
Abstract
Study Design
Systematic Reviews.
Objectives
To investigate predictors of surgical outcomes for mild Degenerative Cervical Myelopathy (DCM) by reviewing all related studies conducted at this point.
Methods
An electronic search was carried out in PubMed, EMBASE, Scopus, and Web of Science until June 23, 2021. Full-text articles reporting surgical outcome predictors of mild DCM cases were eligible. We included studies with mild DCM which was defined as a modified Japanese Orthopaedic Association score of 15 to 17 or a Japanese Orthopaedic Association score of 13 to 16. Independent reviewers screened all the records, and discrepancies between the reviewers were solved in a session with the senior author. For risk of bias assessment, RoB 2 tool was used for randomized clinical trials and ROBINS-I for non-randomized studies.
Results
After screening 6 087 manuscripts, only 8 studies met the inclusion criteria. Lower pre-operative mJOA scores and quality-of-life measurement scores were reported by multiple studies to predict better surgical outcomes compared to other groups. High-intensity pre-operative T2 magnetic resonance imaging (MRI) was also reported to predict poor outcomes. Neck pain before intervention resulted in improved patient-reported outcomes. Two studies also reported motor symptoms prior to surgery as outcome predictors.
Conclusion
Lower quality of life before surgery, neck pain, lower pre-operative mJOA scores, motor symptoms before surgery, female gender, gastrointestinal comorbidities, surgical procedure and surgeon’s experience with specific techniques, and high signal intensity of cord in T2 MRI were the surgical outcome predictors reported in the literature. Lower Quality of Life (QoL) score and neck prior to surgery were reported as predictors of the more improved outcome, but high cord signal intensity in T2 MRI was reported as an unfavorable outcome predictor.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is a chronic progressive compressive spinal disorder and the most widespread reason for spinal cord abnormality in adults. Its incidence has been reported as present in 2% of adult populations.1,2 One study in 2017, demonstrated the prevalence of DCM to be 1 120 per 1 million, with an incidence of hospitalizations at 4 per 100 000 person-years. 3 DCM affects the quality of life of affected individuals to a great degree measured by tools like the Short-Form Health Survey (SF-36). 4
Its pathogenesis is through age-related degenerative changes in the spinal column, including hypertrophy and calcification of ligaments, intervertebral discs, vertebral bodies, and osseous tissue. These changes can lead to stenosis of the cervical spinal canal, which imposes and compresses the spinal cord and results in neurological decline.1,5 Degenerative Cervical Myelopathy (DCM) is adults’ most common cause of spinal cord-related dysfunction, 6 and it is particularly important in aging populations.
Evidence-based guidelines and literature recommend surgical decompression for moderate and severe DCM.7-9 However, both surgical and non-operative management are options for mild DCM.9-11 There is a lack of evidence regarding the best treatment between surgery and non-operative management of mild DCM.7,12 The literature notes that patients treated non-operatively deteriorate from 20-60 percent in the long-term follow-ups.13-15
DCM symptoms range from mild pain and paresthesia (numbness and tingling) to severe defects such as quadriplegia and incontinence. 16 These symptoms are also reported as outcome predictors and factors influencing the decision to choose between the non-operative or surgical treatment of mild DCM cases. After a diagnosis of mild DCM, the timing for surgery and determining the optimal surgical procedure are the main challenge of care. Some suggest that surgical delays could lead to severe decline and lifetime disability.16,17
Unfortunately, the pattern of progression of DCM is not fully understood and could not be predicted. 18 Recently Arbeitsgemeinschaft für Osteosynthesefragen (AO) spine, as a part of the Research Objectives and Common Data Elements for Degenerative Cervical Myelopathy (AO Spine RECODE-DCM) project, reported the top ten research priorities in DCM research. Recognizing patient progression was a priority (Improving Awareness Could Transfer Outcomes in DCM) as well as Optimizing the Application of Surgery for DCM Priority 10).19-21
The reported outcome predictors could help clinicians make a better judgment regarding managing mild DCM. Therefore, this study aims to investigate predictors of surgical outcomes for mild DCM by reviewing all related studies conducted at this point.
Methods
Our protocol included the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol for the systematic reviews.
