (68.9%) patients as Normal-TK, and 27 (8.6%) patients as Hypo-TK. Cross tabulation with preoperative TK grouping revealed that 13/31 (41.9%) of Hyper-TK patients improved to Normal-TK postoperatively, while 18/31 (58.1%) remained Hyper-TK. Of the patients categorized as Normal-TK preoperatively, 121/176 (68.8%) remained at Normal-TK, 51/176 (29.0%) deteriorated to Hyper-TK, and 4/176 (2.3%) deteriorated to Hypo-TK. Among patients who were preoperatively Hypo-TK, 83/108 (76.9%) improved to Normal-TK, 2/108 (1.9%) became Hyper-TK, and 23/108 (21.3%) remained Hypo-TK (Figure 4). 41 (57.7%) patients categorized as Hyper-TK post-operatively developed some radiographic PJK. Similarly, 83 (38.2%) patients categorized as Normal-TK and 4 (14.8%) patients categorized as Hypo-TK demonstrated sign of radiographic PJK. Preoperative and postoperative “average shape” and isolines of probability of presence stratified by preoperative and postoperative group of Thoracic Kyphosis.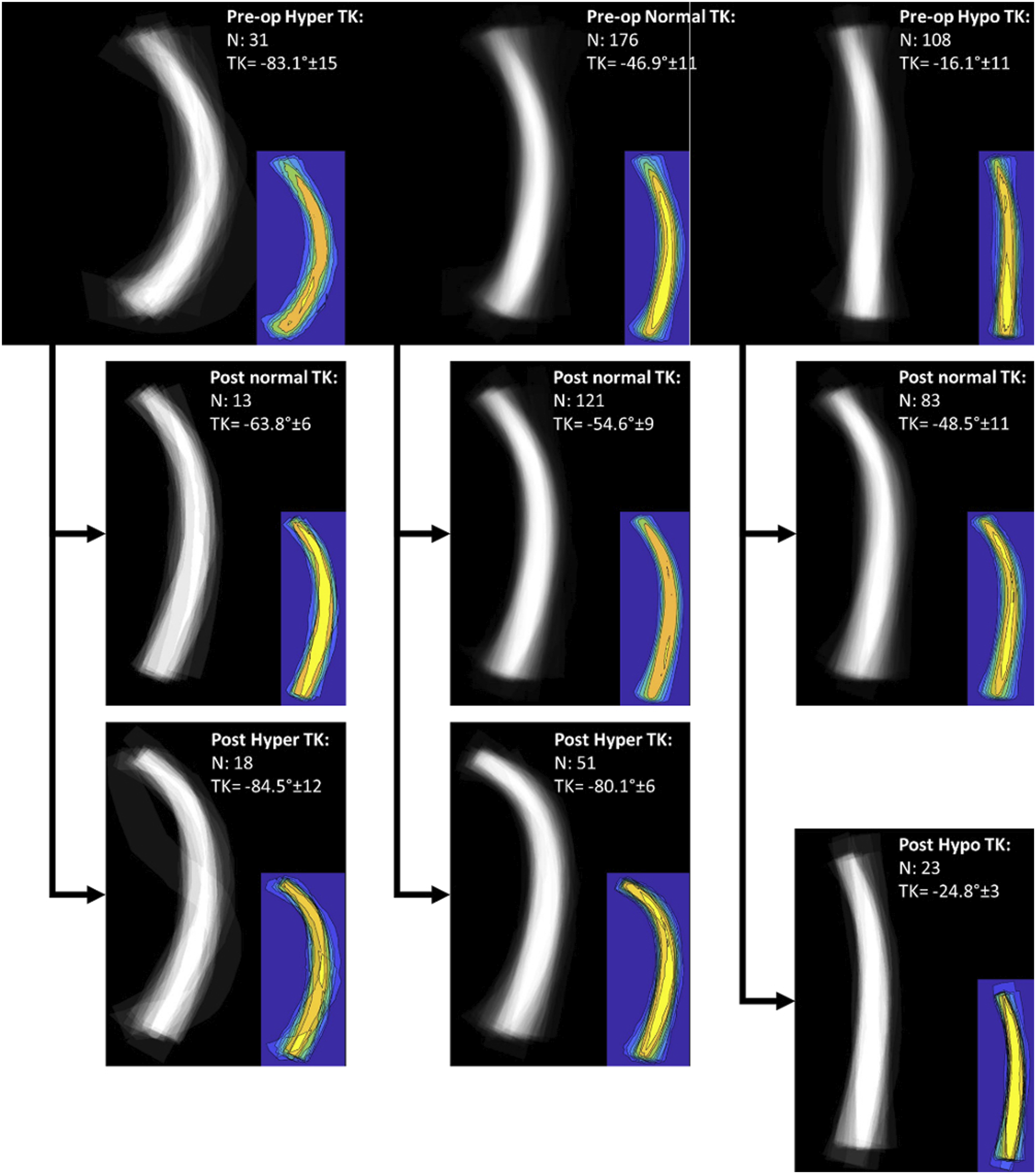
Comparison of patient satisfaction scores based on TK groups demonstrated that patients who were Normal-TK preoperatively but deteriorated to Hyper-TK postoperatively had a significantly lower rate of satisfaction (59.6% vs 77.3%, P = .032) and a trend toward lower SRS-Satisfaction scores (median 4 [IQR 3 - 5] vs median 4.5 [IQR 3.5 - 5], P = .051). However, there was no significant difference in the patients’ willingness to undergo the same management again (70.2% vs 81.8%, P = .137).
Discussion
Correction of sagittal spinal alignment is associated with improvements in disability and pain in ASD patients.3,5,28 Although many prior studies have focused on the lumbar curvature, little is known about the changes in TK following ASD surgery. To address this deficiency in the current literature, our study aimed to provide a descriptive analysis of the shape and distribution of TK in ASD patients before and after long thoracic fusion surgery.
