
Abstract
Study Design:
Retrospective review of an administrative database.
Objectives:
The aim of our study was to investigate the distribution of spending for the entire episode of care among nonelderly, commercially insured patients undergoing elective, inpatient anterior cervical discectomy and fusion (ACDF) surgeries for degenerative cervical pathology.
Methods:
Using a private insurance claims database, we identified patients who underwent single-level, inpatient ACDF for degenerative spinal disease. Patients were selected using a combination of Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) codes. Entire episode of care was defined as 6-months before (preoperative) to 6 months after (postoperative) the surgical admission.
Results:
In our cohort containing 33 209 patients, perioperative median spending per patient (MSPP) within the year encompassing surgery totaled $37 020 (interquartile range [IQR] $28 363-$49 206), with preoperative, surgical admission, and postoperative spending accounting for 9.8%, 80.7%, and 9.5% of total spending, respectively. Preoperatively, MSPP was $3109 (IQR $1806-$5215), 48% of patients underwent physical therapy, and 31% underwent injections in the 6 months period prior to surgery. Postoperatively, MSPP was $1416 (IQR $398-$3962), and unplanned hospital readmission (6% incidence) accounted for 33% of the overall postoperative spending. Discharge to a nonhome discharge disposition was associated with higher postoperative spending ($14 216) compared with patients discharged home ($1468) and home with home care ($2903), P < .001.
Conclusion:
Understanding the elements and distribution of perioperative spending for the episode of care in patients undergoing ACDF surgery for degenerative conditions is important for health care planning and resource allocation.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is a commonly performed surgical procedure for treatment of symptomatic degenerative disease of the cervical spine. 1 An estimated 1.6 out of every 100 000 individuals undergo surgical decompression for cervical spondylosis. 2 In addition to the cost of the hospitalization and surgical care, preoperative diagnostic workup, conservative treatment, postoperative care and imaging may all contribute to the cost of care. 2 -7 With increased focus on high-value care in the United States, novel payments models such as bundled payments are gaining popularity. 8 -11 Thus, it has become increasingly important to understand the consumption of health care resources and associated costs of care for the care continuum.
Patients who undergo elective ACDF have all undergone varying degrees of diagnostic workup and/or one or more trials of nonoperative treatment. 3 -6 Given the high costs of surgery, it is likely that the majority of spending on patients in the 1-year period surrounding inpatient ACDF is spent on the surgery itself. However, patients inevitably utilize a large degree of health resources in the pre- and postoperative period. In recent years, novel payment models, which include bundling perioperative payments for a given surgical procedure, have been implemented. 7 -9 Although such payment models are widely used by the Centers for Medicare and Medicaid Services (CMS), private payers have yet to fully adopt these new payment strategies. 10
The aim of our study was to investigate the distribution of spending for the entire episode of care among nonelderly patients (ie, patients who are ≤65 years old) undergoing elective, inpatient single-level ACDF surgeries for degenerative cervical pathology. The episode of care was defined as: 6-months preoperatively to 6-months postoperatively.
Methods
Study Design
This study was a retrospective analysis of the Truven Health MarketScan Commerical Claims and Encounters Database. The MarketScan database contains over 500 million paid claims and de-identified medical information for approximately 51 million commercially insured patients across the United States. The database includes information on inpatient, outpatient and pharmacy services for patients that are younger than 65 years. Enrollees are assigned unique identifiers to allow patient data to be linked across the different services. Data is housed in Health Insurance Portability and Accountability Act (HIPAA) compliant manner. This study was exempt from institutional review board approval.
Study Population
The MarketScan database was queried to identify patients who underwent single-level ACDF from January 2011 to December 2015. Our cohort of patients undergoing ACDF for degenerative pathologies were selected using a combination of Current Procedural Terminology (CPT) and International Classification of Diseases–Ninth and Tenth Revisions, Clinical Modification (ICD-9 CM and ICD-10 CM) codes (supplemental appendix, available in the online version of the article). Patients older than 21 years and ≤65 years were included in this study if they underwent single level ACDF and had a diagnosis of cervical disc displacement, spondylosis, stenosis, or degenerative disc disease. Patients were required to have continuous enrollment 6 months preoperatively and 6 months postoperatively. We excluded patients that underwent multilevel ACDF, corpectomy or posterior fusion or had a diagnosis of trauma, spinal cord injury, infection, or cancer. Patients with a hospital admission within 6 months prior to surgery were also excluded (Figure 1).