22
An electronic search with no language restriction was carried out in PubMed, EMBASE, Scopus, and Web of Science registered with PROSPERO (CRD42020190748) until June 23, 2022. The PRISMA flowchart of this study is available in Figure 1. Flowchart of studies excluded and included for this study.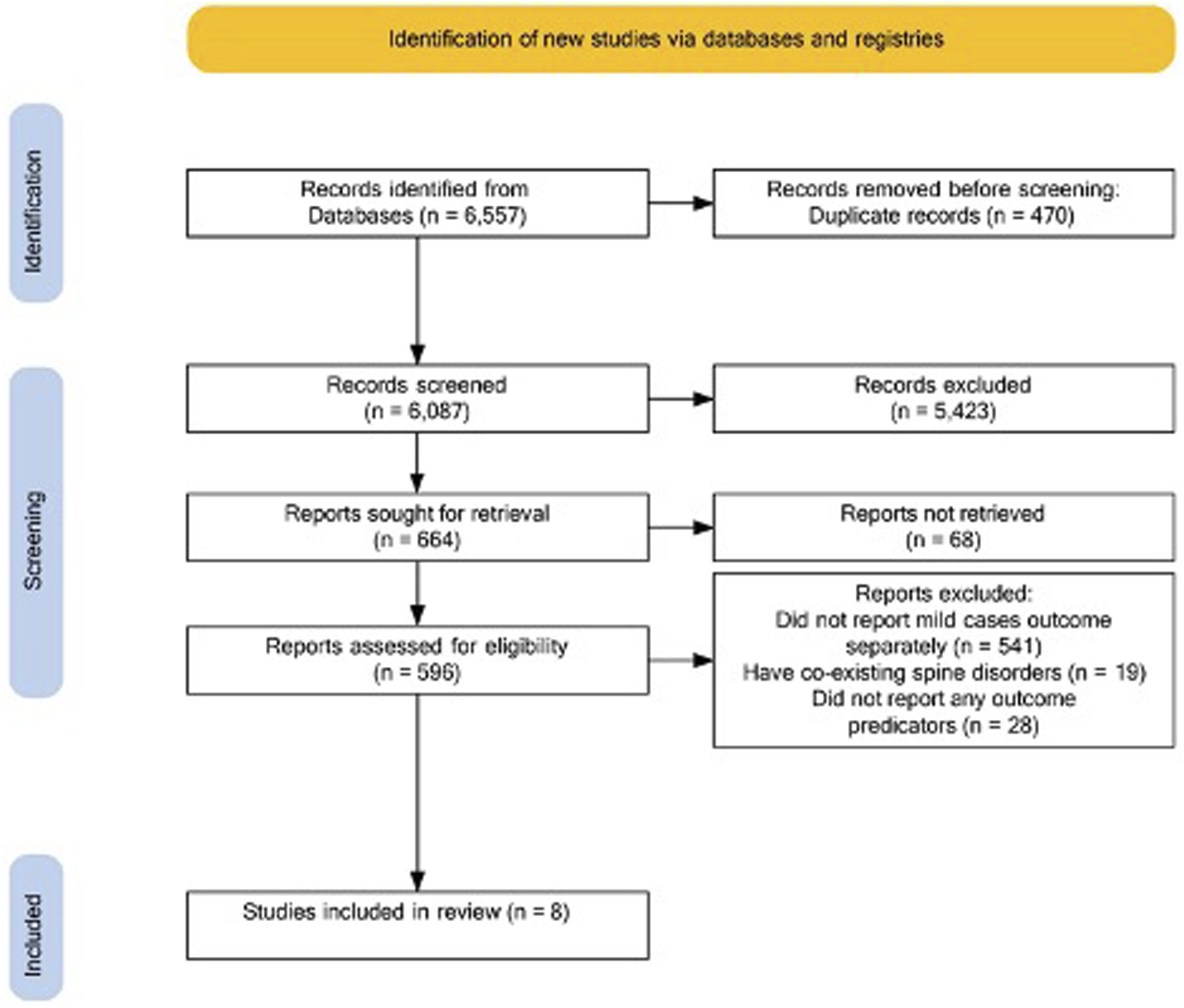
Full-text articles without language limitations reporting surgical outcome predictors of mild DCM cases were eligible. Those with mJOA of 15 to 17 or JOA of 13 to 16 were considered mild DCM cases. We included randomized clinical trials, non-randomized clinical trials, cohorts, case-control, administrative databases, surveys, and case series while excluding other types of studies during screening. Studies that did not report mild cases outcomes separately and studies with co-existing spine disease (such as hemangiomas) were excluded.
Search results were imported into EndNote (X9, Thomson Reuters), duplicates were removed, and 2 groups of 2 reviewers screened titles and abstracts independently. Any reviewer discrepancies were resolved in a session with the senior author. After obtaining full texts, they were checked with inclusion and exclusion criteria by 2 reviewers. Again, in this step senior author resolved any disagreements between the 2 reviewers. Finally, the included studies were reviewed for data extraction after reviewing the complete text. We extracted the first author, publication year, location of study, type of study, number of mild cases, male to female ratio, age (mean and standard deviation or, in some cases, median and range), diagnosis [Ossification of Posterior Longitudinal Ligament (OPLL) and Cervical Spondylotic Myelopathy], outcome measurement tools, and surgical outcome predictors from included studies. We used the class of evidence criteria suggested by the Journal of Bone and Joint Surgery for studies investigating treatment results for assessing methodological quality. 23 For risk of bias assessment, RoB 2 tool was used for randomized clinical trials and ROBINS-I for non-randomized studies as recommended by the Cochrane Handbook for Systematic Reviews of Interventions.24-26
Results
Characteristics and level of evidence of included studies.
