
Abstract
Study Design:
Longitudinal cohort.
Objectives:
The Hospital Anxiety and Depression Scale (HADS) was developed to provide clinicians a reliable, valid, and practical tool to identify and quantify the anxiety and depression in medical patients. Several studies have shown that patients with chronic low back pain may have subclinical depression and impairments in mental health and that these in turn may lead to less than optimal results after lumbar spine surgery. The purpose of this study is to determine if there are associations between preoperative HADS and differences in pre- and postoperative health-related quality-of-life (HRQOLs) scores after spine surgery.
Methods:
From a single center, a consecutive series of patients completed the HADS, Oswestry Disability Index (ODI), Short Form-36 (SF-36), EuroQOL-5D (EQ-5D), and Visual Analog Scale (VAS) for back and leg pain. Except for HADS, the patients completed the same HRQOLs 1 year after surgery.
Results:
Of 308 eligible cases, 208 (68%) had follow-up data available and were included in the analysis. Patients in the HADS-Anxiety (HADS-A) Abnormal category had the worst preoperative HRQOLs but had the greatest improvement in 1-year postoperative scores. Except for VAS Leg Pain, preoperative HRQOLs were better in patients in the HADS-Depressed (HADS-D) Normal category. Patients in the HADS-D Abnormal category had statistically significantly greater improvement in 1-year postoperative EQ-5D and ODI scores when compared with the other cohorts.
Conclusion:
Worse HADS-A and HADS-D scores are associated with worse preoperative HRQOL scores in patients with lumbar degenerative disorders scheduled for spine surgery. However, similar improvements in HRQOLs can be expected 1 year postoperative regardless of the patients’ HADS scores.
Keywords
Introduction
Several studies have shown that patients with anxiety or depression may have poorer outcomes after surgery for lumbar degenerative disorders. 1 -9 These conclusions were drawn from questionnaires specifically designed to measure anxiety and depression such as the Distress and Risk Assessment Method, 3,10 Minnesota Multiphasic Personality Inventory, 11 or the Beck Depression Inventory. 5,12 These questionnaires are not routinely administered in the spine surgery clinic.
The Hospital Anxiety and Depression Scale (HADS) 13 was developed to provide clinicians with a reliable, valid, and practical tool to identify and quantify anxiety and depression specifically in patients seeking medical care for nonpsychiatric conditions. The HADS does not include physical symptoms of psychological distress such as weight loss and headache, which may be due to an underlying medical condition. 13 -15 It also leaves out symptoms indicating pathologic psychological conditions in order to improve acceptability by respondents in the medical or surgical clinic and to increase sensitivity to milder forms of psychiatric disorders.
The HADS is a patient-completed survey consisting of 14 items with responses on a 4-point Likert-type scale scored 0 to 3. 13 There are 2 domains: Anxiety (7 items) and Depression (7 items). The HADS Anxiety domain (HADS-A) consists of items identifying symptoms of generalized anxiety disorder. The HADS Depression domain (HADS-D) consists of items identifying anhedonia. The total score is the sum of the 14 items, and for each domain, the score is the sum of the respective 7 items. For each domain, scores range from 0 to 21, with higher values denoting worse scores with the following threshold values: 0 to 7 is Normal, 8 to 10 is Borderline, and 11 to 21 is Abnormal. 13,14 Normal denotes that Anxiety and/or Depression are probably absent, Borderline indicates that Anxiety and/or Depression are possibly present, and Abnormal denotes that Anxiety and/or Depression are probably present. 13,14 Previous studies have shown that it is reliable, valid, and sensitive to change. 15 Factor analysis confirmed the presence of 2 domains, with items loading appropriately to the respective scale. 13 -16
The purpose of this study is to determine if there are associations between preoperative HADS and differences in pre- and postoperative health-related quality-of-life (HRQOL) scores after spine surgery.
Methods
From a single spine center, a consecutive series of patients completed the HADS, 13 Oswestry Disability Index (ODI), 17,18 Short Form-36 (SF-36), 19 EuroQOL (EQ-5D), 20 and Visual Analog Scale (VAS) for back and leg pain 21,22 in the hospital prior to their surgery on the day of admission. Except for HADS, the patients completed the same HRQOL questionnaire 1 year after surgery via mail. Patients were classified into Normal, Borderline, and Abnormal based on their HADS-A and HADS-D scores. 13,14 Standard demographic data including age, sex, height, weight, smoking status, and surgical data including type of surgery and number of levels fused were also collected.
