
Abstract
Study design
Systematic review and meta-analysis.
Objective
To compare outcomes and complication rates in patients undergoing bariatric surgery (BS) prior to spine surgery.
Methods
A systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines comparing the outcomes of spine surgery between subjects with prior bariatric surgery to those who were considered obese with no prior bariatric surgery.
Results
A total of 183, 570 patients were included in the 4 studies meeting inclusion criteria. The mean patient age was 52.9 years, and the majority were female (68%). The two groups consisted of a total of 36, 876 patients with prior BS and 146, 694 obese patients without prior BS. The overall rate of complications in the prior BS group was 6.4% (4.5%–38.7%) compared to 11.9% (11.2%–55.4%) in the non-prior BS obese group with a statistically significant difference between the two groups. The prior BS group had lower rates of renal, neurological, and thromboembolic complications, with a lower mortality and readmission rate. In a subgroup undergoing cervical spine surgery, patients with prior BS had fewer cardiac, GI, and total complications. For patients undergoing thoracolumbar spine surgery, patients with prior BS had fewer thromboembolic and total complications.
Conclusion
Patients undergoing bariatric surgery prior to spine surgery had fewer renal, neurological, and thromboembolic complications as well as a decreased mortality and readmission rate.
Introduction
According to the World Health Organization, worldwide obesity rates have nearly tripled. 1
A recent report by the New England Journal of Medicine (NEJM) 2019 estimated that nearly half of adults in the USA will be obese by 2030, indicating that prevalence will be at least 35% in any state, and nearly one in four will have severe obesity. 2 Severe obesity has direct implications on existing co-morbidities and increases the risk of developing or worsening existing spinal pathologies. Furthermore, up to 80% of patients undergoing lumbar spine surgery are obese. 3 As a result, preoperative weight loss has been strongly recommended to facilitate optimal therapeutic, surgical, and functional outcomes for patients with severe obesity (defined as BMI of >35 kg/m2) undergoing spinal surgery. This is supported by evidence documenting the relationship between high BMI and increased rates of adverse clinical outcomes including—but not limited to—extended length of stay, increased intraoperative blood loss, wound complications, and delayed healing amongst others.4,7
Bariatric surgery (BS) is a well-established and effective surgical weight loss intervention. It has been reported that morbidly obese patients achieve an average of 67% of their maximum weight loss in the first 2 years after BS, and most patients, including the super morbidly obese, or those with a BMI above 50 kg/m2 will achieve at least 50% of their maximum weight loss within the same time period.8,9 However, there is also a growing body of evidence that the altered Vitamin D metabolism seen in patients who have undergone BS has a negative effect on bone mineral density. This could predispose these patients to fragility fractures and enhance potential risk in instrumented spine surgery.
A limited number of studies have investigated any correlations between BS and spine surgery outcomes. Jain et al. 10 found that patients who underwent BS before lumbar spine surgery had significantly lower rates of medical complications and infections than their severely obese counterparts; however, rates of infection, revision, and readmission were still higher when compared to non-obese patients. Similarly, Passias et al. 11 noted improved outcomes in patients with prior BS undergoing cervical and thoracolumbar spinal surgery. In light of these observations, critical empiric evaluation is merited to determine the impact of BS on spinal surgery outcomes.
The objective of this review is to examine whether prior BS has an association with peri-operative complications in patients undergoing spine surgery. The two groups studied were obese patients with or without prior BS preceding spine surgery.
Materials and Methods
A systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 12 A search was performed in the MEDLINE, PubMed, EMBASE, Google scholar and Cochrane databases using the search terms ((((Bariatric surgery OR gastric band* OR “weight loss surgery” OR “obesity surgery”))) AND ((spine OR spinal fusion OR spinal surgery OR spinal disease*))) AND ((Postoperat* OR outcomes OR satisfaction OR results)). The final search was performed on May 31, 2020. In addition to these databases, the references of each article were also assessed manually for potential inclusion in the study.
Selection Criteria
Clinical studies were evaluated and included if they were in English and reported on surgical treatment of the spine, comparing subjects with prior bariatric surgery to obese patients without prior bariatric surgery. Nonclinical studies, literature reviews, expert opinions, case reports, and those not reporting both of the described cohorts were excluded. Studies were reviewed by two of the study authors (AA, NA), who performed title and abstract reviews separately. The full texts of the articles meeting inclusion criteria based on title and abstract were then reviewed for final inclusion in the study, with authors coming to a consensus in case of disagreement.
Quality Evaluation
Non-randomized included studies were evaluated using the Newcastle–Ottawa Scale. 13 This quality assessment was performed independently by two authors (AA, IM).