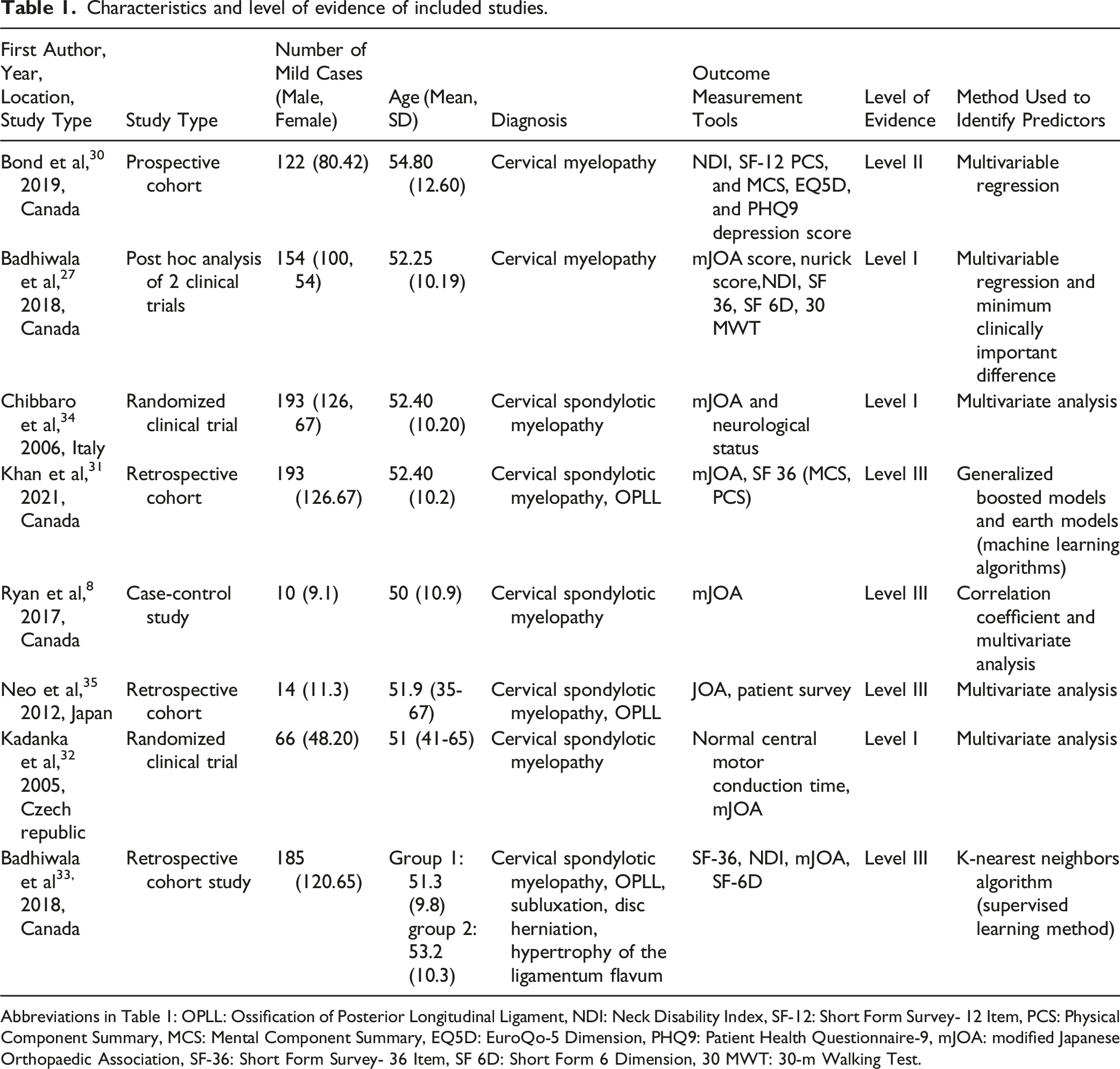
Abbreviations in Table 1: OPLL: Ossification of Posterior Longitudinal Ligament, NDI: Neck Disability Index, SF-12: Short Form Survey- 12 Item, PCS: Physical Component Summary, MCS: Mental Component Summary, EQ5D: EuroQo-5 Dimension, PHQ9: Patient Health Questionnaire-9, mJOA: modified Japanese Orthopaedic Association, SF-36: Short Form Survey- 36 Item, SF 6D: Short Form 6 Dimension, 30 MWT: 30-m Walking Test.
