
Abstract
Study Design:
Systematic review.
Objectives:
To determine the preoperative computed tomography (CT) myelogram imaging parameters in patients diagnosed with degenerative cervical myelopathy (DCM) that correlate with severity of DCM and predict postoperative patients’ functional outcome.
Methods:
An electronic database search was performed using Ovid Medline and Embase. CT myelogram studies investigating the correlation between imaging characteristics and DCM severity or postoperative outcomes were included. Two independent reviewers performed citation screening, selection, qualitative assessment, and data extraction using an objective and blinded protocol.
Results:
A total of 5 studies (402 patients) were included in this review and investigated the role of preoperative CT myelogram parameters in predicting the functional outcome after surgical treatment of DCM. All studies were retrospective cohort studies. CT myelogram characteristics included the transverse area of the spinal cord at maximum level of compression, spinal canal narrowing, number of blocks, spinal canal diameter, and flattening ratio. There is low evidence suggesting that patients with a preoperative transverse area of the spinal cord >30 mm2 at the level of maximum compression have better postoperative recovery and outcome. We found no studies investigating the correlation between preoperative CT myelogram parameters and DCM severity.
Conclusions:
Patients with greater transverse area of spinal cord at the level of maximum compression on the preoperative CT myelogram are more likely to have better neurological outcome after surgery. There is insufficient evidence to suggest that any of the other CT myelogram parameters investigated are predictors of postoperative outcomes in patients with DCM.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is the most common cause of spinal cord disorders in the older population, and its symptoms can progress from paresthesia to weakness or even full tetraplegia. 1 The underlying pathology is degenerative narrowing of the spinal canal at one or more levels that compresses the spinal cord and results in neurological impairment. This degenerative narrowing can be secondary to different etiologies, including cervical disc herniation; an ossified posterior longitudinal ligament (OPLL); cervical kyphosis; or degenerative changes affecting the vertebrae, intervertebral discs, facet joints, uncovertebral joints of the cervical spine, and associated ligaments. 2,3
Magnetic resonance imaging (MRI) is currently the best imaging modality to identify the structural causes of a patient’s myelopathy and visualize neural tissue and spinal cord abnormalities. 2 Computed tomography (CT) scan may also be used to assess the amount of canal compromise, as it is superior to MRI in evaluating bony lesions. 4 Additionally, CT scan was found to be superior to other radiographic modalities in diagnosing and classifying the type of OPLL. 5 Also, it has been used effectively to assess for OPLL progression and for preoperative planning. 6 Although the use of CT myelography has considerably declined in recent years, this invasive procedure is still commonly used in selected cases where MRI is technically difficult or contraindicated. 7,8 Common MRI contraindications include patients with intracranial aneurysm clips, cardiac pacemakers, or implantable cardioverter defibrillators. 9
Some authors believe that the CT scan is complementary to MRI for diagnosing DCM, 8 whereas others perform both imaging tests to further assess cord compression and foraminal stenosis. 8,10,11
Previous systematic reviews have evaluated clinical predictors of outcome, including age; the baseline severity score; duration of symptoms; smoking status; and various signs, symptoms, and comorbidities. 12,13 A recent systematic review also examined possible MRI characteristics that can affect treatment decisions and predict postsurgical outcomes in patients with DCM. 14 Although, CT myelography is an important alternative imaging modality for diagnosing DCM, the relationship between different CT parameters (eg, the spinal canal diameter, degree of cord compression, and neuroforaminal encroachment), and the clinical presentation or outcomes of DCM remain unclear. Clarifying and identifying radiological parameters that are reliable predictors of the surgical outcome would be helpful to determine which patients can benefit from surgical interventions. Furthermore, it will aid in managing patients’ concerns and expectations objectively.
Therefore, the purpose of this systematic review was to answer the following questions: Do any preoperative CT myelogram imaging parameters in patients diagnosed with DCM (1) correlate with the severity of DCM and (2) predict the patients’ postoperative functional outcome?
Methods
Electronic Literature Search and Study Selection
A comprehensive medical literature search was conducted to identify all potential studies published through September 10, 2016. An electronic database search of Ovid Medline, and Embase was performed using medical subject headings and text word searching. Search strategies used for each key question are listed in the Supplemental Digital Content Tables. Only studies on humans that were written in English and contained abstracts were considered for inclusion. Reference lists from relevant articles were individually searched for additional articles. To determine CT myelogram imaging parameters in patients with DCM that correlated with the disease severity, we sought studies that aimed to correlate CT scan or CT myelography characteristics with the severity of DCM symptoms. Using objective severity measures, including the modified Japanese Orthopaedic Association (mJOA) score, JOA recovery rate, Nurick grade, and neck disability index (NDI). To evaluate preoperative CT myelogram imaging parameters in patients diagnosed with DCM that could predict the postoperative outcome, we identified studies that were performed to evaluate preoperative CT myelography parameters affecting post-surgery outcomes in patients treated for DCM. The inclusion and exclusion criteria are presented in Table 1.
