
Abstract
Study design
Retrospective cohort study.
Objectives
To examine differences in postoperative complications, recovery course, and costs between patients with and without obstructive sleep apnea (OSA) undergoing single-level anterior cervical discectomy and fusion (ACDF).
Methods
The National Inpatient Sample (NIS) database was queried to identify patients undergoing single-level ACDF between 2016 and 2022. After exclusions, patients were divided into OSA and control groups. Propensity score matching (1:2) controlled for age, sex, obesity, and year of surgery to balance characteristics. Postoperative outcomes, including complications, length of stay (LOS), hospital costs, and discharge disposition, were compared using chi-square tests for categorical variables and t-tests for continuous variables. A Bonferroni correction was applied, with significance set at P < 0.002.
Results
A total of 36,000 matched cases were analyzed (12,000 OSA and 24,000 controls). OSA patients had significantly higher rates of acute respiratory failure (4.7% vs 1.9%; P < 0.001) and mechanical ventilation (1.5% vs 0.6%; P < 0.001). The OSA cohort also had a longer LOS (2.3 vs 1.9 days; P < 0.001), higher hospital costs ($23,300 vs $21,100; P < 0.001), and greater non-routine discharge rates (20.4% vs 16.8%; P < 0.001).
Conclusions
OSA is associated with increased respiratory complications, prolonged LOS, and higher costs in single-level ACDF. These findings underscore the importance of preoperative screening and tailored perioperative management to improve outcomes in this high-risk population.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is a widely performed and reliable surgical treatment for degenerative cervical disc disease. In the U.S., ACDF outpaces cervical disc arthroplasty by a ratio of 81:1, reinforcing its role as the gold standard for cervical radiculopathy and myelopathy due to its high success rates and durable symptom relief.1,2 With an aging population, the demand for ACDF has risen, bringing an increasing number of patients with significant comorbidities that complicate perioperative management.3,4 While ACDF is considered a safe procedure, its anterior surgical approach carries risks of severe complications, such as airway compromise from laryngeal edema or hematoma, pulmonary embolism, and myocardial infarction. 5 These complications, although rare, highlight the critical need for identifying high-risk patients to improve surgical outcomes and inform decision-making.
Obstructive sleep apnea (OSA), characterized by recurrent upper airway collapse during sleep, is a significant comorbidity in ACDF patients. 6 OSA has a multifaceted relationship with ACDF, serving both as a predictor of perioperative morbidity and as a potential postoperative complication.6,7 In North America, OSA affects 15%-30% of men and 10%-15% of women, with prevalence rising due to increasing obesity rates and an aging population.8,9 Postoperative OSA progression has been attributed to anatomical changes in the pharyngeal space caused by anterior fixation devices and the intraoperative manipulation of cervical structures, which may exacerbate upper airway narrowing. 7 Untreated OSA increases respiratory and cardiovascular risks, complicating perioperative management and highlighting the need for thorough preoperative assessment.
Although ACDF complications have been studied, data on OSA-specific outcomes remain limited. The aim of this study is to use propensity score matching to compare postoperative complications, recovery, and costs between ACDF patients with and without OSA. We hypothesize that OSA patients will have higher complication rates, longer hospital stays, more non-routine discharges, and increased costs.
Methods
Data Collection
The National Inpatient Sample (NIS) database was utilized for analysis and integrated with the corresponding cost-to-charge ratio database for the period from January 1st, 2016 to December 31st, 2022. Sponsored by the Healthcare Cost and Utilization Project (HCUP) under the Agency for Healthcare Research and Quality, the NIS is the largest publicly accessible all-payer inpatient healthcare database in the U.S., designed to generate national and regional estimates of inpatient utilization, access, costs, quality, and outcomes. 10 The database includes a 20% stratified sample of inpatient encounters from U.S. acute-care hospitals, covering over 95% of the U.S. population. 10 Weighted estimates were calculated using HCUP’s discharge weights. Institutional review board (IRB) approval was not necessary, as the dataset is publicly available.
