
Abstract
Study Design
Retrospective, propensity-matched analysis
Objectives
Cervical disc arthroplasty (CDA) is being increasingly utilized for cervical disc generation. Surgeon specialty has been shown to influence the risk for postoperative complications in spine surgery, but this has not yet been explored for CDA. Thus, the purpose of this study is to determine whether there is any difference in 30-day complications between patients undergoing single-level CDA by neurosurgeons vs by orthopaedic surgeons.
Methods
A retrospective, 1:1 propensity score matched analysis was performed using the NSQIP database from 2015 to 2020. Patient demographics, operative characteristics, and postoperative complications were recorded. Independent multivariate logistic regression models were constructed using the propensity-matched dataset to assess surgical specialty influence on any complication, any site complication, any operative infection, and any medical complications.
Results
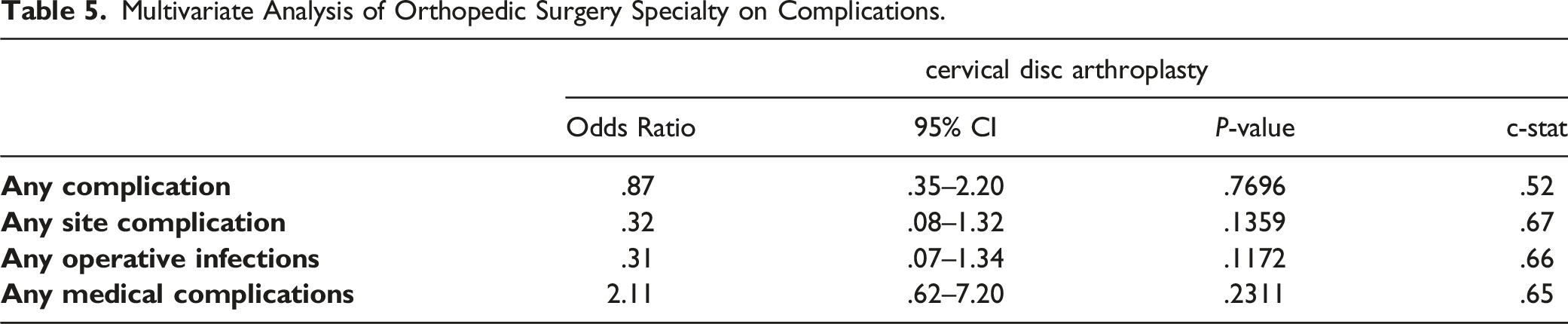
3179 single-level CDAs (28.8% orthopaedic surgery patients, 71.2% neurosurgery patients) were identified that met the inclusion criteria. Well-matched cohorts of 916 patients each were generated. After controlling for all possible confounders, orthopedic surgery specialty was not associated with a higher odds for any complication (OR: .87, 95% CI: .35 – 2.20, P = .7696), any site complication (OR: .32, 95% CI: .08 – 1.32, P = .1359), any operative infection (OR: .31, 95% CI: .07 – 1.34), P = .1172), nor any medical complication (OR: 2.11, 95% CI: .62 – 7.20, P = .2311) vs neurosurgery.
Conclusion
This is the first propensity-matched analysis to show that spine surgeon specialty does not influence the risk for any complication, any site complication, any operative infection, nor any medical complication following single-level CDA within the first 30 days after surgery.
Introduction
Cervical disc arthroplasty (CDA) is being increasingly utilized, with an estimated 22,282 CDA procedures performed between 2004 and 2013 in the United States.1,2 Although anterior cervical discectomy and fusion (ACDF) has generally been considered the gold standard for cervical disc generation, CDA is being utilized as an alternative due to several advantages. Most importantly, CDA preserves more physiologic motion of the spine and may decrease the risk for adjacent segment disease.3,4 Additionally, prior research suggests that reoperation rates at the index level and adjacent levels are significantly less following CDA compared to ACDF.5,6 Likewise, a national database study showed that CDA has a lower rate of complications, a lower rate of 90-day readmissions, and a shorter length of stay. 7 Although CDA may have these benefits, it is not without complications.
