
Abstract
Study Method:
Systematic review (update).
Objective:
Degenerative cervical myelopathy (DCM) is a degenerative spine disease and the most common cause of spinal cord dysfunction in adults worldwide. The objective of this study is to determine the natural history of DCM by updating the systematic review by Karadimas et al. The specific aims of this review were (1) to describe the natural history of DCM and (2) to determine potential risk factors of disease progression.
Method:
An updated search based on a previous protocol was conducted in PubMed and the Cochrane Collaboration library for studies published between November 2012 and February 15, 2015.
Results:
The updated search yielded 3 additional citations that met inclusion criteria and reported the incidence of spinal cord injury and severe disability in patients with DCM. Based on 2 retrospective cohort studies, the incidence rate of hospitalization for spinal cord injury is 13.9 per 1000 person-years in patients with cervical spondylotic myelopathy and 4.8 per 1000 person-years in patients with myelopathy secondary to ossification of the posterior longitudinal ligament (OPLL). In a third small prospective study, the risk of being wheelchair bound or bedridden was 66.7% in DCM patients with OPLL.
Conclusion:
The overall level of evidence for these estimated rates of hospitalization following spinal cord injury was rated as low.
Introduction
Degenerative cervical myelopathy (DCM) is a degenerative spine disease and the most common cause of spinal cord dysfunction in adults worldwide. 1 The term DCM encompasses cord compression secondary to osteoarthritic changes to the spine, disc degeneration, ligamentous aberrations, and progressive kyphosis. Patients with DCM may present with a wide range of neurological signs and symptoms, including pain, lower limb spasticity, decreased hand dexterity, hyperreflexia, and sphincter disturbance.
The pattern of progression in DCM is not well defined. Early reports of the natural history suggest that DCM is a relatively benign disorder and that patients are more likely to remain stable over time than to deteriorate. 2 In the most recent systematic review of the literature, there was moderate evidence that 20% to 62% of patients with symptomatic myelopathy will decline by at least 1 point on the Japanese Orthopaedic Association scale if not managed surgically. 3 The objective of this study was to update the systematic review by Karadimas et al 3 that investigated (1) the natural history of DCM and (2) the potential risk factors of disease progression.
