
Abstract
Posterior cervical laminoforaminotomy is an effective treatment for cervical radiculopathy due to disc herniations or spondylosis. Over the last decade, minimally invasive (i.e., percutaneous) procedures have become increasingly popular due to a smaller incision size and presumed benefits in postoperative outcomes. We performed a systematic review of the literature and identified studies of open or percutaneous laminoforaminotomy that reported one or more perioperative outcomes. Of 162 publications found by our initial screening, 19 were included in the final analysis. Summative results indicate that patients undergoing percutaneous cervical laminoforaminotomy have lower blood loss by 120.7 mL (open: 173.5 mL, percutaneous: 52.8 mL, n = 670), a shorter surgical time by 50.0 minutes (open: 108.3 minutes, percutaneous: 58.3 minutes, n = 882), less inpatient analgesic use by 25.1 Eq (open: 27.6 Eq, percutaneous: 2.5 Eq, n = 356), and a shorter hospital stay by 2.2 days (open: 3.2 days, percutaneous: 1.0 days, n = 1472), compared with patients undergoing open procedures. However, the heterogeneous nature of published data calls into question the reliability of these summative results. Further structured trials should be conducted to better characterize the risks and benefits of percutaneous laminoforaminotomy.
Keywords
Posterior laminoforaminotomy is a well-established technique for cervical radiculopathy, first described in the mid-20th century by Spurling and Scoville, 1 and soon after by Frykholm. 2 For over five decades, the traditional posterior foraminotomy relied on an open “keyhole” approach performed through a midline incision. In 2001, Adamson published the first report of microendoscopic laminoforaminotomy. 