Oswestry Disability Index
The ODI 17,18 is a self-administered questionnaire measuring “back-specific function” on a 10-item scale with 6 response categories each. Each item scores from 0 to 5, which is transformed into a 0 to 100 scale. Patients with scores between 0 and 20 have Minimal Disability, between 21 and 40 have Moderate Disability, between 41 and 60 have Severe Disability, 61 to 80 are crippled, and 81 to 100 are bed-bound or exaggerating their symptoms.
Short-Form 36
The SF-36 is a 36-item self-administered short-form health status survey developed in the Medical Outcomes Study that evaluates physical function, social function, limitations in role due to physical health, limitation in role due to mental health, vitality, bodily pain, and general health. 19 Two composite scores can be calculated: a physical composite summary score (PCS) and a mental composite summary score (MCS). 23
EuroQOL-5D
The EQ-5D-3 Level 20 consists of 2 pages—a descriptive system and a visual analogue scale (EQ VAS). The descriptive system has 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression; each with 3 levels: no problems, some problems, and extreme problems. The respondent indicates his/her health state by marking the box with the most appropriate statement in each of the 5 dimensions. The EQ VAS records the respondent’s self-rated health on a vertical, visual analogue scale where the endpoints are “Best imaginable health state” and “Worst imaginable health state.” The scoring algorithm for the population of the United Kingdom was used to assign a value, or index score, that incorporates UK population–based preference weights 1. The EQ-5D scores for the UK population range from −-0.59 (worse than death) to 1.0 (full health), with a score of 0 indicating death. 24
Visual Analog Scale (VAS) for Back and Leg Pain
VAS for back and leg pain is a respondent-completed, unidimensional measure of pain intensity using a continuous scale on a horizontal line 100 mm in length, anchored by “no pain” (score of 0) and “worst imaginable pain” (score of 100). The respondent is asked to place a mark on the VAS line at the point that represents their pain intensity. The score is determined by measuring the distance between the “no pain” anchor and the patient’s mark, providing a range of scores from 0 to 100. 21,22
All statistical analyses were conducted using IBM SPSS Statistics Version 20 (IBM Corporation, Armonk, NY). In order to account for multiple concurrent analyses, significance was set at the P < .01 level for all comparisons. Analysis of variance (ANOVA) with post hoc Bonferroni correction was used to determine any significant differences in continuous variables among groups, and Fisher exact test was used to compare categorical variables among groups. Spearman correlation coefficients were determined to examine associations between HADS scores and preoperative and 1-year change in HRQOL scores.
All patient data are strictly confidential and stored according to the Danish Open Administration Act, the Danish Act on Processing of Personal Data, and the Health Act. This study was reviewed and approved by the Research Board of the Center for Spine Surgery and Research, Middelfart Hospital.
Results
Of 308 eligible cases, only the 208 cases (68%) with complete preoperative and 1-year follow-up data available were included in the analysis. Cases with any missing questionnaire preoperatively or at follow-up were excluded. Looking at the Anxiety domain, the majority of cases were in the HADS-A Normal category (110, 53%), followed by Abnormal (57, 27%) and Borderline (41, 20%; Table 1). Patients had similar demographics among the 3 cohorts (Table 1). Preoperative HRQOL scores were consistently worse in patients in the HADS-A Abnormal category. Patients in the HADS-A Abnormal category had the greatest improvement in 1-year postoperative scores but this was only statistically significant for the EQ-5D (Table 1).
Summary of Demographic and Health-Related Quality of Life Data Stratified by HADS Anxiety Category.