Data Extraction and Analysis
The data items that were collected included (1) study characteristics (author name, study year, level of evidence, follow-up period, and number of patients), (2) patient demographics (age, sex), (3) number of patients undergoing spinal surgery who had prior BS or obese patients without prior BS and (4) outcome measures. The primary outcome measure was total number of complications (overall, including both medical and surgical in cervical and thoracolumbar surgery subgroups). The secondary outcome measures included medical and surgical complications (cardiac, pulmonary, renal, neurological and gastrointestinal (GI)), thromboembolism (DVT, PE), wound complications, readmission rate, reoperation rates, and mortality rate. The data was extracted by two authors independently (AA, NH).
The data analysis was performed by constructing a random-effects model using open Meta-Analysis Software. For non-continuous variables, the odds ratio was utilized to estimate effect, with the values depicted in a forest plot diagram including 95% confidence intervals (CI). Statistical heterogeneity across the studies was tested using I2.
Results
Study Characteristics and Patient Demographics
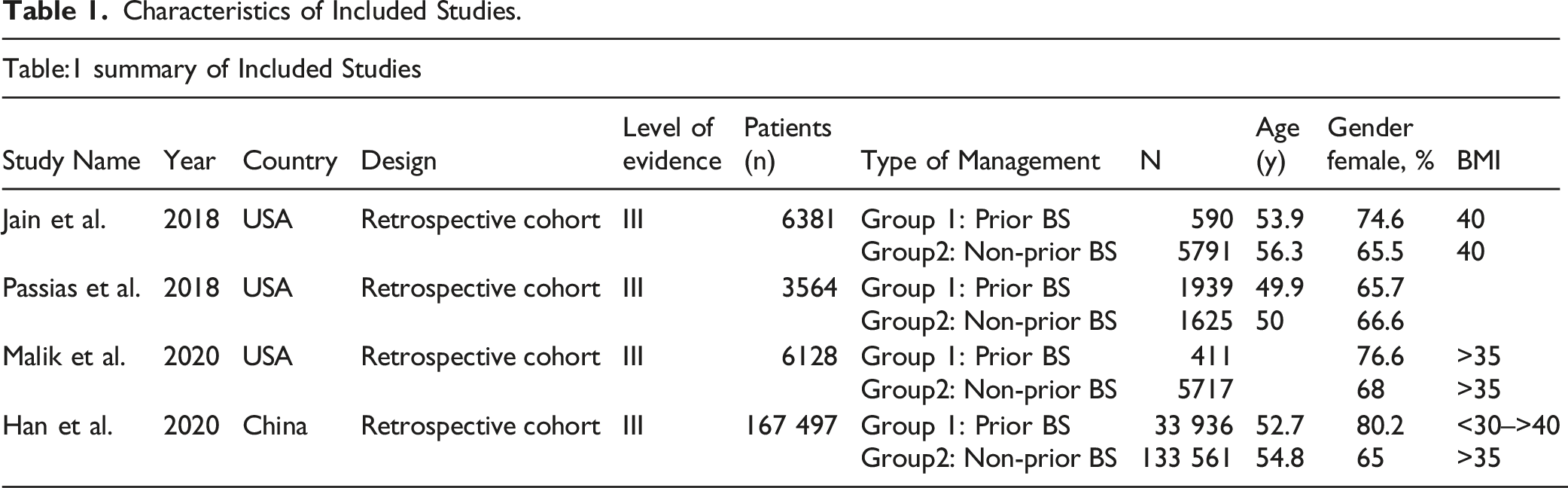
A total of 4 studies were included, with the selection process summarized in Figure 1. The characteristics of included studies and details of interventions are shown in Table 1. The four included studies were retrospective cohort studies, and all were evidence level III. A total of 183, 570 patients were included in the 4 studies (68% female; mean age 52.9 years). This encapsulates a total of 36, 876 with prior BS and 146, 694 in the obese, non-prior BS group. PRISMA flow chart. Characteristics of Included Studies.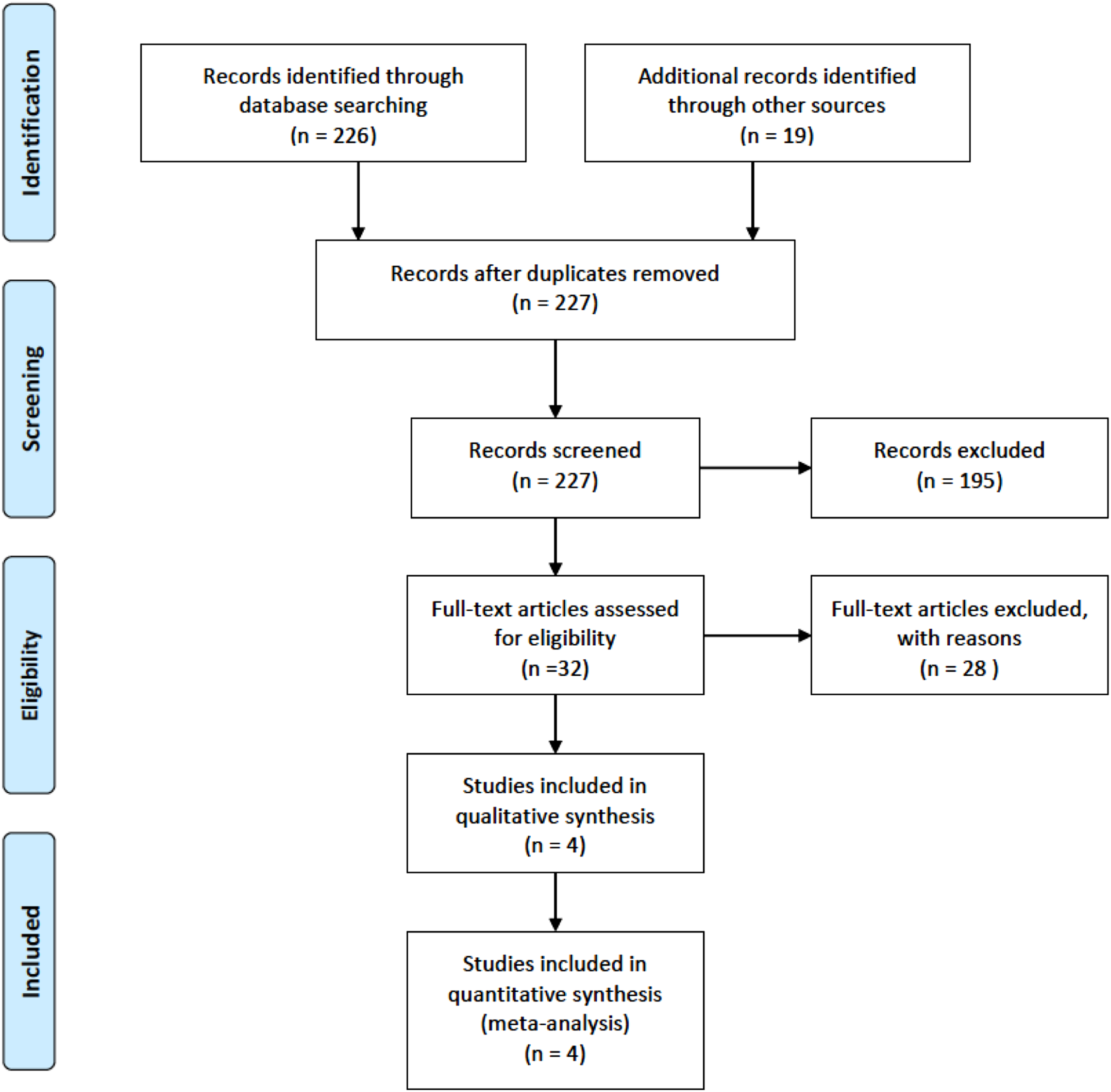