3 Since then, multiple reports of similar procedures have been published.45678910–11 Percutaneous laminoforaminotomy is appealing due to a smaller incision size and presumed benefits in blood loss, hospital stay, and pain medication use. However, percutaneous procedures may also be associated with longer surgical time, increased risk of intraoperative and postoperative complications, and a longer surgeon learning curve. 12
In this systematic review, we compare published blood loss, surgical time, pain medication use, and postoperative hospital stay in open and percutaneous laminoforaminotomy.
Materials and Methods
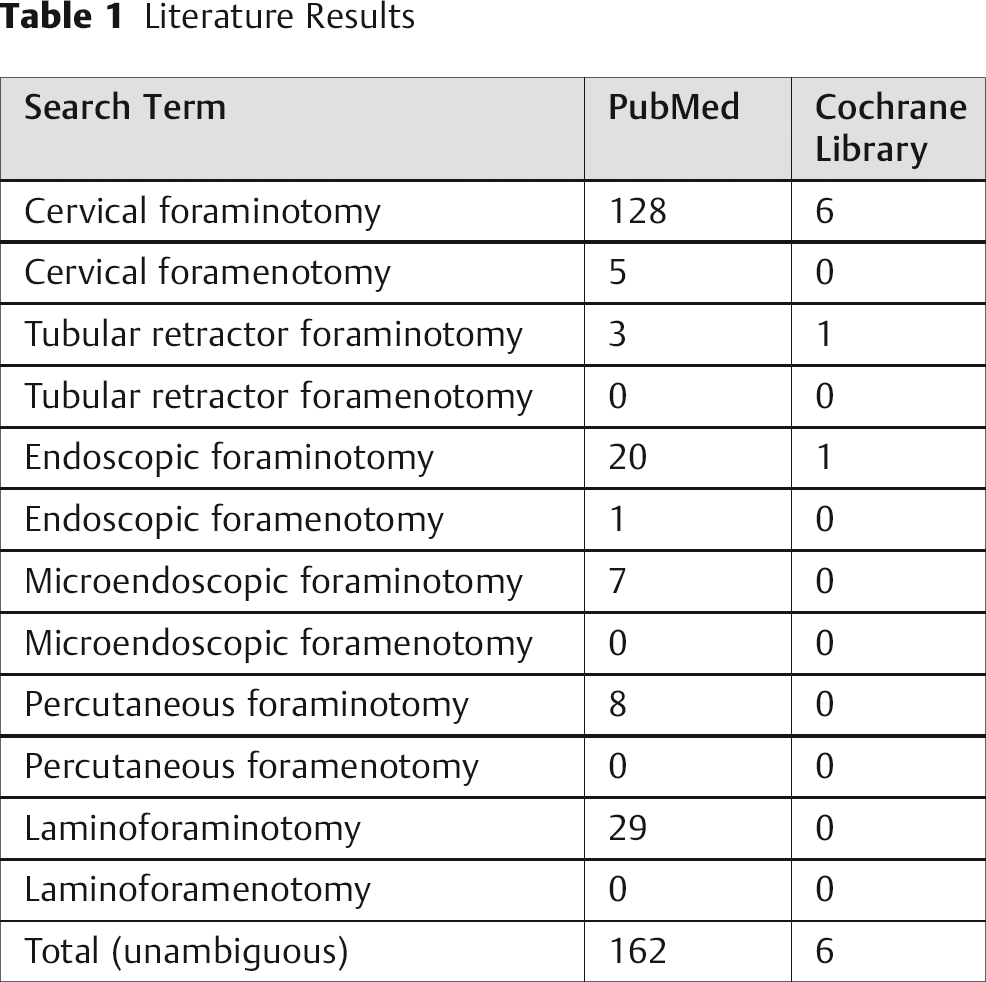
The PubMed and Cochrane library databases were searched in April of 2011 to find English-language publications reporting outcomes from percutaneous or open cervical laminoforaminotomy (Table 1). An initial search found 162 papers published between January 1990 and April 2011. Titles and abstracts of these papers were examined to identify reports that contained objective surgical outcomes. Studies that contained pooled open and percutaneous data, case reports, procedures related to the atlantoaxial junction, and laminoforaminotomy with laminoplasty were excluded. The remaining 29 publications received a full review. Nine of these failed to report data regarding blood loss, surgical time, pain medication use, and postoperative hospital stay. One was excluded because it reported follow-up outcomes on the same cohort. The remaining 19 publications (Fig. 1) were assigned an evidence class based upon the standards established by Matz et al. 13
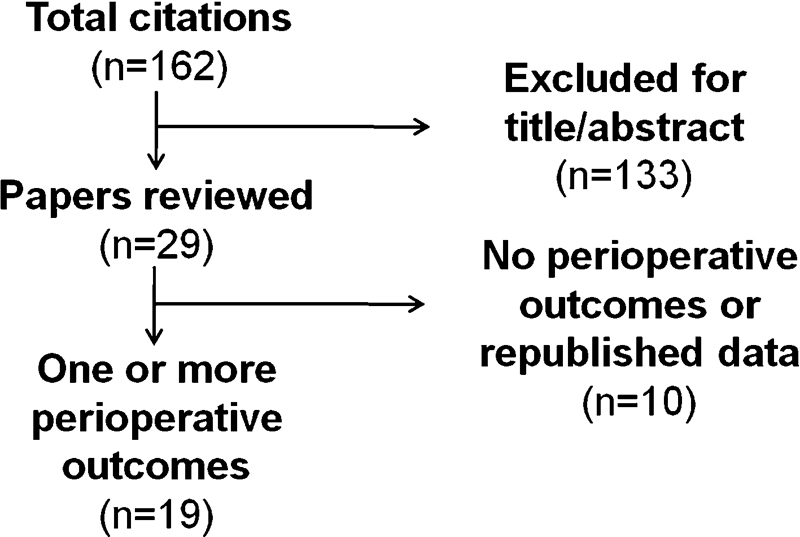
Identification of papers reporting perioperative outcomes.
