
Abstract
Degenerative cervical myelopathy (DCM) is a progressive spine disease and the most common cause of spinal cord dysfunction in adults worldwide. Patients with DCM may present with common signs and symptoms of neurological dysfunction, such as paresthesia, abnormal gait, decreased hand dexterity, hyperreflexia, increased tone, and sensory dysfunction. Clinicians across several specialties encounter patients with DCM, including primary care physicians, rehabilitation specialists, therapists, rheumatologists, neurologists, and spinal surgeons. Currently, there are no guidelines that outline how to best manage patients with mild (defined as a modified Japanese Orthopedic Association (mJOA) score of 15-17), moderate (mJOA = 12-14), or severe (mJOA ≤ 11) myelopathy, or nonmyelopathic patients with evidence of cord compression. This guideline provides evidence-based recommendations to specify appropriate treatment strategies for these populations. The intent of our recommendations is to (1) help identify patients at high risk of neurological deterioration, (2) define the role of nonoperative and operative management in each patient population, and (3) determine which patients are most likely to benefit from surgical intervention. The ultimate goal of these guidelines is to improve outcomes and reduce morbidity in patients with DCM by promoting standardization of care and encouraging clinicians to make evidence-informed decisions.
Keywords
Introduction and Background Information
Degenerative cervical myelopathy (DCM) is a progressive degenerative spine disease and the most common cause of spinal cord dysfunction in adults worldwide. 1,2 The underlying pathophysiology involves age-related degeneration of the tissues of the spinal column, resulting in static spinal cord compression, and repetitive dynamic injury due to increased spinal column mobility. 3 The structural changes involved in DCM include (1) degeneration of intervertebral discs, vertebral bodies, and facet joints; (2) hypertrophy of the ligamentum flavum; and (3) ossification of the posterior longitudinal ligament (OPLL). 4 These changes significantly narrow the spinal canal and reduce the space available for the spinal cord. Compression of the spinal cord results in a series of pathobiological events, which may impair normal neurological function and cause irreversible cytological and histological damage: (1) ischemia and alterations of vascular architecture, (2) endothelial cell impairment and disruption of the blood spinal cord barrier, (3) neuroinflammation, and (4) oligodendrocyte and neuronal apoptosis. 5,6
Aging initially leads to biochemical and biomechanical alterations to the spine, which can progress to micro- and macrostructural changes to its anatomy. 7 The degenerative process begins as the discs degenerate and can no longer maintain their weight-bearing and load-transferring functions. 8 As a result, there is increased stress on the articular cartilage endplates which results in synovial inflammation, joint space narrowing and facet hypertrophy. Compensatory mechanisms include (1) development of osteophytes to increase the surface area of the endplates and to stabilize abnormal spinal mobility, (2) stiffening and buckling of the ligamentum flavum in response to reduced disc height and straightening of cervical lordosis, and (3) hypertrophy or ossification of other ligaments. In the most recent evaluation of asymptomatic patients, Nakashima et al 9 reported significant disc bulging in 87.6% of volunteers aged 20 to 79 years. Others studies have identified that 70% to 95% of individuals aged 60 to 65 years display evidence of degenerative changes on lateral cervical spine radiographs 10 and that 86% of subjects over the age of 60 years exhibit varying degrees of disc degeneration. 11 Although spinal degeneration is common in the elderly population, only a small portion will eventually develop myelopathy.
Patients with significant spinal cord compression may present with common signs and symptoms of neurological dysfunction. The underlying degenerative spinal pathology may cause localized and radiating neck pain. 1,12 Neurological symptoms include paresthesia (numbness and tingling), abnormal gait/balance and falls, decreased hand dexterity, and sphincter dysfunction. Concomitant radicular pain and weakness may also be present from spinal nerve root compression. Signs on clinical examination include upper motor neuron features of hyperreflexia and increased (spastic) tone, sensory and motor dysfunction, and gait abnormality. DCM is diagnosed when a patient presents with signs and symptoms consistent with myelopathy and image (usually magnetic resonance imaging [MRI]) evidence of spinal cord compression.