Patient Population
Patients who underwent single-level ACDF were identified using the International Classification of Diseases, 10th Revision (ICD-10) procedural code 0RG10A0. Individuals younger than 18 years were excluded. Cohorts were determined based on the presence of OSA, identified using the ICD-10-CM code G47.33. Additional exclusions included non-elective cases and patients with missing data for variables such as sex, race, income quartile, insurance payer, hospital bed size, teaching hospital status, total costs, and length of stay (LOS). Discharge disposition was categorized as routine (home discharge), non-routine (transfer to a short-term hospital, skilled nursing facility, intermediate care facility, or home with healthcare services), or other (discharged against medical advice, in-hospital death, or unknown destination). Patients with discharge dispositions classified as “other” were excluded from the analysis.
Variable Selection
The independent variables analyzed included age, sex, race, hospital bed size, teaching hospital status, geographic region, total charges, and LOS. Charges were converted to costs using the cost-to-charge ratios from the cost-to-charge ratio database. To account for data spanning multiple years, all cost values were adjusted for inflation to 2022 US dollars using appropriate weighting factors. 11 Patient comorbidities were determined using the Elixhauser comorbidity software, refined for ICD-10-CM through HCUP, which identifies 38 distinct pre-existing conditions based on secondary diagnoses. 12
Primary Outcome Variables
The primary outcomes analyzed included postoperative complications such as acute post-hemorrhagic anemia, wound disruption, dysphagia, mechanical complications, hematoma, nervous system complications, acute deep vein thrombosis, pulmonary embolism, myocardial