Literature Results
The following assumptions were made to standardize the data for quantitative comparison. Blood loss that could not be measured (too minimal) was assumed to be 10 mL (two reports). Surgical time was defined to include anesthesia time if that was the only reported outcome (one report). Pain medication use was reported as postoperative pain medication use or postdischarge pain medication use. Only the five publications that reported pain treatments in equivalents were included in the overall analysis of analgesic use. Hospital stay was standardized to patient days. Publications that only reported the day on which patients left were recorded as follows: same day (0.5 patient days), next day (1.0 patient days), second day (2.0 patient days). In the infrequent case that a study only reported a median for any data point, this was estimated to be the mean for the purpose of our analysis. All data were averaged on a per-patient basis rather than a per-study basis.
Results
Summative Results
Of the 18 publications identified, 17 were classified as class III evidence due to lack of an adequate comparison group or substantial limitations in the cohort design. The remaining trial by Kim and Kim 10 was a randomized clinical trial that was classified as class II evidence (as opposed to class I) due to the small number of patients in the study (n = 41). Each publication reported one or more perioperative outcomes related to blood loss (n = 8), surgical time (n = 10), pain medication use (n = 7), and hospital stay (n = 17; Table 2, Table 3). The heterogeneous nature of the reported procedures and outcomes made strict meta-analysis impossible. However, data aggregated from these reports found that patients undergoing percutaneous cervical laminoforaminotomy have lower blood loss by 120.7 mL (open: 173.5 mL, percutaneous: 52.8 mL, n = 670), a shorter surgical time by 50.0 minutes (open: 108.3 minutes, percutaneous: 58.3 minutes, n = 882), less inpatient analgesic use by 25.1 Eq (open: 27.6 Eq, percutaneous: 2.5 Eq, n = 356), and a shorter hospital stay by 2.2 days (open: 3.2 days, percutaneous: 1.0 days, n = 1472), compared with patients undergoing open procedures (Fig. 2).
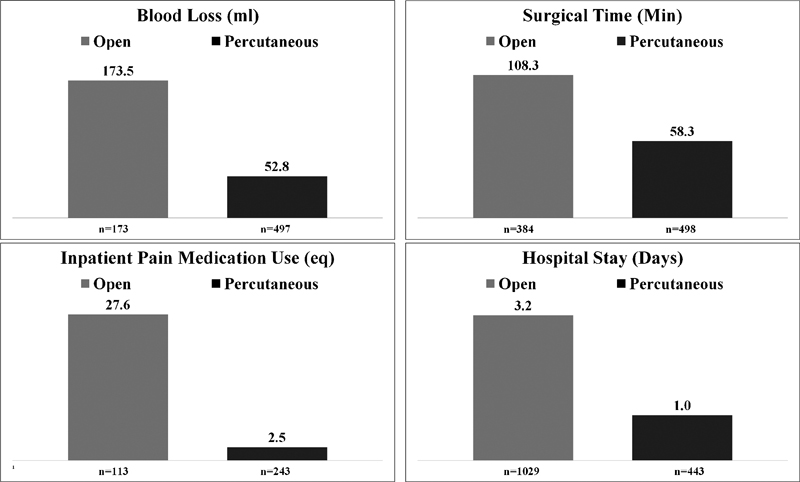
Summative perioperative results.
