
Abstract
Study Design
Retrospective cohort study.
Objectives
This study aims to evaluate the impact of hospital volume on postoperative outcomes following single-level cervical disc arthroplasty (CDA), focusing on non-routine discharge rates, length of stay (LOS), and hospital costs.
Methods
After applying the appropriate exclusion criteria, the National Inpatient Sample (NIS) was queried to identify 14,315 weighted cases of patients undergoing single-level CDA between 2016 and 2020. Patients were stratified by hospital volume into low, intermediate, and high categories based on annual case numbers. Multivariate logistic regression evaluated odds of non-routine discharge and complications, while linear regression analyzed LOS and hospital costs. Models were adjusted for age, sex, and comorbidities. Statistical significance was set at P < .05.
Results
Patients in high-volume hospitals had significantly lower odds of non-routine discharge compared to both intermediate-volume (OR: 0.63, 95% CI: 0.44-0.91, P = .014) and low-volume hospitals (OR: 0.66, 95% CI: 0.45-0.98, P = .040). Patients in high-volume hospitals also incurred significantly higher costs compared to low-volume hospitals (coefficient: $1,232.22, 95% CI: $189.05-$2,275.38, P = .021), while length of stay did not differ significantly across volume categories.
Conclusions
High-volume hospitals are associated with improved discharge outcomes, but also increased costs following single-level CDA. These findings underscore the need to disseminate high-volume center practices to lower-volume hospitals while addressing cost management. Further research should explore the impact of outpatient settings and long-term outcomes to enhance care delivery for CDA patients.
Keywords
Introduction
Cervical disc arthroplasty (CDA) has emerged as an effective surgical option for managing cervical degenerative disc disease, particularly in younger patients with moderate disc degeneration.1,2 Unlike anterior cervical discectomy and fusion (ACDF), a widely adopted procedure that raises concerns about adjacent segment degeneration (ASD) due to stress on adjacent spinal levels after fusion, CDA preserves motion at the treated level, potentially mitigating ASD risk.2-4 Furthermore, CDA has been associated with benefits such as lower revision rates, fewer adverse events, and improved clinical outcomes.4-6 Despite these advantages, non-routine discharge, where patients require additional care through rehabilitation facilities or home health services, can contribute to increased healthcare costs and resource utilization. Understanding the factors influencing discharge outcomes is particularly important for elective procedures like CDA, where optimizing recovery pathways and reducing the burden on healthcare systems are key considerations.
Hospital surgical volume plays a critical role in shaping postoperative outcomes. Higher-volume hospitals often demonstrate better results, including lower postoperative mortality and reduced lengths of stay (LOS).7,8 This relationship has been observed in various spine surgeries, such as ACDF and cervical fusions. 9 For instance, Basques et al. reported decreased complications, shorter LOS, and lower costs for ACDF performed by high-volume surgeons.10,11 These findings suggest that institutional experience and familiarity with complex cases can lead to improved care. However, the specific impact of hospital volume on non-routine discharge rates following single-level CDA has not been thoroughly investigated.
Previous studies have shown that higher hospital volume is associated with increased charges and LOS following elective single-level ACDF. 12 However, the relationship between hospital volume and non-routine discharge rates after single-level CDA remains unexplored. This study seeks to address this gap by examining demographic and geographic variations across hospital volumes and assessing their impact on postoperative outcomes for patients undergoing single-level CDA. We hypothesize that high-volume hospitals, compared to intermediate-volume hospitals, will be associated with decreased rates of non-routine discharge, shorter LOS, and reduced hospital costs in patients undergoing single-level CDA.
Methods
Data Collection
The National Inpatient Sample (NIS), covering January 2016 to December 2020, was analyzed alongside cost-to-charge ratio data. This dataset, managed by the Healthcare Cost and Utilization Project (HCUP) under the Agency for Healthcare Research and Quality, is the largest publicly available inpatient database in the U.S., providing regional and national insights into inpatient utilization, access, costs, quality, and outcomes. 13 The NIS includes a 20% sample of inpatient encounters from acute-care hospitals, capturing data that represents over 95% of the U.S. population. 13 Estimates were weighted using HCUP discharge weights, and no institutional review board (IRB) approval was needed due to the public nature of the data.
