
Abstract
Study Design:
Retrospective study.
Objective:
To examine the associated indications, procedures, and postoperative outcomes after revision ACDA.
Methods:
We utilized a national database to identify adult(≥18 years) patients who underwent either a primary ACDA or removal of ACDA over a 10-year period(2008-2017). An in-depth assessment of the reasons for revision surgery and the subsequent procedures performed after the removal of ACDA was done by using both Current Procedural Terminology(CPT) and International Statistical Classification of Diseases (ICD-9,10) coding.
Results:
From 2008 to 2017, a total of 3,350 elective, primary ACDA cases were performed. During this time, 69 patients had a revision surgery requiring the removal of ACDA. The most common reasons for revision surgery included cervical spondylosis(59.4%) and mechanical complications(27.5%). After removal of ACDA, common procedures performed included anterior cervical fusion with or without decompression(69.6%), combined anterior/posterior fusion/decompression (11.6%), and replacement of ACDA (7.2%). The indications for surgery did not vary significantly among the different procedures performed (p = 0.318). Patients requiring revision surgery for mechanical complications or those who underwent a combined surgical approach were at significantly higher risk for subsequent short-term complications (p<0.05).
Conclusion:
Over a 10-year period, the rate of revision surgery for ACDA was low (2.1%). Nearly 90% of revision cases were due to either cervical spondylosis or mechanical complications. These indications for surgery did not vary significantly among the different procedures performed. These findings will be important during the shared-decision making process for patients undergoing primary or revision ACDA.
Keywords
Introduction
Cervical degenerative disease (CDD) is most commonly treated with decompression and fusion, which has demonstrated successful outcomes; however, there is concern that fusion might lead to accelerated degeneration of adjacent levels of the spine.1,2 As a result, anterior cervical disc arthroplasty (ACDA) has emerged as a motion-sparing alternative to anterior cervical discectomy and fusion (ACDF). Over the last 2 decades, numerous studies have demonstrated comparable outcomes between these 2 procedures.3-9 In a recent systematic review, Findlay et al found that ACDA is at least as effective as ACDF at mid- to long-term follow-up (4-7 years) for most patient-reported and clinical outcomes, and concluded a reduced risk for adjacent segment disease with up to a 10-year follow-up. 7
Despite these encouraging results, ACDA is not free of complications or the possibility of reoperation. Prior studies have reported reoperation rates as low as 0.4-0.6% (30-day follow-up) and as high 3-15% (5-year follow-up).5,10-14 Many of these studies are comparative analyses between primary ACDA and other procedures and, as a result, do not focus on the outcomes after revision ACDA. Furthermore, it is unclear what the failure rate is for the ACDA implants since the cause for revision surgery is not well-defined in many studies; a revision surgery for a wound debridement is not the same as a secondary surgery requiring the removal of ACDA.
In comparison to prior literature, this study uses a national database to focus on revision ACDA patients. We define revision surgery as the removal of the primary ACDA implant. The purpose of this study is to examine the associated indications, secondary procedures, and postoperative outcomes after revision surgery for ACDA failure. No prior study has focused on this population at a national level.
Materials and Methods
Database
The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was used in this study. This database contains a comprehensive set of patient factors, operative conditions, and postoperative outcomes up to 30 days after surgery. These are Health Insurance Portability and Accountability Act (HIPAA) compliant, de-identified data from over 700 sites participating in NSQIP. Current 2017 NSQIP contains more than 1 million patient encounters. In comparison to administrative billings data, this dataset was created with the intent to improve the quality of care for surgical patients. Therefore, several quality assurance mechanisms (e.g. data collection by highly trained surgical clinical reviewers, a systematic sampling process to control for selection bias, random audits, exclusion of any participating site with an inter-rater reliability disagreement rate >5%) are in place to ensure data of the highest quality. 15
Population Definitions
The NSQIP database was queried to identify adult (≥18 years) patients who underwent either a primary ACDA (Current Procedural Terminology [CPT]: 22856, 22858) or removal of ACDA (CPT: 22864) over a 10-year period (2008-2017). A detailed definition for each cohort can be seen below: Primary ACDA: Any patient with a principal CPT 22856 (Total disc arthroplasty, anterior approach, including discectomy with endplate preparation, single interspace; cervical), CPT 22858 (Total disc arthroplasty, anterior approach, including discectomy with end plate preparation; second level, cervical). These patients did not have a concurrent CPT for removal of ACDA. Revision ACDA: This cohort was defined as having any CPT for the removal of an ACDA – CPT 22864 (Removal of total disc arthroplasty (artificial disc), anterior approach, single interspace; cervical. To account for the number of levels removed, concurrent CPT 0095 T was used (Removal of total disc arthroplasty (artificial disc), anterior approach, each additional interspace, cervical.
The International Statistical Classification of Diseases and Related Health Problems (ICD) codes were used to define the indications for revision ACDA surgery. Both ICD-9 (prior to 2016) and ICD-10 (2016-2017) codes were used. The main categories included cervical spondylosis (with myelopathy [ICD9 – 721.1, 722.71; ICD10-M47.12, M47.13, M50.00], with radiculopathy [ICD10 – M47.22, M47.23, M50.12, M54.12], without myeloradiculopathy [ICD9-721.0, 722.0, 722.4; ICD10-M47.812, M47.813]), mechanical complications (dislocation [ICD9-996.42; ICD10-T84.029A], displacement [ICD10-T84.226A, T85.628A], other mechanical [ICD9-996.2, 996.47, 996.49, 996.59, 996.78, 996.79; ICD10-T84.84XA, T84.89XA]), acquired deformity (ICD9-737.19), trauma (ICD10-M48.32), and other (ICD9-723.4, 723.8).