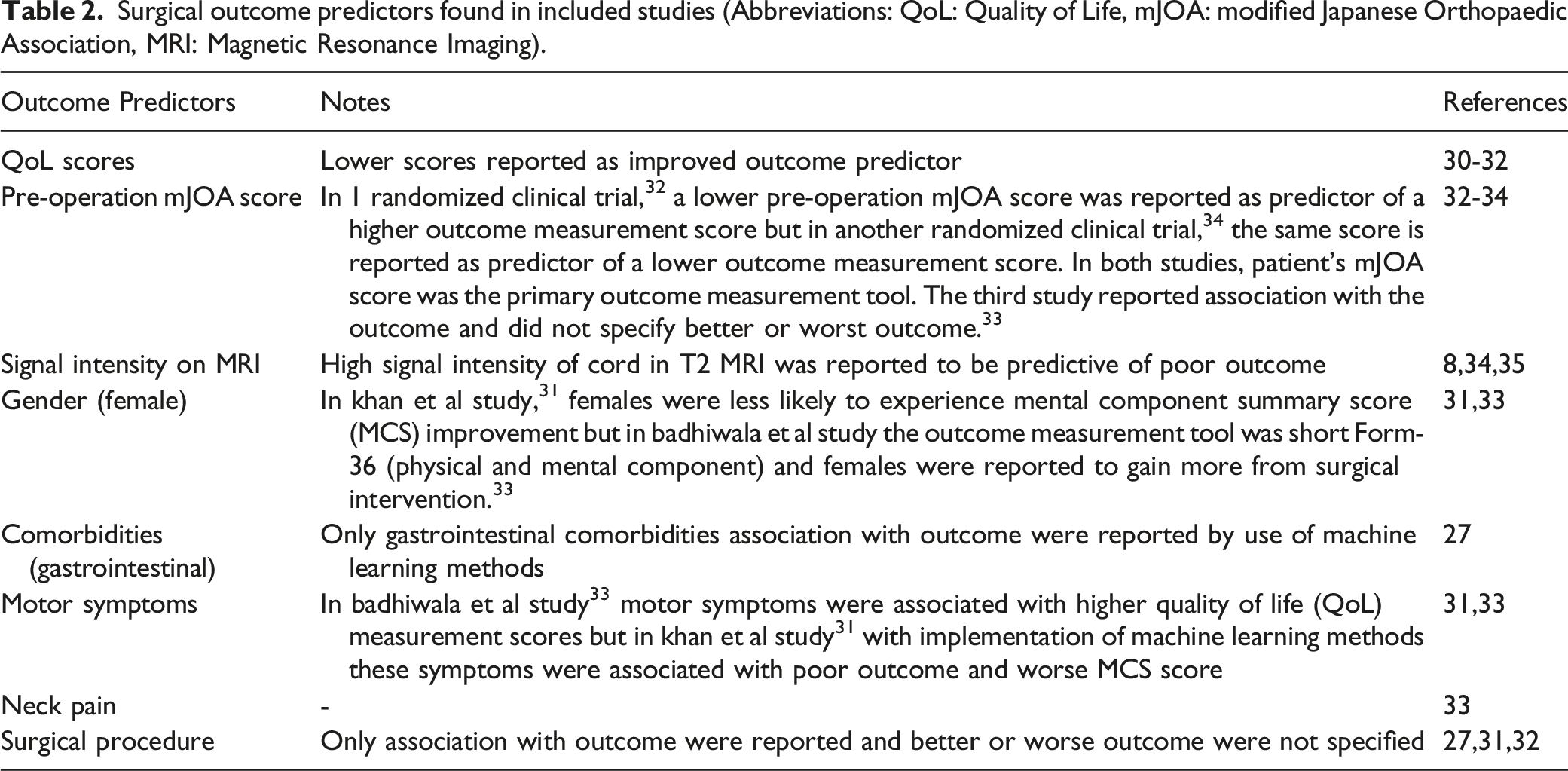
Surgical outcome predictors found in included studies (Abbreviations: QoL: Quality of Life, mJOA: modified Japanese Orthopaedic Association, MRI: Magnetic Resonance Imaging).