Quality Assessment
Quality assessment. (Newcastle–Ottawa Scale).

Total Number of Complications
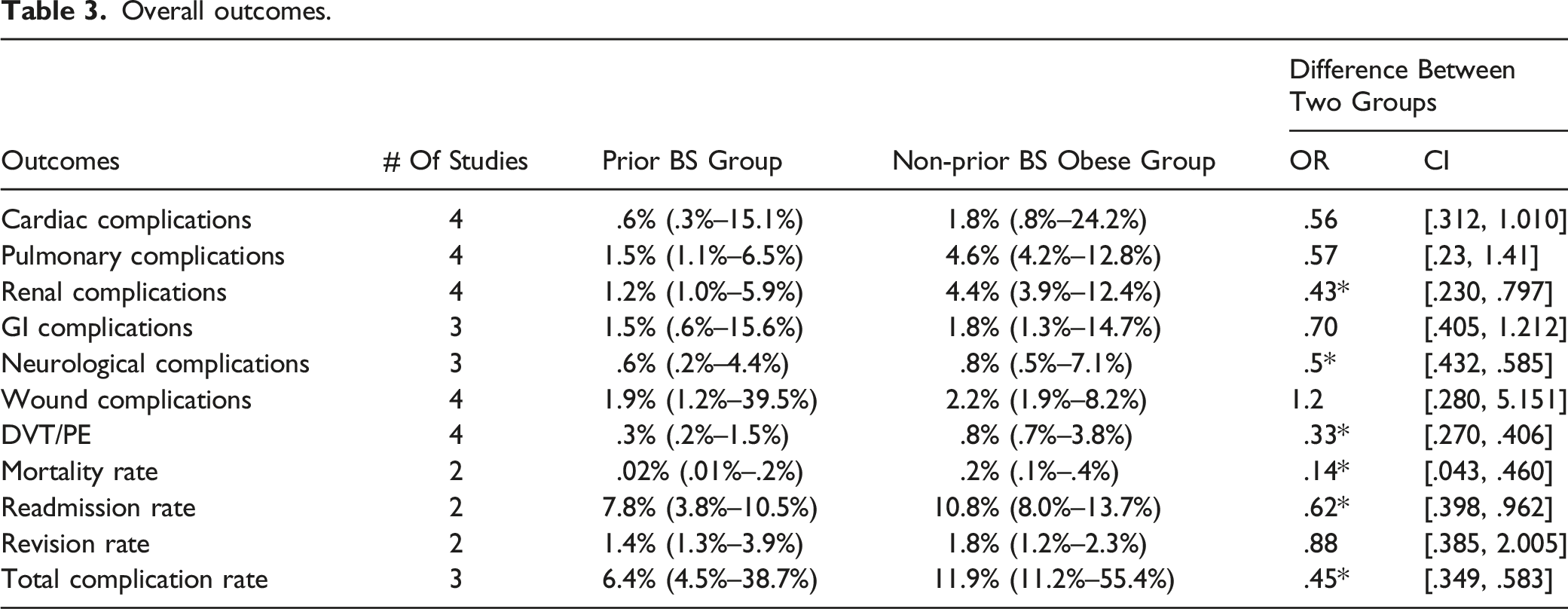
The overall rate of complications in the prior BS group was 6.4% (4.5%–38.7%) compared to 11.9% (11.2%–55.4%) in the non-prior BS obese group with a statistically significant difference between the two groups (OR: .45; 95% CI: [.349, .583] I2: 90.8%) (Figure 2, Table 3). Overall complications. Overall outcomes.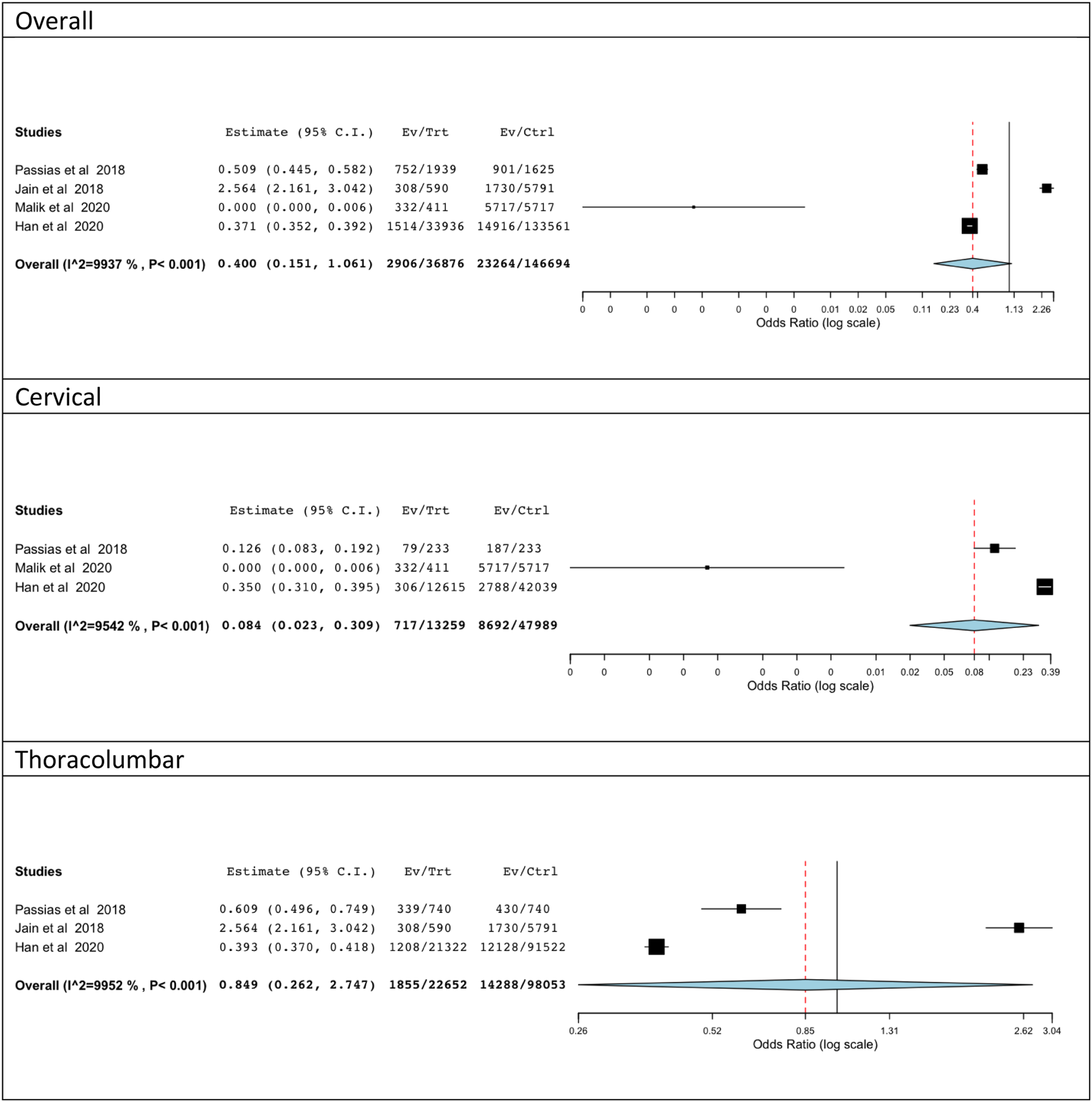
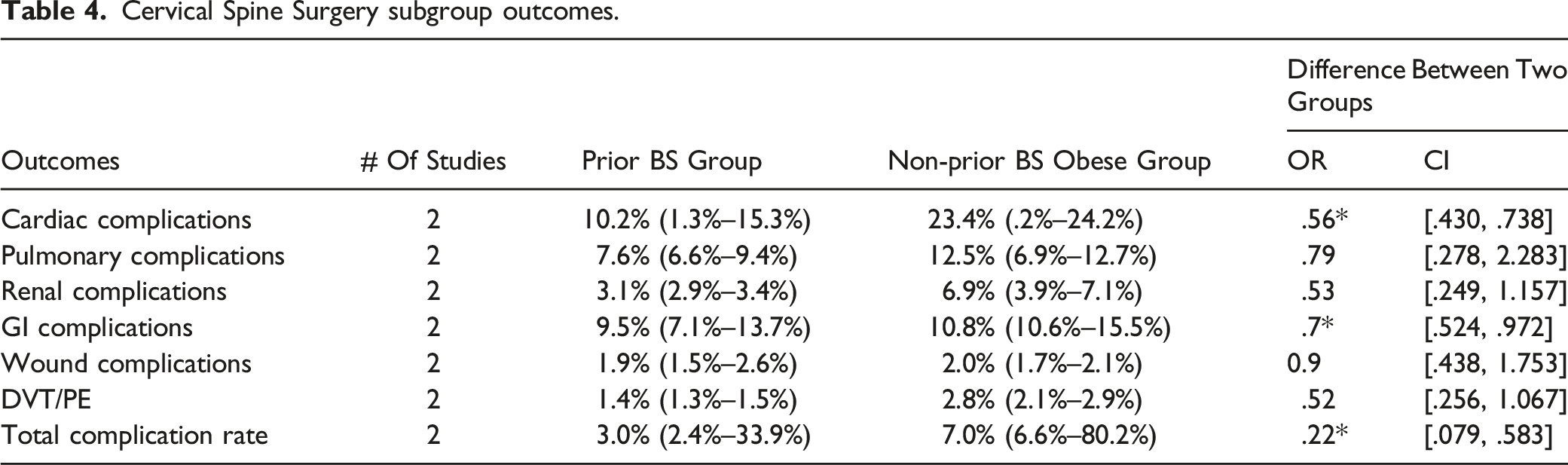
Cervical Spine Surgery subgroup outcomes.