Inclusion and Exclusion Criteria.
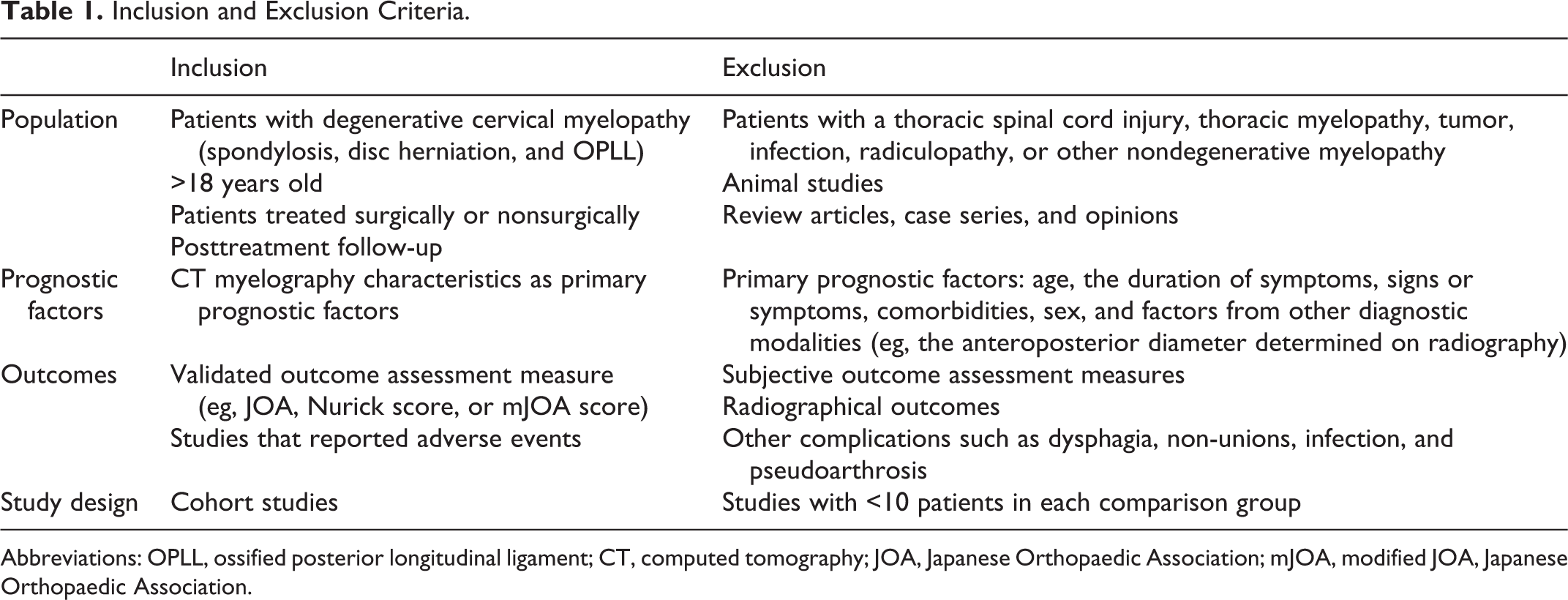
Abbreviations: OPLL, ossified posterior longitudinal ligament; CT, computed tomography; JOA, Japanese Orthopaedic Association; mJOA, modified JOA, Japanese Orthopaedic Association.
Two independent reviewers (F.W. and F.A.) screened titles and abstracts for eligibility, and were blinded to the authors, institutions, and journal of publication. Based on the abstract review, articles were included only if both reviewers independently determined that all the inclusion criteria were met. Any disagreements were resolved by discussion and mediation by a third reviewer (M.W.), if necessary. Case reports, meeting abstracts/proceedings, review articles, and editorials were excluded. The flowchart of the included studies is shown in Figure 1.
