
Abstract
Study Design
Retrospective cohort study.
Objectives
As of 2022, the Centers for Medicare and Medicaid Services does not provide nationwide coverage for cervical disc arthroplasty (CDA). The aim was to determine whether Medicare beneficiaries have differences in: (1) lengths of stay (LOS); (2) complications; (3) readmissions; and (4) costs of care.
Methods
Using the 2010 to 2020 PearlDiver database, we queried patients undergoing primary CDA for degenerative disc pathology. Study groups patients were those undergoing CDA with Medicare coverage (n = 1467); patients without Medicare coverage were the comparison cohort (n = 15,389). Endpoints were to compare demographics and comorbidities within the Elixhauser comorbidity index (ECI), LOS, 90-day complications, 90-day readmissions, and 90-day reimbursements. A multivariate logistic regression was used to calculate odds (OR) of medical complications and readmissions within 90-days. A P-value less than .003 was significant.
Results
Patients with Medicare coverage undergoing CDA had higher mean ECI compared to alternative payers (5.24 vs 3.26; P < .0001). Mean LOS was significantly higher for Medicare beneficiaries (2.20 vs 1.76 days; P < .010). There was no significant differences in odds of all medical complications (OR: 1.19, 95% CI: .98-1.44; P = .069) or readmission rates (1.77% vs 1.33%, OR:0.82, 95% CI: .50-1.29; P = .417) within 90-days following the index procedure among Medicare beneficiaries vs alternative payers. Non-Medicare beneficiaries had higher 90-day reimbursements compared to Medicare beneficiaries ($6,700 vs $7,086,P < .001).
Conclusions
Medicare beneficiaries despite having slightly longer lengths of stay did not have higher rates of medical complications or readmissions. Surgeons and policy makers may use this data to consider alternative treatments in Medicare patients.
Keywords
Introduction
Cervical disc arthroplasty (CDA) is a motion sparing procedure for degenerative cervical disc pathology, performed in younger patients aimed at improving clinical outcomes while preventing adjacent segment disease.1-3 Because this surgery is focused on the younger, active patient population with 1-2 level cervical disc degeneration, implant longevity and complications become imperative for spine surgeons to study. CDA complications arise in the form of implant wear, heterotopic ossification, and implant failure due to subsidence or migration.2,4,5 These complications ultimately require revision surgery. 6 Due to unknown implant longevity and long-term success of CDA, the historical gold standard, anterior cervical discectomy and fusion (ACDF) has been the favored procedure. Additionally, CDA has historically been disincentivized by Medicare due to the proposed higher costs. Despite a lack of nationwide Medicare Coverage by the Centers for Medicare and Medicaid Services (CMS) for CDA, the utilization of this procedure has risen in popularity over the last decade. To aid in patient counseling, the economics and complications of this surgical option should be further understood as its utilization in younger patients as well as patients over 65 has been increasing nationwide.
Multiple randomized controlled trials have compared the efficacy, complications, and patient reported outcomes following anterior cervical discectomy and fusion (ACDF) vs CDA.7-15 As spine surgeons become more comfortable utilizing CDA within their practices, the annual healthcare utilization is impacted. Studies assessing primary and revision CDA procedural volume and complications are largely outdated and limited to periods prior to 2015.16-20 With cervical spine surgical volumes including ACDF expected to increase by 13-19% by 2040, a comparison of outcomes between different payer mixes may help spine surgeons as they broaden the indications and utilization of CDA. 21
In light of the increased utilization of CDA nationwide, the purpose of this study was to utilize an administrative claims database from 2010 to 2020 to compare outcomes between Medicare beneficiaries vs alternative payers. We aimed to determine whether Medicare beneficiaries undergoing CDA have differences in: (1) lengths of stay (LOS); (2) medical complications; (3) readmission rates; and (4) costs of care.
Materials and Methods
Database and Patient Inclusion
A retrospective query was performed from January 1st, 2010 to October 31st, 2020 using an insurance claims database from the subscription based PearlDiver Platform (www.pearldiver.com; PearlDiver Technologies; Fort Wayne, Indiana, USA). The database, comprised of over 150 million patients, is housed within a proprietary user interface available for researchers to design detailed research queries related to patient demographics, surgical complications, healthcare expenses, and more. Records and individual patient visits are from those insured nationally from Medicare in addition to the private insurance company known as Mariner. After tailoring a research query, researchers define cohorts of interest utilizing Current Procedural Terminology (CPT) codes, International Classification of Disease, Ninth Revision (ICD-9), ICD-10 diagnostic and procedural codes, Diagnostic Related Group codes, and National Drug Codes. Information is subsequently extracted as a text (.TXT) file for manipulation and statistical processing. The database is unable to report granular details that would compromise patient identity, therefore this Health Insurance Portability and Accountability Act (HIPAA) compliant study was exempt from institutional review board (IRB) approval.