Virk et al analyzed complications of 1347 entries of 7 different FDA-approved CDA implants and found that 25.2% had migration of the implant, 23.3% had insertion problem/failure, and 8.1% had heterotopic ossification. 8 Likewise, Shah et al conducted a retrospective study of 16,510 patients from a state database and found that those who had undergone 1- or 2-level CDA had an increased risk for 2-year surgical complications, overall complications, and revisions compared to ACDF patients. 9 Furthermore, a systematic review by Xu et al found that rates for dysphagia/dysphonia ranged from 1.3% to 27.2%, rates for cervical wound infection ranged from 1.2% to 22.5%, rates for vascular compromise ranged from 1.1% to 2.4%, and rates for cerebrospinal fluid leak ranged from .8% to 7.1%. 10
There is a need to better identify risk factors for complications and worse outcomes in order to improve patient outcomes. One area of interest has been the influence of surgeon specialty on complication rates. For example, Bronheim et al conducted a retrospective study using a national database of 3182 patients undergoing anterior lumbar fusion and found that those patients undergoing surgery by a neurosurgeon had a higher risk of reoperation and urinary tract infection within 30-days compared to those undergoing surgery by an orthopaedic surgeon. 11 Any differences in complication rates between neurosurgery and orthopaedic surgery patients may also have long-term impacts on surgical residency and fellowship training models, reimbursements, and other aspects of the healthcare system. Whether or not such an influence of spine surgeon specialty exists on 30-day complications following single-level CDA has not yet been explored. Thus, this is the first study to conduct a propensity-matched analysis for examining whether there is any difference in 30-day complication rates between patients undergoing single-level CDA by neurosurgeons vs by orthopaedic surgeons.
Methods
Database
A retrospective analysis was conducted using the National Surgical Quality Improvement Program (NSQIP). The NSQIP is a prospective, multi-institutional database utilized to assess surgical quality improvement within the Unites States. The methodologies for data collection for NSQIP have been previously described elsewhere. 12 This study was deemed exempt from requiring informed consent as all data used was deidentified and publicly available. This study did not receive any grant or other external funding.
Population Selection
All patients who underwent a single-level CDA from the years 2015 to 2020 were identified using Current Procedure Terminology (CPT) Code 22856. Patients undergoing any concomitant procedures were excluded from the analysis. Patients with “null” and missing preoperative variables were also excluded from the analysis.
Data Collection
Demographic variables (age, sex, BMI, race, patient status (inpatient or outpatient), functional status), comorbidities (diabetes, smoking status, history of chronic obstructive pulmonary disease, hypertension, ascites, cancer, chronic health failure, steroid use, bleeding disorders, and American Society of Anesthesiologists (ASA) classification), operative characteristics (operative (OR) time, length of stay, discharge location), and complications were collected and compared between the 2 surgical specialties.
Postoperative complications were then stratified as any surgical site complication, any medical complication, and any complication overall in which all the above was included. Surgical site complications included any operative infection such as superficial surgical site infections (SSI), deep incisional SSI, organ/space SSI, and wound disruption. Medical complications consisted of urinary tract infections (UTI), sepsis, septic shock, pneumonia, unplanned intubation, pulmonary embolisms (PE), being on a ventilator for greater than 48hrs, renal insufficiency, acute renal failure, stoke, cardiac arrest, myocardial infraction, blood transfusions, deep vein thrombosis (DVT), and any unplanned reoperations within the 30-day period. All the variables used in this analysis were used as defined by the NSQIP user guide and outcomes were followed for 30 days after the initial surgery. 13
Statistical Analysis
Univariate analysis was conducted to compare the aforementioned variables for any statistical differences between the 2 surgical specialties. Both fisher’s exact test and chi-squared tests were used to compare categorical variables while independent t-tests were used to compare continuous variables. In all cases, a P-value of .05 or less was considered to be statistically significant. Propensity score matching analysis was then conducted to account for any differences in the aforementioned variables between the 2 cohorts. Propensity score matching was used to minimize any potential bias that may have risen due to the nonrandomization design of this study. This type of analysis allows for a more accurate estimate of the effect of surgical specialty by simultaneously controlling for any possible confounders between the 2 cohorts. The matching was completed using a 1:1 nearest neighbor algorithm signifying that for each randomly selection case from the orthopedic cohort, a case from the neurosurgery cohort with the closest propensity score was paired based on the matched preoperative and demographical characteristics. This process was repeated until every orthopedic case was matched with a neurosurgery case. Independent multivariate logistic regression models were then constructed using the propensity-matched dataset for single-level CDA to assess the association of surgical specialty with the following outcomes: any complication, any site complication, any operative infection, and any medical complications. Preoperative variables with a P-value < .2 were identified and included in each regression model. Neurosurgery served as the reference specialty. Hosmer-Lemeshow and C statistics were calculated to assess the calibration and goodness-of-fit of the model, respectively. All descriptive and comparative statistics were performed using SAS software, version 9.2 (SAS Institute, Cary, NC).