Secondary procedures after the removal of ACDA included anterior cervical fusion, combined anterior and posterior approach, and replacement of ACDA. The anterior cervical fusion group included those with decompression (CPT 22551 with a concomitant CPT 22552 for each additional interspace) and without decompression (CPT 22554 with a concomitant CPT 22585 for each additional level). The combined anterior and posterior group included either those with anterior fusion and posterior decompression (anterior cervical fusion CPT codes (as above) with posterior decompression CPT codes: 63001, 63015, 63020, 63040, 63045) or anterior and posterior fusion with decompression (anterior cervical fusion CPT codes (as above) with posterior cervical fusion CPT codes: 22600, 22614, 22842). The ACDA replacement cohort was defined by the CPT code 22861 (Revision including replacement of total disc arthroplasty (artificial disc), anterior approach, single interspace; cervical). For additional levels, this cohort included CPT 0098 T (Revision including replacement of total disc arthroplasty (artificial disc), anterior approach, each additional interspace, cervical). Other concomitant operative factors included corpectomy (63081, 63082), interbody device (22851, 22853, 22854), autograft (20936, 20937, 20938), allograft (20930, 20931).
Patient Characteristics and Outcomes
Clinical variables included patient age, sex, body mass index (BMI), and an extensive list of comorbidities. “Other_Race” included Asian, American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, or Unknown/Not Reported. The comorbidity profile was examined with the Charlson Comorbidity Index (CCI) and American Society of Anesthesiologists (ASA). Outcome and complication data was collected up to 30 days after surgery. The “Any Complication” variable does not include readmissions or reoperations; instead, these included death, wound complication (superficial surgical site infection [SSI], deep SSI, wound dehiscence, organ space SSI), pulmonary complications (pneumonia, unplanned intubation, ventilator use >48 hours), deep venous thrombosis/pulmonary embolism (DVT/PE), acute renal failure, urinary tract infection (UTI), stroke/cerebrovascular accident, cardiac complications (cardiac arrest requiring CPR, myocardial infection), perioperative transfusion (intraoperative and up to 72 hours postoperative), and sepsis. Unplanned 30-day readmissions included unplanned 30-day reoperations in our analysis. “Extended” length of hospital stay was defined as >2 days.
Statistical Analysis
The 30-day outcomes (e.g. Any complications, unplanned readmissions, extended LOS) after revision surgery was compared among different indications and revision procedures in the bivariate analyses. Chi-square or Fisher’s exact test (where appropriate) and t-tests/ANOVA were used for categorical and continuous variables, respectively. Statistical significance was defined as P-value <0.05. SAS software (Version 9.3; SAS Institute Inc, Cary, NC) was used for all statistical analyses.
Results
From 2008 to 2017, a total of 3,350 elective, primary ACDA cases were performed. During this time, 69 patients had a revision surgery requiring the removal of the ACDA (10-year ratio of total revision cases / total primary cases = 2.1%) (Figure 1). Revision patients were older (mean age (±standard deviation) = 48.5 ± 11 years) and more often female (60.9%, N = 42) than primary cases (age = 45.6 ± 10.2, p = 0.019; female = 46.9% (N = 1571), p = 0.022), but the comorbidity burden was similar between these cohorts (revision: CCI = 0.7 ± 1.1, ASA >2 = 26.1% vs primary: CCI = 0.52 ± 0.81 p = 0.066, ASA >2 = 21.2% p = 0.323). Revision cases (operative time: 157 ± 104 minutes) were nearly 45 minutes longer than primary cases (operative time: 111 ± 52.1 minutes, p<0.001), were less often outpatient (27.5% vs. 43.5%, p = 0.008), and required nearly 2.5 additional days in the hospital (p<0.001) (Table 1).