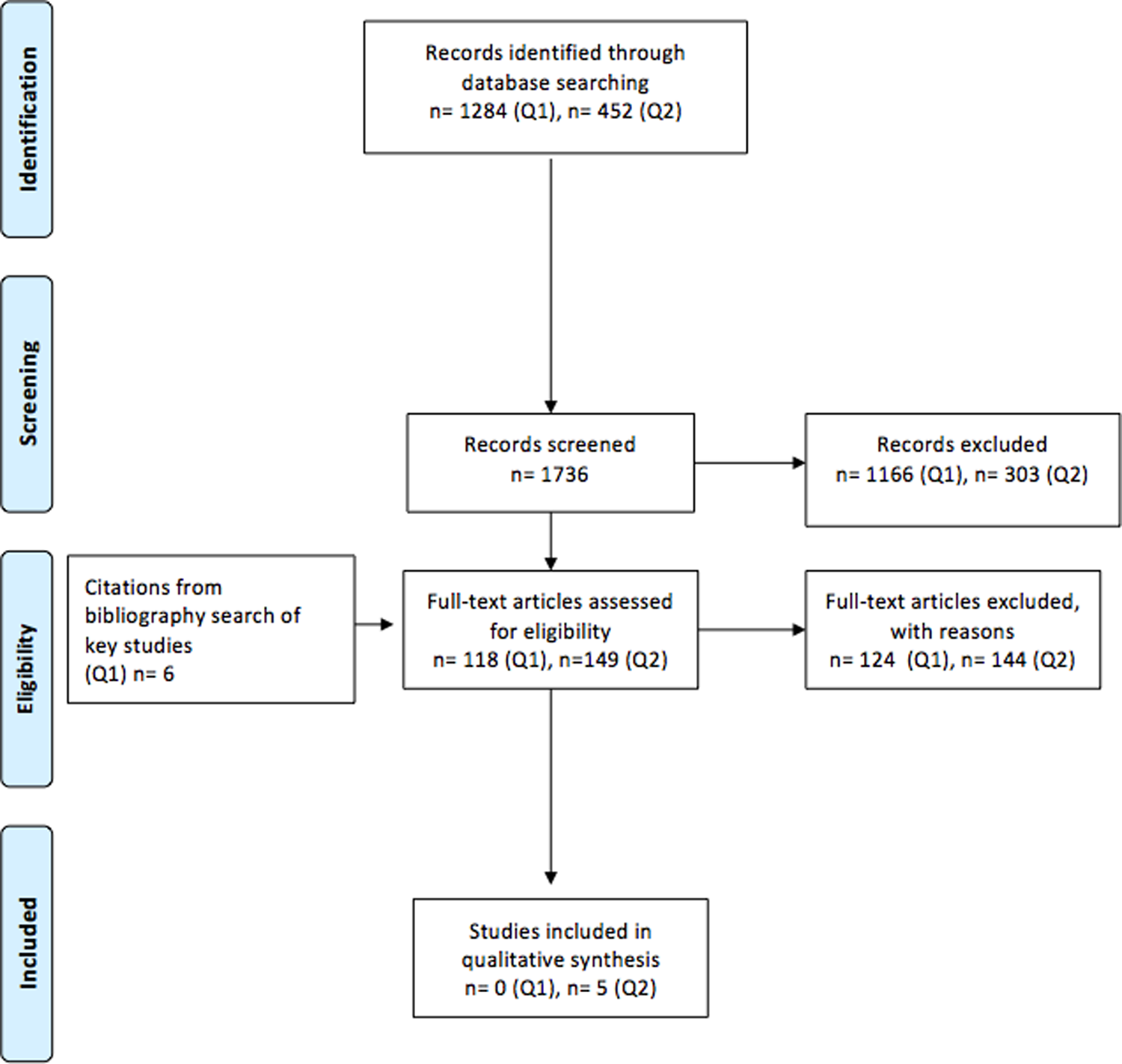
Flowchart showing results of literature search.
Data Extraction and Study Quality Assessment
The following data was extracted from the included articles: study design; patient characteristics, including the diagnosis and treatment administered; follow-up duration and the number of patients who completed the follow-up; preoperative CT myelography and other prognostic factors evaluated; outcome measures; and clinical results as reported by the authors.
A class of evidence ratings was assigned to each article independently by 2 reviewers (F.W. and. F.A.) using criteria from The Journal of Bone & Joint Surgery for prognostic studies. 15 This was modified based on the criteria associated with methodological quality and risk of bias described by Skelly et al. 16 Then the overall body of evidence with respect to each outcome was determined on the basis of precepts outlined by the Grading of Recommendation Assessment, Development and Evaluation Working Group, 17 and recommendations made by the Agency for Healthcare Research and Quality. 18 A qualitative analysis was performed considering the guidelines of the Agency for Healthcare Research and Quality. 19
Risk of Bias in Individual Studies
The initial strength of the overall body of evidence was considered high if the majority of the studies were classified as class I or II, and it was considered low if the majority of the studies were classified as class III or IV. The body of evidence may be downgraded by 1 or 2 levels on the basis of the following criteria: (1) inconsistency of the results, (2) indirectness of the evidence, (3) imprecision of the effect estimates (eg, wide confidence intervals [CIs]), or (4) non–a priori statement of the subgroup analyses. The body of evidence may be upgraded by 1 or 2 levels on the basis of the following criteria: (1) a large magnitude of effect or (2) dose-response gradient.