Materials and Methods
Electronic Literature Search
An updated search based on a previous protocol 4 was conducted in PubMed and the Cochrane Collaboration library for studies published between November 2012 and February 15, 2015. Inclusion and exclusion criteria for the search were previously published, as well as methods for data abstraction, data analysis, evaluation of study quality, and assessment of the overall strength of evidence.
Results
Study Selection
The updated electronic search yielded 122 new citations (Figure 1). An additional 40 citations were identified through directed manual search. One hundred and fifty-seven studies were excluded following title and abstract review, and 5 studies were further investigated. Following full text review, a single study was excluded because all patients underwent surgery for DCM, and another for including nonmyelopathic patients with ossification of the posterior longitudinal ligament (OPLL; Table 1). 5 Three other studies presented new information relevant to key question 1 and reported the incidence of spinal cord injury and severe disability in patients with DCM. 6 –8
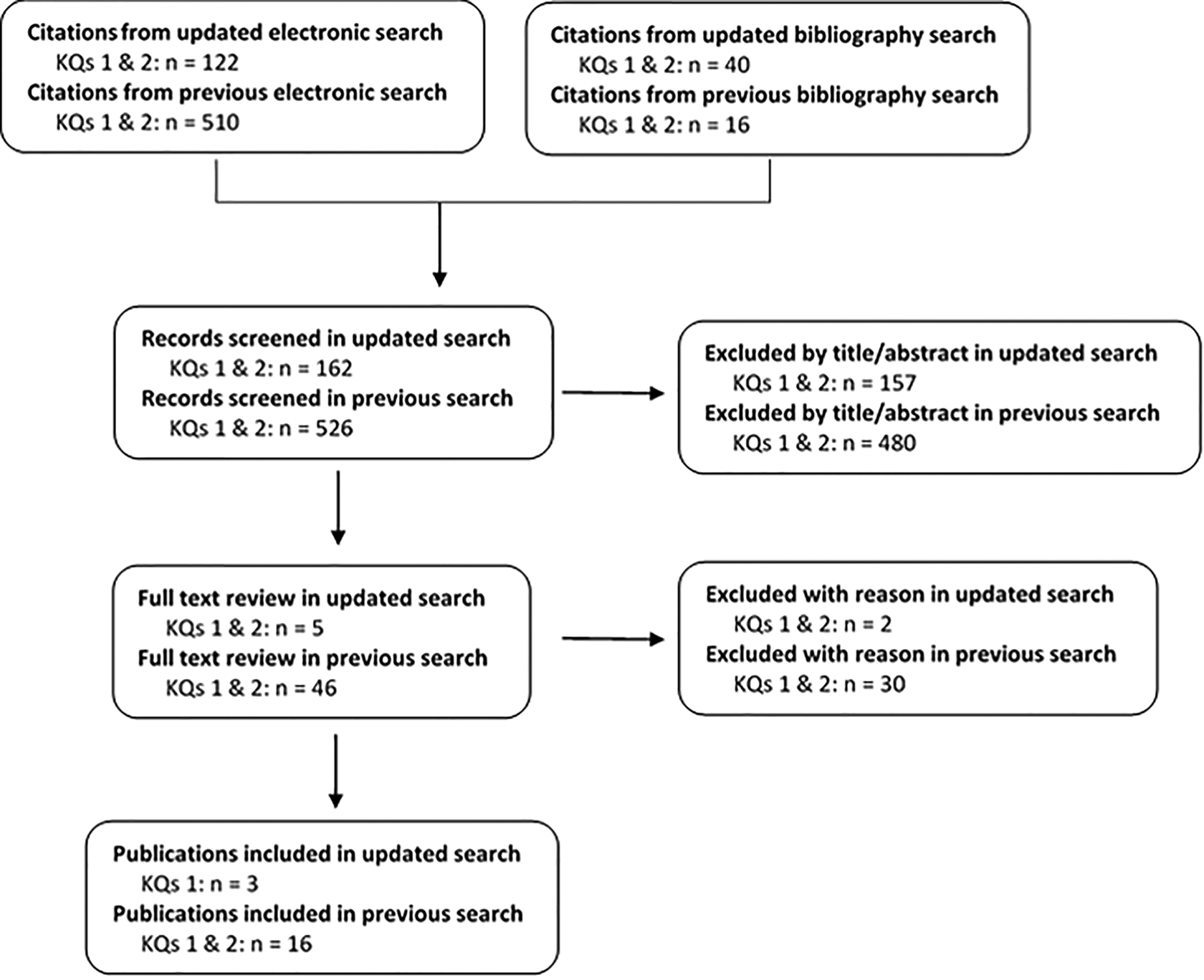
Results of updated and originally published literature searches. KQ = key question.
Excluded Studies and Reasons for Exclusion.
Abbreviation: OPLL, ossification of the posterior longitudinal ligament.
Two retrospective cohort studies used the National Health Insurance Research Database, which contains records for 23 million administered insurants in Taiwan (approximately 99% of the entire population). 7,8 The first study included 14 140 patients hospitalized for cervical spondylotic myelopathy (CSM) with at least 1 year of follow-up (Table 2). 8 The second study consisted of 5604 patients with myelopathy secondary to OPLL and at least 3 years of follow-up. 7 A third prospective cohort study reported outcomes on 450 patients with myelopathy secondary to OPLL; however, only 36 were managed conservatively after refusing surgical treatment.
Characteristics of New Studies Addressing the Natural History of DCM.

Abbreviations: DCM, degenerative cervical myelopathy; ICD-9, International Classification of Diseases, Ninth Edition; CSM, cervical spondylotic myelopathy; NR, not reported; OPLL, ossification of the posterior longitudinal ligament.
aN = 450 in study; 36 patients were treated conservatively for myelopathy symptoms.
