
Abstract
Study Design
Retrospective, multicenter.
Objectives
This study aims to evaluate the immediate postoperative effect of, and define indications for, an anterior release (discectomy) in large AIS curves utilizing 3D deformity analysis.
Methods
A multicenter registry was queried for AIS patients with main thoracic curves ≥70° treated with either anterior/posterior (AP) or posterior-only surgery and biplanar stereoradiographic pre-operative and first-erect (FE) postoperative images. Standard 2D radiographic and 3D parameters were analyzed using custom MATLAB software. 3D thoracic kyphosis (3DTK) was calculated by removing the error induced by axial rotation and coronal deformity.
Results
109 patients were included, 21 AP and 88 posterior-only. The AP group had larger (89° vs 76°, P < .001), less flexible (9% vs 21%, P = .001) curves, though greater percent correction (79% vs 71%, P = .003), producing similar postoperative curve magnitude (19° vs 22°, P = 0.1). The AP group had less preoperative 3DTK (−15° vs −3°, P < .001), though similar postoperative 3DTK (24° vs 20°, P = .1), nearly double the improvement (39° vs 23°, P < .001). No cases with preoperative 3DTK < −18° achieved postoperative 3DTK >25° without anterior release. Segmental data of each motion segment demonstrated anterior release led to greater change in the coronal (P < .001) and sagittal (P = .003) planes, though not axial rotation of the apical vertebra (P = .157).
Conclusion
In a cohort of AIS patients with thoracic curve magnitude >70°, 3D analysis comparing anterior/posterior vs posterior-only approach demonstrated improved correction in the coronal and sagittal, but not the axial plane. If 3DTK preop was <−18° only anterior release patients achieved postoperative 3DTK >25°.
Level of Evidence
III.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is a complex three-dimensional deformity of the spine involving the coronal, sagittal, and axial planes 1 and characterized by a discrepancy in the anterior vs posterior column lengths of the spine with relative or absolute anterior column lengthening and/or posterior column shortening.1,2 Historically, an anterior release was shown to improve posterior instrumented deformity correction by increasing flexibility, as well as addressing the discrepant anterior and posterior column lengths by shortening the anterior column via discectomy. 3 This may allow for greater reconstitution of kyphosis and additionally serve to increase correction of a “large stiff” deformity in all 3 planes.4,5
With improvements in segmental instrumentation and the adoption of thoracic pedicle screws, affording strong three-column fixation, the trend in AIS treatment has been towards posterior-only surgery.3,6 Authors have demonstrated excellent results with all-posterior approaches even for severe deformities. 7 Subsequently, the use of anterior approaches in the surgical management of AIS has declined. 6 Given the increasing reliance on all-posterior approaches, the modern indications for anterior release in AIS surgery remain poorly defined. Prior literature evaluating the role of anterior surgery with modern posterior instrumentation relies primarily on two-dimensional radiographs and reports conflicting results on the utility of an anterior release. Some report the additional anterior approach leads to no difference in postoperative radiographic parameters. 8 Others demonstrate no difference in coronal correction, but do show increased T5-T12 kyphosis, 9 while others an improvement in both coronal and sagittal plane correction when an anterior release precedes a posterior instrumented fusion. 5
However, evaluating the sagittal and axial planes is particularly difficult on standard two-dimensional radiographs as the axial rotation and coronal deformity prevents obtaining a true lateral view for much of the spine, often underestimating the degree of hypokyphosis in the thoracic spine.10,11 Biplanar stereoradiographic imaging allows for three-dimensional (3D) reconstructions and segmental analysis of each vertebra/motion segment in all 3 planes. This segmental analysis reveals the “true” kyphosis at each vertebral segment, demonstrating significantly more hypokyphosis or even lordotic alignment of the thoracic spine in AIS, which may not be as apparent on standard radiographs. 10 This is especially true for large AIS deformities.
This study aims to evaluate the effect of an anterior approach (thoracic discectomies) on the immediate 3D deformity correction in large main thoracic AIS curves to help establish modern indications for an anterior release. This study is unique in utilizing biplanar radiographs to perform 3D segmental analysis. We hypothesize that anterior release in larger AIS curves improves the intra-operative 3D correction following posterior instrumentation with greater correction of the coronal curve, axial rotation, and restoration of thoracic kyphosis.
Methods
A multicenter registry was queried for AIS patients with main thoracic curves ≥70° treated with either anterior/posterior (AP) or posterior-only (P) surgery. Written informed consent was obtained from all patients for inclusion into the study. This study was approved by the UC San Diego Institutional Review Board (protocol 150406) on January 03, 2021. All patients had biplanar stereoradiographic preoperative and first erect (FE) postoperative (∼4-6 weeks) images. Since we were interested in the effect of anterior release on immediate 3D correction, we chose to evaluate the comparison of preoperative to early postoperative radiographs. Standard two-dimensional (2D) radiographic and three-dimensional (3D) radiographic parameters were compared. Custom MATLAB software was used to evaluate the segmental measures of deformity in “local” reference planes of the vertebrae. 3D “true” thoracic kyphosis (3DTK) was calculated with the summed segmental (T5-T12) method (removing the error induced by axial rotation and coronal deformity) (Figure 1). Apical axial rotation was measured as the rotation of the apical vertebra relative to the pelvis pre-operatively and post-operatively.