Patient Population
Patients who underwent single-level cervical disc arthroplasty (CDA) were identified using the International Classification of Diseases, 10th Revision (ICD-10) procedural codes 0RR307Z, 0RR30JZ, and 0RR30KZ. Those who underwent multi-level CDA were excluded if multiple CDA-related ICD-10 codes were recorded during the same hospital admission. Patients under 18 years old were also excluded. The cohorts were categorized by hospital volume: low, intermediate, and high, corresponding to the 25th and 75th percentiles of our dataset. This resulted in a cutoff for low volume being 5 or fewer cases annually, and high volume as 20 or more cases annually. Additionally, non-elective patients and those missing information on sex, race, income quartile, insurance payer, hospital bed size, teaching hospital/location status, total costs, and LOS were excluded. Discharge disposition was categorized as routine (patients discharged to home), non-routine (patients transferred to a short-term hospital, skilled nursing facility, intermediate care facility, or home with healthcare services), and other (patients who left against medical advice, died in hospital, or had an unknown discharge destination). Patients with a discharge disposition categorized as “other” were excluded from the analysis. The predominant insurance payer types included Medicare, Medicaid, and private insurance. Medicare is a federal program that provides coverage for individuals aged 65 and older. Medicaid is a state-administered program that insures individuals with low income. Private insurance is typically obtained through employers or purchased individually. These payer types may influence outcomes by affecting access to elective procedures, discharge planning, and availability of postoperative support services.
Variable Selection
The independent variables collected included age, sex, race, hospital bed size, teaching hospital designation, geographic region, charges, and LOS. Hospital charges were converted to costs using the cost-to-charge ratios from the relevant database. To account for data from multiple years, all costs were inflation-adjusted to 2020 U.S. dollars using specific weighting factors. 14 Patient comorbidities were identified using the Elixhauser comorbidity software, which is adapted for ICD-10-CM codes and provided by HCUP, enabling the identification of 38 pre-existing conditions through secondary diagnoses. 15
Primary Outcome Variables
The primary outcomes analyzed were post-operative medical/surgical complications, categorized as follows: cardiovascular complications (transfusion, venous thromboembolism, acute post-hemorrhagic anemia, myocardial infarction), neurological complications (cerebrovascular accident, nervous system complication, CSF leak/dural tear), surgical complications (dysphagia, mechanical complication, hematoma), and systemic complications (acute kidney injury, sepsis, hypoglycemic episode). Additionally, adverse events were defined as the occurrence of one or more of these complications. Additional outcomes included LOS, total hospital costs, and discharge disposition.
Statistical Analysis
Chi-square tests were used to analyze categorical variables across different hospital volumes, while weighted ANOVA tests assessed continuous variables, such as age and Elixhauser Comorbidity Index (ECI), across volume categories. For outcomes, survey-weighted logistic regression models, adjusted for age, sex, and ECI, were used to evaluate the odds of non-routine discharge and perioperative complications. Comparisons were made using intermediate volume as the reference category to assess both low and high-volume hospitals, and an additional analysis was performed to directly compare high-volume to low-volume hospitals by setting low volume as the reference category. For continuous outcomes, such as LOS and adjusted costs, weighted linear regression was used, also controlling for age and ECI. All statistical analyses were performed in R (version 4.4.0; R Project for Statistical Computing, Vienna, Austria), with significance set at the P < .05 level.
Results
Demographics
A total of 3,868 unweighted cases of CDA, corresponding to 19,340 weighted cases, were identified. After filtering for single-level procedures and applying exclusion criteria, 2,863 unweighted cases, corresponding to 14,315 weighted cases, remained. The mean age of patients varied slightly across hospital volumes, with high-volume hospitals showing a significantly older patient population with a mean age of 49.4 years compared to low- and intermediate-volume hospitals (46.9 and 47.1 years, respectively; P < .001). The distribution of race, sex, and income quartiles, showed no significant differences between hospital volume categories (P > .05 for all).
Baseline Demographic Characteristics Stratified by Hospital Volume.