Differential diagnoses of the clinical presentation are important to consider, including intracranial, demyelinating, motor neuron, infectious, inflammatory, and metabolic diseases. 13 In a recent narrative review, Kim et al 13 identified multiple sclerosis, vitamin B12 deficiency, amyotrophic lateral sclerosis, and peripheral nerve entrapment as the major differential diagnoses of DCM. This review concluded that a combination of clinical and imaging findings is necessary to confirm the diagnosis of DCM and to rule out other diagnoses.
Previous Guidelines
In 2009, the Joint Section on Disorders of the Spine and Peripheral Nerves of the American Association of Neurological Surgeons/Congress of Neurological Surgeons undertook an initiative to develop recommendations for the surgical management of cervical degenerative disease. Topics in this focus issue included the natural history of DCM, clinical and imaging predictors of surgical outcome, surgical techniques (laminectomy, laminoplasty, and anterior decompression), functional assessment tools, management of pseudoarthrosis, and electrophysiological monitoring during surgery. Recommendations for each of these topics were formulated by a panel of experts in orthopedic or neurosurgery and were based primarily on an assessment of the current body of evidence. Expert consensus was used to develop each recommendation and to assign a final grade for strength.
In 2013, a second focus issue on DCM was published in Spine and included recommendations and consensus statements for the natural history of DCM, predictors of neurologic dysfunction in the nonmyelopathic patient, nonoperative management, differential diagnosis, imaging predictors of outcome, ancillary outcome assessment tools, genetics and heritability, the influence of spinal deformity on management, and surgical treatments. Similarly, these recommendations and statements were formulated through expert consensus and a Delphi procedure.
The current guidelines complement the existing focus issues. In addition, the development of these recommendations (1) adhered to current methodological standards; (2) incorporated the opinions of experts in the fields of spine surgery, neurology, rheumatology, rehabilitation medicine, physiatry, and primary care; and (3) considered factors other than the strength of existing evidence, including patient values, resource use, balance of benefits and harms, acceptability, feasibility, and impact on health inequities. These guidelines will provide important recommendations for the management of patients with mild, moderate, and severe disease as well as nonmyelopathic patients with image evidence of canal stenosis and/or cord compression and will consider disease natural history; operative and nonoperative management; and predictors of myelopathy development, neurological deterioration, and treatment outcomes.
Rationale and General Scope
There are several important reasons for developing guidelines for the management of patients with DCM. First, according to the World Health Organization, the proportion of the population older than 60 years is projected to double from 11% in 2010 to 22% in 2050. 7 The aging of the population will be accompanied by an “epidemiologic transition” from communicable to noncommunicable disease and an increase in age-related disorders of the spine, including DCM. 7 This unprecedented upward shift in the age structure of the global population will pose unique challenges to health care systems worldwide as elderly patients tend to have multiple medical comorbidities, decreased mobility, poor balance, a greater propensity to falls and more severe spinal degeneration. Furthermore, these individuals experience age-related changes in the composition of their spinal cord, have reduced physiological reserves, and may be less tolerant of certain interventions. 14,15 By summarizing current evidence, these guidelines will help evaluate the safety and efficacy of various treatment modalities and provide guidance on the management of elderly myelopathic patients.
Second, there is also an increased reported prevalence of myelopathy in individuals aged 50 to 60 years, likely due to improved diagnostic techniques. In the recent prospective AOSpine studies, the mean age of patients (n = 757) was approximately 56 years, 16,17 which is a decade younger than the typical retirement age for many countries. 17 Patients with myelopathy experience greater functional impairment, a decrease in social independence, and substantially reduced quality of life. Long-term disability in patients aged 50 to 60 years also poses greater financial burden on society as individuals in their mid-50s are at the peak of their working career. These guidelines will therefore not only ensure appropriate management in the elderly population but will also define treatment strategies for patients whose professional duties and other activities of daily living might be significantly impaired.