Publications Reporting Perioperative Outcomes from Open Laminoforaminotomy
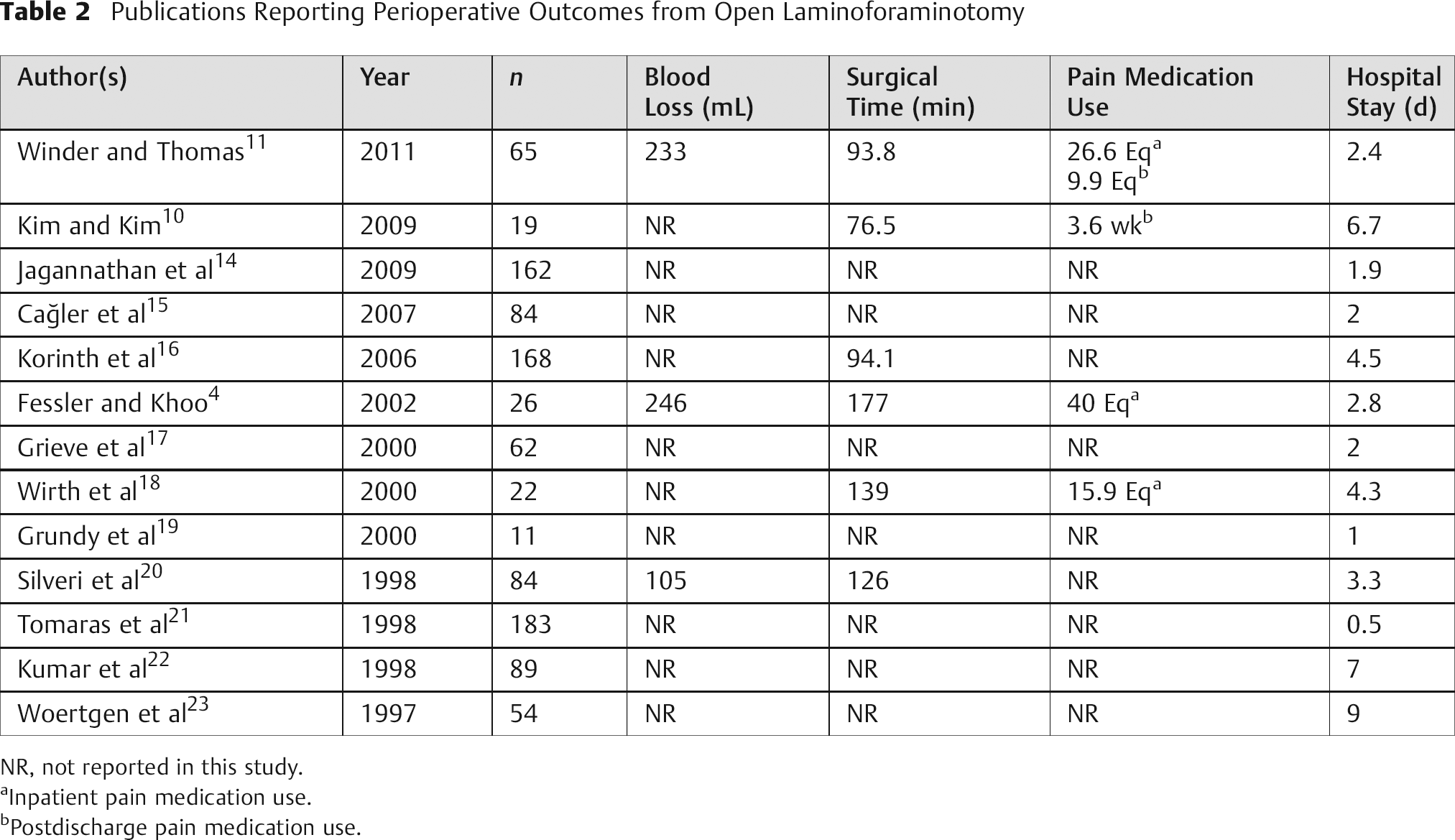
NR, not reported in this study.
Inpatient pain medication use.
Postdischarge pain medication use.