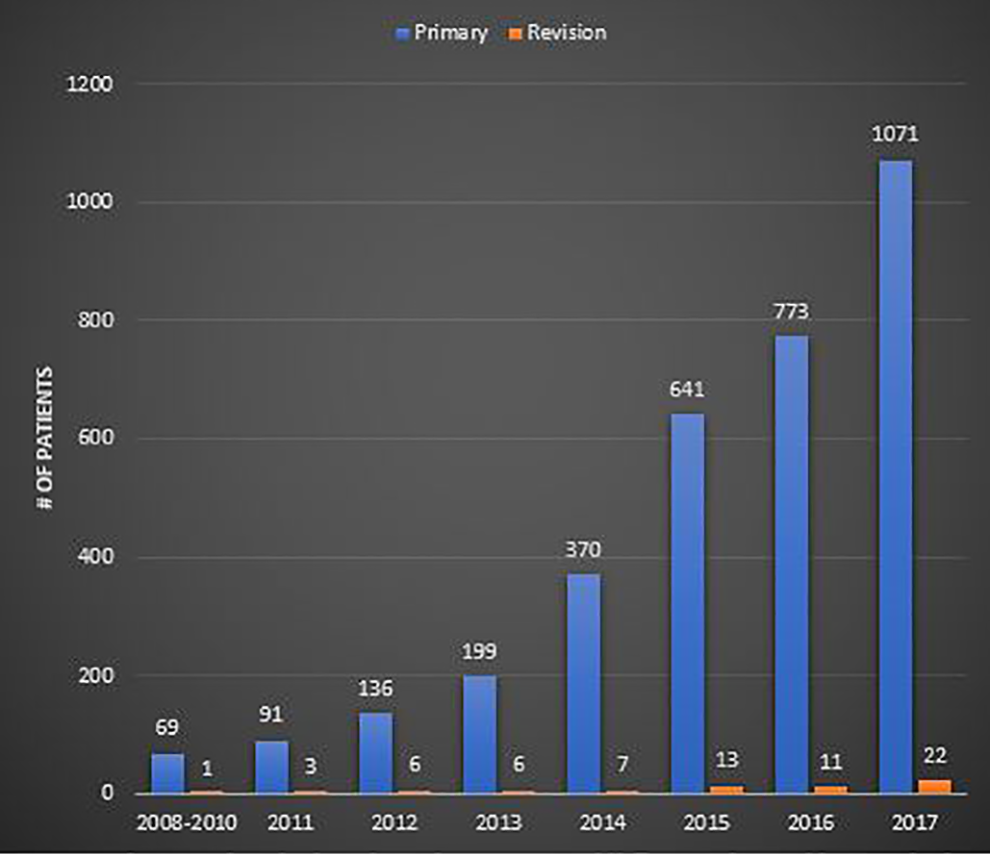
Distribution of the number of primary ACDA and Revision cases by year (from 2008 to 2017).
Patient and Clinical Factors for Primary and Revision ACDA (2008-2017).
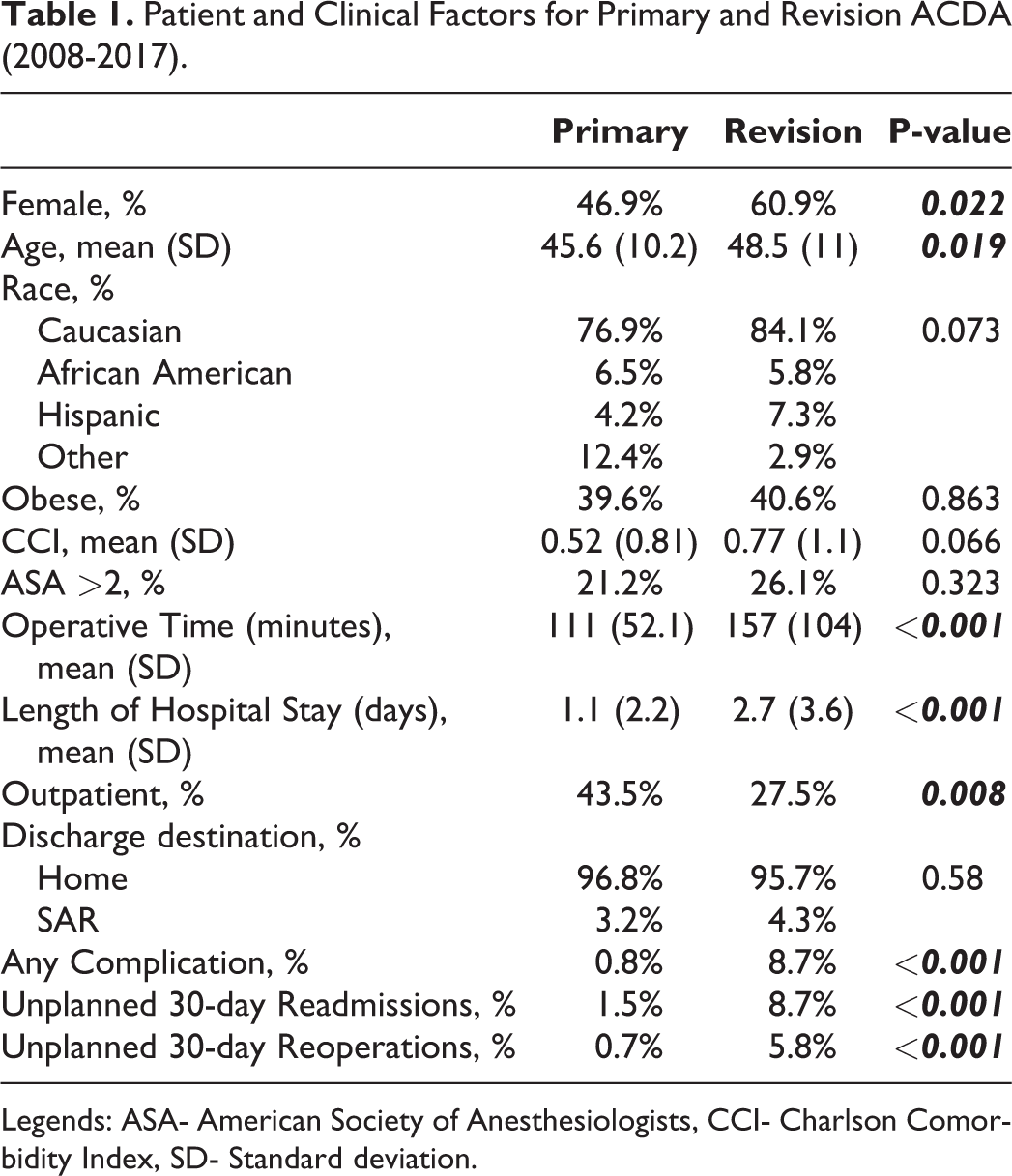
Legends: ASA- American Society of Anesthesiologists, CCI- Charlson Comorbidity Index, SD- Standard deviation.