Hospitalization for Spinal Cord Injury
Based on 2 retrospective cohort studies, the incidence rate of hospitalization for spinal cord injury was 13.9 per 1000 person-years (95% confidence interval [CI] = 11.6-16.6) in patients diagnosed with CSM 8 and 4.8 per 1000 person-years (95% CI = 2.3-10.1) in patients with myelopathy secondary to OPLL 7 (Table 3). The rate of hospitalization for spinal cord injury in patients with DCM from OPLL was significantly higher than the rate observed in a healthy population (0.18 per 1000 person-years; hazard ratio = 32.2; 95% CI = 10.4-99.0; P < .001). 7 These studies both had moderately low risk of bias (Table 4).
Incidence Rate or Risk of Spinal Cord Injury and Disability in Patients Not Treated Surgically.
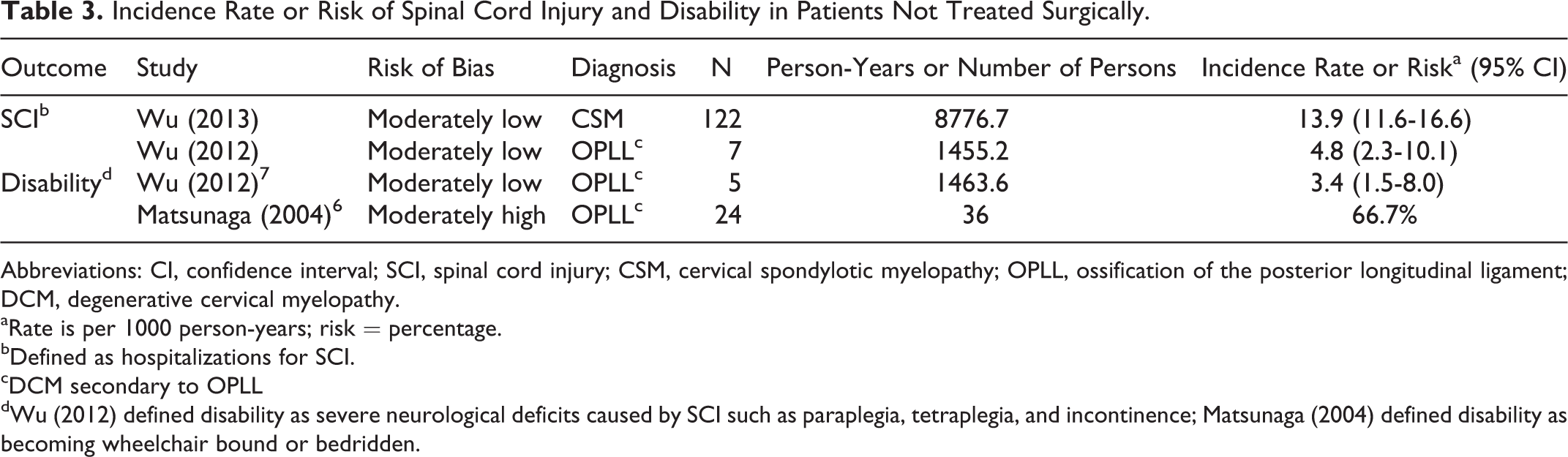
Abbreviations: CI, confidence interval; SCI, spinal cord injury; CSM, cervical spondylotic myelopathy; OPLL, ossification of the posterior longitudinal ligament; DCM, degenerative cervical myelopathy.
aRate is per 1000 person-years; risk = percentage.
bDefined as hospitalizations for SCI.
cDCM secondary to OPLL
dWu (2012) defined disability as severe neurological deficits caused by SCI such as paraplegia, tetraplegia, and incontinence; Matsunaga (2004) defined disability as becoming wheelchair bound or bedridden.
Class of Evidence for Prognostic Studies.