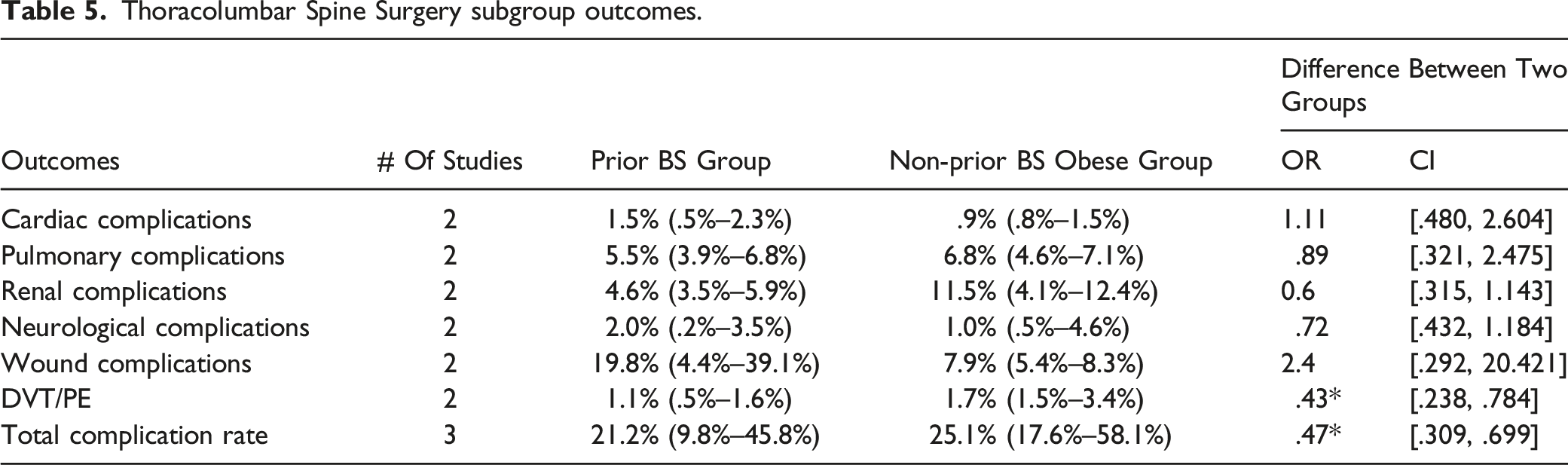
Thoracolumbar Spine Surgery subgroup outcomes.
Medical Complications
The total number of cardiac complications in the prior BS group was .6% (.3%–15.1%) vs 1.8% (.8%–24.2%) in the non-prior BS group with no statistical difference between the two groups (OR: .56; 95% CI: [.312, 1.010] I2: 89.6%) (Table 3).
In the cervical subgroup, the risk of cardiac complications in the prior BS group was less compared to the non-prior BS group (OR: .56; 95% CI: [.430, .738] I2: 0%), whereas no statistical difference in the risk of cardiac complications was noted between the two thoracolumbar subgroups (OR: 1.11; 95% CI: [.480, 2.604] I2: 36.05%) (Tables 4 and 5)
The total number of pulmonary complications in the prior BS group was 1.5% (1.1%–6.5%) vs 4.6% (4.2%–12.8%) in the non-prior BS group with no significant difference between the two groups (OR: .57 95% CI: [.23, 1.41] I2: 97.7%). Similarly, there was no significant difference in the risk of pulmonary complications between cohorts in the cervical (OR: .79; 95% CI: [.278, 2.283] I2: 86.3%) and thoracolumbar subgroups (OR: .89; 95% CI: [.321, 2.475] I2: 90.7%) (Tables 3–5).
The overall risk of renal complications was significantly less in the prior BS group (OR: .43; 95% CI: [.230, .797] I2: 93.2%). However, no significantly decreased risk of GI complications was seen in the prior BS group (OR: .70; 95% CI: [.405, 1.212] I2: 95.1%) (Tables 3–5).
The prior BS group had a lower overall neurological complication rate (OR: .50; 95% CI: [.432, .585] I2: 0%) (Table 3).
Thromboembolic Complications
The total number of thromboembolic events (DVT, PE) was significantly less in the prior BS group compared to non-BS obese group (OR: .33; 95% CI: [.270, .406] I2: 0%). There was no statistically significant difference in the subgroup analysis of the cervical (OR: .52; 95% CI: [.256, 1.067] I2: 0%) cohort for thromboembolic events; however, the thoracolumbar cohort did demonstrate a statistically significant difference (OR: .43; 95% CI: [.238, .784] I2: 0%) (Tables 3-5).
Wound Complications
There was no statistically significant difference in the overall risk of wound complications between the two cohorts (OR: 1.2; 95% CI: [.280, 5.151] I2: 98.3%), which was maintained in the cervical (OR: .9; 95% CI: [.438, 1.753] I2: 0%) and thoracolumbar subgroup analysis (OR: 2.4; 95% CI: [.292, 20.421] I2: 99.4%). Notably, the odds ratio did demonstrate an elevated though nonsignificant risk associated with wound complications in the prior BS group (Tables 3–5).