Publications Reporting Perioperative Outcomes from Percutaneous Laminoforaminotomy
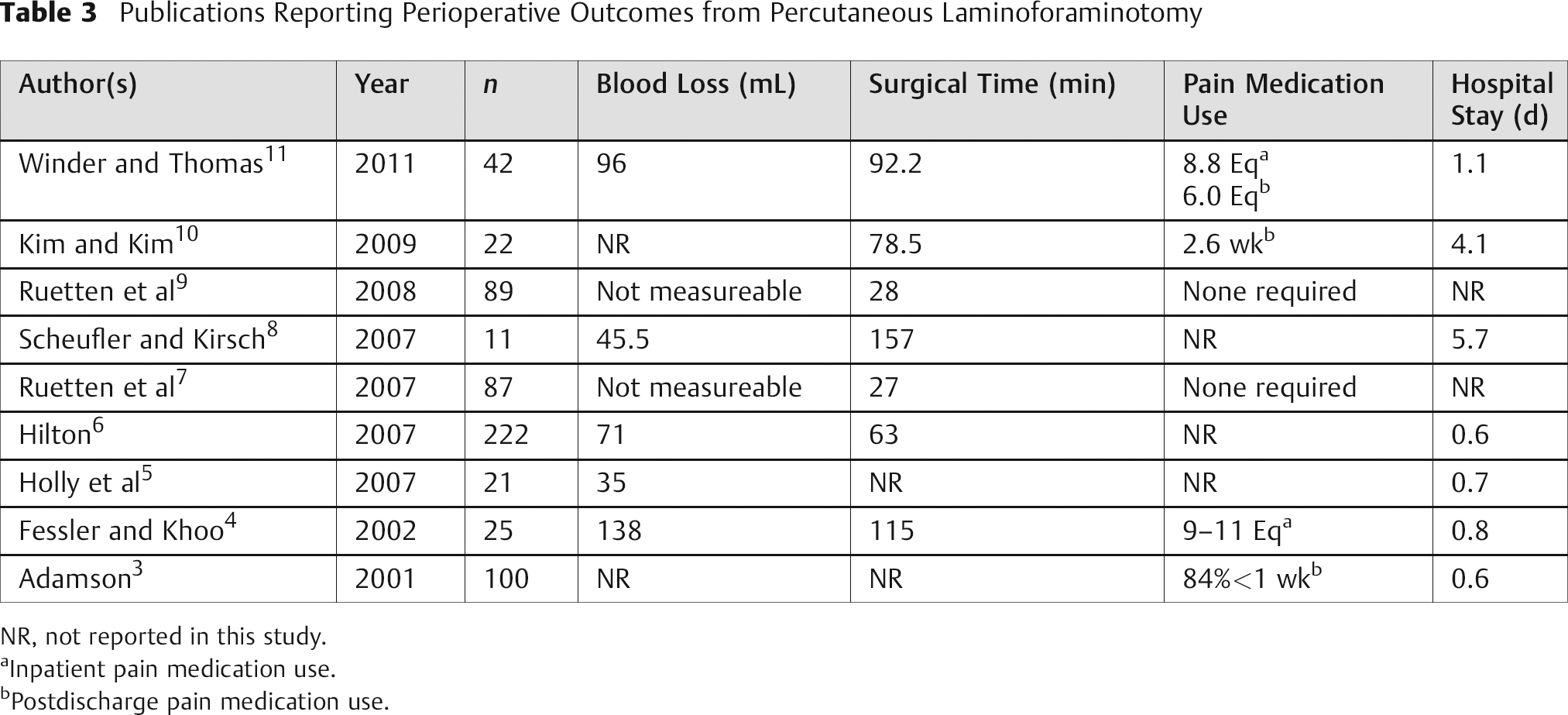
NR, not reported in this study.
Inpatient pain medication use.
Postdischarge pain medication use.
Retrospective and Prospective Cohort Studies Comparing Procedures
Two cohort studies directly compared open and percutaneous cervical laminoforaminotomy. The first, by Fessler and Khoo, 4 was a small prospective cohort study of patients who underwent open (n = 26) or percutaneous (n = 25) laminoforaminotomy by a single surgeon. This study reported that percutaneous cases had lower blood loss by 108 mL (open: 246 mL, percutaneous: 138 mL), a shorter surgical time by 62 minutes (open: 177 minutes, percutaneous: 115 minutes), less analgesic use by 29 to 31 Eq (open: 40 Eq, percutaneous: 9 to 11 Eq), and a shorter hospital stay by 48 hours (open: 68 hours, percutaneous: 20 hours) compared with open controls. The patient was placed in a prone position in all controls and 13 of the cases, and in a sitting position in 12 percutaneous cases. The seated percutaneous cases had notably lower blood loss (27 mL), operative time (90 minutes), and hospital stay (8.1 hours) than the prone percutaneous cases. In addition, the 26 controls underwent decompression at 42 levels, and the 25 percutaneous cases underwent decompression at 33 levels. No significant difference was found in hospital stay among single- and multilevel procedures. Complications included three durotomies, with two leaks and one partial thickness violation.