Finally, these guidelines aim to provide clinicians with guidance that is evidence-based and representative of both the state of existing literature and perspectives of various stakeholders. The 3 main areas of focus are (1) the neurological natural history of DCM; (2) the management of mild, moderate, and severe myelopathic patients and the expected outcomes of surgical and non-surgical treatment; and (3) the management of nonmyelopathic patients with MRI evidence of cord compression or canal stenosis.
These guidelines will provide the basis for more informed and shared decision-making between clinicians and patients. The ultimate goal of these guidelines is to improve outcomes and reduce morbidity in patients with DCM by decreasing the heterogeneity of management strategies and encouraging clinicians to make evidence-informed decisions.
Overall Objective
The main objective of this guideline is to outline how to best manage patients with mild, moderate and severe myelopathy and nonmyelopathic patients with evidence of cervical cord compression.
Specific Scope and Aspects of Care
Specific conditions that are covered in this guideline include Degenerative cervical myelopathies: Spondylosis/osteophytosis Disc degeneration Disc herniation/bulging Hypertrophy of the ligamentum flavum Ossification of the posterior longitudinal ligament Calcification of the spinal ligaments Degenerative spondylolisthesis Facet hypertrophy Facet joint instability Subluxation
Specific conditions that are not covered in this guideline include Other compressive myelopathies: Spinal epidural abscess Spinal epidural hematoma Syringomyelia Chiari malformation Spinal tumors Spinal cord tumors Noncompressive myelopathies: Traumatic spinal cord injury (including central cord syndrome) Spinal cord infarction Inflammatory and immune myelopathies (eg, multiple sclerosis, rheumatoid arthritis) Radiation myelopathy Infection Amyotrophic lateral sclerosis Radiculopathy Peripheral nerve entrapment Congenital hypermobility syndromes
The following aspects of care are addressed in this guideline: Effectiveness and safety of nonsurgical treatment for DCM. Effectiveness and safety of surgical treatment for DCM. The role of preoperative myelopathy severity and duration of symptoms on treatment outcomes. When is the optimal time to operate? Should patients with mild myelopathy be treated surgically? Monitoring and management strategies for nonmyelopathic patients with evidence of cord compression. What patients are at a high risk of myelopathy development?
Specific treatments or aspects of care that are not addressed in this guideline include: The differential diagnosis of DCM. Relative efficacy, effectiveness, and safety of anterior versus posterior surgery. Relative efficacy, effectiveness, and safety of laminoplasty versus laminectomy with fusion. Use of neuroprotective agents such as methylprednisolone or riluzole. Novel imaging and diagnostic techniques. Diagnostic tools to quantify impairment.
Relevant Definitions
This guideline discusses management strategies for patients with either symptomatic degenerative myelopathy or nonmyelopathic patients with evidence of cord compression.
The following definitions are important in order to understand the scope of this guideline:
Cervical myelopathy is defined as a clinical disease involving loss of fine motor control and coordination, gait dysfunction with long tract signs and imaging evidence of cervical cord compression.
Degenerative cervical myelopathy is defined as symptomatic myelopathy caused by degenerative changes to the spinal axis. These include osteoarthritic changes such as spondylosis, disc herniation and facet arthropathy as well as ligamentous aberrations, including calcification, hypertrophy, or ossification of the ligamentum flavum and posterior longitudinal ligament.
4,18
Cervical spondylotic myelopathy is defined as myelopathy secondary to spondylotic changes or disc degeneration.
Ossification of the posterior longitudinal ligament is defined as ectopic bone formation within the posterior longitudinal ligament. Patients with OPLL may be asymptomatic or present with signs and symptoms of myelopathy.
Nonmyelopathic patients have MRI evidence of spinal cord compression and symptoms of neck pain but do not present with signs of myelopathy.
Radiculopathy is defined as compression or irritation of a nerve as it exits the spinal canal. Radiculopathy may be diagnosed through clinical, imaging and/or electrophysiological examination. The modified Japanese Orthopedic Association (mJOA) scale is an investigator-administered DCM-specific index that separately addresses motor function of the upper and lower extremities, sensory function of the upper extremities and sphincter function.
19,20
A score of 18 indicates normal function, whereas a lower score reflects more severe neurological impairment. The mJOA is composed of 2 dimensions, has moderate internal consistency, is responsive to change and demonstrates both convergent and divergent validity.