Data Analysis and Synthesis
Because of the low number of included studies, we were unable to perform a meta-analysis. Therefore, the association between the preoperative CT myelography characteristics and outcome (ie, no association, a negative association, or a positive association) was assessed qualitatively. This study was performed following the PRISMA guidelines and checklist. 20 Clinical recommendations or consensus statements were made by using the Grading of Recommendation Assessment, Development and Evaluation/Agency for Healthcare Research and Quality criteria.
Results
Study Selection
With regard to our study aim to determine the CT myelogram imaging parameters in patients with DCM that correlated with the disease severity, our search strategy yielded 1284 potentially relevant citations. After reviewing the studies’ titles and abstracts, 1166 were excluded. Additional 6 articles from citations from bibliography search of key studies were added and therefore, 124 articles were fully reviewed for inclusion, but none met our inclusion criteria. A list of studies excluded and the reason for exclusion can be found in the online supplementary material.
Regarding our study aim to evaluate the preoperative CT myelogram imaging parameters in patients diagnosed with DCM that could predict the postoperative outcome, the search strategy yielded 452 potentially relevant citations. After reviewing the studies’ titles and abstracts, 303 were excluded. Therefore, 144 articles were considered for inclusion, but only 5 met our inclusion criteria; all of them were retrospective studies (402 patients). 21 -25 Table 2 summarizes the included studies.
Summary of the Study Design, Sample Size, Duration of Follow-up, Type of Clinical Outcome Measures, and Quality of Evidence for the Included Studies.
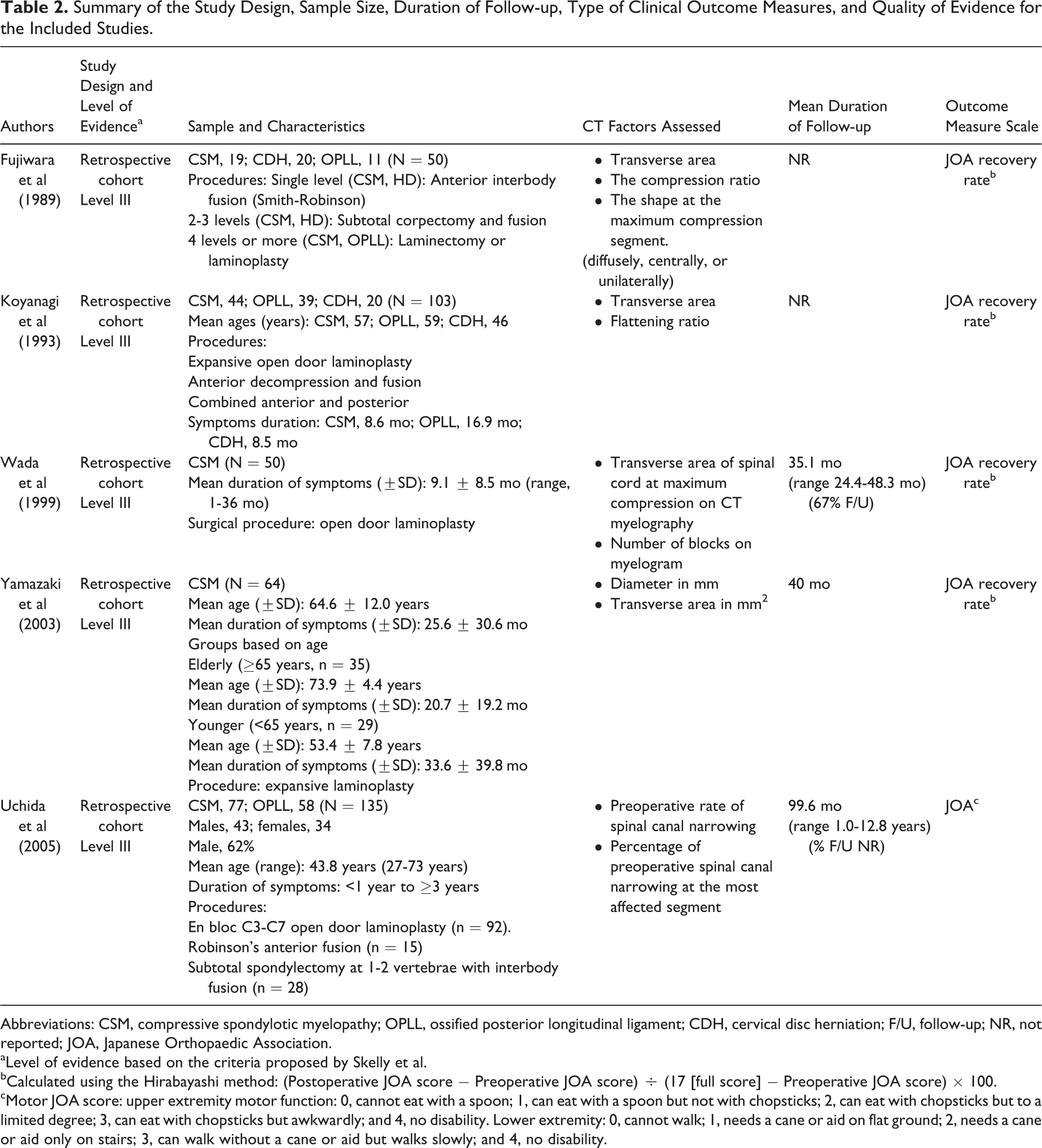
Abbreviations: CSM, compressive spondylotic myelopathy; OPLL, ossified posterior longitudinal ligament; CDH, cervical disc herniation; F/U, follow-up; NR, not reported; JOA, Japanese Orthopaedic Association.
