
Abstract
Study Design
Retrospective cohort study.
Objective
Despite increasing cannabis use, its prevalence in specific surgical groups is unclear, and its impact on perioperative care and outcomes is understudied. This study estimates cannabis use incidence in patients undergoing lumbar spine surgery and explores associations between preoperative use and anxiety, pain scores, and postoperative opioid consumption. We hypothesized a correlation between cannabis use and decreased reliance on opioids for postoperative pain relief.
Methods
This single-center retrospective cohort study included 204 patients undergoing single or multilevel spinal fusion surgery between July 2022 and August 2023. Self-reported cannabis use, demographics, surgical characteristics, numeric rating scale (NRS) pain scores, anxiety, inpatient opioid consumption, and discharge prescribing (total morphine equivalent dose) were extracted from electronic medical records (EMR). Patients were categorized into cannabis users or non-cannabis users, and group differences were analyzed using bivariable and multivariable regression.
Results
Of 204 patients, 27 (13.2%) were cannabis users and 177 (86.8%) were non-users. Cannabis users were younger (P = 0.007), more likely male (P = 0.028), and Caucasian (P = 0.032) than non-users. Preoperative cannabis use correlated significantly with anxiety disorder (P = 0.023) and higher preoperative (P = 0.016) and postoperative (P = 0.002) NRS pain scores. Multivariable analysis showed cannabis use associated with higher preoperative (P = 0.015) but not postoperative (P = 0.073) pain scores. No significant differences were found in preoperative, discharge opioid prescribing or postoperative opioid consumption.
Conclusion
The incidence of cannabis use was low, but positively associated with anxiety and higher preoperative NRS pain scores. Large, well-powered trials are needed to understand cannabis’s impact on spine surgery outcomes.
Introduction
The widespread use of cannabis is evident on a global scale: The 2021 United Nations World Drug Report estimates approximately 219 million users, constituting 4.3% of the global adult population. 1 In the United States, cannabis ranks as the third most used recreational substance, with 15% of the population overall and 22% of individuals aged 12 or older reporting cannabis use in the past year. 2 In parallel, as of April 2023, medical cannabis programs operate in 38 states and 4 territories, with 24 states allowing non-medical use. 3 These trends suggest the need to explore the incidence of cannabis use among select surgical populations, to evaluate the impact of use on outcomes after surgery, and to consider whether there are differential effects of cannabis on outcomes after painful procedures, including spine surgery. Each of these topics are currently undefined and understudied.
Despite advances in multimodal analgesic strategies for spine surgery, opioids remain the cornerstone of pain management regimens.4,5 The ongoing opioid epidemic has prompted a search for alternative pain management strategies, and recent studies suggest a potential synergistic effect between cannabis and reduced opioid use, with preclinical data demonstrating opioid-sparing effects of cannabis. 6 These forces, combined with trends in population use highlight the need to understand how baseline cannabis use influences postoperative outcomes after spine surgery.
The primary objective of this study is to estimate the incidence of cannabis use among patients presenting for lumbar spine surgery. We additionally aimed to assess the impact of patient-reported preoperative cannabis use on pain scores and opioid consumption for postoperative analgesia. We hypothesized the incidence of cannabis use would mirror population use, and that cannabis use would correlate with lower pain scores and decreased opioid prescribing after lumbar spinal fusion.
Methods
Study Design and Patients
This is a single-center observational, retrospective cohort study. The study was performed after approval from the Institutional Review Board at Hospital for Special Surgery (HSS-IRB #2021-2137). Written patient consent was waived by the IRB due to the anonymous, retrospective nature of the data collection.
The study population comprised consecutive patients undergoing single or multilevel spinal fusion surgery at our institution between July 2022 and August 2023. All patients with documented cannabis use or non- use in the electronic medical record (EMR) were eligible for inclusion in the analysis. Surgical procedures included posterior lumbar interbody fusion (PLIF), extreme lateral interbody fusion (XLIF), anterior lumbar interbody fusion (ALIF), and circumferential fusion (A/PLIF). Exclusion criteria included emergency surgery and surgery for trauma, infection, or neoplasm.