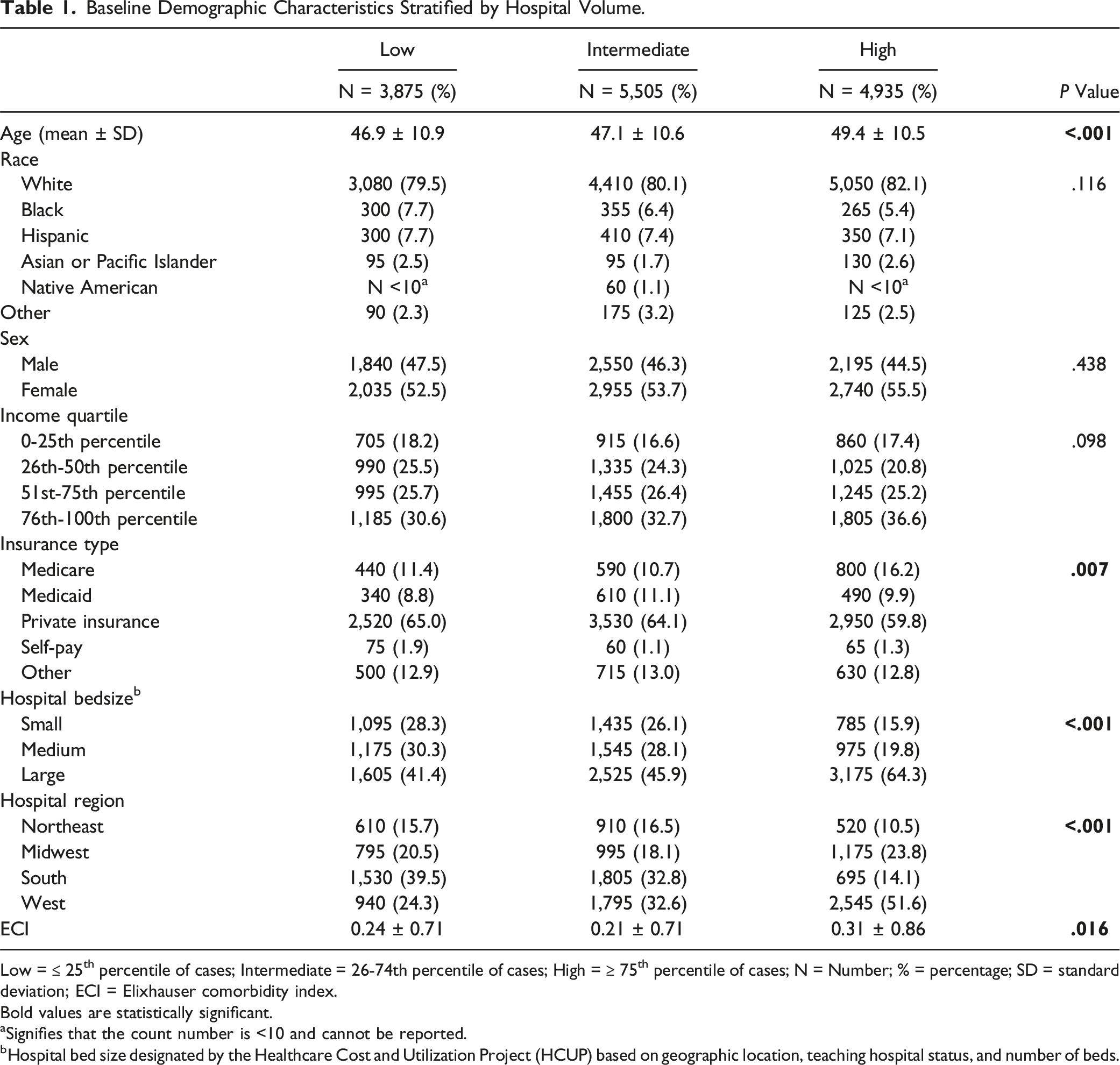
Low =
Bold values are statistically significant.
aSignifies that the count number is <10 and cannot be reported.
bHospital bed size designated by the Healthcare Cost and Utilization Project (HCUP) based on geographic location, teaching hospital status, and number of beds.
Perioperative Complications
Multivariate Logistic Regression Analysis of Complications and Hospital Course Between Hospitals Based on Volume.