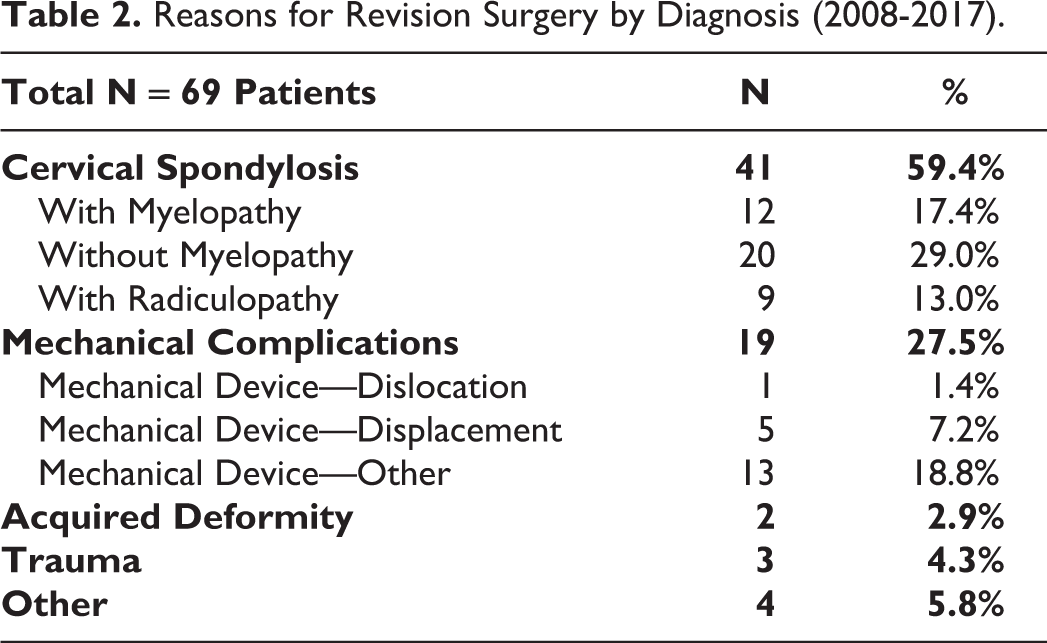
The most common reasons for revision surgery included cervical spondylosis (59.4%, N = 41) and mechanical complications (27.5%, N = 19). Based on the Cochran-armitage trend test, no significant trend in the indications for revision surgery occurred over time (p-value = 0.090) (Figure 2). About half of those presenting with cervical spondylosis had either myelopathy or radiculopathy (N = 21). Nearly a third of those with mechanical complications had either a dislocation or displacement of the ACDA (N = 6). Other indications for revision surgery included acquired deformity (2.9^%, N = 2) and trauma (4.3%, N = 3) (Table 2).
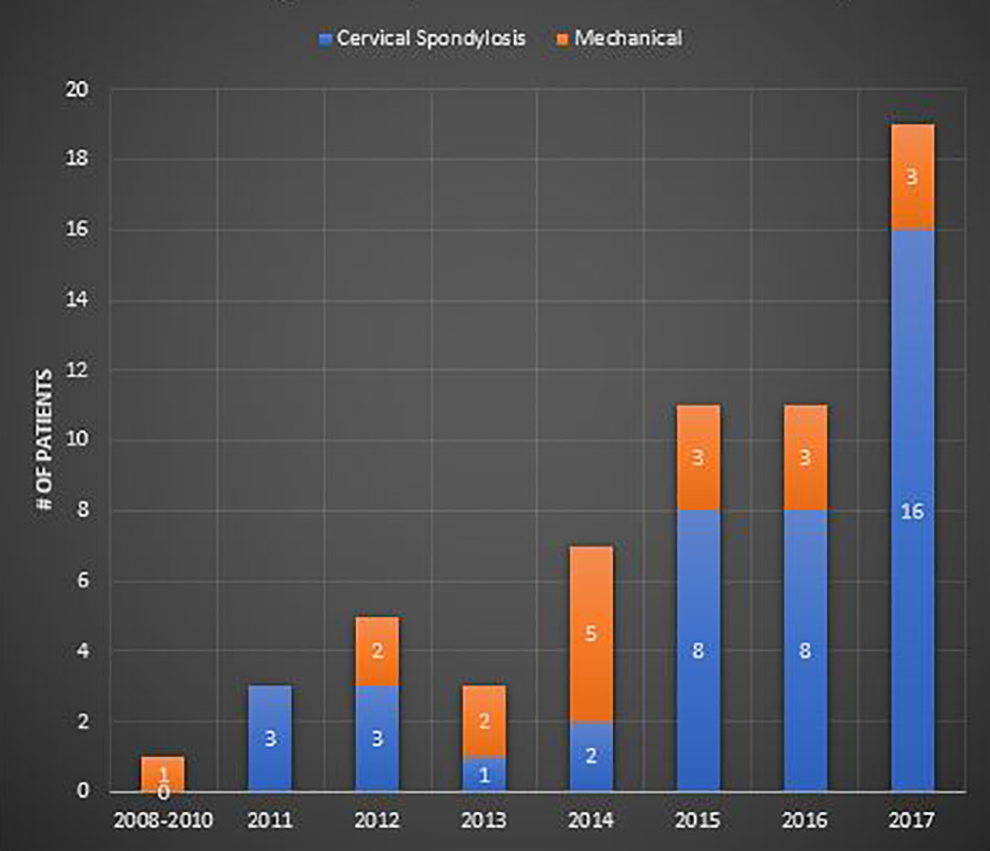
Distribution of the indications for removal of ACDA by year (from 2008 to 2017).