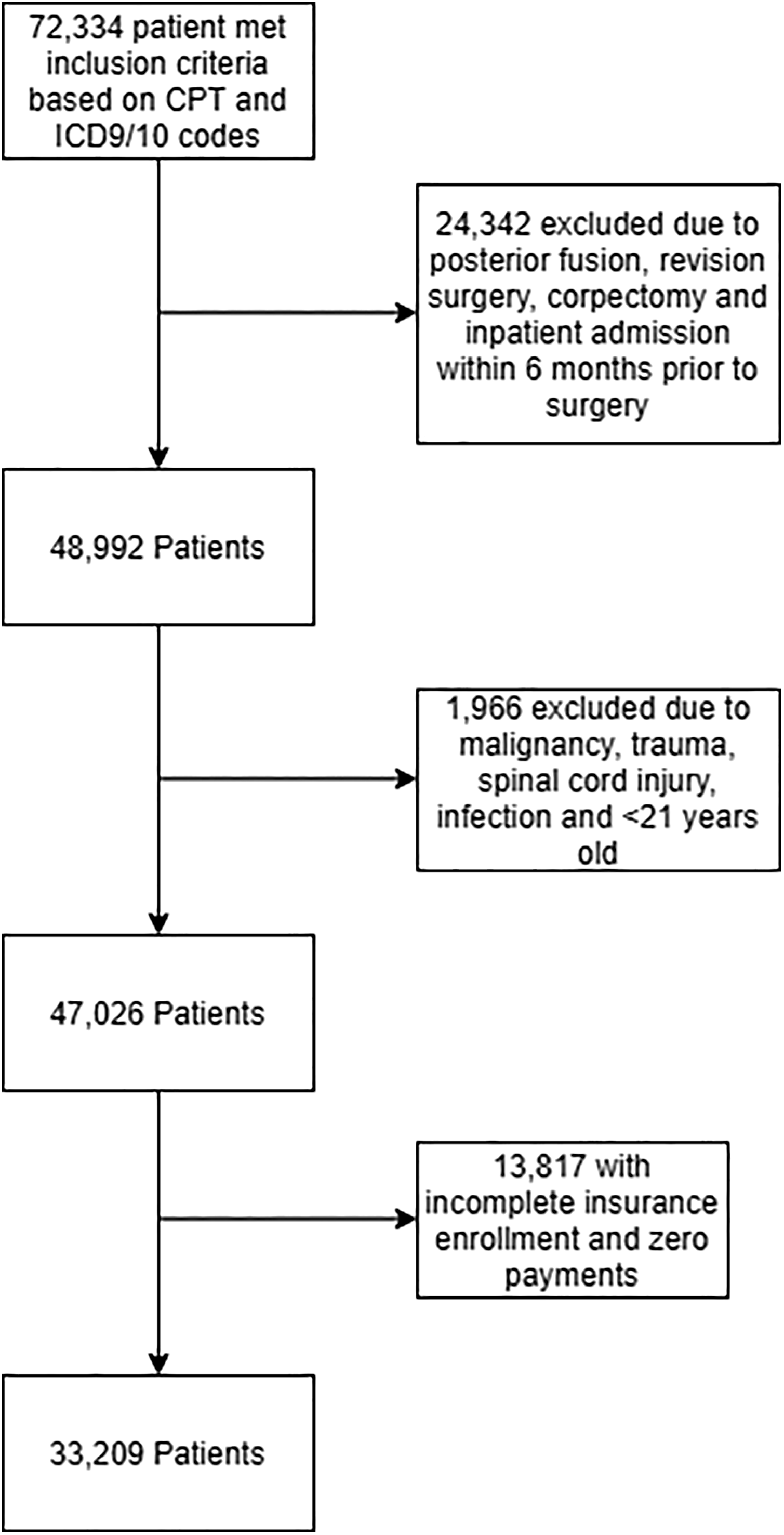
Selection of patients undergoing anterior cervical discectomy and fusion (ACDF) procedure between 2011 and 2015.
Outcomes
Our primary outcome was perioperative median spending per patient (MSPP) associated with single-level ACDF in the year surrounding surgery. ACDF-related spending 6 months prior to and 6 months following surgery was determined. We defined our preoperative time period in accordance with a previous similar study that used this time period per CMS’ bundling norms. 11 The postoperative time period was chosen based on our clinical experience to encompass the full postoperative period and allow us to assess resource utilization (imaging, injections, physical therapy, and narcotics) during the time period. We specifically assessed gross health care perioperative payments on outpatient health services, prescription pain medication, hospital admission (including ACDF surgery) and postoperative all cause hospital readmissions (within 6 months). Outpatient health services assessed included office visits, emergency department (ED) visits, physical therapy, imaging, tests (lab tests and cardiopulmonary testing), medical supplies and durable medical equipment, injections, home health services, and procedures. Major diagnostic categories associated with a body system or disease-related grouping of clinical conditions were used to determine related perioperative services. Payments for claims associated with diseases and disorders of the nervous system, musculoskeletal system and connective tissue were considered to be related to the index procedure. Procedure groups related to CPT, ICD, and Health Common Procedure Coding System (HCPCS) codes were used to identify the outpatient health services described in this study. Our secondary outcome was the difference in postoperative spending among different discharge dispositions. Post hoc comparison of postoperative spending was compared among those discharged home, home with home care and those that had a nonhome discharge disposition (including skilled nursing facility, intermediate nursing facility, rehabilitation facility and other). In order to adjust for inflation, all costs were converted into 2016 US dollar using consumer price index. 12
Statistical Analysis
Continuous variables, including age, length of stay, and payments were summarized as mean ± standard deviation or median (interquartile range [IQR]). Categorical variables were described as frequency counts and percentages, unless otherwise specified. Mann-Whitney U test was utilized to assess the difference in median postoperative spending among those readmitted and those that were not. To determine variation in spending across different discharge dispositions, a Kruskal-Wallis H test was performed. Sensitivity analysis was performed by calculating average amount of US dollars spent on admission and then determining the average decrease in costs that would be associated with every readmission. P value for significance was set at .05. Data was analyzed using SAS version 9.4 (SAS Institute, Inc, Cary, NC, USA) software.