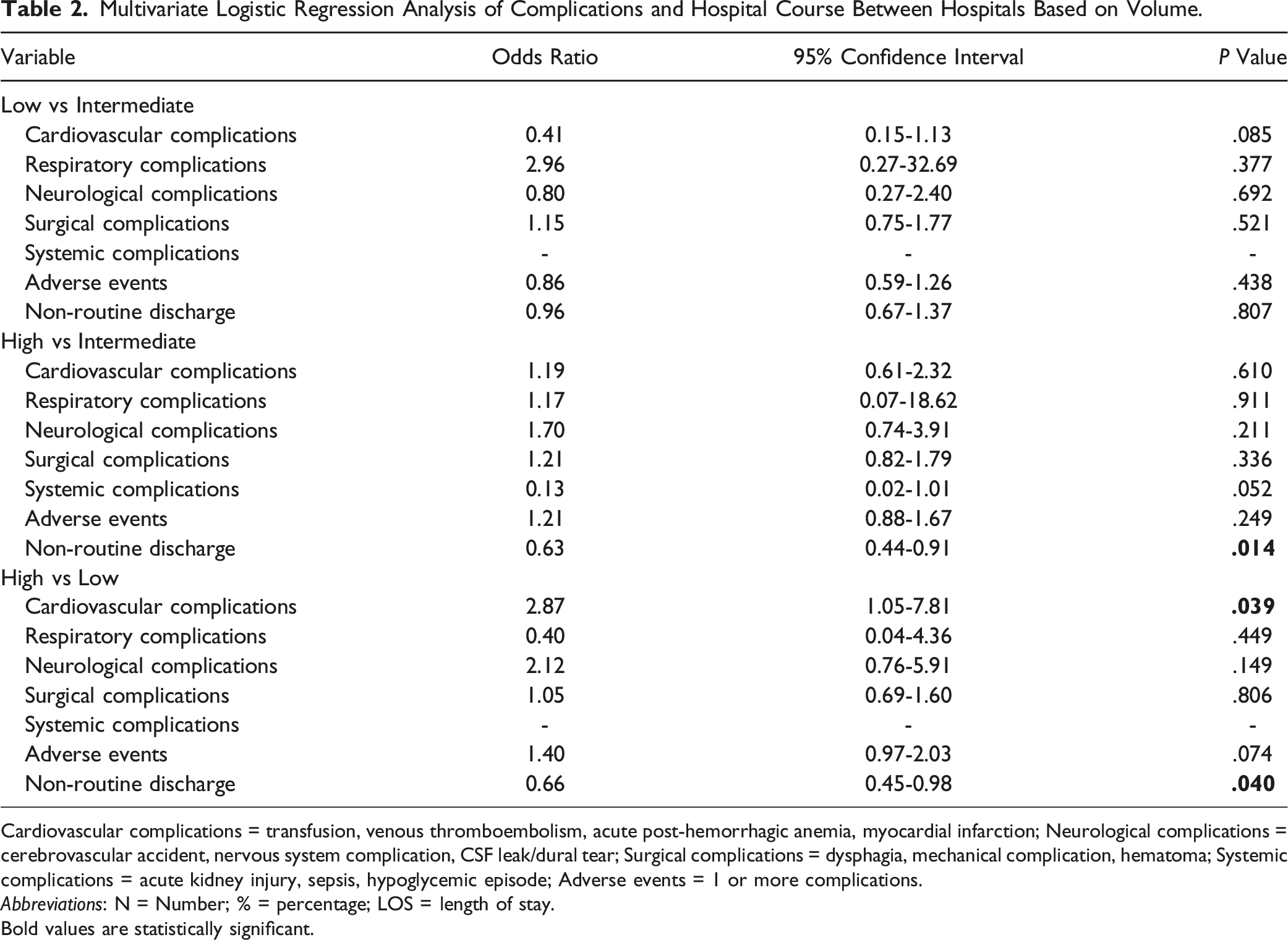
Cardiovascular complications = transfusion, venous thromboembolism, acute post-hemorrhagic anemia, myocardial infarction; Neurological complications = cerebrovascular accident, nervous system complication, CSF leak/dural tear; Surgical complications = dysphagia, mechanical complication, hematoma; Systemic complications = acute kidney injury, sepsis, hypoglycemic episode; Adverse events = 1 or more complications.
Abbreviations: N = Number; % = percentage; LOS = length of stay.
Bold values are statistically significant.
Hospital Course
Multivariate Linear Regression Analysis of Total Hospital Cost and Length of Stay Between Hospitals Based on Volume.