Demographic information, surgical characteristics, and outcomes were extracted through manual EMR chart review. Data extracted included: patient age, gender, race, American Society of Anesthesiologists classification (ASA), body mass index (BMI), history of depression, history of anxiety, chronic pain (diagnosis and/or opioid prescriptions for >3 months before the date of surgery), systemic respiratory or cardiac comorbidity, preoperative numeric rating scale (NRS) pain scores (0-10 where 0 = no pain and 10 = worst imaginable pain), preoperative opioid prescribing (yes/no), antidepressant, benzodiazepine, NSAIDs, and pregabalin/gabapentin use, smoking status, alcohol consumption, and cannabis use.
Hospitalization data included inpatient benzodiazepine administration, opioid consumption during the admission, postoperative NRS pain scores, postoperative nausea and vomiting (PONV), length of stay (LOS) and discharge opioid prescribing. Operative and anesthetic variables included number of operative levels, operative time (from incision to closure), duration of anesthesia (from induction to emergence), and time to emergence from anesthesia (defined as the time between closure of the surgical incision to extubation).
Patients were categorized into cannabis users and non-cannabis users based on self-reported preoperative use. All patients are asked about cannabis use as part of the social history at the pre-surgical screening appointment, by the hospitalist and/or by the surgeon’s office and/or as part of the anesthetic pre-evaluation. Manual review of the EMR was conducted to assess recreational and/or medical cannabis use up to and including the latest preoperative appointment(s) or at the anesthetic evaluation on the day of surgery. Details such as strain, potency, method of intake, or duration of use are not reliably available in the EMR; hence, only “yes/no” documented cannabis use was recorded. Opioid consumption was calculated as the total morphine equivalent dose (MED) of all opioid medications administered during inpatient hospitalization (including oral and intravenous (IV) patient-controlled analgesia (PCA) use). Post-discharge opioid prescribing was calculated as the total MED of opioids prescribed at discharge.
All patients received perioperative comprehensive multimodal analgesia (MMA), including a regional anesthetic technique, according to surgical approach (transversus abdominis plane block for anterior or lateral approach; erector spinae plane blocks for posterior),7,8 ketorolac (15 mg every 8 h up to 3 doses), acetaminophen (1000 mg every 8 h) and opioids on an as-needed basis (tramadol 50 mg every 4 h, or oxycodone, 5-10 mg every 4 h, according to pain scores) and PONV prophylaxis (intraoperative dexamethasone, 4-8 mg and ondansetron 4 mg). 4
Statistical Analysis
The normality of continuous variables was assessed using the Shapiro-Wilk test. Median and Interquartile range (IQR) were utilized to summarize non-normally distributed continuous variables, while count and percentage were calculated for discrete variables. The Kruskal-Wallis test examined differences in continuous variables between 2 groups, and Fisher’s exact test or Chi-square test was applied for categorical variables based on cell sizes. Multivariable linear regression, adjusting for age, sex, BMI, anxiety, levels fused, and procedure, was employed to evaluate the association between cannabis use and preoperative pain score. Similarly, multivariable linear regression adjusting for preoperative pain score, age, sex, BMI, anxiety, levels fused, and procedure, was used to assess the relationship between cannabis use and postoperative pain score. Statistical significance was defined as P < 0.05, and R-Studio version 2023.06.0 was used for statistical analysis. 9
Results
Incidence of Cannabis Use
Patient Demographics.