10
3D reconstructions of the lateral image of the same patient. (A) 3D reconstructed lateral images in the standard lateral reference frame with segmental and regional thoracic kyphosis measures. (B) Manipulated 3D reconstructed lateral view with the vertebral rotated in the neutral sagittal plane with the segmental and regional thoracic kyphosis measurements revealing the significant hypokyphosis of the thoracic spine. Image re-printed with permission “Newton PO, Fujimori T, Doan J, Reighard FG, Bastrom TP, Misaghi A. Defining the “Three-Dimensional Sagittal Plane” in Thoracic Adolescent Idiopathic Scoliosis. (J) Bone Joint Surg Am. Oct 21 2015;97(20):1694-701. doi:10.2106/JBJS.O.00148.”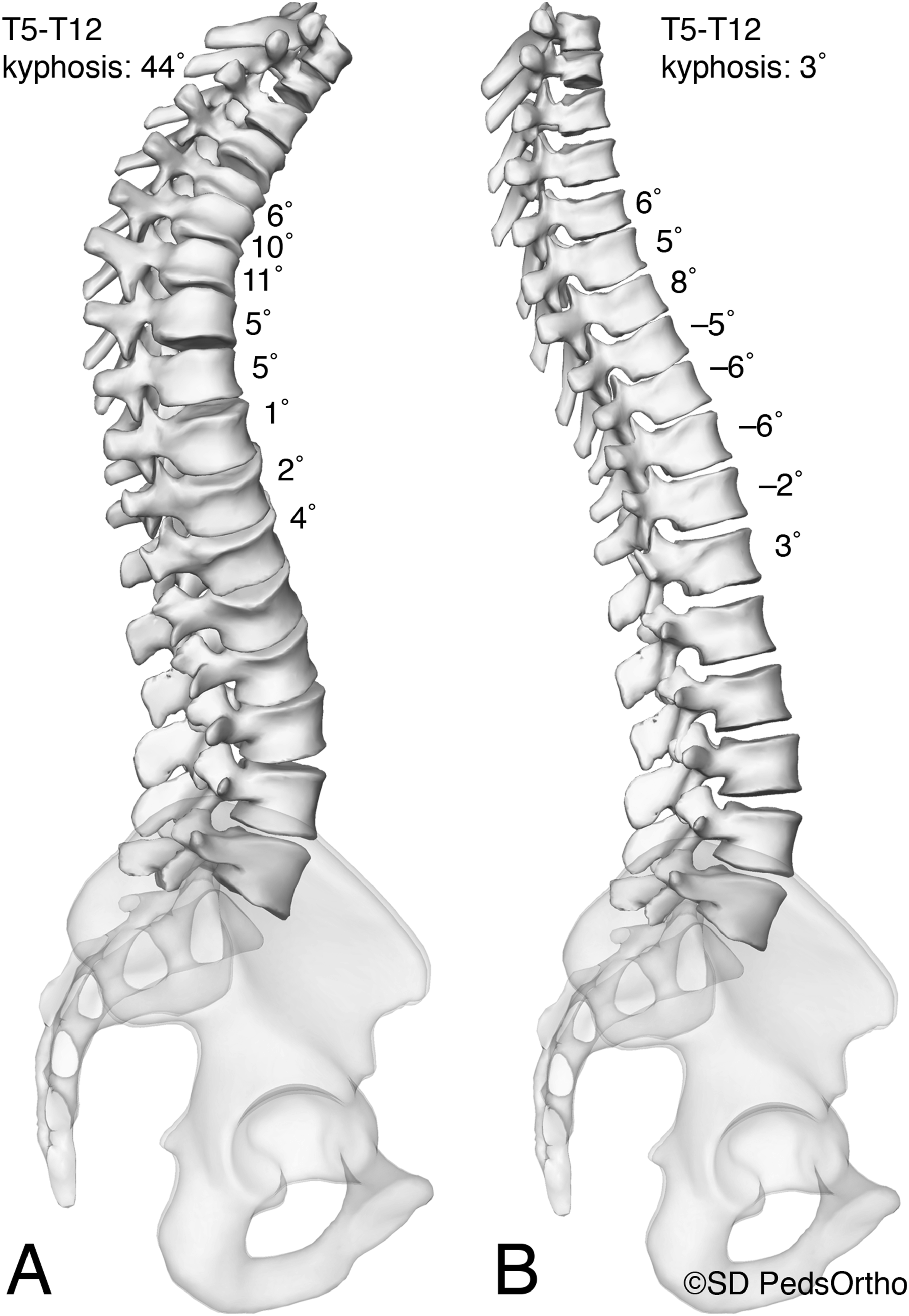
Radiographic Analysis
Radiographs were obtained at the pre-operative and FE time points (Figure 2). All patients had simultaneous, biplanar, slot scanning posteroanterior and lateral full-length scoliosis radiographs obtained with an EOS imaging system with 3D reconstructions created using sterEOS software (Alphatec Spine, Carlsbad, CA). Custom MATLAB (MathWorks, Natick, Massachusetts, USA) software script was used to quantify the 3D vertebral body morphology from the spine reconstructions to perform the 3D segmental radiographic analysis.