Comparison of Baseline Demographics Among Medicare Beneficiaries vs Other Payers for Primary Cervical Disc Arthroplasty.
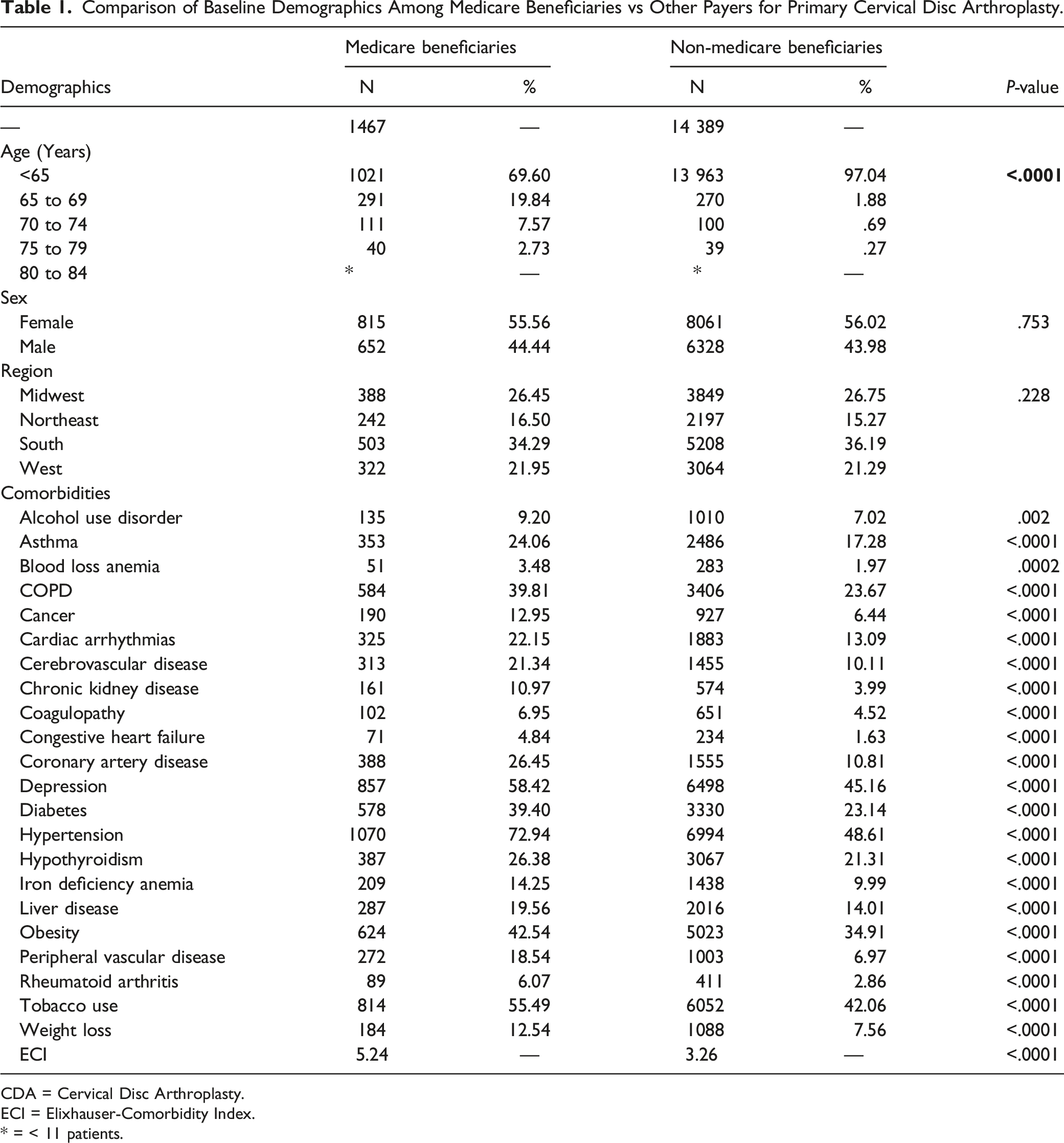
CDA = Cervical Disc Arthroplasty.