infarction, cerebrovascular accident, venous thromboembolism, pneumonia, acute kidney injury, anesthesia-related complications, postoperative pain, acute respiratory failure, circulatory complications, mechanical ventilation, urinary tract infection, and overall rate of adverse events. Additional outcomes included LOS, total hospital cost of admission, and discharge disposition.
Statistical Analysis
For this analysis, 1:2 propensity score-matching was performed between cohorts based on age, sex, a diagnosis of obesity, and year of surgery. Statistical analyses were conducted using R statistical software (version 4.4.0; R Project for Statistical Computing, Vienna, Austria). Chi-square and Student’s t-tests were employed to compare differences in categorical and continuous outcomes between cohorts. A Bonferroni correction was used and statistical significance was set at the P < 0.002 level.
Results
Demographics
Baseline Demographic Characteristics of Patients Prior to Propensity Score-Matching.
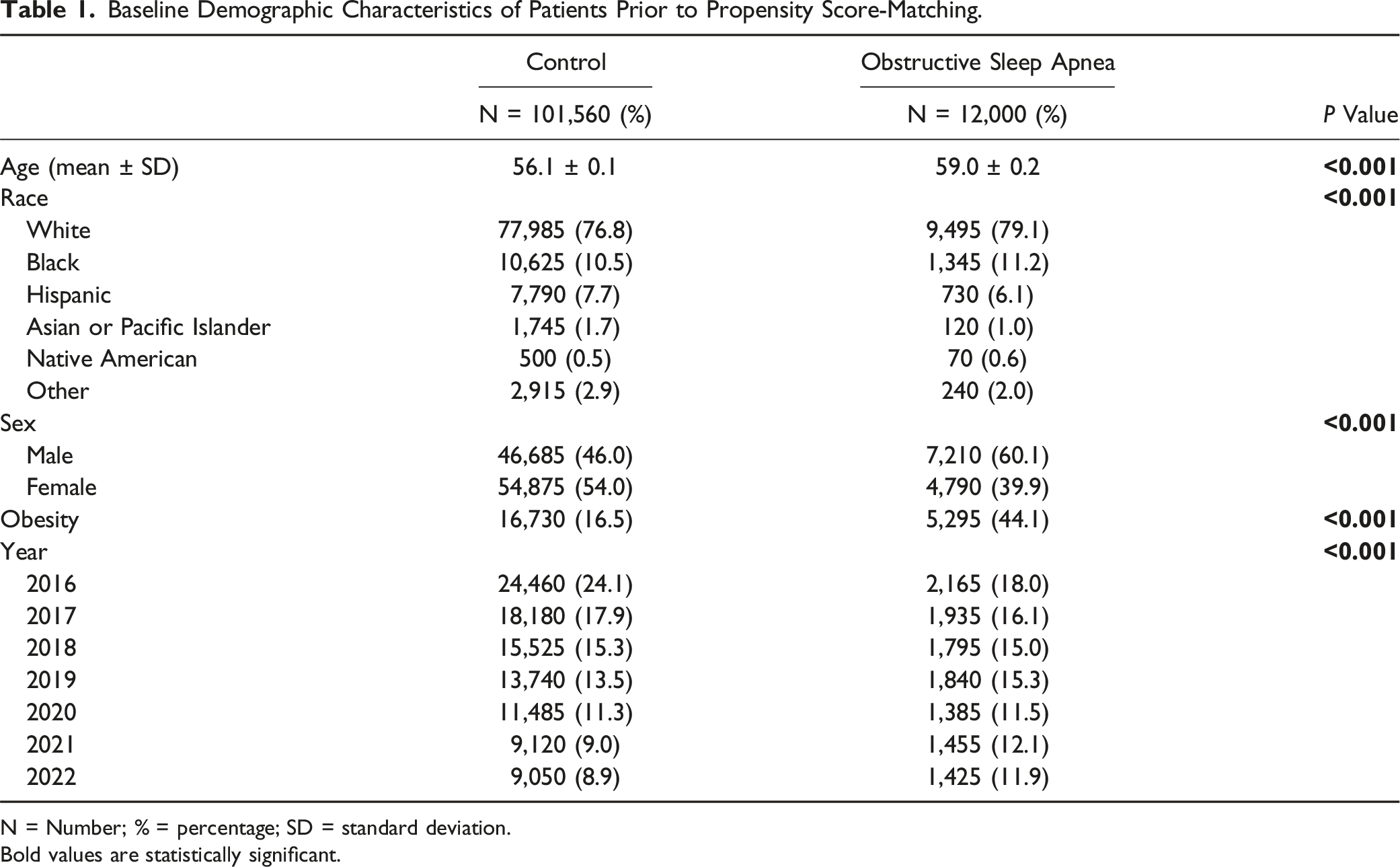
N = Number; % = percentage; SD = standard deviation.
Bold values are statistically significant.
Matched Demographic Characteristics of Patients After Propensity Score-Matching.
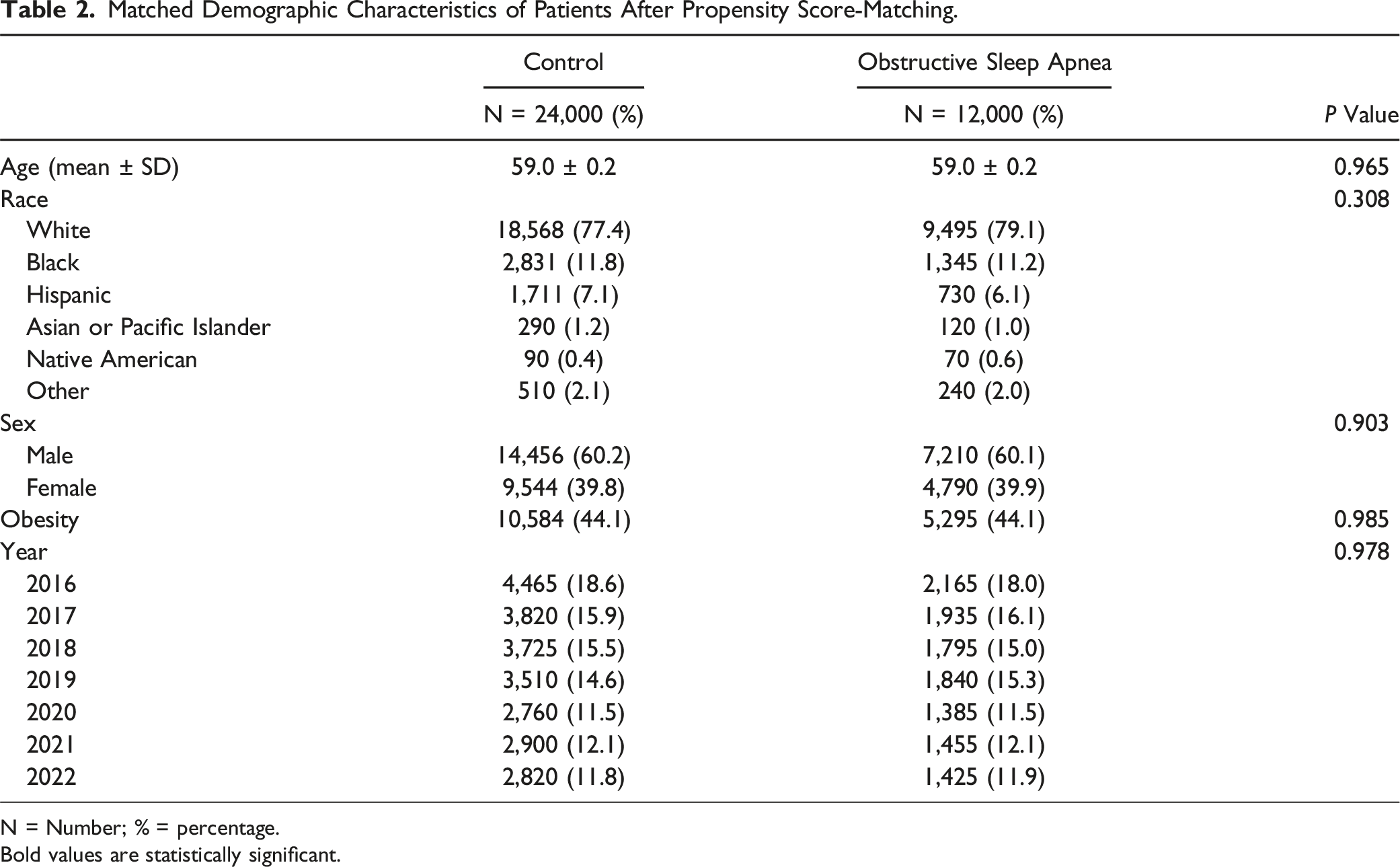
N = Number; % = percentage.
Bold values are statistically significant.
Perioperative Complications
Comparison of Complications Between Cohorts After Propensity Score-Matching.
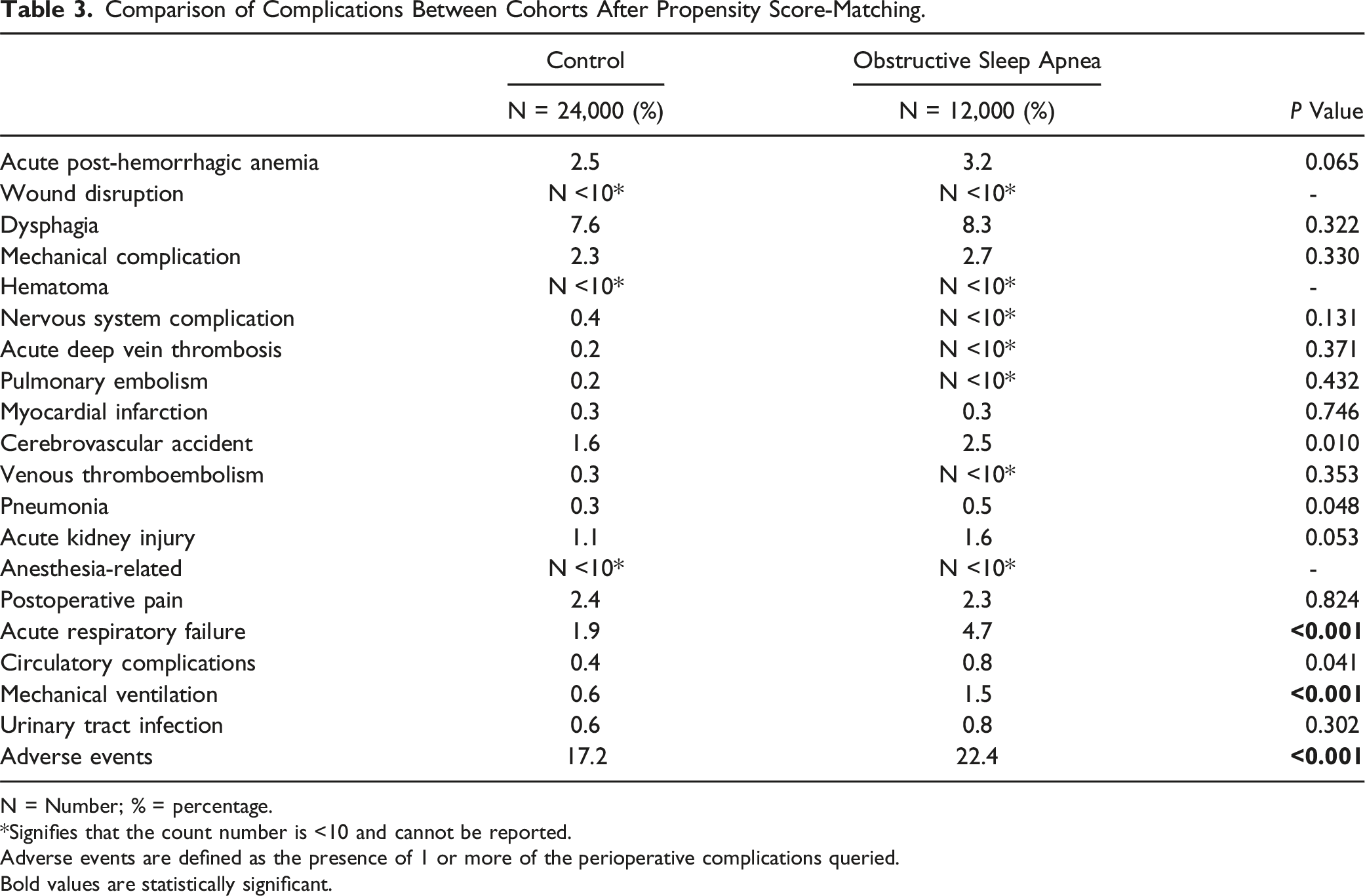
N = Number; % = percentage.
*Signifies that the count number is <10 and cannot be reported.
Adverse events are defined as the presence of 1 or more of the perioperative complications queried.
Bold values are statistically significant.
Hospital Course