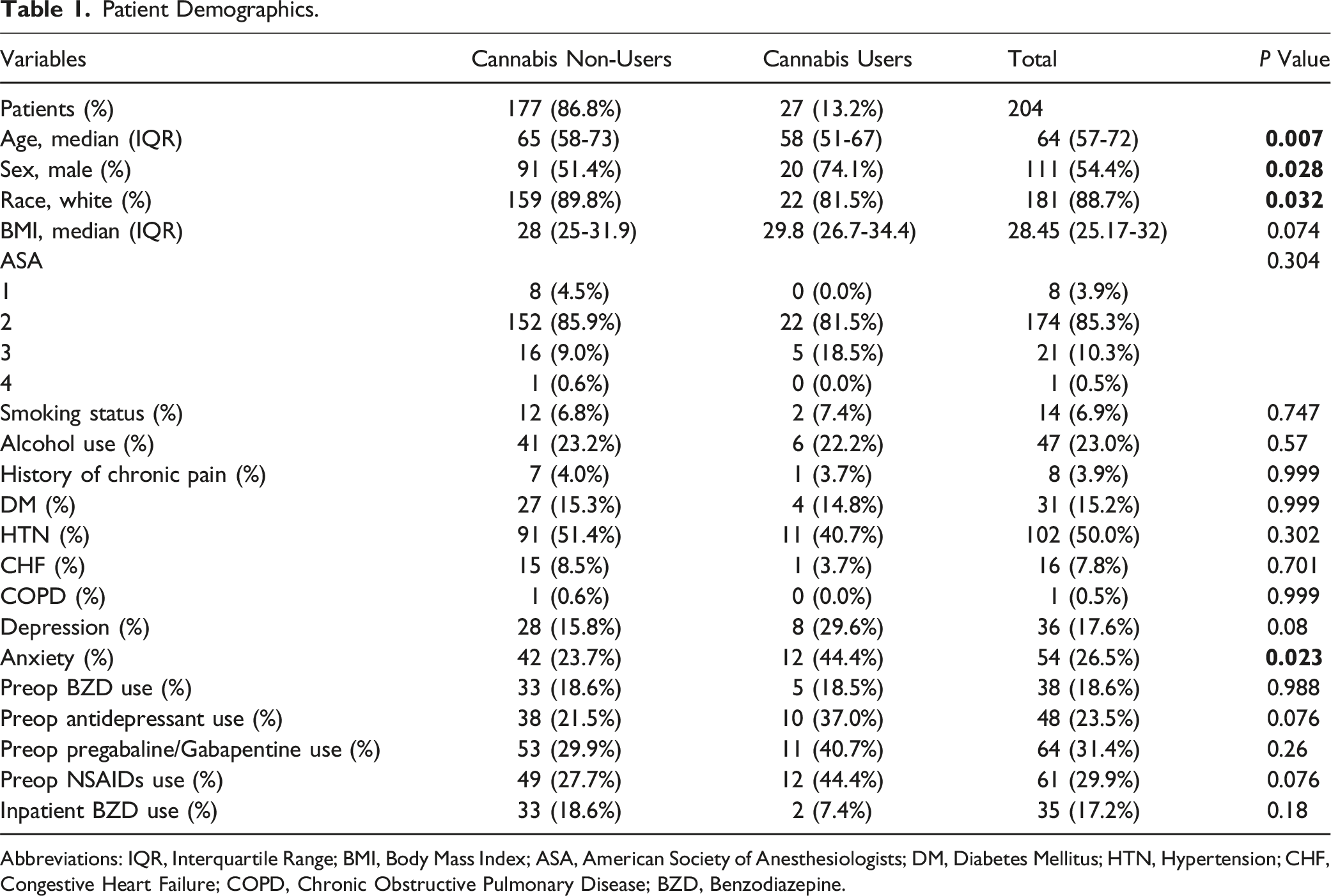
Abbreviations: IQR, Interquartile Range; BMI, Body Mass Index; ASA, American Society of Anesthesiologists; DM, Diabetes Mellitus; HTN, Hypertension; CHF, Congestive Heart Failure; COPD, Chronic Obstructive Pulmonary Disease; BZD, Benzodiazepine.