Winder and Thomas 11 describe retrospective results from a cohort study of 65 open and 42 microscopic tubular-assisted posterior laminoforaminotomies. They reported that percutaneous cases had lower blood loss by 137 mL (open: 233 mL, percutaneous: 96 mL), less recovery room analgesic use by 17.78 Eq (open: 26.57 Eq, percutaneous: 8.79 Eq), less discharge analgesic use by 3.87 Eq (open: 9.88 Eq, percutaneous: 6.01 Eq), and a shorter hospital stay by 31.7 hours (open: 58.6 hours, percutaneous: 26.9 hours) compared with open controls. There was insufficient evidence to conclude that surgical time was different between cases and controls (open: 103.7 minutes, percutaneous: 100.7 minutes). There were seven complications in the open group and three in the percutaneous group with specific complications not reported. In the open group, 3 three-level, 8 two-level, and 11 bilateral procedures were performed compared with 1 three-level, 2 two-level, and 2 bilateral cases in the percutaneous group.
Randomized Trials
Kim and Kim 10 is the only reported randomized clinical trial of open verses percutaneous laminoforaminotomy. Forty-one patients were randomized to open (n = 19) or percutaneous (n = 22) procedures. The percutaneous cases had less postoperative analgesic use by 1 week (open: 3.6 weeks, percutaneous: 2.6 weeks), and a shorter hospital stay by 2.6 days (open: 6.7 days, percutaneous: 4.1 days) compared with open controls. Open surgical time was 76.5 minutes and percutaneous, 78.5 minutes. Blood loss was not reported. However, skin incision size was reported to be smaller in the percutaneous group by 4 mm (open: 3.6 ± 0.4 cm, percutaneous 3.2 ± 0.2 cm, p < 0.05). No complications were reported for any of these surgeries.
Discussion
Posterior laminoforaminotomy is an effective treatment for cervical radiculopathy in appropriately selected patients. These patients typically have radiculopathy due to cervical nerve root compression secondary to spondylosis or lateral displacement of a cervical disk. Due to the growing adoption of percutaneous procedures in the cervical spine, we aimed to identify published benefits and risks associated with percutaneous laminoforaminotomy.
We identified 19 publications that reported perioperative outcomes from open (n = 13) or percutaneous procedures (n = 9). Our analysis identified a total of 1029 open procedures and 619 percutaneous procedures with at least one reported perioperative outcome. To our knowledge, this is the first systematic review of these procedures. Data aggregated from the published literature suggest that blood loss, pain medication use, and hospital stay were reduced in patients who underwent percutaneous rather than open procedures. Surprisingly, surgical time in percutaneous procedures was reported to be shorter than in open procedures. However, it was also clear from our analysis that significant heterogeneity exists within the reported data. Surgical technique, standard hospital procedure, patient selection, and nonstandardized outcome measures all contributed to the variability seen within these outcomes. Although these results accurately report what has been published in the literature, they may not accurately represent the actual outcomes that are seen in everyday practice.
Analysis of a study by Tomaras et al provides insight as to whether perioperative outcomes from open laminoforaminotomy might be similar to outcomes from percutaneous laminoforaminotomy in an appropriately selected patient. 21 In this report, 200 patients underwent open laminoforaminotomy. All patients went home the same day, and the range of incision sizes was reported to be only 1.2 to 3 cm. This incision size would likely be correlated with minimal blood loss, although that outcome was not reported. Postoperative pain medication use would also be relatively low in patients from this study. This theory is supported by Fessler and Khoo's observation that hospitalization time might explain a substantial portion of postoperative pain medication use. 4 Although these hypotheses cannot be generalized to all patients, it is clear that outstanding perioperative outcomes can occur in many open laminoforaminotomy procedures.