A prior analysis aimed at understanding the normal TK magnitude and shape demonstrated that the mean T1-T12 kyphosis among asymptomatic volunteers was −49.5°. 26 In comparison, the current study cohort was found to be relatively hypokyphotic, with a median preoperative global TK of −39.9°. This difference in baseline TK can likely be attributed to the fact that this study included symptomatic patients undergoing surgery for ASD, which is associated with pathologic loss of LL and reciprocal change in TK. 21 This is also supported by the finding that there were disproportionately more patients in the Hypo-TK group (34.3%) compared to Hyper-TK group (9.8%) based on preoperative measurements. Similar to pelvic retroversion, knee flexion, and cervical lordosis, reduction in TK has been highlighted as a compensatory mechanism in the setting of sagittal spinal malalignment, aimed at posteriorly translating the center of gravity to align over the pelvis. 17
Our study cohort demonstrated an asymmetric distribution of kyphosis across the thoracic spine, with the majority of global TK deriving from middle TK (52.3%), followed by distal TK (28.8%), then proximal TK (16.4%). The relative contributions of regional kyphosis to total TK were mostly maintained across TK groups; however, proximal TK contribution was significantly greater for Hypo-TK patients (30.8%) compared to Normal-TK patients (15.0%). Lafage et al 26 similarly showed that TK was asymmetrically distributed and that the proportion between T7-L1 kyphosis and T1-T7 kyphosis increased significantly as overall TK increased. This suggests that the decrease in TK in thoracic hypokyphosis may not occur uniformly but rather occurs to greater degrees in the middle and distal thoracic spine, leading to greater relative contribution by proximal TK in hypokyphotic patients. One possible reason for this is the increased rigidity of the upper thoracic spine secondary to rib cage stabilization. 29 More in-depth segmental analyses of thoracic hypokyphosis in flatback patients are required to further clarify the regional distribution of this compensatory mechanism.