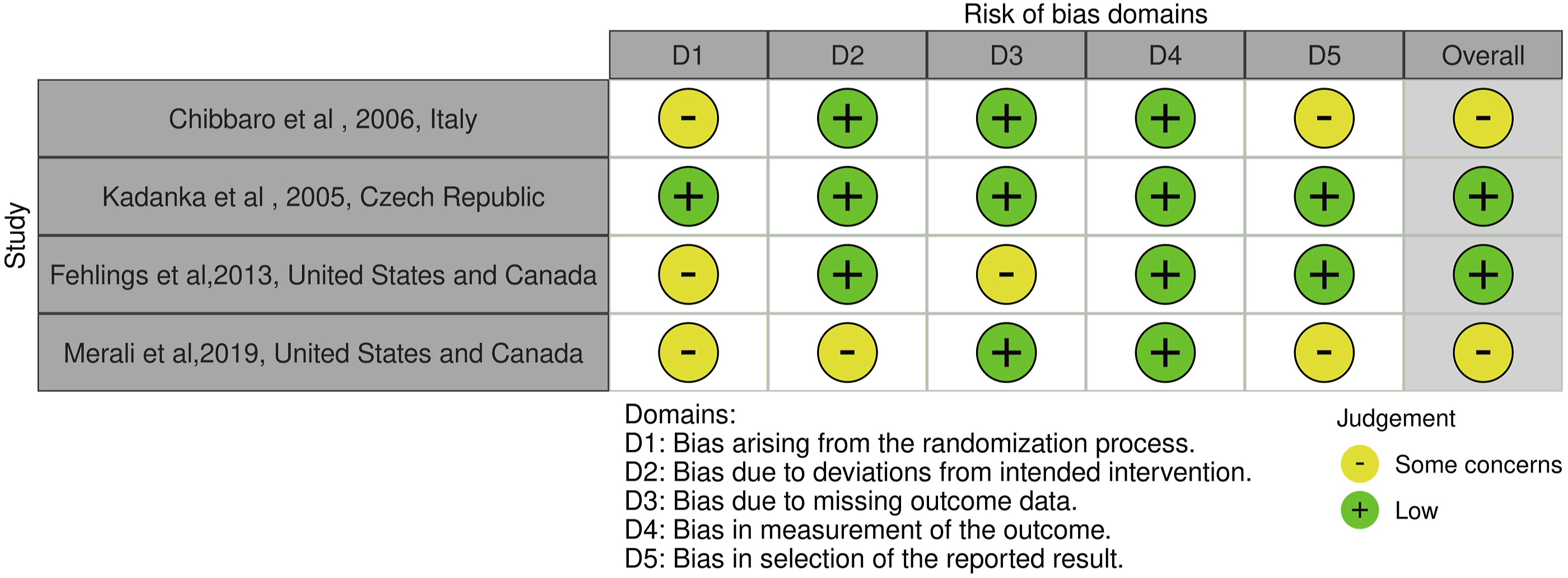
Risk of Bias assessment using RoB 2 tool for randomized clinical trials.
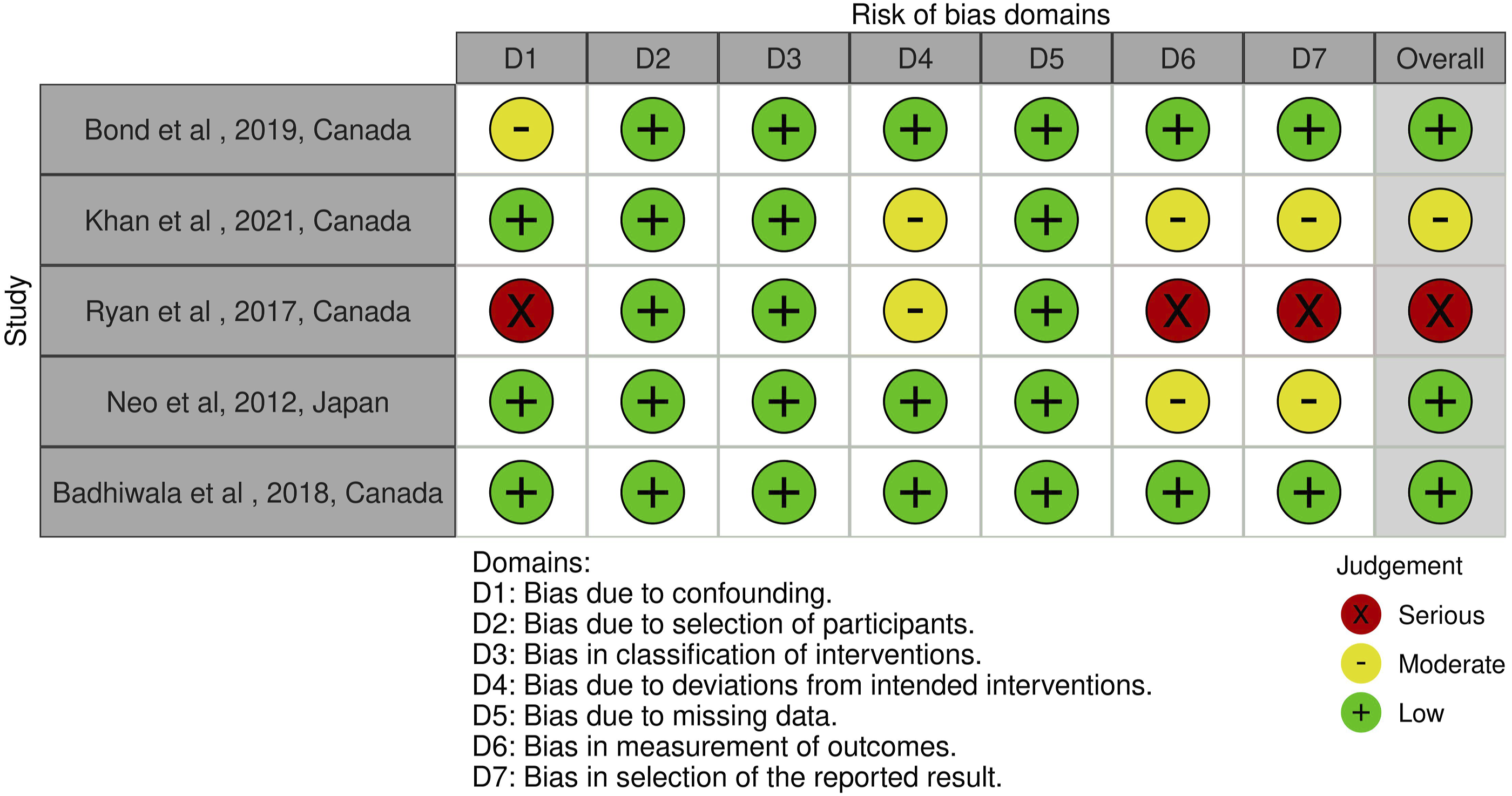
Risk of Bias assessment using ROBINS-1 tool for non-randomized studies.
Quality of Life Scores
Pre-operative Quality of Life (QoL) measurement tools were reported in 3 studies.30-32 In these studies, lower pre-operation QoL life measurement scores were predictors of surgical outcome. In these studies, patients with lower initial more inadequate Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were reported as more likely to present a meaningful increase in the outcome measurement tools.30-32 In Khan et al study, machine learning methods such as generalized boosted and earth models were implemented to find outcome predictors. 31 Lower PCS and MCS score before surgical intervention were reported as predictors of a better outcome. 31
Pre-Operation mJOA Score
Three studies address the pre-operation mJOA association with surgical outcomes.32-34 In a randomized clinical trial (RCT) conducted by Chibbaro et al, the severity of pre-operative dysfunction, measured by mJOA score, was reported to be highly predictive of a lower post-operative mJOA score. 34 In an RCT study by Kadanka et al, the more serious clinical picture was expressed in the pre-operative mJOA score and was predictive of a more significant improvement in the mJOA score. 32 In Badhiwala et study, with the use of principal component analysis (PCA), a group of variables including age, race, pre-operation mJOA (as a measure of severity of myelopathy), etiology of DCM (OPLL and spondylosis, comorbidities (current smoker, gastric, and coronary artery disease), and laminoplasty were reported to be associated with the surgical outcome 27 (Table 1).
Low Signal Intensity of Cord in T1 Magnetic Resonance Imaging (MRI)