Results
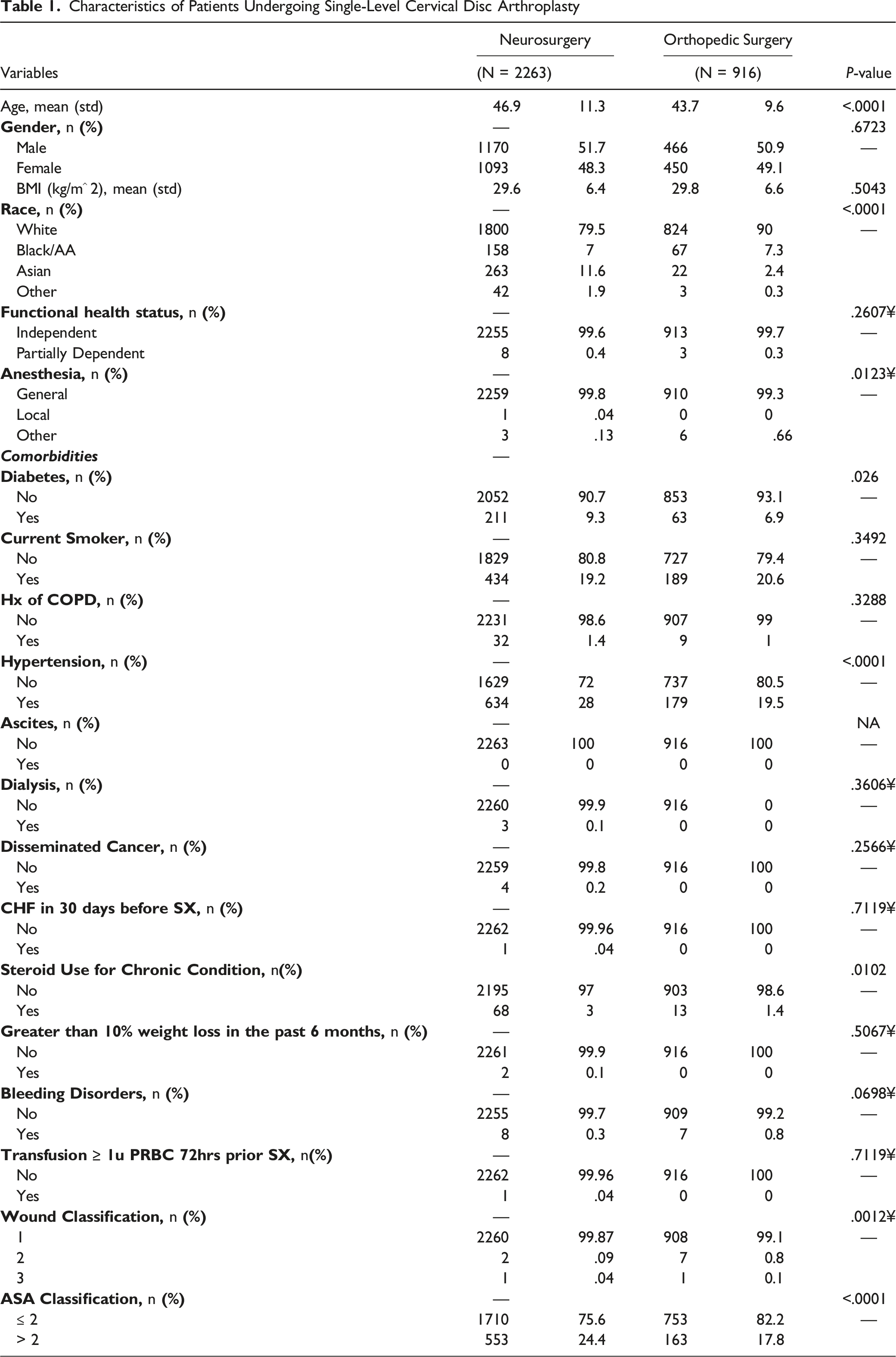
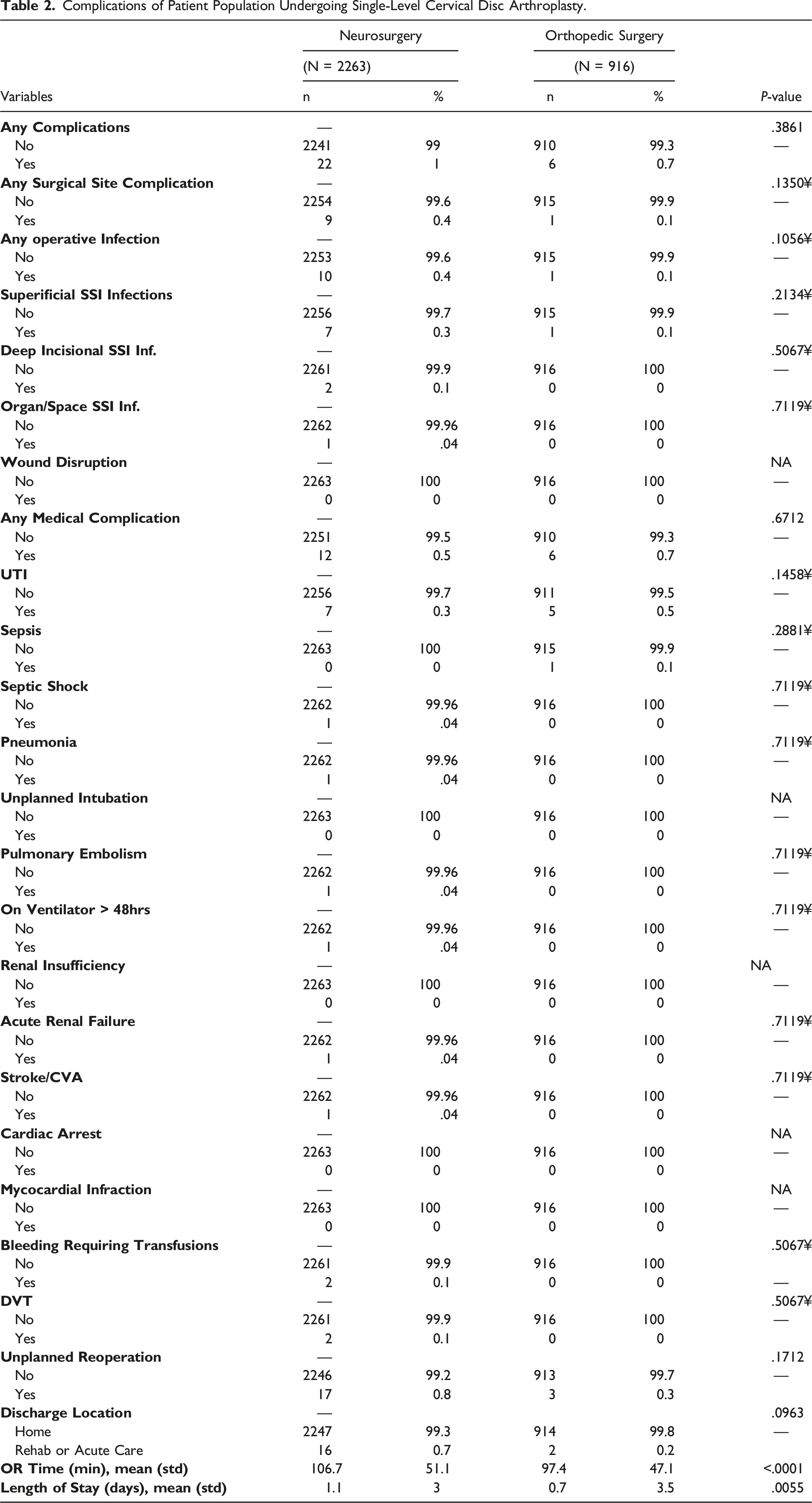
A total of 3179 single-level CDAs were identified that met the inclusion criteria (Figure 1). A total of 377 cases were excluded from the original dataset containing 3556 single-level CDAs due to missing preoperative variables that we would then incorporate into our analysis. There were 916 patients (28.8%) and 2263 patients (71.2%) in the orthopedic