The median LOS was 1 day for both OSA and control groups, indicating that the majority of patients in both cohorts experienced short hospitalizations. However, the mean LOS was significantly longer in the OSA cohort compared to controls (2.3 ± 0.1 days vs 1.9 ± 0.04 days; P < 0.001), suggesting that a subset of OSA patients experienced extended hospitalizations that increased the overall average. A positively skewed distribution of LOS was observed in both the OSA and control groups, as demonstrated in Figure 1. Additionally, total hospital costs were significantly higher in the OSA cohort, averaging $23,300 ± 400 compared to $21,100 ± 200 in the control group (P < 0.001). Non-routine discharge also occurred more frequently among OSA patients (20.4% vs 16.8%; P < 0.001; Table 4). Frequency distribution of number of patients by length of stay (days) for obstructive sleep apnea and control groups. OSA = obstructive sleep apnea.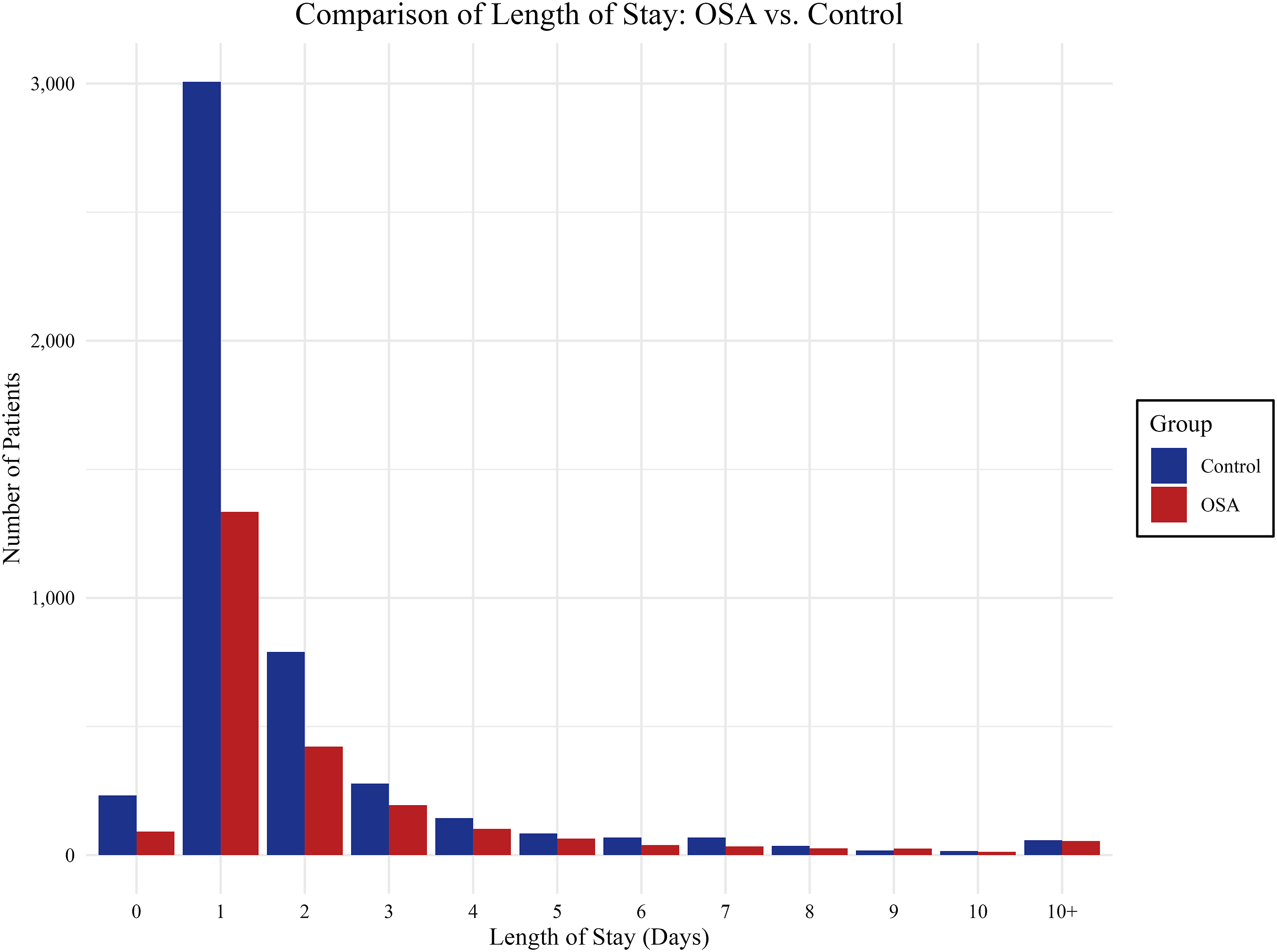
Discussion
Comparison of Hospital Course Between Cohorts After Propensity Score-Matching.