In Chibbaro et al 34 study and Neo et al study, 35 the low signal intensity of the cord on T1 Magnetic Resonance Imaging (MRI) or high signal intensity of the spinal cord on T2 MRI sequences were reported as predictors of surgical outcome for mild DCM. In these studies, MRI signal intensity of the cord was reported as a predictor of lower post-operation outcome measurement scores. More specifically, in Neo et al study, patients with these changes on pre-operative MRI of the cord were reported to have a higher risk of residual numbness post-operation. 35 In Kadanka et al randomized clinical trial of mild DCM, signal intensity was evaluated as a potential predictor and reported as not predictive of the outcome as a secondary outcome. 32 In addition, other variables derived from imaging, including the area of the spinal cord at the level of maximum compression, spinal cord parameters at the stenotic level, spinal canal diameter at the stenotic level, and Pavlov’s index, were not associated with the surgical outcome.
Gender and Comorbidities
The relationship between gender and outcome has been explored. In the Khan et al study, Females were less likely to experience improvement in MCS scores after surgery. However, Badhiwala et al study utilized an unsupervised machine learning approach and K-nearest neighbors algorithm to report patients’ phenotype of mild DCM, neck pain, motor symptoms, and female gender associated with better outcomes measured by improvement in Neck Disability Index (NDI) and SF-36 scores.31,33 In Badhiwala et al study using machine learning methods, gastric comorbidities showed little association with outcome. 27 Race and comorbidities, except for gastrointestinal diseases, showed no association with outcome measurement tools in this study.