Patient Demographics
Significant associations were found in baseline demographics, with cannabis users being younger (median 58, IQR 51-67 vs median 65, IQR 58-73 years, P = .007), predominantly male (74.1% vs 51.4%, P = .028), and of Caucasian race (81.5% vs 89.8%, P = .032). On bivariable comparisons, there was a significant association between cannabis use and the prevalence of anxiety (44.4% vs 23.7%, P = .023), but not between cannabis use and anxiolytic medication use (18.6% of non-users vs 18.5% of users, P = 0.988). There were no significant associations between cannabis use and the prevalence of depression (29.6% of cannabis users vs 15.8% of non-cannabis users, P = .08), or antidepressant and cannabis use (37% of cannabis users vs 21.5% of non-users, P = .076). No statistically significant differences were found in BMI (29.8, 26.7-34.4 vs 28, 25-31.9, P = .074), ASA class (P = .304), smoking status (current smokers: 7.4% vs 6.8%, P = .747), alcohol consumption (22.2% vs 23.2%, P = .57), history of chronic pain (3.7% vs 4%, P = .999), diabetes mellitus (14.8% vs 15.3%, P = .999), hypertension (40.7% vs 51.4%, P = .302), congestive heart failure (CHF) (3.7% vs 8.5%, P = .701), and chronic obstructive pulmonary disease (COPD) (0% vs 0.6%, P = .999). Also, while not reaching statistical significance, a greater number of cannabis users took NSAIDs (44.4% vs 27.7%, P = .076) and pregabalin/gabapentin (40.7% vs 29.9%, P = .26) (Table 1).
Surgical Characteristics
Surgical Characteristics.
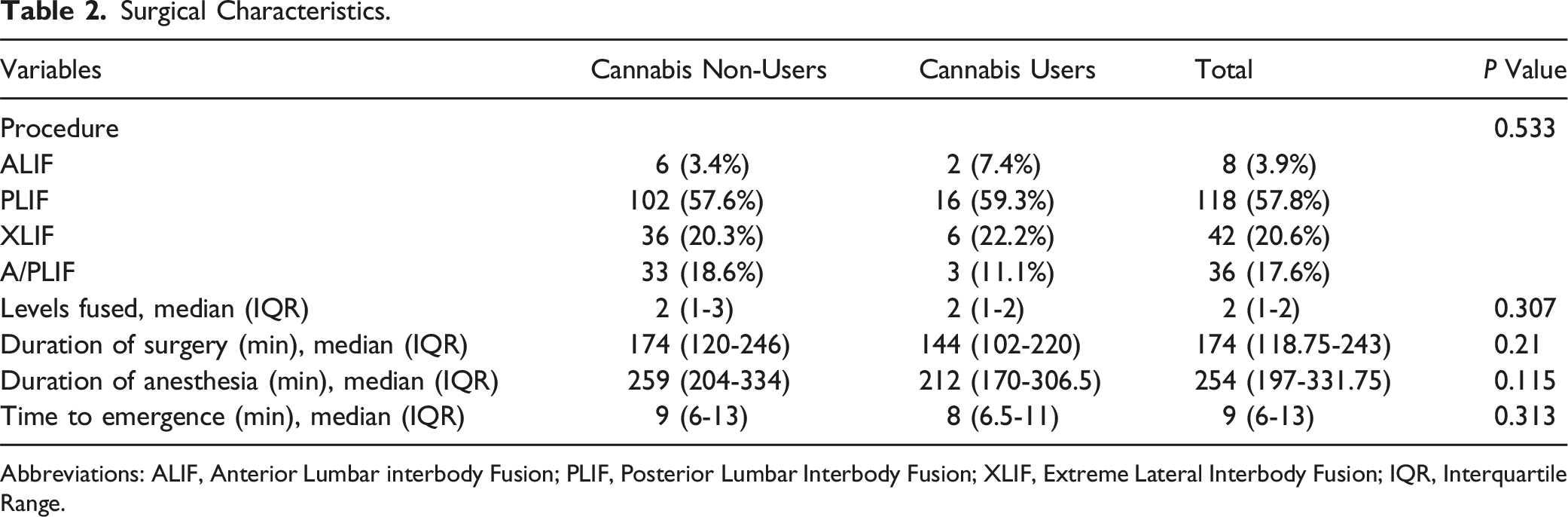
Abbreviations: ALIF, Anterior Lumbar interbody Fusion; PLIF, Posterior Lumbar Interbody Fusion; XLIF, Extreme Lateral Interbody Fusion; IQR, Interquartile Range.