Reasons for Revision Surgery by Diagnosis (2008-2017).
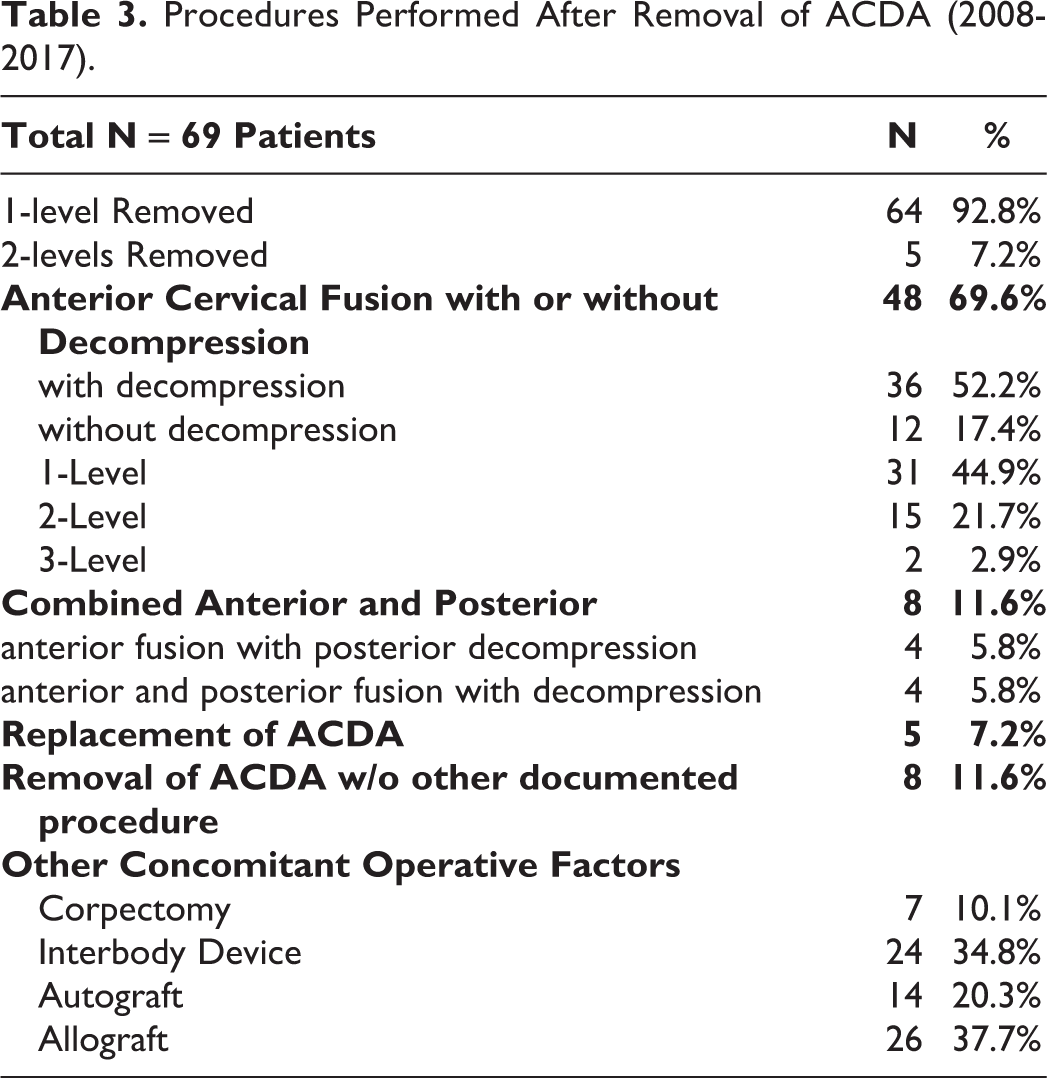
The majority of patients required a 1-level removal (92.8%, N = 64) vs. 2-level (7.2%, N = 5) (Table 3). After removal of ACDA, common procedures performed included anterior cervical fusion with or without decompression (69.6%, N = 48), combined anterior/posterior fusion/decompression (11.6%, N = 8), and replacement of ACDA (7.2%, N = 5). No statistically significant trend in the type of secondary surgeries performed existed over time (p-value = 0.954) (Figure 3). Of the 64 patients who had a 1-level ACDA removed, more than half (51.6%, N = 33) subsequently underwent at least a 2-level anterior cervical fusion. For anterior cervical fusions, 75% of cases (N = 36) involved a decompression and nearly 90% (N = 46) were either 1- or 2-level fusions. The indications for surgery did not vary significantly among the different procedures performed (anterior cervical fusion: cervical spondylosis – 77.8% [N = 28]vs. mechanical complication-82.4%[N = 14] | combined: cervical spondylosis – 11.1%[N = 4] vs. mechanical complication – 17.7%[N = 3] | replacement: cervical spondylosis – 11.1%[N = 4] vs. mechanical complications – 0%[N = 0], p-value > 0.05).