Motor Symptoms and Neck Pain
In 2 studies, motor symptoms before intervention predicted improved QoL scores after surgery. In Badhiwala et al study, clumsy hands, gait difficulty, and motor weakness were grouped as motor symptoms, and patients with these symptoms were reported to have more improvement in QoL measurement scores after surgical intervention. 33 In another study by Khan et al, lower limb spasticity, the presence of a Babinski sign, and hand clumsiness were associated with poor MCS scores. 31 In addition, in Badhiwala et al study, neck pain was reported as a predictor of better surgical outcomes and quality of Life (QoL). 33
Surgical Procedure
In Kadanka et al 32 study, a surgical procedure including the surgeon’s experience was reported as an outcome predictor, and more specifically, in the study by Khan et al 31 with the use of machine learning methods anterior corpectomy and operation at C3 level were a predictor of better outcomes measured by MCS. In Badhiwala et al study, 27 the PCA group of variables, including the surgical approach, were reported to be associated with outcome. For instance, a group of variables, including age, race, mJOA score, OPLL, spondylosis, current smoker, coronary artery disease, gastric comorbidities, and laminoplasty, was reported to have an association with the outcome.
Variables Evaluated and Not Reported as Outcome Predictors
Variables such as age, number of involved levels (single or multiple), Body Mass Index (BMI), duration of symptoms, race, Pavlov’s Index, and height were evaluated by the included studies, and no association with outcome was reported.30-32,34 Two randomized clinical trials evaluated age as a potential predictor (RCT), and both studies found no association between age and surgical outcome. The same 2 RCTs found no association between surgical outcome and the number of involved levels as another potential outcome predictor.32,34
Discussion
Operative management and timing of treatment for mild DCM cases are not straightforward, and there is a paucity of non-operative and surgical intervention treatments to perform a meta-analysis. Physicians having accurate outcome predictors in mild cases is valuable in defining optimal decision-making in mild DCM.
Numerous QoL measurement tools EuroQol- 5d (EQ-5D) or SF-36 MCS and PCS components, were reported as surgical outcome predictors for DCM.30,31 Mild DCM cases that have declined quality of life are candidates to benefit from surgical intervention. These cases have more improvement in outcome measurement scores.
Furthermore, the causes of the patient’s loss of QoL may affect outcomes. Badhiwala et al reported that cervical pain before surgery was a key driver of QoL improvement after surgery. 36 Studies reported that the resolution of neck pain is also essential to patients' satisfaction with surgery and the critical driver for patients opting for surgery. 37 Apart from neck pain and its role in patients' satisfaction, motor symptoms such as gait difficulty and hand clumsiness were reported by a survey of AO Spine as the most critical symptoms in predicting surgical outcomes in patients with DCM. 38 Mild DCM cases with motor symptoms were reported by 1 RCT to have an association with more improvement in outcome measurement score and patient satisfaction from the outcome and by another study to be predictive of poor outcome reflected by worse MCS score after surgery.31,33 Previous literature on mild, moderate, and severe DCM cases reported that motor symptoms such as lower limb spasticity, upgoing plantar reflexes, hyperreflexia, and hand numbness were associated with less functional status improvement (measured by mJOA).39-43 One retrospective cohort in this study with only mild motor symptoms was reported to predict a better outcome and in this study, the outcome measurement tool was a QoL score. 33 Studies using functional outcome measurement tools such as mJOA reported motor symptoms as unfavorable outcome predictors, but in 1 study using QoL scoring tools for outcome measurement, motor symptoms were associated with favorable outcomes.33,39-43
In 3 of the 8 studies in this systematic review, lower mJOA scores before surgery were associated with improved outcomes. In all 3 studies, outcome measures were neurological status and mJOA. However, in the study by Badhiwala et al, 33 on 185 mild DCM cases, pre-operation mJOA scores were evaluated as a surgical outcome predictor, and no associations were reported. In Chibbaro et al, 34 the lower pre-operation mJOA score was associated with a lower post-operative mJOA score, and the primary outcome measure was the mJOA score, while in Kadanka et al study, 32 a lower mJOA score was reported to be highly predictive of improved surgical outcome. All 3 studies, after data analysis, noted that pre-operation was a surgical outcome predictor. Previous studies on mild cases showed improvement in mJOA scores after surgery. However, the findings of previous studies are not in line with each other the improvement of this score in mild cases is minimal, and it showed that mJOA had its limitation as an outcome measurement tool for mild cases as patients’ quality of life reported to improved regardless of improvement in mJOA score.12,30,33,44,45 In DCM cases, the mJOA score has been implemented to evaluate functional impairment, but it has limitations for the assessment of mild cases because of the ceiling effect at the end of the mJOA scale (score of 15, 16, 17). Therefore, using mJOA as the only outcome measurement tool or comparing pre-operation and post-operation mJOA scores limits the outcome assessment because of smaller improvements in mJOA scores. This has led to the suggestion of using the QoL measurement tool for assessing patient outcomes in mild DCM cases.31,33 This finding is the reason behind using quality of life measurement tools as outcome measurement tools in more recent studies.27,31