aLevel of evidence based on the criteria proposed by Skelly et al.
bCalculated using the Hirabayashi method: (Postoperative JOA score − Preoperative JOA score) ÷ (17 [full score] − Preoperative JOA score) × 100.
cMotor JOA score: upper extremity motor function: 0, cannot eat with a spoon; 1, can eat with a spoon but not with chopsticks; 2, can eat with chopsticks but to a limited degree; 3, can eat with chopsticks but awkwardly; and 4, no disability. Lower extremity: 0, cannot walk; 1, needs a cane or aid on flat ground; 2, needs a cane or aid only on stairs; 3, can walk without a cane or aid but walks slowly; and 4, no disability.
CT Myelography Characteristics That Correlate With DCM Severity
This systematic review found that no CT myelogram studies have investigated the correlation between imaging characteristics and the severity of DCM.
CT Myelography Characteristics That Can Predict the Postoperative Outcome
Five CT myelogram studies (402 patients) investigated the correlation between different imaging parameters and postoperative outcomes. Overall, 5 different parameters were evaluated: (1) the transverse area of the spinal cord at the level of maximum compression, (2) percentage of preoperative spinal canal narrowing at the most affected segment, (3) number of blocks on CT myelography, (4) spinal canal diameter, and (5) flattening ratio (Table 3).
CT Myelography Parameters as Predictors of Outcome in Operative Patients.
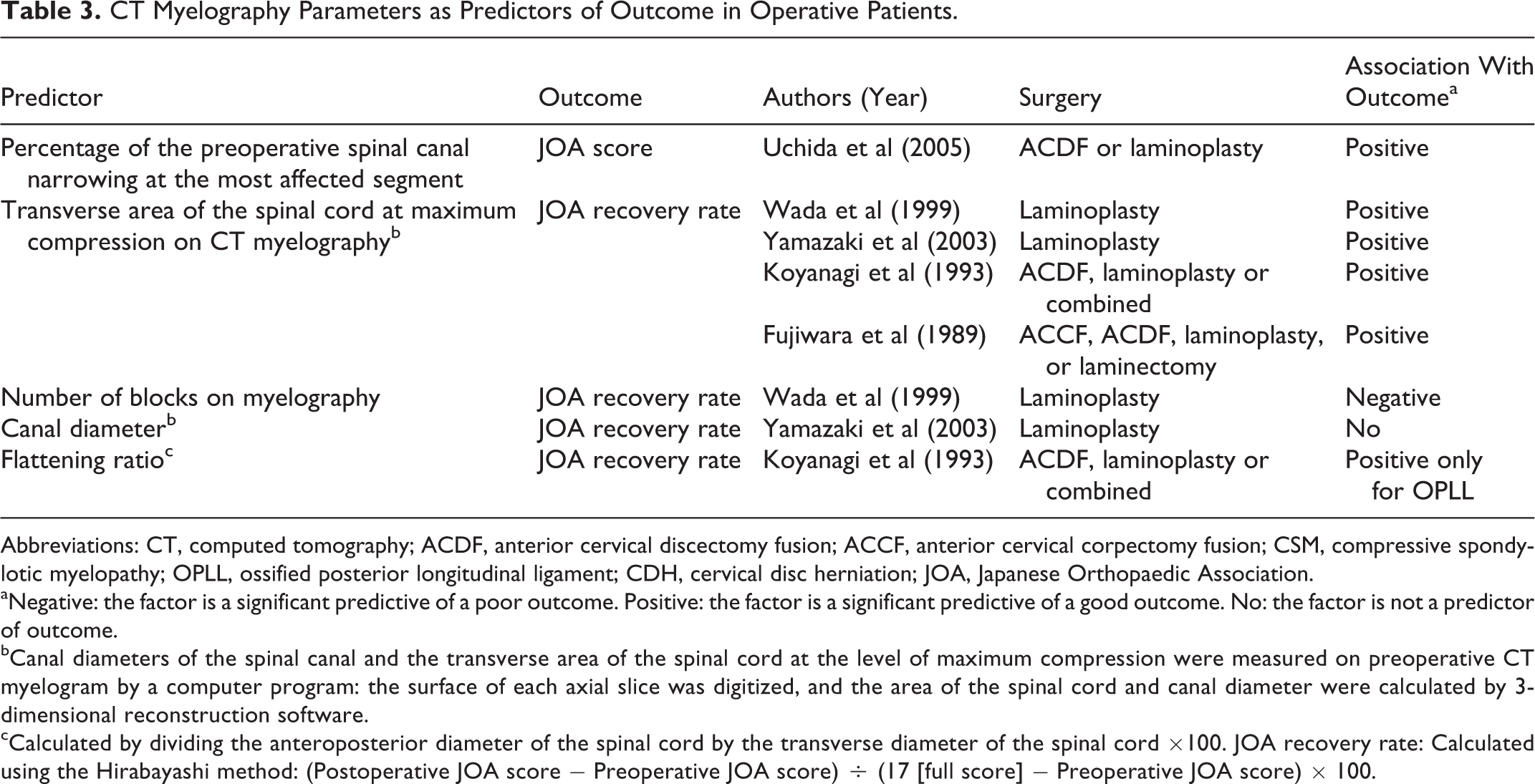
Abbreviations: CT, computed tomography; ACDF, anterior cervical discectomy fusion; ACCF, anterior cervical corpectomy fusion; CSM, compressive spondylotic myelopathy; OPLL, ossified posterior longitudinal ligament; CDH, cervical disc herniation; JOA, Japanese Orthopaedic Association.
aNegative: the factor is a significant predictive of a poor outcome. Positive: the factor is a significant predictive of a good outcome. No: the factor is not a predictor of outcome.
bCanal diameters of the spinal canal and the transverse area of the spinal cord at the level of maximum compression were measured on preoperative CT myelogram by a computer program: the surface of each axial slice was digitized, and the area of the spinal cord and canal diameter were calculated by 3-dimensional reconstruction software. cCalculated by dividing the anteroposterior diameter of the spinal cord by the transverse diameter of the spinal cord ×100. JOA recovery rate: Calculated using the Hirabayashi method: (Postoperative JOA score − Preoperative JOA score) ÷ (17 [full score] − Preoperative JOA score) × 100.
Transverse area of the spinal cord at the level of maximum compression