Overall, there was a significant increase in TK after long thoracic fusion, with a mean increase in global TK of approximately 17°. This is consistent with prior literature; Decker et al 30 reported an average TK increase of 18° following ASD surgery. There were significant increases in TK at the proximal and middle segments, and distal TK decreased on average. The increase in middle TK represents true restoration of the sagittal curvature, while the proximal TK increase is likely highly affected by junctional change between the fused and unfused segments. Moreover, the current study found that baseline TK influenced postoperative TK, with baseline hypokyphotic patients experiencing greater magnitudes of TK increase postoperatively. Similar findings have been previously reported. In an analysis of ASD patients undergoing LL corrective surgery, Yasuda et al 31 found that postoperative change in TK negatively correlated with preoperative TK. This suggests that the magnitude of TK restoration may be influenced by the preoperative capacity for thoracic compensation. Thoracic hypokyphosis is a compensatory mechanism which necessitates spinal flexibility and strong muscular tone, and these factors likely contribute to greater restoration of TK after fusion.17,30
Among the patients preoperatively categorized in the Hypo-TK group, 76.9% of patients were restored to Normal-TK postoperatively while 21.3% remained hypokyphotic (Figure 5). Correction of thoracic hyperkyphosis was found to be less reliably achieved, with over half of the Hyper-TK patients (58.1%) remaining hyperkyphotic at 2 years follow-up (Figure 6). This difference may be related to the reciprocal increase in TK that can occur following LL correction in ASD patients.21,32 The incidence of progressive postoperative increase in TK of greater than 10° has been approximated to be about 40%, and this reciprocal TK change can result in loss of global sagittal balance and increased junctional stress.33-35 Thus, this phenomenon should be further explored as a potential explanation for the large number of patients in which thoracic hyperkyphosis was maintained postoperatively. Anticipation of and correction for postoperative reciprocal TK change may improve radiographic outcomes. Case examples of Hypo-Kyphosis patient: Hypo-Kyphosis maintained pre to post between (A) (10.0°) and (B) (24.1°) and Hypo-Kyphosis increased pre to post between (C) (20.1°) and (D) (46.9°). Case examples of Hyper-Kyphosis patient: Hyper-Kyphosis maintained pre to post between (A) (77.3°) and (B) (87.9°) and Hyper-Kyphosis reduced pre to post between (C) (98.4°) and (D) (59.5°)

While majority (68.8%) of the patients with Normal-TK at baseline were maintained within the normal range, a significant portion (29.0%) of patients was noted to have deteriorated to hyperkyphosis postoperatively (Figure 7). Again, the deterioration to hyperkyphosis in these patients may be related to the reciprocal progression of TK.21,31-33 It is critical to minimize hyperkyphosis in these patients as large postoperative TK has been reported as an iatrogenic risk factor for PJK.33,36 PJK is one of the most important complications of ASD surgery, associated with diminished global corrections and poor quality of life.37-39 In addition to TK magnitude, the level of UIV in the thoracic spine and the presence of preoperative thoracic compensation have also been associated with PJK risk.20,21,40 In a risk analysis performed by Yagi et al,