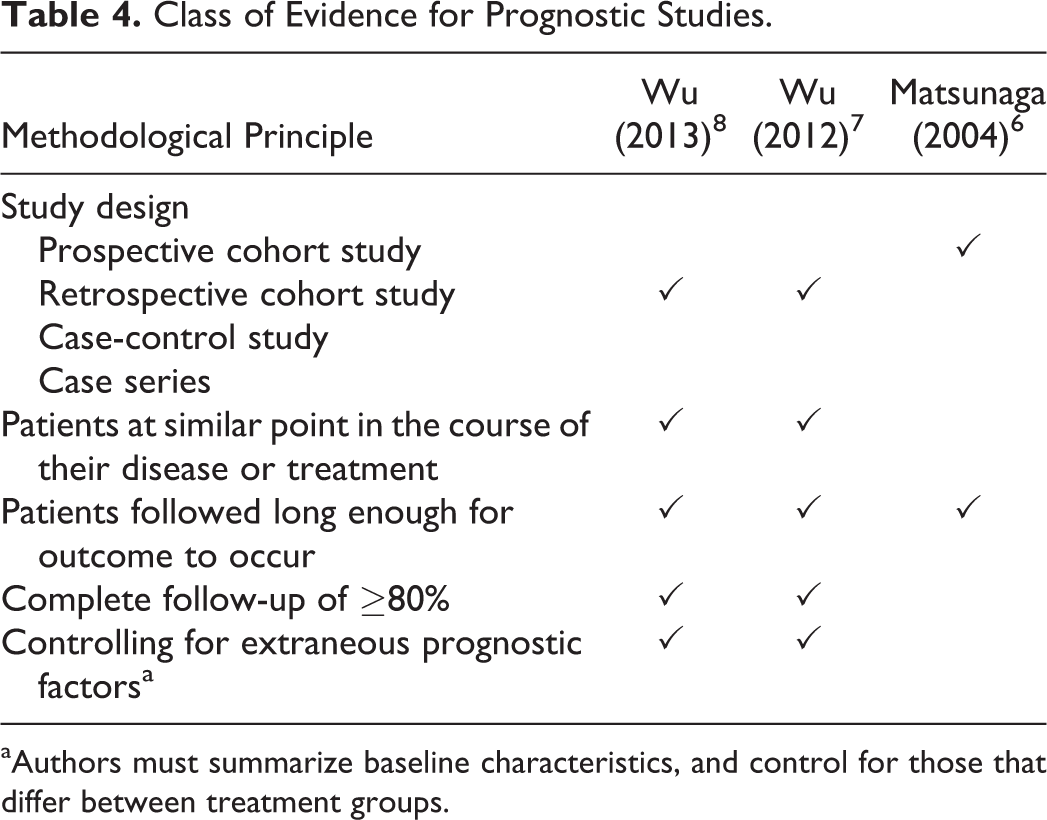
aAuthors must summarize baseline characteristics, and control for those that differ between treatment groups.
Disability
One large retrospective study evaluated the incidence of severe neurological deficits from spinal cord injury in patients with CSM, including paraplegia, tetraplegia, and incontinence; the reported rate was 3.4 per 1000 person-years. 7 A second small prospective study reported that the risk of being wheelchair bound or bedridden was 66.7% (24/36) in patients with DCM secondary to OPLL (Table 3). 6 This study had moderately high risk of bias (Table 4).
Evidence Summary
The rate of hospitalization due to spinal cord injury was 4.8 per 1000 person-years in patients with DCM secondary to OPLL and 13.9 per 1000 person-years in patients with CSM. The rate of severe disability in DCM patients with OPLL was 3.4 per 1000 person-years. The strength of evidence for these estimates was Low (Table 5).
Evidence Summary.