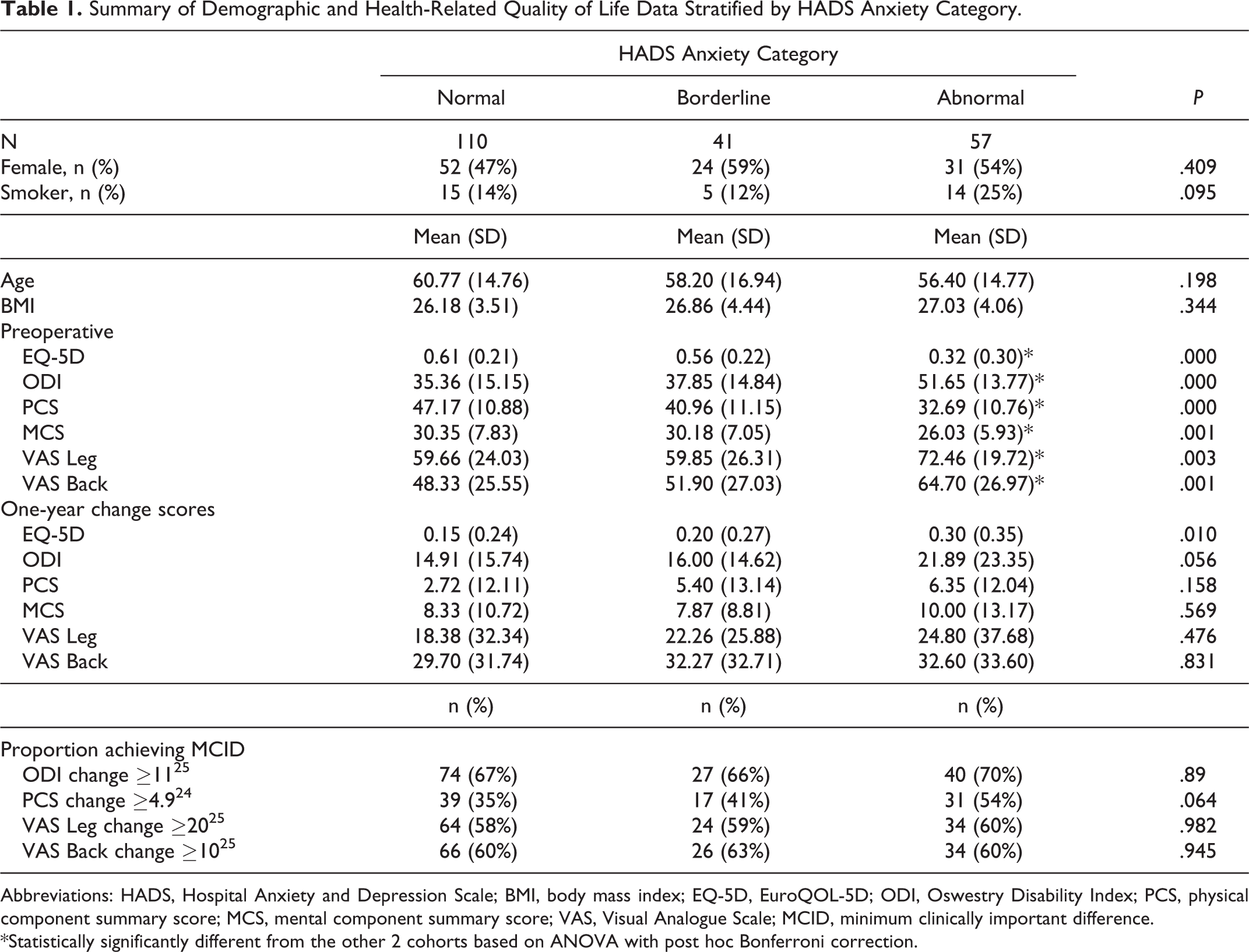
Abbreviations: HADS, Hospital Anxiety and Depression Scale; BMI, body mass index; EQ-5D, EuroQOL-5D; ODI, Oswestry Disability Index; PCS, physical component summary score; MCS, mental component summary score; VAS, Visual Analogue Scale; MCID, minimum clinically important difference.
*Statistically significantly different from the other 2 cohorts based on ANOVA with post hoc Bonferroni correction.
HADS-D: The majority of cases were in the Normal category (136, 65%), followed by Abnormal (41, 20%) and Borderline (31, 15%; Table 2). Patients had similar demographics among the 3 cohorts. Except for VAS Leg Pain, preoperative HRQOLs were consistently better in patients in the HADS-D Normal category. Patients in the HADS-D Abnormal category had statistically significantly greater improvement in 1-year postoperative EQ-5D and ODI scores among the cohorts (Table 2).