Results
Study Population
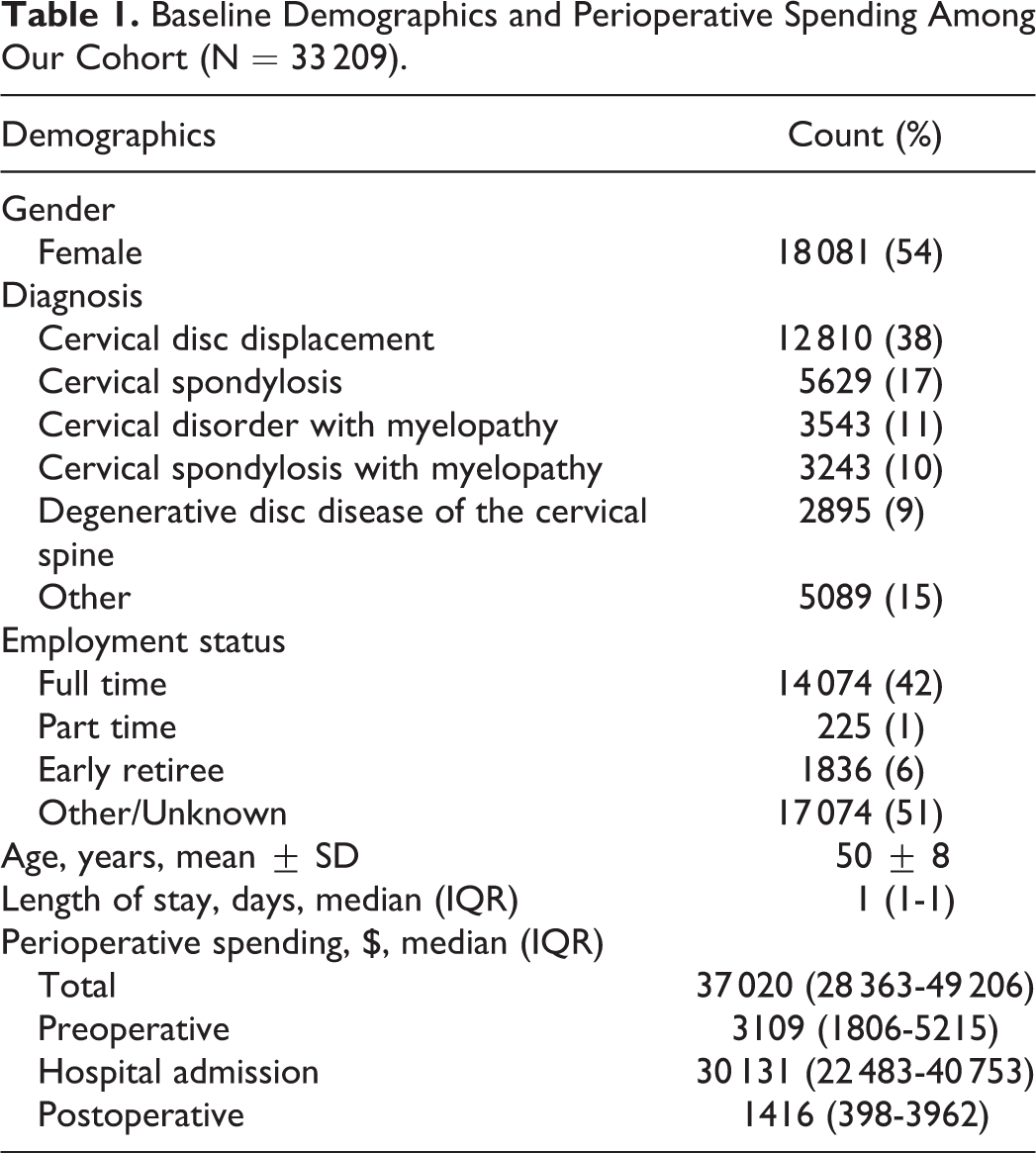
A total of 33 209 patients were included in this study. Of these patients, 18 081(54%) were female and mean age was 50 ± 8 years. Most common diagnoses at time of surgery were cervical disc displacement (38%), cervical spondylosis (17%), and cervical disorder with myelopathy (11%), Table 1.