surgery and neurosurgery cohorts, respectively. Demographically, the neurosurgery cohort was older (46.9±11.3yrs vs 43.7±9.6yrs, P<.0001), and consisted of less patients that identified as white (79.5 vs 90%, P < .0001). The same cohort consisted of more diabetics (9.3 vs 6.9%, P = .026), patients with hypertension (28 vs 19.5%, P < .0001), patients that use steroids for a chronic condition (3 vs 1.4%, P = .0102), patients classified as having a class 1 wound (99.9 vs 99.1, P = .0012), and patients that have an ASA class greater than 2 (24.4% vs 17.8%, P < .0001). All other demographic variables and comorbidities can be found in Table 1. Univariate analyses demonstrated no statistical differences in 30-day postoperative complications nor among the discharge location between the 2 cohorts. However, the neurosurgery cohort did experience longer OR times (106.7±51.1min vs 97.4±47.1min, P < .0001) and a longer length of stay (1.1 ± 3 days vs .7 ± 3.5 days, P = .0055) (Table 2). Flow chart demonstrating patient population selection. Characteristics of Patients Undergoing Single-Level Cervical Disc Arthroplasty Complications of Patient Population Undergoing Single-Level Cervical Disc Arthroplasty.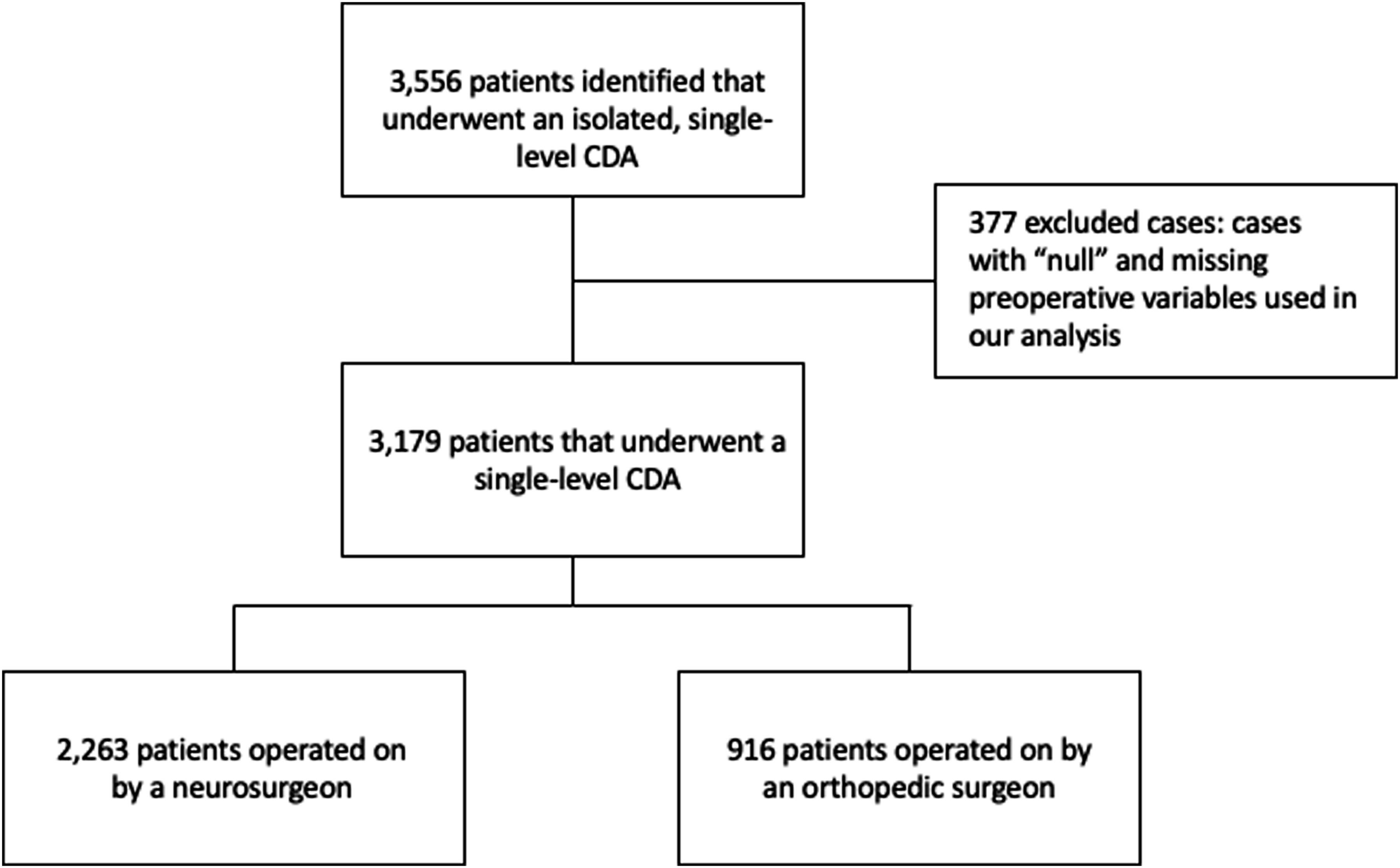
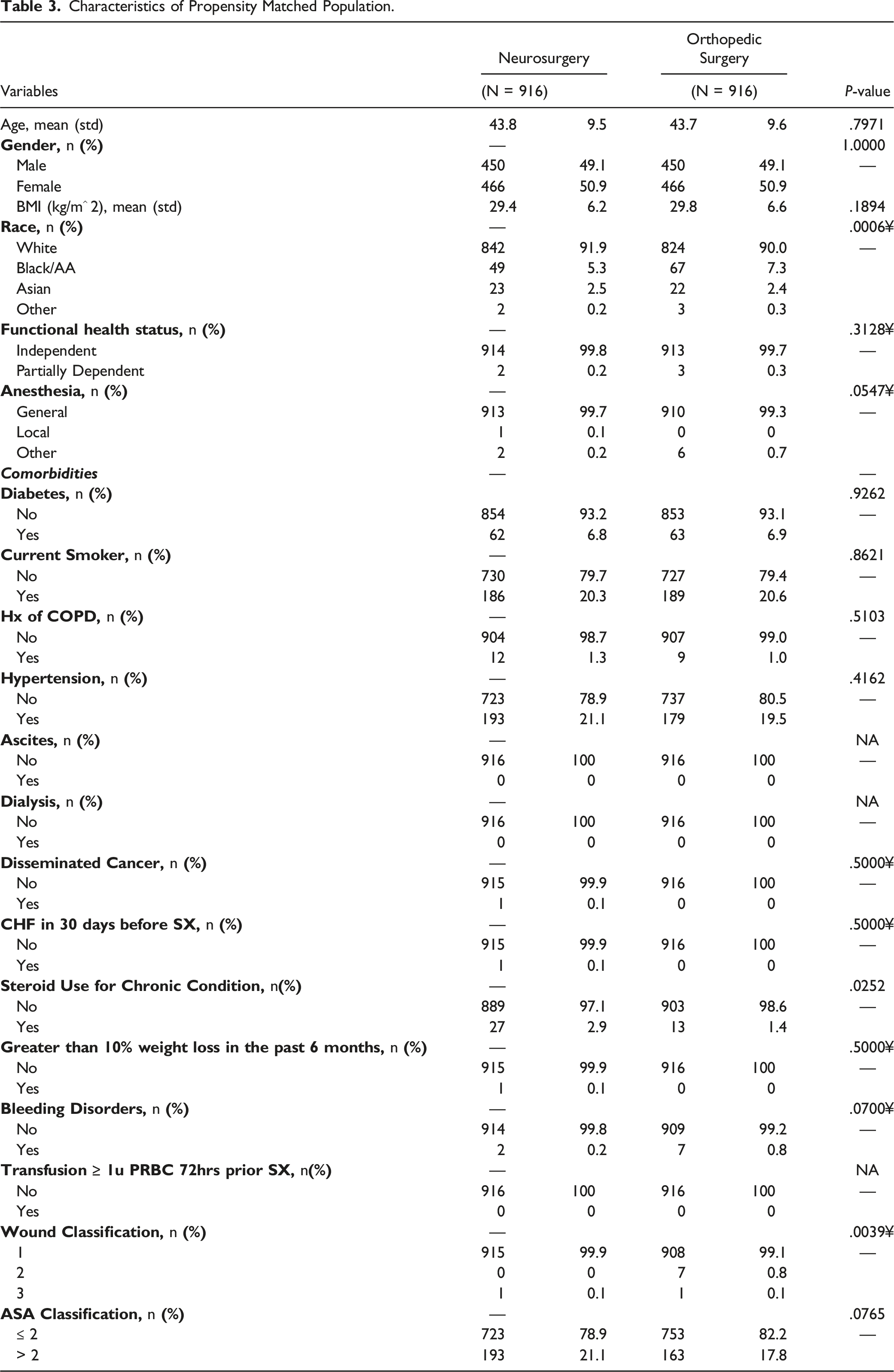
Characteristics of Propensity Matched Population.