Summary of Demographic and Health-Related Quality of Life Data Stratified by HADS Depression Category
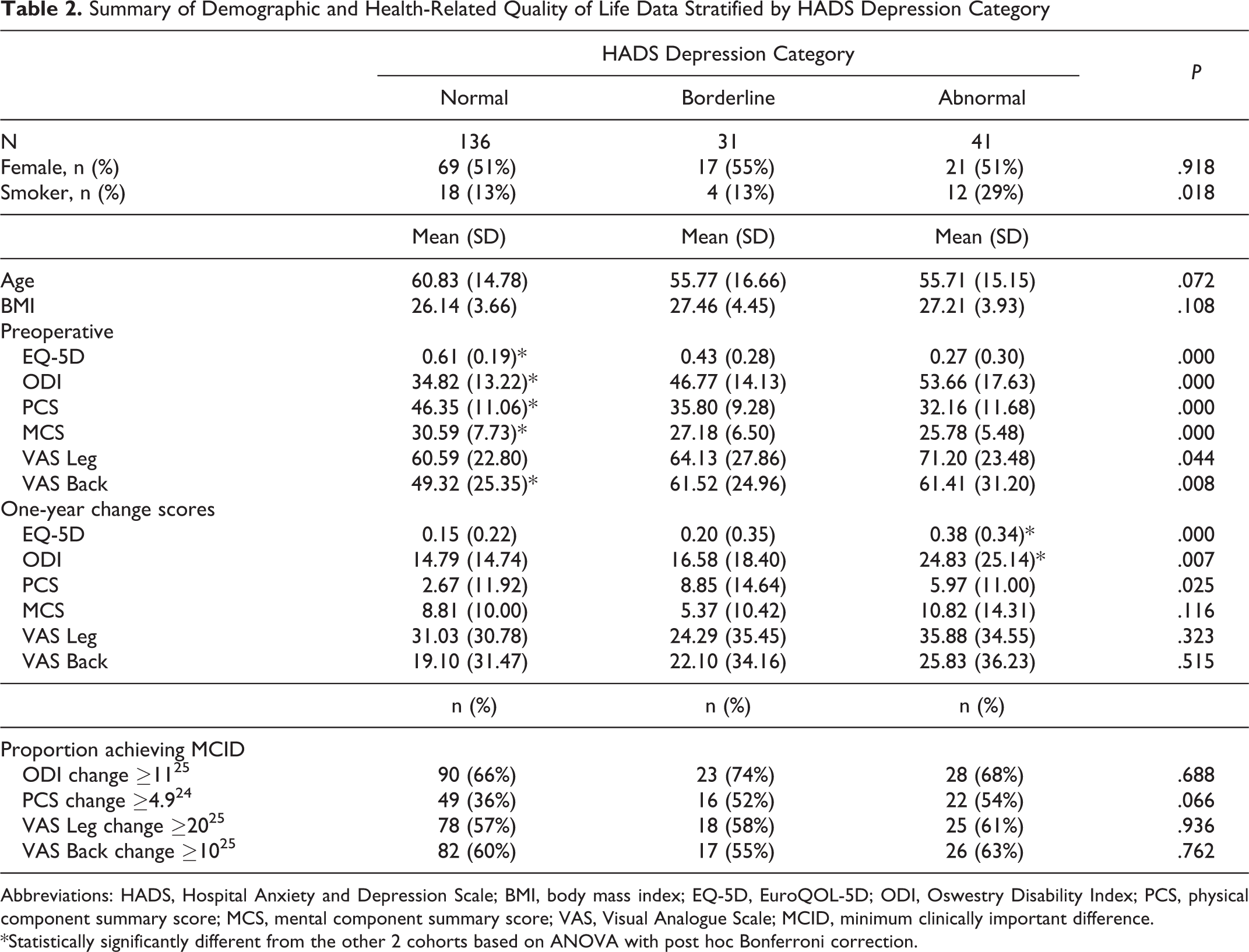
Abbreviations: HADS, Hospital Anxiety and Depression Scale; BMI, body mass index; EQ-5D, EuroQOL-5D; ODI, Oswestry Disability Index; PCS, physical component summary score; MCS, mental component summary score; VAS, Visual Analogue Scale; MCID, minimum clinically important difference.