Four studies examined the association between the transverse area of the spinal cord at the level of maximum compression and postoperative JOA recovery rate. Wada et al 21 investigated a group of 50 patients with cervical spondylotic myelopathy undergoing open door laminoplasty (mean follow-up duration = 35.1 months), and reported a significant correlation between the transverse area at the level of maximum compression and the recovery rate (R = 0.584). Of the 23 patients with a poor surgical outcome (below the mean recovery rate), 18 (78%) had a transverse area <40 mm2. This finding was confirmed by Yamazaki et al 22 in a retrospective study that assessed 64 patients with DCM who underwent canal-expansive cervical laminoplasty. A larger transverse area of the spinal cord (≥30 mm2) at the level of maximum compression was found to be a predictor of excellent recovery rate in both younger (P < .042; odds ratio [OR] = 1.214; 95% CI = 1.007-1.465) and elderly patients (P = .003; OR = 1.264; 95% CI = 0.108-1.47). Moreover, Koyanagi et al 25 followed 103 patients diagnosed with DCM, OPLL, or cervical disc herniation (CDH) who underwent expansive open door laminoplasty, anterior decompression with fusion, or combined anterior and posterior decompression with fusion. They reported a significant relationship between the preoperative transverse area of the spinal cord at the level of maximum compression and the postoperative JOA recovery rate in patients with DCM and OPLL (P < .001). Finally, Fujiwara et al 24 examined 50 patients diagnosed with either DCM, OPLL, or CDH. All patients underwent preoperative CT myelography and were treated surgically with either anterior or posterior cervical surgery (anterior cervical corpectomy and fusion, anterior cervical discectomy and fusion, laminoplasty, or laminectomy). In patients with CDH or OPLL, the most significant predictive factor of an improved outcome was a preoperative transverse area of the spinal cord >30 mm2 on CT myelography at the level of maximum compression (P < .01). A similar trend was also observed in patients with DCM, but this was not significant.
Preoperative spinal canal narrowing at the most affected segment
Only 1 study evaluated spinal canal narrowing at the most affected level as a predictor of postoperative outcomes. Uchida et al 23 evaluated the effect of the preoperative rate of spinal canal narrowing on postoperative JOA scores in a group of 135 patients with degenerative myelopathy who underwent anterior procedure, posterior procedure, or laminoplasty (average follow-up of 8.3 years). Spinal canal narrowing at the most affected segment was measured as a percentage, and a preoperative narrowing rate of >40% was positively correlated with the postoperative neurological outcome (P < .05).