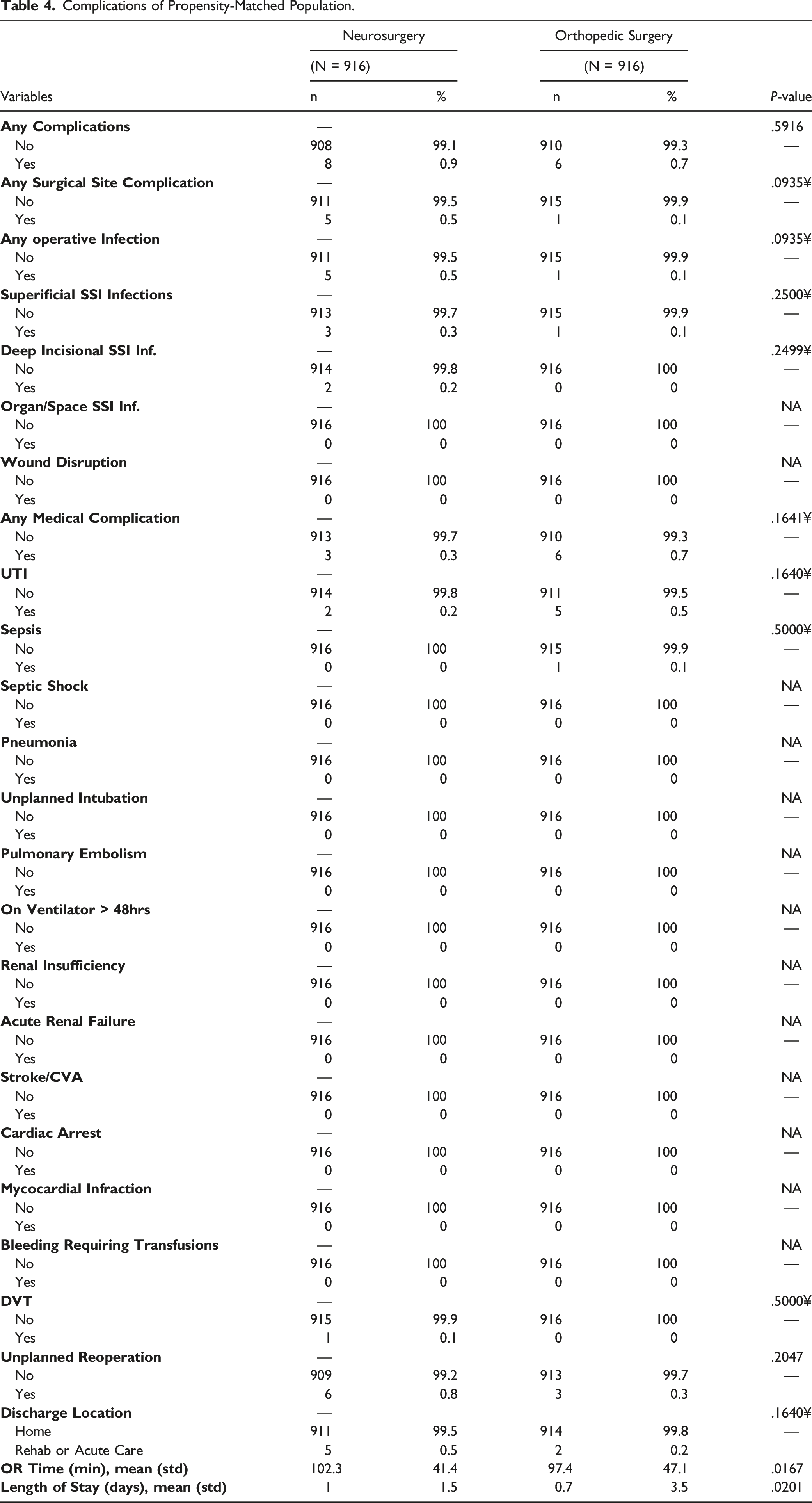
Complications of Propensity-Matched Population.
Multivariate Analysis of Orthopedic Surgery Specialty on Complications.
Discussion
CDA provides a good alternative to ACDF for patients with cervical disc generation by allowing for more preserved physiological motion of the spine and a reduced risk for adjacent disc disease. Nonetheless, it continues to have perioperative complications and identifying risk factors for such complications or worse outcomes is necessary. Such identification can allow us to improve patient outcomes and healthcare delivery. The influence of surgeon specialty on spinal surgery outcomes in other surgeries has been reported previously. However, this is the first study to examine the influence of surgeon specialty on 30-day complications following single-level CDA. In the propensity-matched cohorts, neurosurgery patients were found to have longer OR time and length of stay on bivariate analysis. However, these differences are not clinically significant. On multivariate analysis, orthopaedic surgery specialty was not a risk factor for any complication, any site complication, any operative infections, or any medical complications.