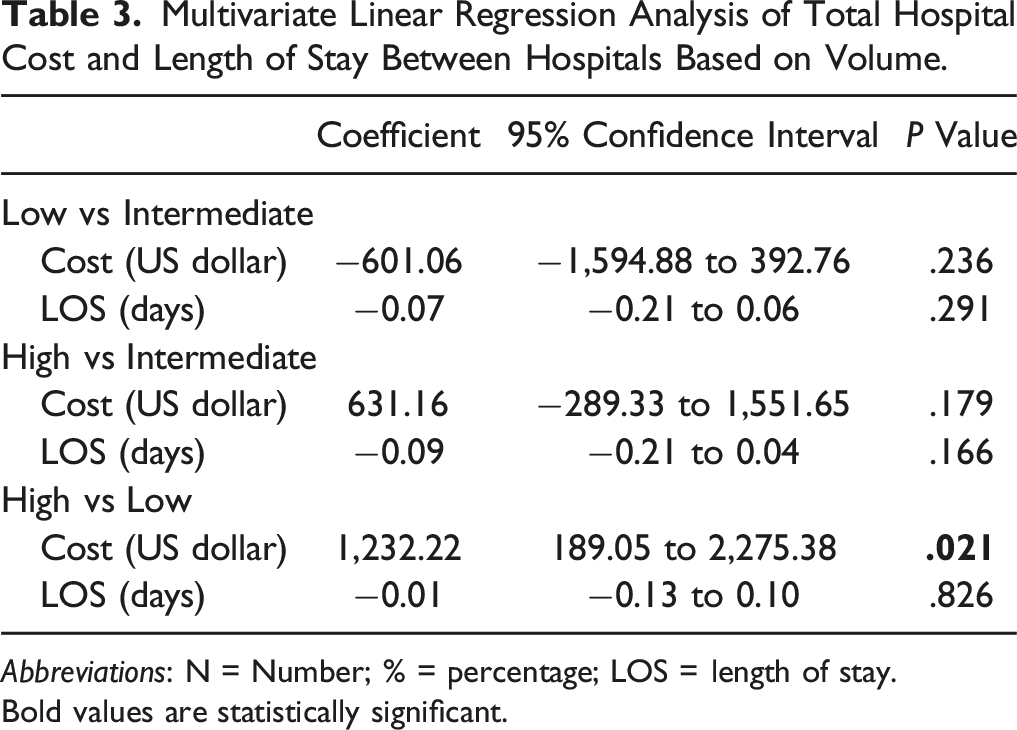
Abbreviations: N = Number; % = percentage; LOS = length of stay.
Bold values are statistically significant.
Discussion
As the demand for CDA continues to rise, understanding the factors that influence postoperative outcomes has become increasingly critical. In particular, the impact of hospital volume on outcomes such as discharge disposition, length of stay, and cost remains an area of ongoing investigation. This study provides important insights into the relationship between hospital volume and postoperative outcomes following single-level CDA. We found that high-volume hospitals were associated with a lower likelihood of non-routine discharge compared to intermediate-volume hospitals, emphasizing the critical role of institutional experience and resources in optimizing discharge outcomes. However, our results also revealed that high-volume hospitals incurred significantly higher costs, underscoring the complexity of balancing resource utilization with improved care quality.
Patients treated at high-volume hospitals had a 37% lower odds of non-routine discharge compared to those treated at intermediate-volume centers and a 34% lower odds compared to those treated at low-volume centers, underscoring the critical influence of institutional factors on recovery quality. Non-routine discharge has long been recognized as a significant determinant of recovery outcomes, contributing to increased healthcare costs, prolonged recovery periods, and higher rates of readmissions.16-18 While previous studies have highlighted patient-level factors, such as advanced age, comorbidities, and functional status, as predictors of non-routine discharge, our findings underscore the importance of hospital-specific factors, including case volume and the infrastructure available at high-volume centers. 19 These facilities often benefit from multidisciplinary teams, standardized care protocols, and enhanced perioperative support systems, all of which likely contribute to their superior discharge outcomes. Disseminating these practices across lower-volume centers could play a pivotal role in reducing disparities in patient outcomes. Implementing targeted training programs, enhancing access to centralized clinical resources, and fostering partnerships with high-volume centers could facilitate the transfer of best practices. These strategies may enable lower-volume centers to replicate the systemic efficiencies and care quality observed in high-volume hospitals, ultimately improving outcomes across diverse healthcare settings.