*Statistically significantly different from the other 2 cohorts based on ANOVA with post hoc Bonferroni correction.
Spearman correlations between preoperative HADS scores all HRQOL scores were statistically significant but showed mostly weak associations (Table 3). Only moderate associations between HADS-D and preoperative EQ-5D and ODI were seen. Spearman correlations between 1-year change in HRQOL scores were statistically significant only for theEQ-5D. However, the correlation coefficients of association (HADS-A, r = 0.21; HADS-D, r = 0.22) were weak (Table 3).
Correlation Coefficients, Signifying Strength of Association Between HADS Scores and HRQOL Scores.
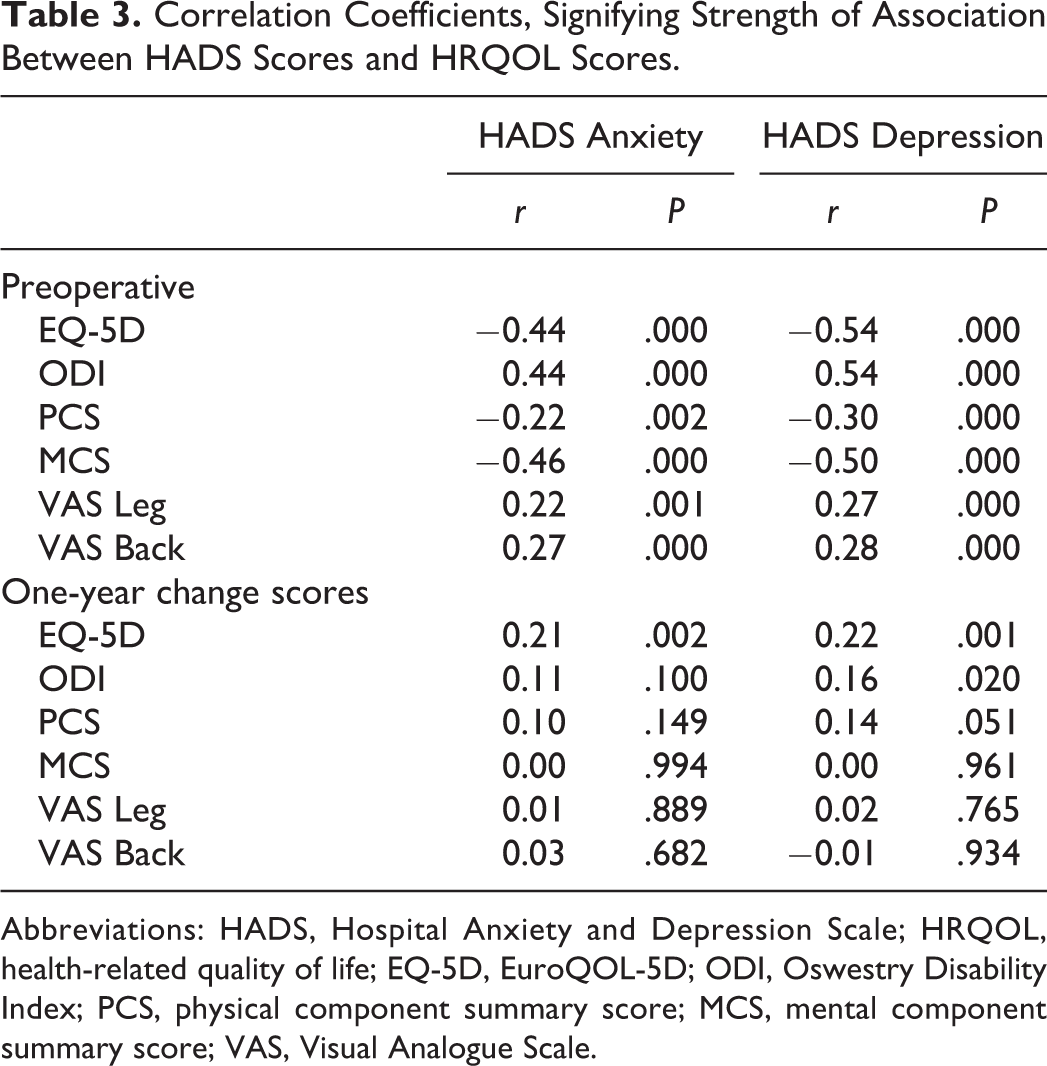
Abbreviations: HADS, Hospital Anxiety and Depression Scale; HRQOL, health-related quality of life; EQ-5D, EuroQOL-5D; ODI, Oswestry Disability Index; PCS, physical component summary score; MCS, mental component summary score; VAS, Visual Analogue Scale.