Procedures Performed After Removal of ACDA (2008-2017).
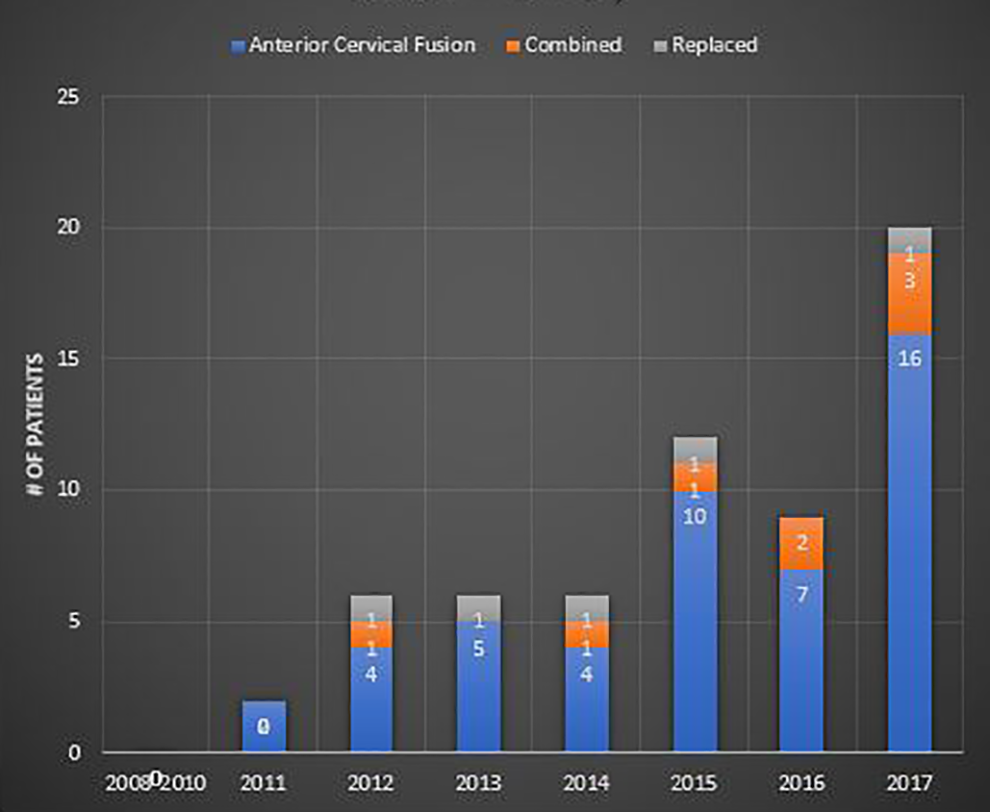
Distribution of the number of secondary procedures after removal of ACDA by year (from 2008 to 2017).
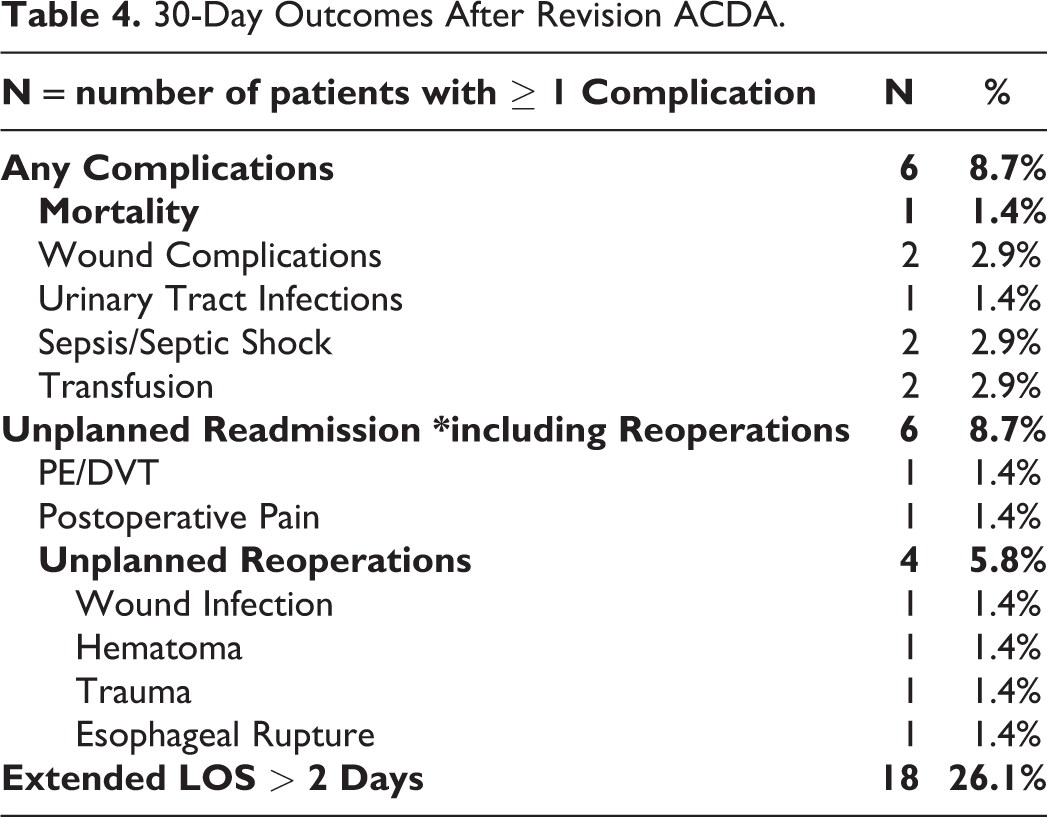
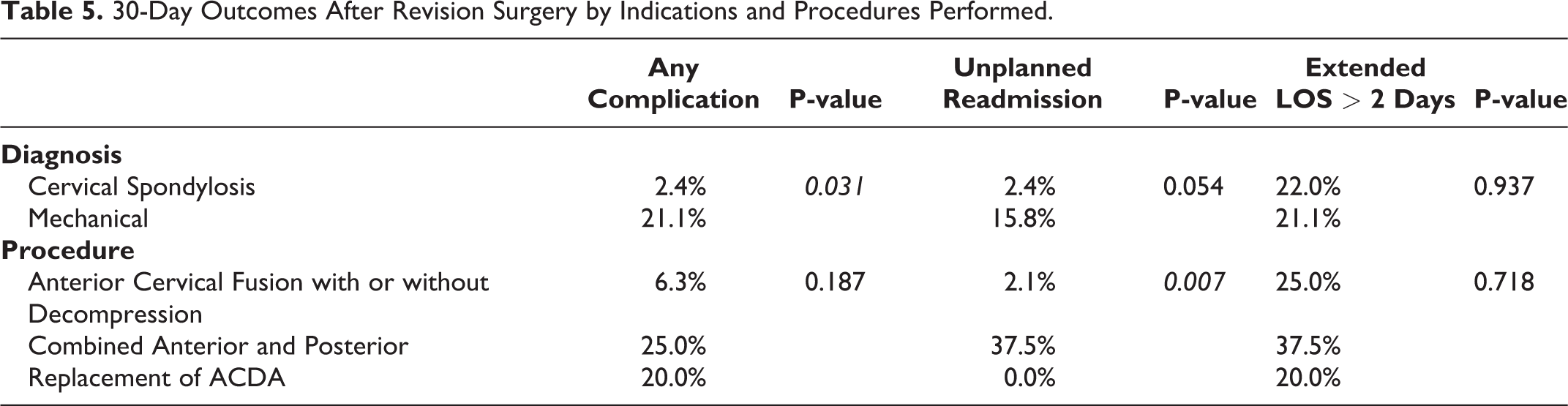
Short-term postoperative complication rates after revision surgery were significantly higher than those seen after primary cases (Any complications: revision = 8.7% (N = 6) vs. primary = 0.78% (N = 26), p<0.001 | Unplanned 30-day Readmission: revision = 8.7%(N = 6) vs. primary = 1.5% (N = 50), p<0.001 | Unplanned 30-day Reoperations: revision = 5.8%(N = 4) vs. primary = 0.66% (N = 22), p<0.001)(Table 4). Revision cases for mechanical complications had significantly higher overall short-term complications (21.1%, N = 4) than those who underwent revision surgery for cervical spondylosis (2.4%, N = 1, p = 0.031). In comparison to anterior cervical fusion (2.1%, N = 1) and replacement of ACDA (0%, N = 0), those who underwent combined approaches (37.5%, N = 3) had significantly higher risk for unplanned readmissions (p = 0.007) (Table 5).
30-Day Outcomes After Revision ACDA.
30-Day Outcomes After Revision Surgery by Indications and Procedures Performed.
Discussion
Although cervical decompression and fusion remains an excellent option for the surgical treatment of CDD, ACDA is becoming an increasingly attractive option with growing evidence to support comparable outcomes. To further validate ACDA as a viable alternative to conventional treatments, an in-depth analysis on ACDA failures is needed. Currently, the data focusing on this patient population is lacking. Understanding the associated indications for revision surgery, and the outcomes of secondary procedures performed after ACDA failure will be important for developing revision strategies to better manage ACDA failure.
In a single-center case series, Park et al examined 21 patients who underwent revision surgery after ACDA failure with a minimum 2-year follow-up. 16 These authors defined ACDA failure as the recurrence or persistence of clinical symptoms such as radiculopathy or myelopathy. The most common cause of failure was determined to be “poor patient selection,” since as many as 80% of patients had severe spondylosis or ossification of the posterior longitudinal ligament prior to the index surgery. The remaining patients has implant-related complications (e.g. subsidence, malposition). Sixteen patients (76%) ultimately had their ACDA removed with subsequent decompression and fusion. The authors report that ultimately these patients did well with 86% of patients reporting “good to excellent” outcomes, over 90% achieving successful fusion, without any major neurologic or wound complication. This study was limited by its small sample size and single-center data, but it revealed that patient selection may need to be further refined for this cohort to reduce unnecessary revision surgery.