Number of blocks on myelography
The correlation between the number of blocks on myelography and postoperative outcomes was investigated in a single study. Wada et al 21 reported a negative correlation between the number of blocks on CT myelography and the postoperative JOA recovery rate (R = −0.366) in a group of 50 patients with DCM.
Spinal canal diameter
The anteroposterior (AP) spinal canal diameter on CT myelography was only examined by Yamazaki et al. 22 The surface of each axial slice was digitized, and the area of the spinal cord and AP canal diameter were calculated by 3-dimensional reconstruction software. In this group of 64 patients with DCM followed for an average of 40 months, there was no significant relationship between the spinal canal diameter and postoperative recovery rate of the JOA score.
Flattening ratio
The relationship between the flattening ratio and JOA recovery rate on CT myelography was only examined by Koyanagi et al. 25 The flattening ratio was positively correlated with the postoperative JOA recovery rate but only in patients with an OPLL (R = 0.43, P < .001).
Evidence Summary
Based on this systematic review, we found low evidence suggesting that a greater transverse area of the spinal cord at the maximum level of compression on the preoperative CT myelography correlates positively with a better postoperative outcome. There was insufficient evidence to suggest that the percentage of preoperative spinal canal narrowing at the most affected segment, number of blocks on the preoperative CT myelography, canal diameter, or flattening ratio are associated with the postoperative outcome (Table 4).
Evidence Summary for CT Myelography.a
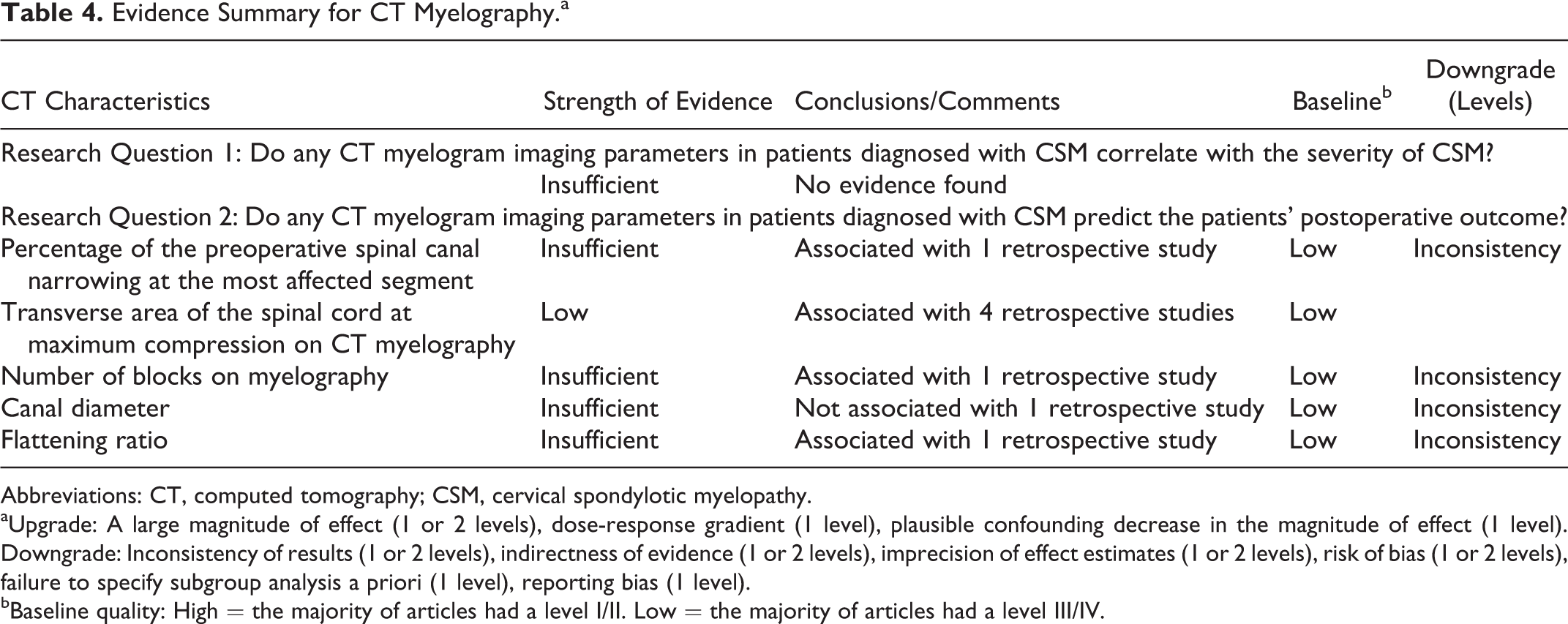
Abbreviations: CT, computed tomography; CSM, cervical spondylotic myelopathy.
aUpgrade: A large magnitude of effect (1 or 2 levels), dose-response gradient (1 level), plausible confounding decrease in the magnitude of effect (1 level). Downgrade: Inconsistency of results (1 or 2 levels), indirectness of evidence (1 or 2 levels), imprecision of effect estimates (1 or 2 levels), risk of bias (1 or 2 levels), failure to specify subgroup analysis a priori (1 level), reporting bias (1 level).
bBaseline quality: High = the majority of articles had a level I/II. Low = the majority of articles had a level III/IV.