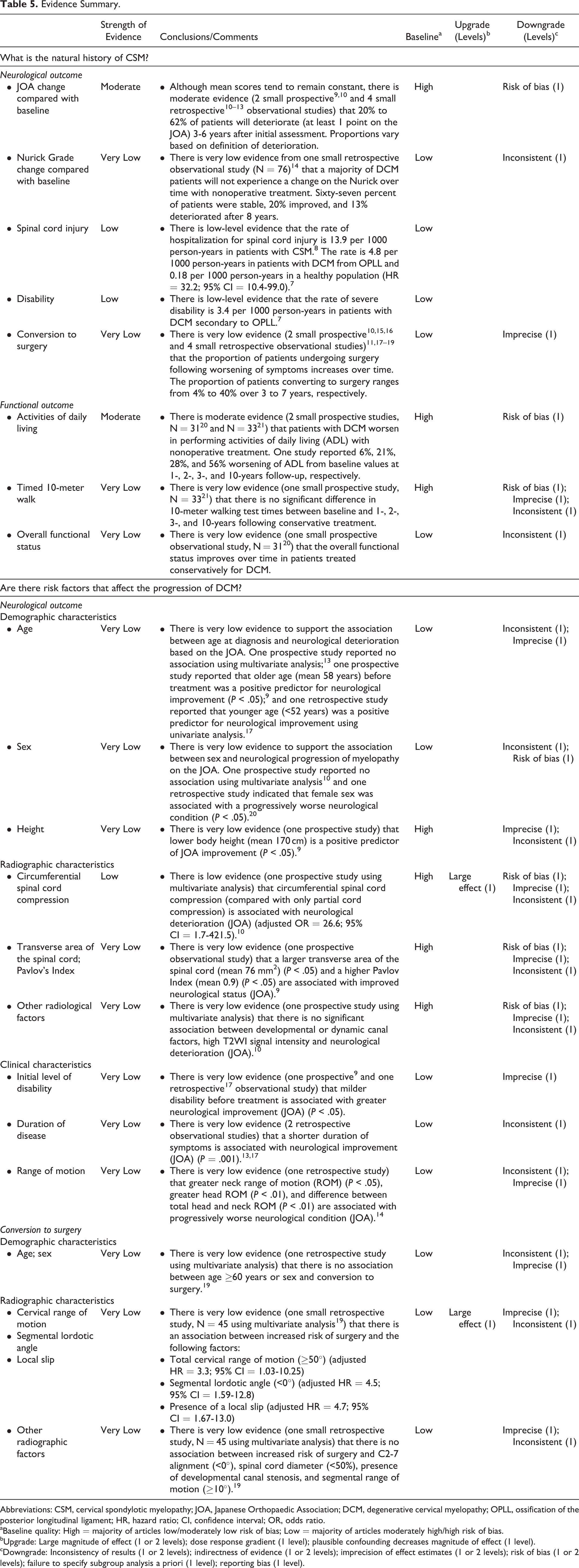
Abbreviations: CSM, cervical spondylotic myelopathy; JOA, Japanese Orthopaedic Association; DCM, degenerative cervical myelopathy; OPLL, ossification of the posterior longitudinal ligament; HR, hazard ratio; CI, confidence interval; OR, odds ratio.
aBaseline quality: High = majority of articles low/moderately low risk of bias; Low = majority of articles moderately high/high risk of bias.
bUpgrade: Large magnitude of effect (1 or 2 levels); dose response gradient (1 level); plausible confounding decreases magnitude of effect (1 level).
cDowngrade: Inconsistency of results (1 or 2 levels); indirectness of evidence (1 or 2 levels); imprecision of effect estimates (1 or 2 levels); risk of bias (1 or 2 levels); failure to specify subgroup analysis a priori (1 level); reporting bias (1 level).
Conclusions
The results of this update indicate that the presence of OPLL or CSM may increase a patient’s risk of severe disability and hospitalization for spinal cord injury. Although these findings are unlikely to directly influence management strategies, patients should be counseled of the possibility of spinal cord injury when discussing the benefits and risks of various treatment options.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AOSpine and also received funding from the Cervical Spine Research Society (CSRS). Dr Fehlings wishes to acknowledge support from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration and the DeZwirek Family Foundation. Dr Tetreault acknowledges support from a Krembil Postdoctoral Fellowship Award.