Pain Scores, Opioid Consumption, and Postoperative Outcomes
Pain Scores, Opioid Consumption and Outcomes.
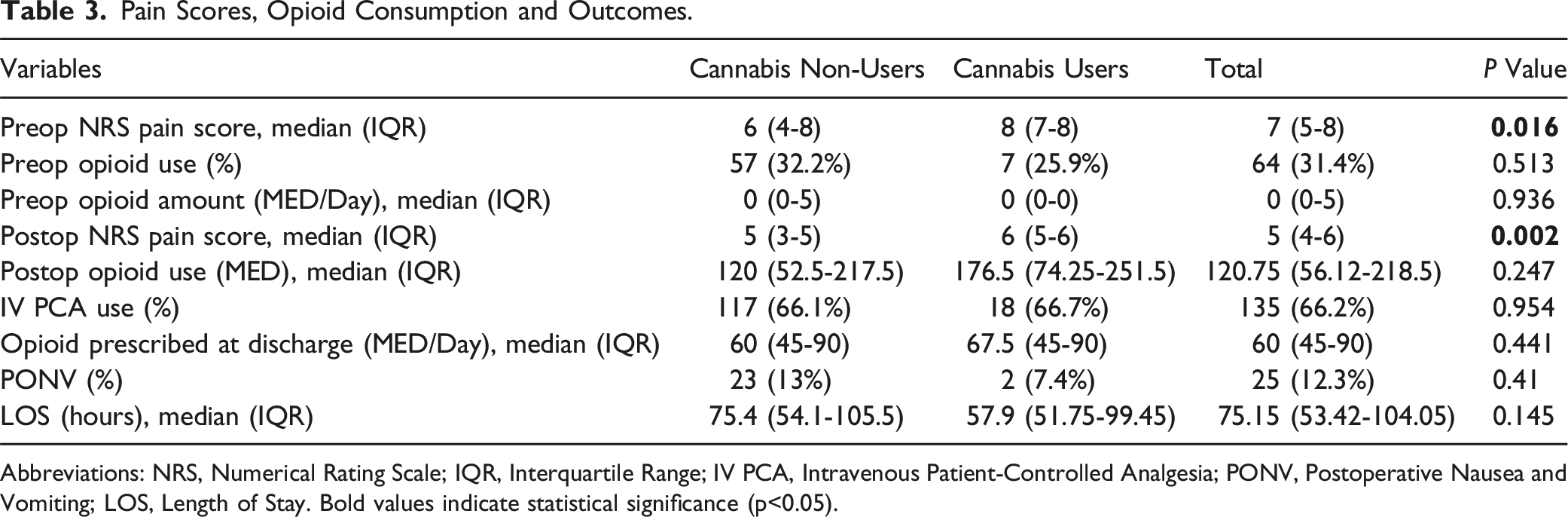
Abbreviations: NRS, Numerical Rating Scale; IQR, Interquartile Range; IV PCA, Intravenous Patient-Controlled Analgesia; PONV, Postoperative Nausea and Vomiting; LOS, Length of Stay. Bold values indicate statistical significance (p<0.05).
Multivariable Linear Regression for Preoperative Pain Scores.