Discussion
MRI has become an indispensable modality for diagnosing cervical myelopathy. 26 However, CT myelography remains a valuable alternative diagnostic modality in cases where MRI is contraindicated. 7,8 Moreover, CT myelography is superior to MRI for assessing foraminal stenosis and distinguishing bony lesions from soft tissue lesions. 7
The objective of this systematic review was to investigate whether CT myelography imaging parameters are associated with the severity of DCM and can predict postoperative outcome. Surgical indications for patients with degenerative cervical myelopathy have been controversial. In general, patients with more advanced neurologic deficits are recommended for surgery. Other factors such as age, the duration of symptoms, and preoperative functional status have also been found to independently influence treatment outcome in patients with DCM. 24,27 Surgical treatment for patients with more advanced symptoms, however, is less likely to improve neurologic symptoms, as surgery typically aims to prevent any further neurological damage. The ideal treatment for patients with mild neurologic symptoms is unclear. Fortunately, in most cases, the progression of the disease is generally slower, and close observation is usually recommended in early cases.
To date, most studies have focused different MRI characteristics as possible predictors of surgical outcomes in patients with DCM. 28 The evidence with regard to the clinical value of CT myelogram imaging parameters in patients with cervical myelopathy is conflicting. It remains uncertain whether changes on CT myelogram imaging represent worsening of the disease process and should be considered as a surgical indication, even in less clinically advanced cases of myelopathy. Among the imaging parameters investigated, the transverse area of the spinal cord on CT myelography was indicated by both the AP diameter and width. Therefore, a reduced transverse area of the cord reflects the severity of spinal cord compression and spinal cord atrophy caused by chronic compression. 21,22,25 A cadaveric study 29 on spondylotic myelopathy suggested that morphologic changes of the cord are associated with the level of pathologic severity, which in turn is also related to the potential for functional recuperation. Therefore, it is expected that the transverse area of the spinal cord has a direct correlation with the JOA recovery rate.
Based on this review, patients with a greater transverse area of the spinal cord at the level of maximum compression on CT myelography had better postoperative outcomes; this finding is in accordance with a previous systematic review that investigated the clinical significance of different MRI parameters in patients with DCM. 28 Their results also showed that patients with a greater spinal cord transverse area at the level of maximum compression on MRI had a better prognosis and postoperative outcome. 30 There was insufficient evidence to suggest that the percentage of preoperative spinal canal narrowing at the most affected segment, number of blocks, canal diameter, or flattening ratio on CT myelography were associated with the postoperative outcome. This finding also corroborates with the systematic review by Tetreault et al 28 on MRI characteristics. Tetreault et al 28 also reported that the number of high signal intensity segments on T2-weighted images, combined T1- and T2-weighted signal changes, and the signal intensity ratio were all negative MRI predictors of surgical outcomes in patients with DCM.
Despite the fact that changes on CT myelogram imaging represent worsening of the disease process and this may be considered a surgical indication, there is still no clear consensus regarding the correlation between our findings such as the preoperative transverse area of the spinal cord and the indication for surgery. We believe that this question is an important endpoint of future clinical research to clarify the predictive features associated with both CT and MRI in patients with DCM and for whom surgery is recommended.
A major limitation of this review was the small number of high-quality studies that evaluated CT myelography characteristics as prognostic factors for DCM. In addition, the definition of DCM varied between studies, and 2 studies included patients with DCM, OPLL, and CDH. All included studies were performed in a Japanese population and used the JOA score as a postoperative outcome measure raising the concern of generalizing the results to non-Japanese patients. Finally, no studies reported on the inter-observer reliability with regard to the different CT myelography parameters obtained, which made it difficult to judge the consistency and agreement of these measurements.
Conclusions
The overall strength of evidence regarding the predictive value of most preoperative CT myelogram imaging parameters in patients with DCM is low. However, there is limited evidence to suggest that patients with DCM and a greater preoperative spinal cord transverse area at the maximum level of compression will have a better neurological outcome postoperatively. CT myelography plays a complementary role for diagnosing DCM in patients who cannot undergo MRI, and it may help assist surgeons in deciding the most appropriate treatment strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.