In the cohort studies we analyzed, there is a possibility that less complicated patients may have been more likely to undergo percutaneous laminoforaminotomy. One possible measure of complexity is the proportion of patients who undergo multilevel and bilateral procedures. In the cohort study by Winder and Thomas, there are a substantially higher number of multilevel and bilateral procedures in the open cohort compared with the percutaneous cohort. 11 However, their analysis of single-level laminoforaminotomies alone still revealed that patients who underwent the percutaneous procedure had statistically significant improvements in blood loss, analgesic use, and hospital stay compared with patients who underwent single-level open procedures. Time is another potential confounder, as the proportion of patients who underwent open laminoforaminotomies decreased over the 10-year period of the study, introducing the possibility that other changes in surgical and medical practice may have accounted for some of the difference between cohorts. In summary, the retrospective nature of this study makes it unclear whether improved outcomes in percutaneous cases come as a result of surgical technique or some other underlying variable. Fessler and Khoo attempted to control for selection bias by performing open and then percutaneous procedures on consecutive patients. However, their results become even more difficult to interpret due to a major change in operative practice midway through the percutaneous cohort. 4
Of particular importance is the small randomized clinical trial conducted by Kim and Kim. 10 Although this study did not report blood loss, it did report significant decreases in hospital stay and postoperative pain medication use. Surgical time and the proportion of patients receiving single-level laminoforaminotomy were similar in both groups. The only reported differences between the two surgical groups are the percutaneous surgical incision, which is shorter by a statistically significant 4 mm over the 3.6 cm opening made during open procedures, and an acknowledgment that periosteal dissection is more extensive in open procedures. These differences may have some clinical relevance. The more extensive exposure may be the reason open procedure patients remained hospitalized for 2.6 days longer and used analgesics for an additional week compared with the percutaneous group. However, there is still the possibility that some other factors may have contributed to the magnitude of improvement in hospital stay and analgesic use.
Large randomized trials are beneficial to the understanding of expected outcomes among well-selected patients. Investigations of this kind have proven to be valuable in the lumbar spine. In 2010, Teli et al published the results of a randomized controlled trial of microendoscopic, microscopic, and open discectomy in 240 patients. Although most clinical outcome measures were comparable in all three groups, the microendoscopic group had longer surgical time (microendoscopic: 56 minutes, microscopic: 43 minutes, open: 36 minutes) and increased hospital stay (microendoscopic: 54 hours, microscopic: 49 hours, open: 49 hours) compared with the other two groups. 24 Arts et al also performed a randomized controlled trial of 328 patients who underwent open or tubular discectomy. The tubular group had similar blood loss (tubular: 92% < 50 mL, open: 85% < 50 mL), longer surgical time (tubular: 47 minutes, open: 36 minutes), and equivalent hospital stay (3.3 days) compared with the open group. 25 These large-scale clinical trials model how similar studies of both perioperative and long-term outcomes could be done in the cervical spine.
As with all systematic reviews, we are aware that less favorable results in percutaneous or open laminoforaminotomy have not been published. In addition, few of these studies take into account the time it takes a surgeon to learn the endoscopic technique. This learning curve is difficult to account for given the nature of surgical reporting; namely, a surgeon may wait until a technique is mastered before reporting outcomes. Additionally, our analysis has ignored differences in long-term outcomes between open and percutaneous laminoforaminotomy. However, we do note that long-term outcomes were observed to be grossly similar in the limited number of studies (only three) that directly compared open and percutaneous procedures.
In conclusion, the data describing open and percutaneous laminoforaminotomy are very heterogeneous, making it difficult to recommend one procedure over the other. As has taken place in the lumbar spine, it is important that more structured and thorough trials be designed to clarify the risks and benefits associated with each of these procedures.