33
larger LL correction, age >75, and sacropelvic fusion were identified as independent predictors of significant progressive TK after scoliosis surgery. Thus, consideration of these factors may be important in avoiding postoperative thoracic hyperkyphosis and PJK, ultimately improving overall outcomes of ASD surgery. Case examples of Normal Kyphosis patient: Normal Kyphosis maintained pre to post between (A) (49.2°) and (B) (54.2°) and Normal Kyphosis increased pre to post between (C) (57.5°) and (D) (80.0°).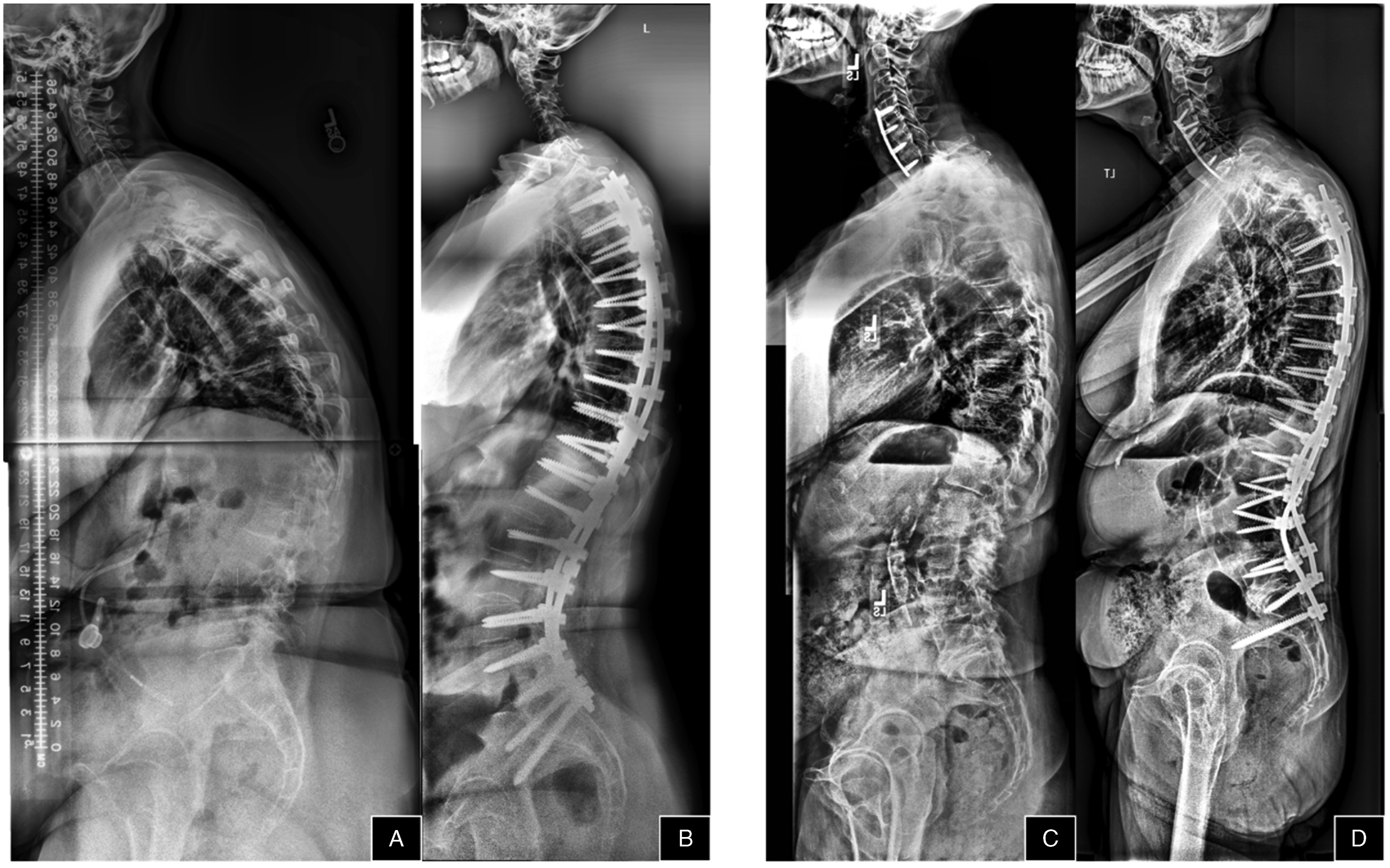
Notably, our study also demonstrates that deterioration from Normal-TK to Hyper-TK is associated with significantly lower patient satisfaction scores. Thus, greater emphasis on identifying and achieving optimal TK may help prevent PJK and improve patient satisfaction in ASD surgery. Future studies should investigate the potential correlation between adequate TK restoration and patient-reported outcome measures in ASD patients.
There are important limitations to consider when interpreting this study. The retrospective study design limits the level of evidence and the conclusions that can be drawn. The generalizability is limited by the relatively small sample size of 315 patients. This limitation also prevented subgroup analysis of TK based on demographic characteristics. Additionally, this study did not utilize three-dimensional or virtual models, which may have provided a more thorough understanding of the postoperative changes in thoracic spine shape. As the study focus was on the thoracic spine, TK measurements were not correlated with cervical or lumbar curvatures – this is a topic of future investigation. Nevertheless, this study provides the most complete evaluation of TK shape and distribution in ASD patients before and after fusion to date. Enhanced understanding of the changes in TK shape and magnitude is paramount in reducing complications such as PJK and improving overall patient satisfaction.
Conclusion
This study characterized the baseline and postoperative change in TK magnitude and shape among patients undergoing surgical correction for ASD. While 60% of patients had a normal TK at baseline, 30% of those patients developed iatrogenic hyperkyphosis postoperatively. Patients with baseline hypokyphosis were more likely to be corrected to normal TK than hyperkyphotic patients. Deterioration from normal TK to hyperkyphosis postoperatively was associated with lower patient satisfaction. Future studies investigating the impact of TK restoration on clinical outcomes and complications after ASD surgery are necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.