Two studies reported the low signal intensity of the cord on T1 or high signal intensity in T2 MRI sequences as an outcome predictor. In an RCT study by Kadanka et al, 32 the low signal intensity of the cord in T1 MRI was reported to be predictive of worse surgical outcomes, and high signal intensity in T2 MRI was predictive of an improved outcome, and the findings of Neo et al study confirmed the same conclusions. 35 Previous studies suggested that more imaging-related outcome predictors such as anterior-posterior diameter, Pavlov’s index, and area of maximum compression were evaluated by studies, and no association with outcome was found in mild cases.46-48
In Chibbaro et al study, 34 with only mild cases, older age was not associated with the outcome, and the same finding was reached by another RCT study. 32
Regarding gender, there are 2 conflicting reports. In a study with 185 patients by Bidhawala et al, 33 the female gender was reported as gaining more from surgical intervention (more improvement in QoL measurement scores), but the study by Khan et al 31 reported that female cases are less likely to experience improvement in MCS component of SF-36. Regarding comorbidities, evaluating current evidence is problematic since, in the Badhiwala study, 27 PCA was used, and comorbidities like cardiovascular and cardiorespiratory were associated with outcomes while grouped with other variables. This study contains significant findings, but interpreting it with other studies is tricky. However, in Khan et al study, 31 the use of machine learning methods revealed interesting findings. The first important finding was the association of gastrointestinal comorbidities with the outcome, which has not been reported in previous studies, and the reason for this finding was the use of machine learning methods that could identify more findings because of its nature and the second important finding was that no other comorbidities were associated with outcome. In Khan et al study, 31 an association between gastrointestinal comorbidities and an improved SF-36 score was reported. Gastrointestinal symptoms could happen both due to cervical myelopathy and gastrointestinal (GI) comorbidities and in patients with a known history of GI problems, it is possible that GI symptoms of DCM go unnoticed. Patients themselves even could attribute these symptoms to their own comorbidity rather than cervical myelopathy. Also, mJOA as a tool for assessment of DCM does not include any measure for the GI system and we could assess the related symptoms. This argument is previously reported in the literature about GI symptoms and the lack of a tool for the assessment in DCM patients.27,49
In 1 randomized clinical trial study, only mild cases of surgical procedures and the experience of a surgeon with a specific approach were associated with the outcome of the surgery, but the number of involved and operating levels were not related to surgical outcome. 32 Finally, Physical attributes like height, weight, and BMI were not associated with the outcome unless in the PCA study by Badhiwala et al grouped with other variables. 27
This study presented the current outcome predictor of surgical intervention in mild DCM cases. This study’s result addresses a research priority in DCM patients. 21 There is a stronger tendency for surgical intervention in DCM patients, yet optimizing candidates for surgery is still a matter of discussion, especially in mild cases, and identifying outcome predictors is the answer. The result of this study is limited by the data reported by the included papers. In mild cases, previous studies did not compare results by the type of surgical approach (anterior or posterior) and this limits us to find further information on the effects of choosing a surgical approach on clinical outcome.
Conclusion
The lack of consensus on the role of surgery in mild DCM cases is driven by the limitation of existing literature, which makes finding surgical outcome predictors as important part of a better understanding of the role of surgery. Lower pre-operative mJOA score, lower quality of life before surgery (low EQ-5D or SF-36 score), neck pain and motor symptoms, and higher signal intensity of cord in T2 MRI, female gender, and gastrointestinal comorbidities are surgical outcome predictors found in the literature. Lower QoL score and neck prior to surgery were reported as predictors of more improved outcomes, but high cord signal intensity in T2 MRI was reported as an unfavorable outcome predictor.
Footnotes
Author contributions
The authors confirm contributions to the paper as follows: Study conception and design: Vafa Rahimi-Movaghar, Farzin Farahbakhsh, Seyed Mohammad Ghodsi, Sepehr Khosravi, Zahra Ghodsi; Screening and Data Collection: Sepehr Khosravi, Marjan Hessari, Alireza Shahmohammadi, Alireza Aliakbargolkar, Zahra Eskandari; data analysis: Farzin Farahbaksh, Vali Baigi; draft manuscript preparation: Sepehr Khosravi, James S Harrop, Marjan Hessari, Zahra Ghodsi, Vafa Rahimi-Movagahr. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tehran University of Medical Sciences [grant number is 99-2-93-49833].
Ethical Approval
The Ethics Committee of Tehran University of Medical Sciences, approved the study, and the reference number is IR.TUMS.SINAHOSPITAL.REC.1399.085.