21
The reliability of the mJOA has not been established. Based on the mJOA score, mild myelopathy is defined as ≥15, moderate as 12 to 14, and severe as ≤11. The Nurick Score is a 6-grade clinician-administered DCM-specific index that focuses on ambulation and employment.
20
Grade 0 = root involvement without spinal cord dysfunction, grade I = signs of spinal cord dysfunction without difficulty in walking, grade II = difficulty in walking without effect on employment, grade III = difficulty in walking with effect on full-time employment, grade IV = can walk only with someone else’s help or with the aid of a frame, and grade V = chair bound or bedridden. The Neck Disability Index is a patient-reported outcome measure which incorporates several components of daily living, including pain intensity, personal care, lifting, reading, headaches, concentration, work, driving, sleeping, and recreation.
20
These 10 subscales are scored from 0 = no disability to 5 = complete disability, summated and multiplied by 2. The higher the score, the greater the disability, with 100 reflecting the maximum score. The Visual Analog Scale (VAS) measures a patient’s pain across a continuum from no pain to extreme pain on an 11-point numerical rating scale.
20
Duration of symptoms is the patient-reported time from symptom onset to treatment. The minimum clinically important difference (MCID) is the smallest change in a treatment outcome that a patient or clinician would define as meaningful.
22
–24
Disease natural history refers to the progress of a disease over time in the absence of intervention.
A successful outcome has been defined differently across studies. The primary objective of treatment is to halt disease progression. Other objectives include to improve function, disability, pain, and quality of life. Success has been defined based on final postoperative score (eg, mJOA ≥ 16), recovery rate or achieving a MCID. A complication is a treatment-related adverse event.
Summary of Contents
Five systematic reviews were conducted to summarize the current body of evidence. Table 1 summarizes the key clinical questions and main results from these reviews. A summary of our recommendations is provided below.
Evidence Summary from the Systematic Reviews used to Develop our Recommendations.
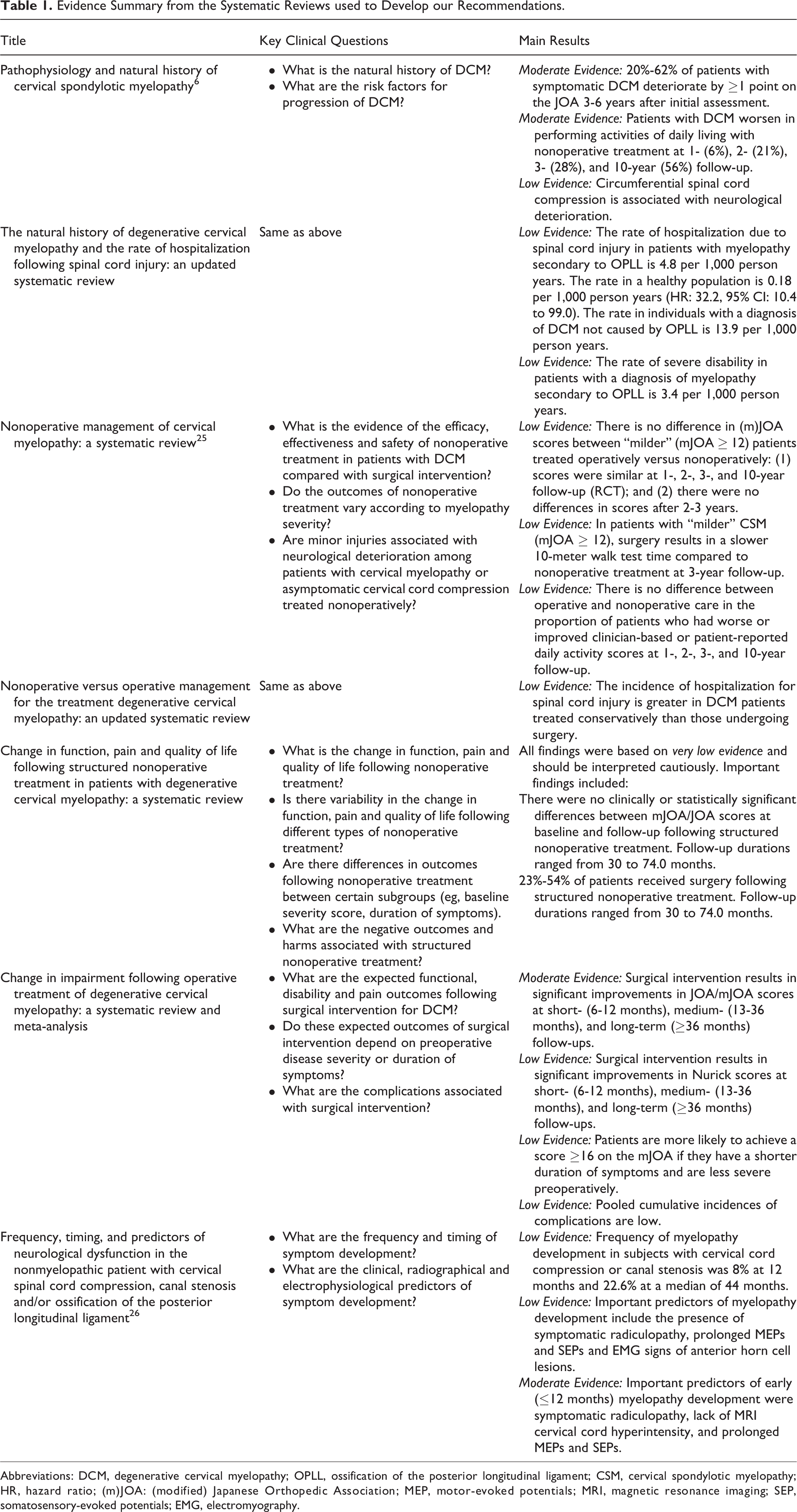