Baseline Demographics and Perioperative Spending Among Our Cohort (N = 33 209).
Total Spending
Total spending for ACDF surgery during the perioperative period was $1.4 billion ($1 415 821 290). Per patient, median spending in the year encompassing ACDF surgery totaled $37 020 (IQR $28 363-$49 206). Preoperative spending (up to 6 months prior to surgery) accounted for 9.8% ($138 807 085) with a median spending of $3109 (IQR $1806-$5215) per person. Postoperative spending (up to 6 months following surgery) accounted for 9.5% ($134 959 519) of total spending, median spending per person was $1416 (IQR $398-$3962) (Figure 2).
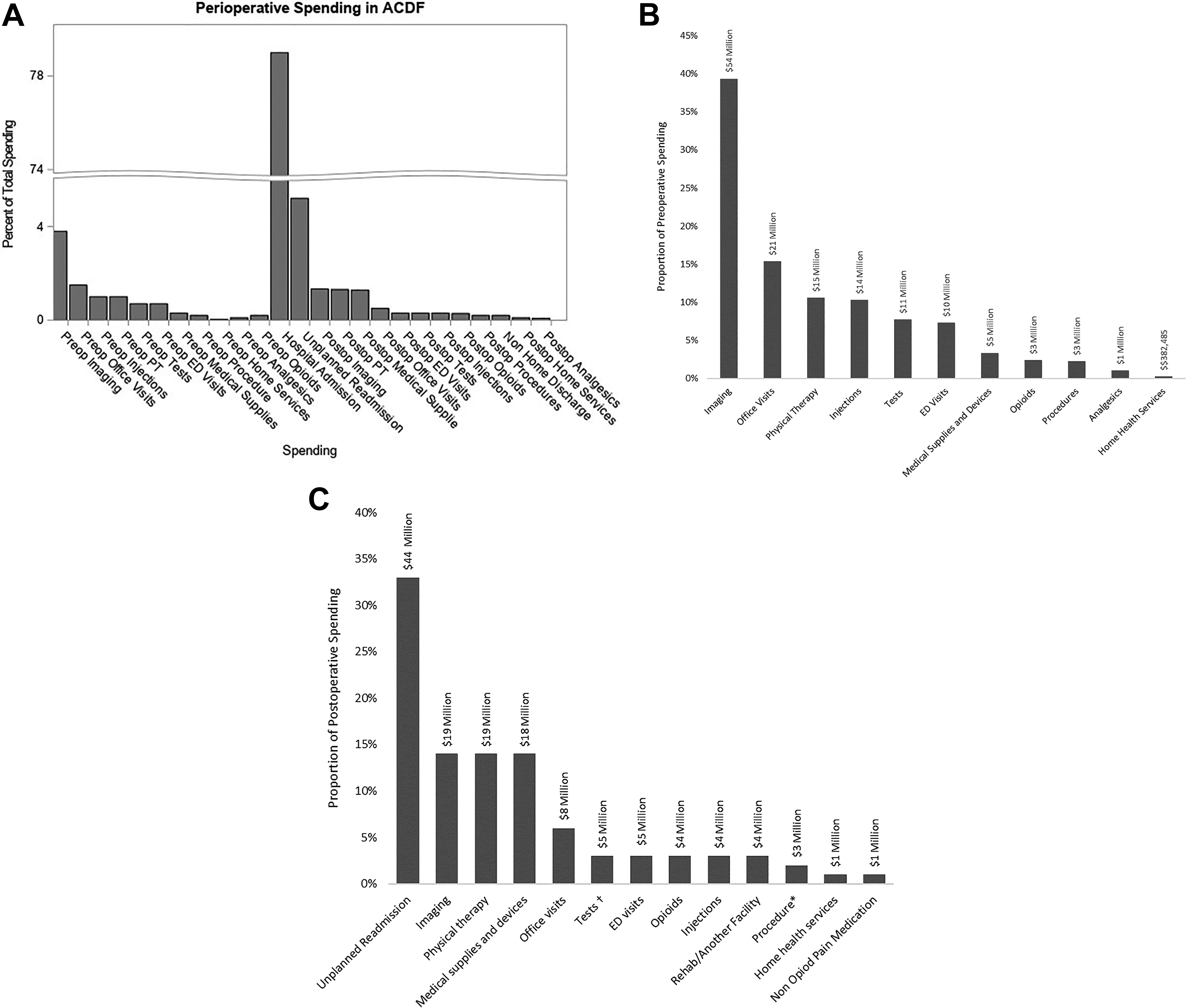
(A) Proportion of spending on outpatient services, prescription pain medications, hospital admission, and readmission for 33 617 patients, 6 months prior and 6 months following surgery. (B) Proportion of spending on outpatient services, prescription pain medications, hospital admission, and readmission for 33 209 patients 6 months prior to surgery. (C). Proportion of spending on outpatient services, prescription pain medications, hospital admission and readmission for 33 209 patients 6 months following surgery.