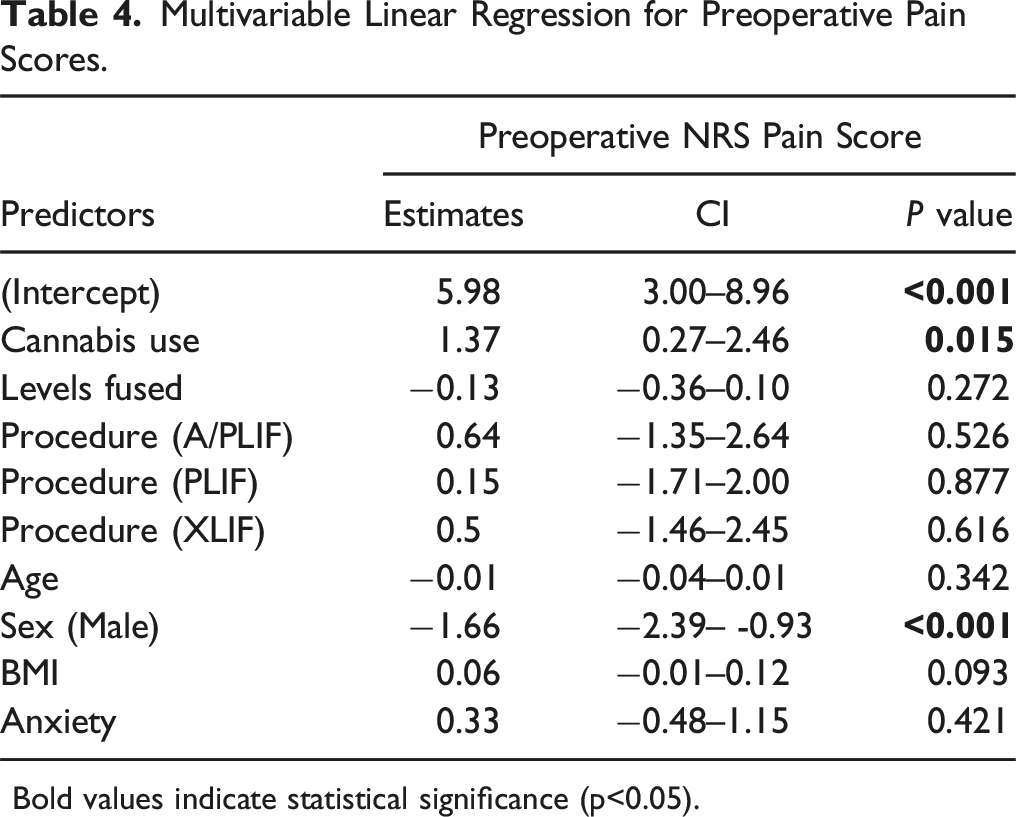
Bold values indicate statistical significance (p<0.05).
Multivariable Linear Regression for Postoperative Pain Scores.
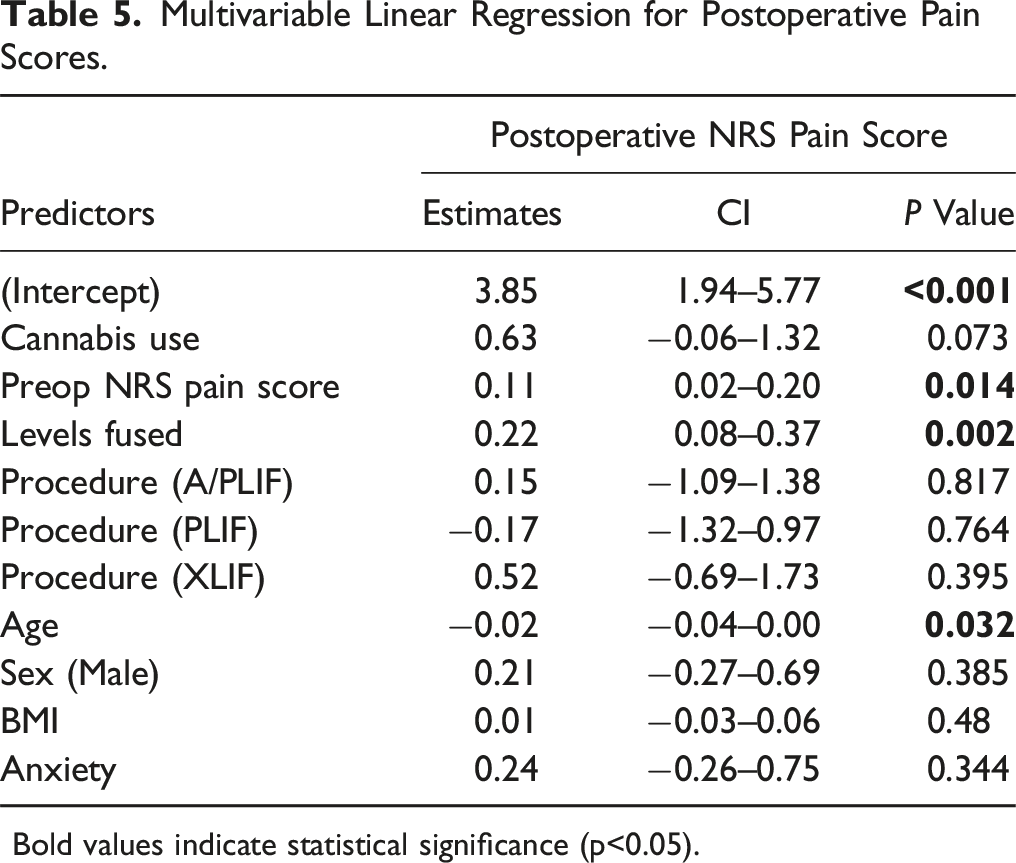
Bold values indicate statistical significance (p<0.05).
Discussion
We estimated the incidence of cannabis use in a cohort presenting for lumbar spinal fusion at 13.2%. Although this represents a substantial number of spine surgery patients anticipated to use cannabis, the proportion of users found here is substantially lower than the population incidence (22%) that has been estimated in national surveys over the past year. 2 This could represent underreporting, since we used self-reporting as our means of estimating cannabis use in this population. However, as the perception of cannabis becomes increasingly favorable and more U.S. states implement decriminalizing legislation, the prevalence of cannabis use is expected to rise. Indeed, the percentage of the population using cannabis in 2018 exceeded the figures reported between 2002 and 2017, reflecting a 6.1% increase in cannabis use over a 5-year period.2,10 These trends suggest prospective investigation of the incidence of cannabis use among spine surgery patients as well as effects on outcomes after surgery are warranted.
Effective pain management after spine surgery contributes to improved outcomes, fewer adverse events, and prompt discharge from hospital without increased readmission. 4 Conversely, inadequate pain control correlates with less patient satisfaction and prolonged hospitalization. Amidst the ongoing opioid epidemic, there is a critical need for alternative pain management strategies to reduce postoperative opioid consumption. The rationale for considering cannabis as an adjunctive analgesic lies in its potential opioid-sparing effects through cannabinoid-receptor 1 (CB1) activation, inhibiting calcium release and reducing nociceptor signaling.11,12 Cannabinoids can also activate cannabinoid-receptor 2 (CB2) on immune cells, releasing cytokines that indirectly stimulate various receptors, including μ-opioid receptors, transient receptor potential vanilloid 1 (TRPV1) located on sensory Aδ and C-fibers, N-methyl-D-aspartate (NMDA) and gamma-aminobutyric acid (GABA) receptors within the nervous system.12-15 An additional factor supporting cannabis use as an analgesic adjunct is the potential to reduce postoperative opioid-induced respiratory depression: Cannabinoids lack CB1 receptors in the central nervous system respiratory center and could improve pain control while minimizing opioid-induced respiratory depression. 14