ECI = Elixhauser-Comorbidity Index.
* = < 11 patients.
Primary Outcomes
The primary endpoints of this study were to compare patient demographics, in-hospital lengths of stay, 90-day medical complications, 90-day readmissions, in addition to day of surgery and total global 90-day episode of care reimbursements between the 2 groups. Baseline demographics of the cohorts analyzed included age, sex, geographic variation, and presence of individual medical comorbidities comprising the Elixhauser-Comorbidity Indices (ECI). 22 Length of stay was compared between Medicare beneficiaries vs alternative payers. Economic reimbursements were conducted by analyzing reimbursements to the surgeon on the day of surgery and during the 90-day episode of care interval, as this standard has been established in previously published studies.23,24 All reimbursements were adjusted for inflation to 2020 U.S. Dollars (USD).
Statistical Analysis
The baseline categorical demographics of age, sex, geographic distribution, and prevalence of comorbidities were compared using Pearson’s Chi-Square analyses. A multivariate logistic regression model was used to calculate odds (OR) and 95% confidence intervals (95%CI) of developing medical complications and being readmitted within 90-days following CDA adjusting for sex, geographic region, and the Elixhauser-Comorbidity Index (ECI). All variables were entered into the model and chosen as they have been demonstrated to be risk factors for outcomes in spine patients.25,26 For continuous variables such as expenditures and lengths of stay, a Shapiro-Wilk test for normality of distribution was carried out, followed by comparison using a student’s t-test. Following a Bonferroni-correction, a P-value less than .003 was considered statistically significant. Data analyses were performed using the open programming language known as R (R, Foundation for Computational Statistics; Vienna, Austria).
Results
Baseline Demographics
In the entire cohort undergoing primary CDA, 2.62% were 65 years of age or older. CDA utilization between sexes and within different regions of the United States were comparable between Medicare beneficiaries vs alternative payers, Table 1. CDA utilization was greatest within the Southern United States, followed by the Midwest. Patients with Medicare coverage undergoing CDA had significantly higher mean ECI compared to alternative payers (5.24 vs 3.26; P < .0001), Table 1.
In-Hospital LOS, Complications, and Readmissions
Mean LOS was significantly higher for Medicare beneficiaries (2.20 vs 1.76 days), P < .010. There was no significant differences in odds of all medical complications (OR: 1.19, 95% CI: .98 – 1.44, P = .069) within 90-days following the index procedure among Medicare beneficiaries compared to alternative payers, Figure 1. Only surgical site infections (OR: 4.40, 95% CI: 1.98 – 9.75, P = .0003) were higher in Medicare patients, Figure 1. Remaining 90-day complications did not have increased incidence and odds within the Medicare population. Additionally, 90-day readmission rates were similar between study and comparison cohorts (1.77% vs 1.33%, OR:0.82, 95% CI: .50-1.29, P = .417, Figure 1. Forest Plot depicting odds ratios of 90-day medical complications and readmissions among Medicare beneficiaries vs other payers. Non-medicare payers are the referent. logistic regression model was controlled for by gender, geographic region, and elixhauser comorbidity index. surgical site infections were the only medical complication significantly higher in medicare beneficiaries.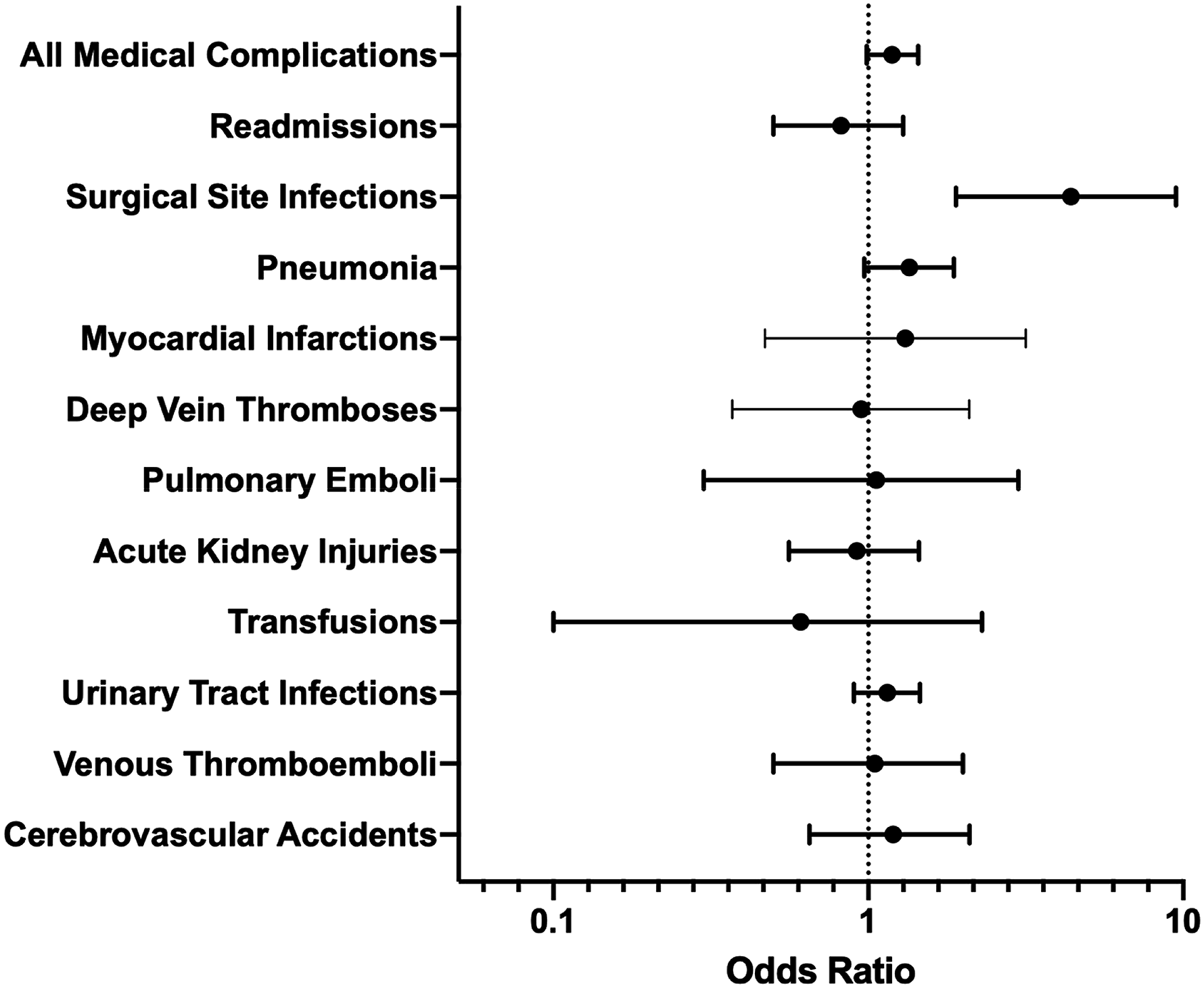