Preoperative Spending
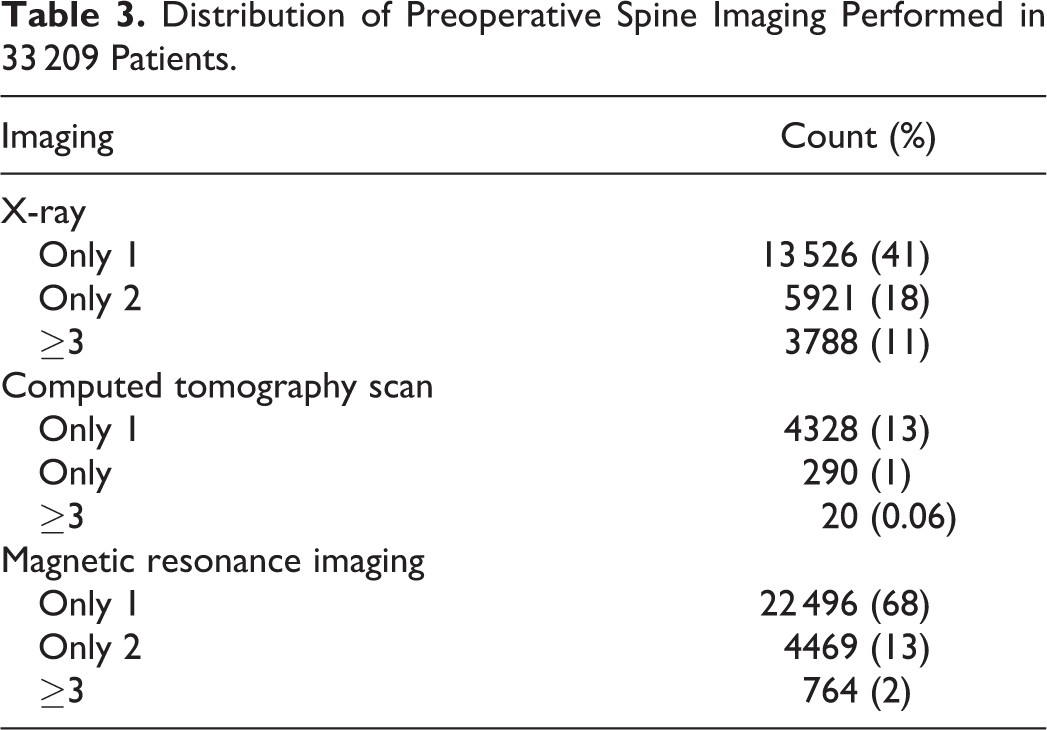
Diagnostic imaging, office visits, and physical therapy were the highest contributors to preoperative spending within 6 months prior to surgery (Table 2). Imaging accounted for 39% of preoperative spending and 3.8% of total spending with a median spending of $1195 (IQR $653-$2146) per patient. Imaging was utilized in 97% of patients. A total of 27 729 (84%) patients underwent magnetic resonance imaging of the spine, and of these, 764 (2%) underwent 3 or more (Table 3). During the preoperative period, physical therapy and injections were utilized by 48% and 31% of patients, respectively. Office visits ($564, IQR $371-$827) and physical therapy ($810, IQR $414-$1610) contributed 15% and 11%, respectively, toward preoperative spending.
Detailed Perioperative Spending on Outpatient, Inpatient, and Pharmacy Services in 33 209 Patients.