Despite its theoretical benefits, clinical evidence on cannabis for perioperative pain management remains inconclusive. While cannabinoids have demonstrated efficacy in neuropathic and cancer-related pain, 11 their role in acute postoperative pain is less clear. Systematic reviews and randomized trials report mixed results, with most studies showing no significant benefit over placebo in acute pain management.16-18
Our findings align with Liu et al, who observed higher preoperative and postoperative pain scores in cannabis users undergoing orthopedic procedures. 19 Although our study identified similar trends, the differences did not reach statistical significance after adjusting for multiple variables. Jennings et al also reported no differences in opioid consumption postoperatively but noted increased early postoperative pain scores in cannabis users. 20 While some studies report no significant differences in postoperative opioid consumption,19-25 others suggest a potential opioid-sparing effect. 26 ' 27 One proposed mechanism is cannabinoid-opioid synergy, as both act on overlapping neural pathways. However, chronic CB1 receptor activation may lead to receptor downregulation, necessitating higher opioid doses for adequate pain control. 11 ' 28 This phenomenon is supported by studies identifying increased postoperative opioid requirements in cannabis users.29,30
Expanding on the relationship between cannabis use and surgical outcomes, Van Halm-Lutterodt et al and Razzouk et al found that cannabis use disorder (CUD) was associated with higher hospital readmission rates, increased revision surgery risk, and greater postoperative opioid consumption after anterior cervical discectomy and fusion (ACDF).31,32 Similarly, Dietz et al and Brenne et al identified increased complication rates, longer hospital stays, and higher opioid consumption among cannabis users undergoing cervical and lumbar spine fusions.33,34 However, Dietz et al also noted a decrease in long-term opioid dependence, suggesting cannabis may aid in opioid tapering strategies. While our study did not demonstrate significant differences in postoperative opioid consumption, it aligns with prior literature indicating that cannabis use does not provide an opioid-sparing effect in the acute postoperative period. Taken together, these studies suggest that cannabis use may be linked to greater perioperative risks, yet its long-term impact on pain management remains uncertain, warranting further research.