Reimbursements
Non-Medicare beneficiaries had significantly higher 90-day reimbursements compared to Medicare beneficiaries ($6,700 vs $7,086), P < .001.
Discussion
As healthcare utilization and expenditures within spine surgery continue to rise in the United States, it is critical to evaluate procedural utilization, complications, and reimbursements of common procedures within the specialty. Using a private all claims insurance database we evaluated patient demographics, complications, and cost differences in patients with Medicare coverage vs alternative insurance coverage. The main findings of our study demonstrate that despite having slightly longer lengths of stay, Medicare beneficiaries did not have higher rates of 90-day medical complications or readmissions rates. These findings are important as the utilization of CDA expands.
The most important findings of our study compared the 90-day complication and readmission rates between the different insured groups. Of the complications assessed, there were only significant differences in surgical site infections. This could be due to older populations insured by Medicare being less independent, and thus could explain these findings. Without the ability to have proper wound care postoperatively, these patients may be at increased risk for SSI. In a systematic review of SSI among patients undergoing spine surgery, diabetes, obesity, increased length of stay, and hypertension were some of the notable risk factors. 27 In our study, Medicare insured patients had all of these risk factors at greater frequencies compared to the control cohort. The most commonly reported adverse events following cervical spine surgery including CDA include radicular symptoms, dysphagia, all cause readmissions, vascular compromise, dural injury, and cervical wound infection.28,29 Despite, these commonly reported complications, Medicare beneficiaries in our study did not have increased incidence or odds of transfusions or all cause readmissions after controlling for comorbidity burden. With the number of ACDFs estimated to rise by 15% by the year 2040, CDA may become more favorable among spine surgeons. 21 It is possible that as the familiarity increases with newer CDA implants and techniques, spine surgeons have demonstrated better technique leading to improved complication rates. With 2 well established procedures for degenerative cervical disc disease, spine surgeon preference may be influenced by other patient specific factors as well. Undergoing surgery for cervical disc disease is a complex consideration for patients and spine surgeons alike. We show that despite an increased patient comorbidity burden of Medicare beneficiaries undergoing primary CDA overall 90-day complications and all cause readmissions were similar to younger privately insured patients.