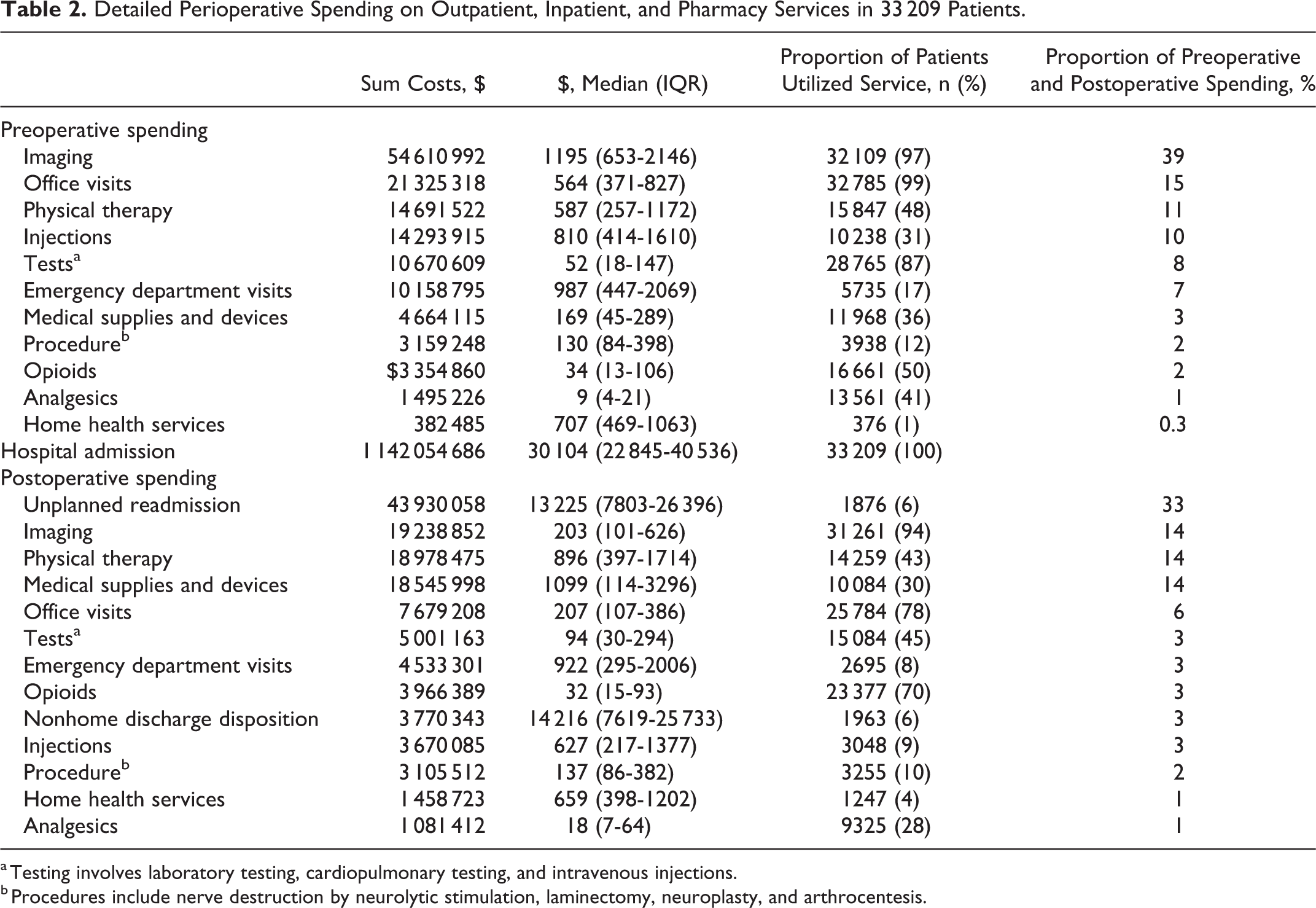
a Testing involves laboratory testing, cardiopulmonary testing, and intravenous injections.
b Procedures include nerve destruction by neurolytic stimulation, laminectomy, neuroplasty, and arthrocentesis.
Distribution of Preoperative Spine Imaging Performed in 33 209 Patients.
Index Surgery
Hospital admission accounted for the highest proportion of total spending, constituting 80.7% ($1 142 054 686) of total costs. Median hospital spending, including ACDF surgery, was $30 104 (IQR $22 845-$40 536) per patient. Median length of stay was 1 day.
Postoperative Spending
Unplanned readmissions contributed the most to postoperative spending, with a median spending of $13 225 (IQR $7 803-26 396) per admission. Imaging (14%) and physical therapy (14%) were the second and third highest contributors to postoperative spending with median spending of $203 (IQR $101-$626) and $896 (IQR $397-$1714), respectively. The most utilized services postoperatively were imaging, office visits, and opioid prescription medication.
Discharge Status
A total of 30 409 (91%) patients were discharged home, 837 (3%) were discharged home with home care services, and 1963 (6%) were discharged to a nonhome discharge disposition (Table 4). Total postoperative spending was significantly higher among those discharged to a nonhome discharge disposition ($14 216) compared with those discharged home ($1468) and home with home care services ($2903), P < .001.
Postoperative Spending Across Different Discharge Dispositions.