The higher costs observed at high-volume hospitals contrast with existing literature, which often associates increased surgical volume with lower costs due to economies of scale.9-11 This discrepancy may be attributed to several factors specific to CDA. High-volume centers may manage more complex CDA cases, such as those involving high-risk patients with advanced comorbidities, requiring additional intraoperative and perioperative resources. Furthermore, the use of advanced motion-preserving implants, which are integral to CDA, may increase procedural costs compared to fusion techniques. Differences in regional healthcare practices, reimbursement structures, and case mix may also contribute to these cost variations. Importantly, the potential downstream costs associated with non-routine discharges—such as rehabilitation and readmissions—might offset the upfront savings observed at lower-volume centers. For example, Passias et al reported higher overall costs for patients discharged to rehabilitation facilities compared to those discharged home, highlighting the financial implications of suboptimal discharge pathways. 19 Tailoring efforts to optimize care pathways for CDA specifically could mitigate these cost discrepancies and enhance value across all hospital volumes.
The absence of significant differences in complication rates across hospital volume categories in our study is noteworthy, suggesting that hospital volume may not directly impact the occurrence of perioperative complications but rather influences the management and downstream outcomes of these events. While our findings did not show significant differences, the broader literature offers mixed insights. For instance, a systematic review evaluating outcomes following spine surgeon based on hospital volume by Adkins et al. reported a lower incidence of complications for surgeries performed in high-volume hospitals. 20 Specifically, Farjoodi et al. reported that lower hospital volumes were associated with higher postoperative complications in lumbar spine surgeries. 21 Similarly, Blais et al. reported higher complication rates for lower-volume surgeons in cervical spine surgeries but found no significant association with hospital volume in the same dataset. 22 However, other studies found no significant association between complication rates and hospital volume. These findings suggest that managing complications effectively, rather than focusing only on preventing them, may be key to improving outcomes in CDA. Efforts should focus on implementing standardized care protocols, improving resource use, and ensuring strong communication among care teams to enhance recovery pathways, regardless of hospital volume.
This study has several limitations inherent to using large administrative datasets like the NIS. Coding inconsistencies and clerical errors may introduce bias, and the absence of critical patient-level data, such as BMI, functional status, pre-admission living conditions, and detailed comorbidity histories, limits the depth of analysis. Additionally, the lack of surgeon-specific data and outpatient cases—where most CDA procedures occur—restricts the generalizability of our findings. Variability and errors in coding and reporting rates further challenge the reliability of the dataset, as does the absence of clear indications for CDA procedures. The dataset also does not capture longer-term outcomes or patient-reported outcome measures, which are critical for evaluating the full impact of CDA. Moreover, the inability to quantify costs with greater precision and analyze their contributing factors limits the study’s implications for economic evaluations. The dataset also does not capture longitudinal outcomes, such as 30-day readmissions, or provide insight into regional variations in healthcare delivery and costs. Future research should incorporate outpatient and longitudinal data to better evaluate the relationship between hospital factors, discharge outcomes, and healthcare costs.
Conclusions
This study underscores the significant influence of hospital volume on postoperative outcomes following single-level CDA. Patients treated at high-volume hospitals experienced lower rates of non-routine discharge, highlighting the potential benefits of institutional practices, such as standardized care protocols and multidisciplinary teams, in improving discharge outcomes. However, the association between high hospital volume and increased costs warrants further investigation to identify the mechanisms driving these expenses and to ensure cost-effectiveness alongside improved care quality. Understanding and disseminating the practices of high-volume hospitals could help optimize care delivery across diverse healthcare settings. Future research should aim to expand upon these findings by incorporating outpatient data and evaluating the long-term impact of hospital-specific factors on patient outcomes and healthcare costs.
Footnotes
Declaration of Conflicting Interests
Mitchell K. Ng is a paid consultant at Johnson & Johnson Ethicon Inc., Pacira BioSciences Inc., Sage Products Inc., Alafair Biosciences Inc., Next Science LLC, Bonutti Technologies Inc., Hippocrates Opportunities Fund LLC, and Ferghana Partners Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
No IRB approval was required for performance of this review.