Historically, Medicare has been resistant to covering cervical disc arthroplasty nationwide with ACDF being a well-established surgical option. In this study, we showed modest $400 difference in total 90-day reimbursements for privately insured patients. In a Markov model analysis of a prospective, randomized, multi-center investigation of the Mobi-C Cervical Disc Prosthesis, both ACDF and CDA were determined to be cost effective treatments for degenerative disc pathology of the cervical spine within 7 years of the primary surgery. 30 However, CDA was superior in the authors’ estimation. This is of importance as spine surgeons consider the increased utilization of CDA and providing appropriate counseling to their patients. In the context of our study, as of 2022 there is no nationwide Medicare Coverage by the Centers for Medicare and Medicaid Services (CMS) for CDA, despite the utilization of this procedure rising in popularity. This begs the question of whether CDA should be covered by Medicare nationwide given the favorable patient reported outcomes and increased utilization nationwide. In a study using data from 2012 to 2017, Lopez et al 31 tracked the trends in ACDF utilization of 265,000 Medicare enrollees. They reported that ACDF procedures increased from 8.0 surgeries per 10,000 Medicare beneficiaries in 2012 to 8.5 per 10,000 Medicare beneficiaries in 2017. Of those which received an ACDF, there may exist a proportion of cervical spine surgery patients of low risk and low comorbidity burden that may benefit from CDA over ACDF via careful selection. Updated projections evaluating low-risk ACDF patients over 65 years of age would represent a next step in identifying how many Medicare enrollees truly could benefit from this motion sparing procedure. Bundling of payments for spine surgery have yet to be universally successful given the heterogeneity of patient population, payer mix, and surgical technique. 32 Ideally value-based care has strived to incorporate financial risk sharing among hospitals and surgeons and prioritize reducing costs. Surgeons inherently have major disincentives which could lead providers and/or hospitals to “cherry-pick” patients with low comorbidity burden to decrease risk. Furthermore, this may lead to lack of access to care for certain groups of patients, notably the elderly patient population. Future investigation into reimbursements and the proportion delegated for surgeons, hospitals, and ancillary staff is needed to better understand the discrepancies in 90-day costs after CDA. Prior studies have shown that facility costs, which include surgical implants, length of inpatient stays, and operating room time, are responsible for nearly 75% of reimbursements for lumbar fusion. 33 Further study may evaluate if similar findings are seen for ACDF and CDA.
There are some limitations to this study that merit discussion. Use of large insurance claims database for research purposes may introduce selection bias and it is possible that our sample is merely a proportion of the nationwide sample undergoing primary CDA. We could not report or control for granular details including surgeon fellowship training, implant characteristics, hospital characteristics, or surgical technique which all have been shown to influence cervical spine complications. The data for this study was queried using ICD-9/ICD-10 diagnostic and procedural codes in addition to CPT codes. Originally these codes were not developed for research purposes and therefore may be subject to errors in diagnosis, coding, or billing and may alter the findings of our study. For instance, we could not reliably control for 1 level CDA with the use of ICD-9 procedural coding, and thus there may be a small proportion of the cohort which had more than 1 level. However, over 82% of the patient sample in this study underwent CPT-22856 (Single level CDA). Hospital reimbursements are the amount paid to the hospital and surgeons for a particular procedure and is subject to variability across regions of the United States. 34 Another limitation is related to the granularity of the reimbursements and what was directly responsible for the greater costs in the non-Medicare beneficiaries. We could not further evaluate the individual reimbursements to hospitals, spine surgeons, and anesthesiologists which would help answer important questions. Despite the limitations of this retrospective database study, it is the first study of its kind to compare the surgical outcomes among Medicare beneficiaries vs alternative payers for CDA.
Conclusion
This study demonstrates that Medicare beneficiaries despite having slightly longer lengths of stay did not have higher rates of medical complications or readmissions rates. The study is vital as it can be utilized by spine surgeons to consider alternative treatments in Medicare patients for cervical degenerative disc pathology. Based on these data, further policy changes and re-evaluations may be warranted to increase the indications for cervical disc arthroplasty.
Ethical committee statement: This study was determined to be exempt from the Institutional Review Board (IRB) of Maimonides Medical Center.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.