Re-Admission, ReOperation, and Mortality
There were significantly fewer readmissions in the prior BS group compared to the non-prior BS group (OR: .62; 95% CI: [.398, .962] I2: 60.3%), whereas no statistical difference was noted between the two groups with regards to revision (OR: .88; 95% CI: [.385, 2.005] I2: 58.6%). The prior BS group also demonstrated a lower mortality rate (OR: .14; 95% CI: [.043, .460] I2: 32.5%) compared to non-prior BS obese group (Figure 3; Tables 3–5). Overall Re-admission rate, overall operation rate, overall mortality.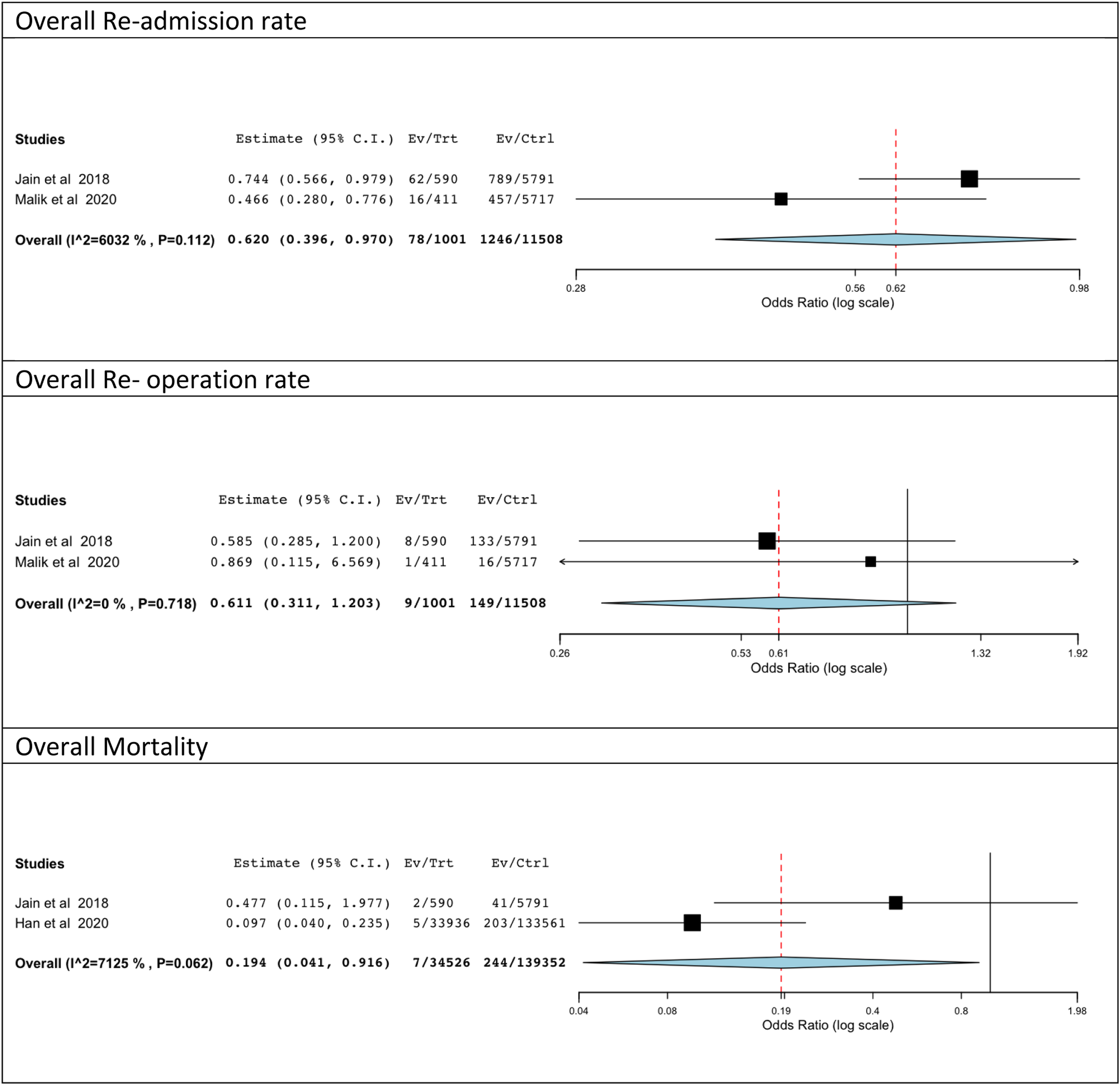
Discussion
Bariatric surgery is a rapid weight reduction procedure with a high patient satisfaction rate. Short and long-term effects of this procedure, especially as they relate to musculoskeletal health, are varied and have been extensively reported. Expected changes after BS include fat loss, muscle wasting, significant alterations in skeletal muscle metabolism, and improved exercise capacity.28,29,30,31 Given the generally positive effects of BS on weight and overall health, similar improvements in peri-operative outcomes after spine surgery may be expected. In this meta-analysis comparing outcomes between more than 180 000 obese patients undergoing spine surgery, we found that the overall complication rate of the prior BS group was lower compared to the obese non-prior BS group. Furthermore, this study demonstrated that prior BS was associated with fewer renal, neurological, and thromboembolic complications, as well as decreased mortality and readmission rates. It is also noted that the BS patients had a significantly lower medical comorbidity burden and a shorter length of hospital stay as compared to obese patients without prior BS, which may be indirect contributors to the observed lower total complication rate in this cohort.23-25
It is well established that obesity is an independent risk factor for postoperative complications. 33 These complications may be inherent to surgical intervention, such as deep or superficial surgical wound infections. Additionally, systematic complications such as DVT, UTI, ARDS may stem from co-morbidities typically associated with obesity.3,14,15 As demonstrated in this study, there does appear to be an overall benefit associated with bariatric surgery prior to spine surgery. However, despite the suspected and observed benefits, the effect of bariatric surgery on bone metabolism may raise issues related to long-term complication rates following spine surgery, particularly fusion procedures. The available evidence indicates that the negative effects on bone homeostasis leading to increased bone turnover, significant vitamin deficiencies (D, B12, E), and decreased bone mineral density may persist for several years after bariatric surgery.16,21 The potential resultant effects on rates of pseudarthrosis and implant complications have not been well studied.