Our study also found a positive association between cannabis use and baseline anxiety disorders. A prospective study by Blanco et al reported increased odds of developing anxiety disorders with cannabis use, 35 though adjusted models did not confirm this association. 36 Anxiety is a well-established predictor of heightened postoperative pain perception,35-39 which may confound interpretations of cannabis’ effects on surgical pain. In our study, cannabis users demonstrated increased pain scores, but no significant association was observed between anxiety and postoperative pain after adjustment for confounders.
This study has several limitations. As a retrospective, single-center study at a specialty orthopedic hospital, generalizability is limited. While perioperative pain management regimens were standardized, variations in surgical technique across providers may have influenced pain and opioid consumption outcomes. Although the primary goal was to estimate the incidence of cannabis use in spinal fusion patients, the proportion of patients reporting use was low, which hampers attempts to draw strong conclusions regarding associations between other variables of interest. Additionally, the reliance on self-reported cannabis use likely led to underestimation, introducing potential bias. Details such as cannabis potency, strain, frequency, and method of consumption were inconsistently documented and thus could not be analyzed.
While our study assessed pain scores and opioid use, we did not evaluate functional outcomes, such as return to daily activities or work. These metrics would provide greater insight into cannabis’ clinical impact on postoperative recovery. However, due to the retrospective nature of our study, such data were not consistently recorded in medical records. Future prospective studies should incorporate standardized functional assessments to better characterize cannabis’ role in perioperative care. Finally, we were unable to determine whether cannabis use persisted postoperatively, limiting our ability to analyze its impact on longer-term recovery.
Conclusion
We estimated the incidence of cannabis use in a cohort undergoing lumbar spinal fusion to be low, and lower than population estimates of use. We found significant associations between cannabis use and anxiety disorder, and cannabis use and higher preoperative pain scores. It is unclear whether anxiety was risk factor for cannabis use, or if cannabis use led to a higher likelihood of anxiety in this cohort, but neither factor appeared to negatively affect the outcomes analyzed here. Likewise, postoperative pain scores, opioid consumption and discharge opioid prescribing were not different between cannabis users and non-users, suggesting pre-operative cannabis use did not negatively influence recovery after spine surgery. These results highlight the need for continued prospective research in this evolving landscape.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.