In a more recent single-center series, Zigler et al reported a revision rate of 5.6% (30/535 patients) with a 2-year minimum follow up. 17 The mean time from index to revision surgery was 78 months (ranging from 24 to 181 months). In contrast to the Park et al study, only 10% (N = 3) of the revised cases required a removal of ACDA. The majority of revised cases were for the treatment of adjacent segment disease (70%, N = 21), however, it is unclear from this study what secondary procedures were performed for these 21 patients. Interestingly, no mechanical complications were reported in this study. It is important to note the conflicts of interest disclosed by these authors, which may contribute to possible bias. Nevertheless, these findings provide additional insight on the reasons for revision ACDA and the need for larger studies.
Jackson et al performed a prospective, multicenter, randomized clinical trial with a 5-year minimum follow up to compare the revision surgery rates between ACDA and ACDF. 14 These authors defined revision surgery as any secondary surgery after the primary one. The revision rates for ACDA was significantly lower than those for ACDF for both 1- and 2-level cases. The rate of removal of ACDA for 1- and 2-level cases were 2.2% (4/179) and 3.0% (7/234), respectively. All patients with a removal of ACDA were fused anteriorly at the index level with possible fusion to the supra- or infra-adjacent level as well. For 1-level ACDA cases, there were 4 times fewer patients requiring a secondary surgery for adjacent segment disease than those who underwent ACDF (2.2% TDR vs. 11.1% ACDF, p<0.05). In contrast to prior studies, these authors provide a detailed description of the reasons for revision surgery and subsequent procedures involved.
Our study provides the first and largest multicenter assessment of patients who required the removal of ACDA over a 10-year period. The overall rate of revision ACDA appeared low (2.1%) with a growing number of primary ACDA every year. However, the consequence of revision surgery was significant. In comparison to primary ACDA, revision cases had significantly longer operative times (+45 minutes), longer hospital stays (+2.5 days), and higher complication rates (10-fold higher). The most common reasons for revision surgery included cervical spondylosis (59.4%) or mechanical complications (27.5%). It is likely that “cervical spondylosis” refers to adjacent segment disease or inadequate decompression at the time of the index surgery. Interestingly, our data shows that a substantial number of revision cases for spondylosis were due to adjacent segment disease since nearly 35% (n = 17) of 1-level cases resulted in at least a 2-level surgery. As mentioned by Park et al, it is also possible that a number of those with more severe cervical spondylosis were inappropriately indicated for ACDA at their index surgery. In terms of subsequent procedures, failed ACDA resulted in fusion more often than replacement. The majority (70%) of patients underwent anterior cervical fusion with or without decompression versus a combined approach. Although the indications for revision surgery were not significantly different among the procedures performed, patients with mechanical complications or those who underwent a combined anterior and posterior approach had significantly higher risk for short-term postoperative complications.
A number of limitations should be considered in this study. Although large national databases can provide insight on incidences and trends, they often lack the granularity of procedure-specific data. For instance, this database is not designed to provide data on implant subsidence, heterotopic ossification, or the presence of adjacent level stenosis at the time of the index operation, which may influence revision surgery. Due to the de-identified nature of the NSQIP database, we are unable to link primary cases with those who required the removal of ACDA. Therefore, direct comparisons between those with and without the removal of ACDA after primary ACDA surgery as well as the timing between primary and revision cases were not performed in this study. Our study’s rate of revision ACDA over a 10-year period is defined as the ratio of the total number of revision cases divided by the total number of primary cases performed between 2008 and 2017. We acknowledge that our reported 2.1% is likely lower than the true prevalence since primary cases which occurred in 2017 may eventually require removal of ACDA beyond our study’s time-frame as well as be readmitted to other hospitals outside of NSQIP data. It is possible that primary cases occurred prior to 2008; however, no primary ACDA cases were identified prior to our study’s timeframe including up to 2005, which is the earliest NSQIP data available. This may, at least in part, be due to the fact that the first cervical disc arthroplasty was not FDA approved in the United Sates until 2007. 18 The absence of radiographic data made it difficult to elucidate the true extent of mechanical complications and cervical spondylosis, which can influence surgical treatment. The relatively small sample size of revision patients and few short-term complications precluded our ability to perform multivariate regression analyses on outcomes. As more ACDA cases are performed each year, larger studies will be possible.
Conclusion
It is well-acknowledged that ACDA can achieve comparable outcomes to ACDF at the index surgery for mild spondylosis. However, it remains unclear how surgeons are treating patients when ACDA fails. Our study seeks to shed light on this topic using multicentered national-level data. We found that the rate of ACDA failure over a 10-year period is low (2.1%); however, the consequence of revision surgery is significant as short-term complication rates are nearly 10-fold greater than those seen after primary cases. Nearly 90% of revision cases were due to either cervical spondylosis or mechanical complications. These indications for surgery did not vary significantly among the different procedures performed. Patients requiring revision surgery for mechanical complications or those who underwent a combined surgical approach were at significantly higher risk for subsequent short-term complications. These findings will be important during the shared-decision making process for patients undergoing either primary or revision ACDA.
Footnotes
Authors’ Note
This study was qualified as exempt by the Institutional Review Board
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.