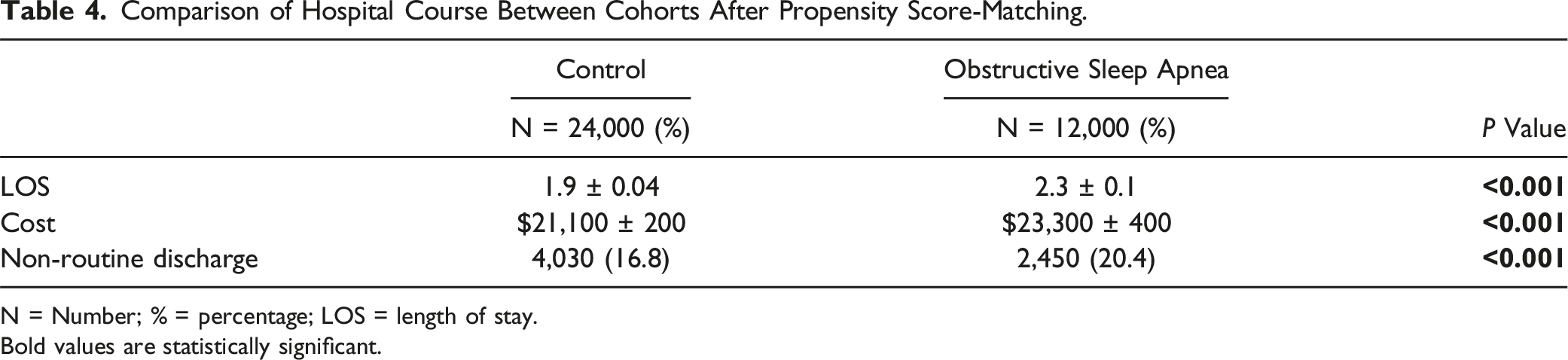
N = Number; % = percentage; LOS = length of stay.
Bold values are statistically significant.
The relationship between OSA and airway complications—particularly acute respiratory failure and the need for mechanical ventilation—was a notable finding in this study. Acute respiratory failure occurred in 4.7% of OSA patients vs 1.9% in non-OSA patients. Likewise, mechanical ventilation was needed in 1.5% of OSA patients compared to 0.6% of non-OSA patients. Prior studies suggest that OSA increases the risk of perioperative airway instability, likely due to upper airway collapsibility, exacerbation of hypoxemia, and heightened sensitivity to anesthetic agents.7,13 Medications used during surgery can further heighten these risks. Sedatives and opioids, known to suppress respiratory drive, may exacerbate airway obstruction in patients with OSA. Beyond pharmacologic influences, anatomical factors also contribute. A reduced craniovertebral angle, indicating less retropharyngeal space, is seen in cervical fusion patients and improving this angle postoperatively has been linked to OSA symptom relief. 14 Postoperative positioning may also play a role. For instance, certain head and neck positions, such as head extension and increased cervical lordosis, have been found to reduce airway collapse and improve OSA symptoms.15,16 Given these risks, close perioperative monitoring is essential. Tailored anesthesia protocols, careful medication management, and strategic positioning can help mitigate complications and optimize patient outcomes. 17
LOS was another critical outcome, with patients in the OSA cohort remaining hospitalized for an average of 0.4 days longer than those without OSA. Prolonged LOS has been similarly reported in other surgical populations with OSA, often attributed to increased postoperative complications such as respiratory issues, delays in mobilization, and the need for closer monitoring during recovery. 13 In our study, the median LOS was 1 day for both groups, though a positively skewed distribution was observed in the OSA cohort, suggesting that extended hospitalizations in a subset of patients contributed to the higher mean LOS. Longer hospital stays not only elevate the risk of hospital-acquired complications, including infections and venous thromboembolism, but also increase the burden on healthcare resources. 18 This underscores the importance of implementing enhanced perioperative care protocols, such as early mobilization, optimized pain management, and vigilant respiratory monitoring, to expedite recovery and reduce LOS in this high-risk group. 19 These strategies could improve outcomes and reduce the strain on healthcare systems posed by prolonged hospitalizations.