Abbreviations: DCM, degenerative cervical myelopathy; OPLL, ossification of the posterior longitudinal ligament; CSM, cervical spondylotic myelopathy; HR, hazard ratio; (m)JOA: (modified) Japanese Orthopedic Association; MEP, motor-evoked potentials; MRI, magnetic resonance imaging; SEP, somatosensory-evoked potentials; EMG, electromyography.
Patients with severe DCM: We recommend surgical intervention for patients with severe DCM. (Grade: Strong Recommendation; Moderate Evidence)
Patients with moderate DCM: We recommend surgical intervention for patients with moderate DCM. (Grade: Strong Recommendation; Moderate Evidence)
Patients with mild DCM: We suggest offering surgical intervention or a supervised trial of structured rehabilitation for patients with mild DCM. If initial nonoperative management is pursued, we recommend operative intervention if there is neurological deterioration and suggest operative intervention if the patient fails to improve. (Grade: Weak Recommendation; Very Low to Low Evidence)
Nonmyelopathic patients with evidence of cord compression without signs and symptoms of radiculopathy: We suggest not offering prophylactic surgery for non-myelopathic patients with evidence of cervical cord compression without signs or symptoms of radiculopathy. We suggest that these patients be counseled as to potential risks of progression, educated about relevant signs and symptoms of myelopathy, and be followed clinically. (Grade: Weak Recommendation; No Evidence Identified, based on expert opinion)
Nonmyelopathic patients with image evidence of cord compression and clinical and/or electrophysiological evidence of radiculopathy: Nonmyelopathic patients with cord compression and clinical evidence of radiculopathy with or without electrophysiological confirmation are at a higher risk of developing myelopathy and should be counseled about this risk. We suggest offering either surgical intervention or nonoperative treatment consisting of close serial follow-up or a supervised trial of structured rehabilitation. In the event of myelopathic development, the patient should be managed according to the recommendations above. (Grade: Weak Recommendation; Low Evidence).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AOSpine and the Cervical Spine Research Society (CSRS). Dr Fehlings wishes to acknowledge support from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration and the DeZwirek Family Foundation. Dr Tetreault acknowledges support from a Krembil Postdoctoral Fellowship Award.