Discussion
Several studies have shown that patients presenting with some form of psychological distress have lower and HRQOL scores 7,9,25,26 after surgery for lumbar degenerative disorders. However, these studies used measures such as the Distress and Risk Assessment Method, 3,10 the Zung Depression Scale, 2,27 or the Pain Catastrophizing Scale, 4,28 which are designed to detect pathologic psychological conditions. Thus, these patients may actually have conditions that required medical and psychotherapeutic intervention prior to their surgery rather than a subclinical depression or mild impairments in mental health.
In the current study, although patients in the HADS-A Abnormal category had worse HRQOL scores preoperatively compared with the other 2 groups, they had similar improvements in all HRQOLs as patients in the HADS-A Normal and Borderline groups. Similarly, even though patients in the HADS-D Normal category had better preoperative HRQOL scores than patients in either the HADS-D Borderline and Abnormal categories, improvements in SF-36 PCS, SF-36 MCS, leg and back pain were similar among the HADS-D categories. While patients in the HADS-D Abnormal category had statistically significantly greater improvements in EQ-5D and ODI scores at 1-year postoperative. The findings in this study are similar to a previous study of patients undergoing surgery for various degenerative cervical and lumbar spine pathologies 29 that showed worse HADS scores in patients with poor physical functioning prior to surgery, but no associations between HADS scores and improvement in physical functioning after surgery.
Two studies with small sample sizes showed that that preoperative HADS-A was predictive of unsatisfactory results in patients undergoing lumbar discectomy. 30,31 This may be due to the presence of lower extremity radiculopathy along with back pain. Studies have shown that patients who complain of back and leg pain have more severe pain and disability, and take longer to recover compared with those with back pain alone. 32,33 Neither of these 2 studies used validated measures of physical function.
The results of the current study show that preoperative HADS scores cannot be used to help identify patients who may have worse HRQOL scores 1 year after lumbar spine surgery. HADS is probably identifying a normal psychological reaction to being in the hospital and being prepared to undergo major surgery. This is in contrast to other measures such as the Distress and Risk Assessment Method, 10 the Zung Depression Scale, 27 and the Pain Catastrophizing Scale, 28 which diagnose the presence of actual pathologic psychological conditions and have been found to be associated with postsurgical treatment outcomes.
There are limitations to this study. These include a disparity in the number of subjects in the 3 cohorts, with the majority of the patients being in the HADS Normal category. Larger sample sizes in the Borderline and Abnormal categories may have shown a difference in outcomes in these cohorts. Longer term follow-up would have been ideal, but PRO data was available only at the 1-year follow-up. This study was performed at a single institution, which may limit the external validity of the conclusions reached in this study. Replication of the current study in other institutions, and even other countries, may be warranted to determine if similar results will be seen.
In conclusion, although both the HADS-A and HADS-D are associated with worse HRQOL scores in patients with lumbar degenerative disorders scheduled for spine surgery, they are not associated with the extent of improvement in HRQOL scores after surgery. That is, similar improvements in HRQOL scores can be expected 1 year after lumbar spine surgery regardless of the patients’ HADS scores. Some emotional distress in the form of anxiety and depression can be expected in patients scheduled for lumbar spine surgery.
Footnotes
Authors’ Note
No other person aside from the authors made substantial contributions to conception, design, acquisition of data, or analysis and interpretation of data, or was involved in drafting the manuscript or revising it critically for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LYC is an employee of Norton Healthcare; Member, Editorial Advisory Board, Spine Deformity, Spine, and Spine Journal; Institutional Review Board Member, University of Louisville; Research Committee Member, Scoliosis Research Society; receives research funds from the Orthopedic Research and Educational Fund, 2013-present; received funds for travel for Study Planning Meetings from the Center for Spine Surgery and Research of the University of Southern Denmark; University of Louisville. ABJ, CCS, KHJ, and MOA have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.