Bariatric surgery and its relation to axial back pain is still under investigation. Notably, Epstein et al found that bariatric surgery may lead to reduced axial back pain which may mitigate the necessity of extended nonoperative treatment or primary surgical intervention. 16 On the other hand, Passias et al. 22 compared obese patients with and without BS and found that the BS population had an elevated risk of a spine disease diagnosis which may lead to a higher rate of spinal procedures. These disparate findings serve to highlight the complex relationship between obesity and spinal pathology and potential opportunities for future study.
In the context of our analysis, several studies have suggested the utility of bariatric surgery to improve spine surgery outcomes in morbidly obese individuals. In contrast, Jain et al. demonstrated that BS patients undergoing posterior lumbar spine fusion had significantly increased rates of wound infection, reoperation, and readmission rates, when compared to non-obese patient undergoing the same procedure. However, there was no significant difference in the length of hospital stay and systemic complications between the two groups. 25 With regards to the increased wound infection rate in the thoracolumbar BS group as compared to the non-BS group, a number of explanations are plausible. Metabolic derangements, as noted above in the context of bone mineralization, can also affect wound healing. D’Ettore et al found when investigating wound protein composition that non-smoking patients with prior BS had decreased wound collagen content similar to patients with a history of smoking, a known contributor to impaired healing. 32 Moreover, BS can lower levels of factors known to influence wound healing, such as vitamins B9, B12, and D. Therefore, it seems that BS is associated with a suboptimal healing response, which provides further context for the increased wound complications seen in BS patients.
This study has several limitations. As all of the compiled studies included in this meta-analysis were retrospective database studies, our results are subject to the limitations of database research including potential miscoding, the inability to track patients across multiple admission, and absence of more granular, patient-level data which might allow more definite conclusions to be drawn. Furthermore, the BMI or BMI range of patients who had previous bariatric surgery vs those without was not largely available (only one study reported the BMI range for the BS cohort at time of surgery), nor was the exact time from BS to spine surgery, precluding our ability to say that the observed decreased risk for postoperative complications conferred by BS was related to resulting weight loss or decreased BMI. However, Han et al did note in a subgroup analysis of patients with BMI <35 kg/m2 that the benefits of prior BS appeared to be more pronounced in patients with documented weight loss after BS, though these results were also observed, albeit to a lesser degree, in the subgroup with prior BS and BMI >35 kg/m2. As previously discussed, due to the sources of the compiled data, this paper also fails to adequately evaluate the risk for long-term medical or surgical complications. This study demonstrates that bariatric surgery appears to confer an overall benefit with regards to short-term systemic complications, readmission, and mortality rates following spine surgery. Further research is merited to discuss the utility of prior bariatric surgery in mitigating adverse outcomes from spine surgery in morbidly obese patients, especially in the context of the metabolic derangements and their resulting effects on bone mineral density and wound healing.
Conclusion
Despite the high rate of overall complications in prior BS patients undergoing spine surgery, there does appear to be a benefit conferred to patients with BS as compared to obese patients without BS in terms of renal, GI, neurological, and thromboembolic complications, as well as readmission and mortality rates. Spine surgeons should be aware of the benefits of bariatric surgery as a strong weight loss management strategy prior to spine surgery procedures, while also recognizing that bariatric surgery may also contribute to Vitamin D deficiency and decreased bone mineral density, the long-term effects of which are poorly understood as they relate to spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
No direct funding was received for this study. However, this study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.