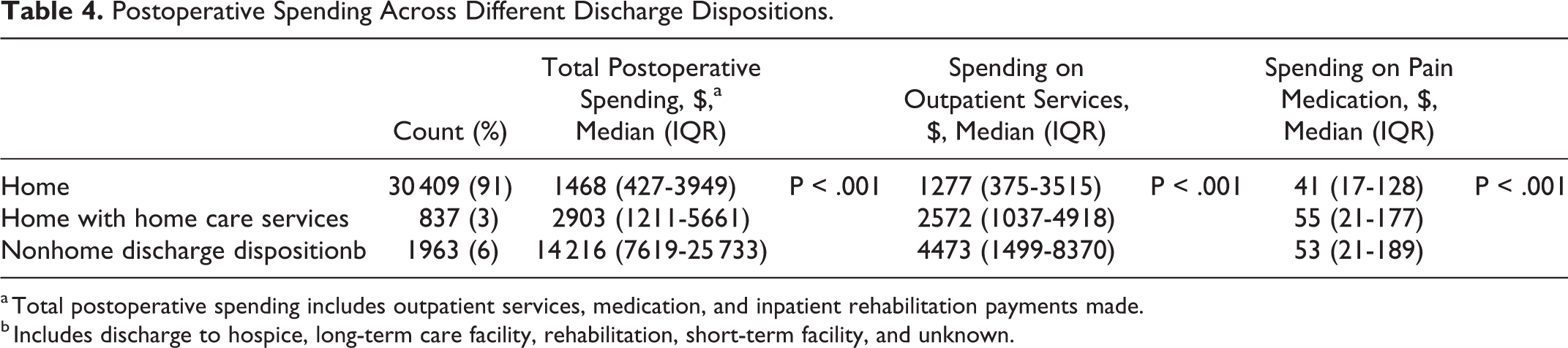
a Total postoperative spending includes outpatient services, medication, and inpatient rehabilitation payments made.
b Includes discharge to hospice, long-term care facility, rehabilitation, short-term facility, and unknown.
Hospital Readmission
The unplanned readmission rate was 6%, resulting in an overall added cost of $43 930 058. Unplanned readmission accounted for the largest proportion of postoperative spending (33%) and the third largest contributor to the total spending, following hospital admission for index surgery and preoperative imaging. The most common reasons for readmission was postoperative infection. There was significant difference in total postoperative spending among those readmitted versus those who were not ($19 935 vs $1339, P < .001).
Sensitivity analysis demonstrated that a 1% reduction (from 6% to 5% incidence) in readmission rate results in a reduction of 5% in postoperative costs and $7.3 million incurred on overall costs. A 2% reduction (from 6% to 4% incidence) resulted in a reduction of 11% in postoperative costs and $15 million incurred on overall costs. A 3% reduction (from 6% to 3% incidence) in unplanned readmission results in 16% reduction in the postoperative cost and 2% reduction in overall costs ($22 million).
Discussion
The aim of our study was to investigate the health care resource utilization and associated spending for the entire episode of care among patients undergoing elective, single-level ACDF surgery for cervical degenerative pathology. Our results demonstrated that of the $1.4 billion (median $37 020 per capita) cumulative expenditure in our population, preoperative spending accounted for 9.8%, and postoperative spending accounted for 9.5% of the perioperative spending. The majority of preoperative spending could be attributed to diagnostic imaging, while the highest proportion of overall postoperative spending was directed toward unplanned readmissions. Interestingly, this means a 1% decrease in readmission rate leads to a reduction of $7 321 676 incurred on total spending. This reduction is more than that spent on postoperative injections, home health services, and analgesics combined.
As anticipated, the majority of spending in the 1-year period surrounding elective ACDF can be attributed to the surgical admission itself, with median payments of $30 104 per patient. As the largest category of spending, reducing the cost of surgery represents the greatest potential for improving the value of ACDF. Efforts to reduce the overall cost of surgery may be aimed at performing surgery in relatively lower cost settings, such as outpatient in appropriately selected patients, decreasing length of stay, or reducing the cost of surgical implants. Outpatient cervical spine surgery has been shown to have a similar risk of morbidity compared with inpatient surgery in appropriately selected patients 13,14 and exhibits lower resource utilization by patients and hospitals. 1,15,16 In a meta-analysis of 7 studies, McClelland et al 14 showed that outpatient ACDF has comparably low complication and readmission rates compared with ACDF. While outpatient ACDF maybe an attractive cost-saving measure for a subset of the population, that is, the young, healthy patient, it may not be an appropriate strategy for treatment of the older patient with comorbidities.
In ACDF surgeries that warrant inpatient admission, minimizing hospital length of stay may serve as an important potential cost reduction measure, as length of stay is known to be a large driver of hospitalization costs. 17,18 There are many known risk factors that may predispose patients to prolonged length of stay following spine surgery, 19 and there is evidence that implementation of accelerated discharge pathways may reduce length of stay. 20 Actively mitigating these risk factors and implementing interventions aimed at reducing length of stay may be potential targets for surgery-related cost reduction. Furthermore, costs associated with instrumentation and choice of interbody implants maybe significant. 21 Thus, supply chain optimization maybe a key focus for cost containment.