Hospital costs were significantly higher in OSA patients, averaging nearly $2,200 more than in non-OSA patients. This increase is likely multifactorial, driven by the greater complexity of care required for OSA patients. Factors contributing to these higher costs include extended LOS, the need for additional perioperative monitoring, and increased interventions to manage complications such as acute respiratory failure and mechanical intubation. The elevated risk of postoperative complications in OSA patients often necessitates specialized care, such as ICU admission and continuous respiratory monitoring, which further inflates costs. Prior studies have consistently highlighted the economic burden of OSA in surgical populations, linking it to higher resource utilization, longer ICU stays, and greater dependency on advanced respiratory support systems. 20 For example, untreated OSA has been associated with prolonged hospital stays and increased readmissions, compounding the financial impact on healthcare systems. 21 Addressing these costs requires a proactive approach that includes preoperative identification of OSA, adherence to CPAP therapy, and tailored anesthetic and postoperative management. Implementing these measures can help mitigate complications, reduce LOS, and ultimately decrease the financial strain posed by OSA patients, benefiting both healthcare providers and payers. Additionally, optimizing perioperative protocols for this high-risk group has the potential to improve cost-efficiency while enhancing patient outcomes.
Given these risks and economic implications, a multidisciplinary perioperative approach is essential for optimizing outcomes in ACDF patients with OSA. Preoperative CPAP therapy should be initiated in diagnosed cases to reduce cardiovascular complications and improve surgical outcomes. 17 Intraoperative management should focus on minimizing sedative agents that exacerbate airway collapsibility, carefully monitoring neuromuscular blockade reversal, and limiting opioid use to prevent respiratory depression.22,23 Postoperatively, continuous pulse oximetry monitoring is crucial during the first 24 hours, as over 80% of respiratory events occur within this period. 24 Early mobilization and proactive respiratory support may further reduce the likelihood of complications. Close collaboration between surgeons, anesthesiologists, and respiratory specialists is key to ensuring safe perioperative care in this high-risk population.
This study has several limitations. The retrospective design introduces potential biases, including unmeasured confounding, which limits causal inference despite the use of propensity score matching to control for key variables such as age, sex, and comorbidity burden. The reliance on the NIS database, while robust and nationally representative, is subject to coding inaccuracies and lacks detailed clinical information, such as the severity of OSA, surgical techniques, and perioperative management strategies. The absence of polysomnographic data further prohibits stratification of OSA severity, an essential factor in understanding its impact on outcomes. Additionally, because the primary rationale for admission is determined by the primary diagnosis code, the database does not capture whether some OSA patients were admitted primarily for postoperative monitoring rather than a medical necessity, potentially leading to an overestimation of length of stay in this population. While the median LOS was consistent between groups, the mean LOS in OSA patients was influenced by a subset with prolonged hospitalizations, resulting in a positively skewed distribution. This highlights the impact of outliers on average LOS and should be considered when interpreting cost and resource utilization. Furthermore, the administrative nature of the NIS database prevents evaluation of long-term outcomes, such as readmissions, symptom recurrence, or quality of life, which are critical for assessing the full scope of ACDF in patients with OSA. The cost data, derived from hospital charges and adjusted using cost-to-charge ratios, may not fully capture actual resource utilization or account for regional variations in healthcare delivery. Moreover, adherence to CPAP therapy among diagnosed patients, a key determinant of perioperative risk, was not captured, limiting the study’s applicability to clinical practice. 22 These limitations necessitate prospective, multicenter studies with detailed clinical data and long-term follow-up to better characterize the relationship between OSA and ACDF outcomes and to develop optimized management strategies for this high-risk population.
Conclusion
OSA significantly impacts perioperative outcomes in single-level ACDF, leading to higher respiratory complications, longer hospital stays, and increased costs. Preoperative screening and optimized management, including CPAP therapy and early mobilization, may improve outcomes. Future studies with long-term follow-up are needed to refine management strategies for this high-risk population.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mitchell K. Ng is a paid consultant at Pacria BioSciences Inc., Sage Products Inc., Alafair Biosciences Inc., Next Science LLC, Bonutti Technologies Inc., Johnson & Johnson Ethicon Inc., Hippocrates Opportunities Fund LLC, and Ferghana Partners Inc. Arya Varthi is a paid consultant for DePuy Synthes Spine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.