This study’s findings are consistent with prior studies showing that spine surgeon specialty does not increase the risk for overall perioperative complications.14–16 Kim et al conducted a propensity score matching analysis using a national database of patients undergoing single-level lumbar fusion to evaluate the influence of the surgeon’s specialty. 16 The authors found no significant differences in the risk for developing any complication, medical complications, surgical complications, or reoperation within 30-days of surgery. 16 Similarly, Minhas et al conducted a propensity score-matching analysis of single-level ACDF patients comparing neurosurgery and orthopaedic surgery patients. 15 The authors found that spine surgery specialty did not influence the risk for overall complications, surgical site complications, or medical complications. 15 Furthermore, Malik et al used a national database to assess the influence of surgeon specialty on risks following fusions, laminectomies, or osteotomy/corpectomy for spinal metastases. 14 The authors did not find any significant differences in risk for 90-day complications, readmission, or mortality between both spine surgery specialties. 14
However, several studies are not consistent with this study’s findings.17–20 Alomari et al conducted a retrospective, 1:4 propensity score-matched analysis using a national database to evaluate the influence of spine surgeon specialty on outcomes following elective posterior spinal fusion for adolescent idiopathic scoliosis. 18 The authors found that orthopaedic surgery patients had a shorter total hospital stay, shorter operation time, lower rate of return to operating room within same admission, and lower unplanned readmission rates, whereas neurosurgery patients had only a lower perioperative blood transfusion rate. 18 Likewise, Alomari et al also conducted a retrospective, 1:1 propensity score-matched study using a national database to evaluate the influence of surgeon specialty on outcomes following elective single-level and multilevel anterior/lateral lumbar interbody fusion. 19 The authors found that neurosurgery patients had longer operative times, shorter total hospital stays, lower rates of return to the operating room, lower rates of nonhome discharge, and lower rates of perioperative blood transfusion in both single and multilevel surgery. 19 Furthermore, another 1:1 propensity score-matched study of patients undergoing elective ACDF aimed to evaluate the influence of spine surgeon specialty on 30-day outcomes. 17 The authors found that in both single-level and multilevel ACDF, neurosurgery patients had shorter total hospital stay and lower rates of return to operating room, nonhome discharge, sepsis, and perioperative blood transfusion but longer operative times compared to orthopaedic surgery patients. 17 Additionally, Seicean et al conducted a propensity matched analysis of patients undergoing elective spine fusion and laminectomy by neurosurgeons and orthopaedic surgeons. 20 The authors found that patients operated on by orthopaedic surgeons had an increased risk for a prolonged length of stay and perioperative transfusion. 20
Further investigations on the influence of spine surgeon specialty on patient outcomes following other surgeries are warranted. Both neurosurgery and orthopaedic surgery specialists operate on the spine despite having significant differences in training, but the impact this has on clinical outcomes has not been explored for all spine surgeries. For example, it was recently found that graduating neurosurgery residents have logged 6.8 times more adult spine cases when graduating compared to orthopaedic surgery residents. 21 Moreover, spine procedures were found to have accounted for 33.5% of all total surgical cases over 10-years for neurosurgery residents compared to 6.2% for orthopaedic surgery residents. 22 However, although orthopaedic residents perform less spine cases than neurosurgery residents, fellowship training likely equalizes this difference as significantly more orthopaedic spine surgeons are fellowship trained compared to neurosurgery spine surgeons.23,24 Therefore, this study finding no clinically significant difference in complication rates between both specialties provides further evidence supporting the equalizing effect of fellowship training.
This study is not without limitations. A large national database is prone to erroneous data entry or omission, although this likely occurs at too low of a rate to significantly influence this study’s results due to quality control measures. Additionally, the database does not have surgeon experience available for analysis, as that may influence risks from each specialty. Moreover, the database is limited to only 30-day outcomes, and it is possible that there may be differences in risks seen with spine surgery specialties with 90-day or longer outcomes. For example, complications associated with surgeon technique such as heterotopic ossification, poor range of motion secondary to misplacement, and implant subsidence or migration may not be recognized in the first 30 days after surgery. Despite these limitations, this is the first well-powered, propensity score matched analysis to evaluate the influence of spine surgeon specialty on complications following single-level CDA.
Conclusion
Single-level CDA is performed by both neurosurgeons and orthopaedic surgeons. This is the first propensity-matched analysis to show that spine surgeon specialty does not influence the risk for any complication, any site complication, any operative infection, nor any medical complication following single-level CDA within the first 30 days after surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.