We found that diagnostic imaging and office visits accounted for majority of the preoperative costs. This is similar to prior studies, which have shown that diagnostic testing is responsible for the majority of spending in patients with cervical spinal disorders. Fifteen percent of our cohort underwent 2 or more magnetic resonance imaging of the spine within 6 months prior to surgery. Pugely et al 22 conducted a retrospective review of 12 514 privately insured patients with cervical radiculopathy and showed that diagnostic testing accounted for approximately 62% of preoperative costs. In our study, 48% patients underwent physical therapy and 31% underwent injections preoperatively. Given the demonstrated benefit of nonoperative care in potentially obviating the need for surgery in cases of cervical radiculopathy, 23,24 the low utilization of non-operative measures represents another potential area for improvement and cost-containment. However, it is possible that some of these patients may have had cervical myelopathy or cord compression, in which case, nonoperative care would not be the appropriate treatment choice.
Although only 6% of patients had a hospital readmission in the 6-month period following ACDF, the largest portion of overall postoperative spending was related to unplanned inpatient readmissions (33%). Thus, it seems apparent that measures aimed at reducing the rate of readmissions following ACDF would result in substantial reduction in the costs of postoperative care. Common causes of early readmission following spine surgery include pain, wound related complications and medical issues. 25 Thus, strategies aimed at controlling postoperative pain and education on proper wound care may aid in decreasing readmission rates. Postoperative communication strategies, such as patient phone calls 1 week following surgery may also help decrease readmission rates. 26 In addition, 8% of patients had ED visits following surgery, accounting for 3% of overall postoperative spending. Previous studies have demonstrated that postoperative ED visits in this population are typically related to pain and medical concerns. 27 Since many ED visits are avoidable following spine surgery, 28 interventions aimed at decreasing unnecessary ED visits may help reduce the overall cost of postoperative care for patients following ACDF. Apart from readmissions, the 3 largest contributors to postoperative spending were imaging, physical therapy, and medical supplies/devices (13.7% to 14.3%). Unnecessary advanced imaging is commonly performed in patients following ACDF, 29 and minimizing it may help reduce post-operative costs.
Payment reform strategies for surgical procedures are evolving rapidly. 30,31 Although these models of payment should be founded upon the triple-aim of patient satisfaction, high-quality care, and decreased cost, 32 bundled payment models may have shortcomings if the contributors to perioperative costs are not considered carefully. Furthermore, unplanned readmissions and postoperative ED visits incur significant costs according to our results. In the development of bundled payment models, it is important that such “adverse” events are accurately accounted for.
Although our results report novel and valuable information to surgeons, payers, and policy makers, they should be interpreted with several limitations in mind. Regional and intercenter variations exist when considering charges for surgical procedures, cost of implants, and healthcare quality. 33 -36 Therefore, these generalized findings may not be applicable to all hospitals or health care networks, but serve as a broad summary of the contribution of various health services to overall perioperative payments for ACDF. In addition, the working-age patients younger than 65 years we have targeted in our study may exhibit a substantially different perioperative spending pattern than retired patients who are aged 65 years or older. 37 We hypothesize that the rate of postoperative rehabilitation or home-health needs would be substantially greater in the older population, which may alter the spending distribution toward additional spending in the postoperative phase. Our study focused on health insurance in the United States in which direct spending cannot be extrapolated to other countries. Nonetheless the perioperative proportions of both spending and resource utilization can be of benefit to the non-US surgeon. Last, the use of administrative claims data and inability to perform manual chart review prevents us from being able to definitively link all healthcare services to the diagnosis for which surgery is being performed; however, we addressed this concern by limiting our analysis to health services that were related to musculoskeletal, nervous system, and connective diagnoses. Despite these limitations, however, we have defined a detailed breakdown of the perioperative payments surrounding ACDF that is among the most comprehensive studies on this topic in the published literature.
Conclusion
Understanding the elements and distribution of perioperative spending for the episode of care is important for health care planning and resource allocation. Furthermore, it is an essential step toward identifying targets for reducing wasteful spending. These results may be of use for decision making by surgeons, health care administrators, and policy makers.
Supplemental Material
Supplemental Material, Appendix - Health Care Resource Utilization in Commercially Insured Patients Undergoing Anterior Cervical Discectomy and Fusion for Degenerative Cervical Pathology
Supplemental Material, Appendix for Health Care Resource Utilization in Commercially Insured Patients Undergoing Anterior Cervical Discectomy and Fusion for Degenerative Cervical Pathology by Majd Marrache, Andrew B. Harris, Varun Puvanesarajah, Micheal Raad, Hamid Hassanzadeh, Lee H. Riley, Richard L. Skolasky, Mark Bicket and Amit Jain in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.