10
(A) 15-year-old female AIS patient treated with anterior/posterior spinal fusion. (A) Pre-operative PA radiograph and (B) lateral radiographs. (C) First erect post-operative PA radiograph (D) and lateral radiograph.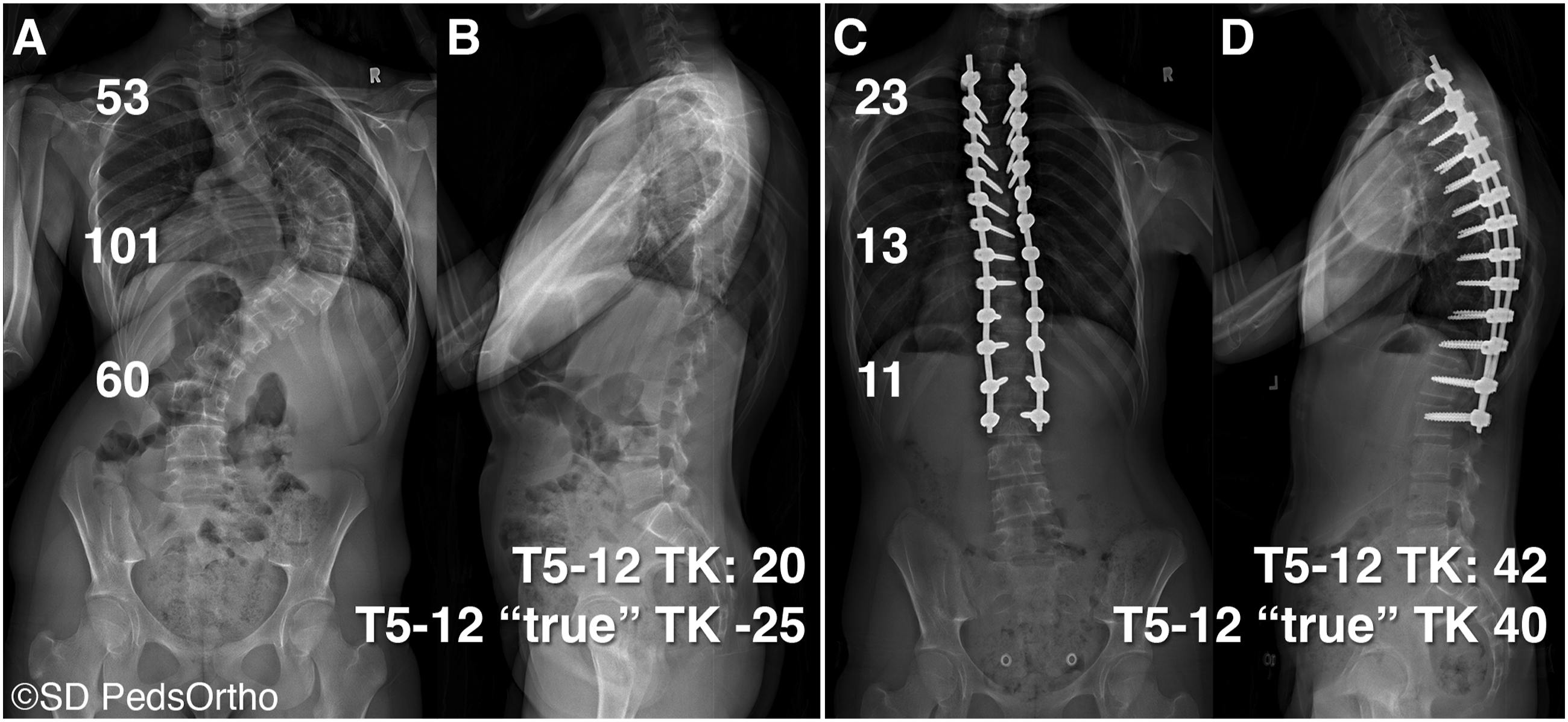
Statistics
Standard descriptive summary statistics (eg, means and standard deviations for continuous variables such as age and percentage for categorical variables such as gender) were used to summarize demographic variables. Comparisons of categorical variables between subgroups were made using the Chi-square test or the Fisher’s exact test for cases when expected values were less than 5. Comparisons of continuous variables were completed using independent t-tests. Pre-operative and post-operative data were compared using paired t-tests. Alpha was set at P < .05 to declare significance.
In the segmental analysis each motion segment was analyzed as unique subjects to compare levels with no release, posterior column osteotomy (PCO), or anterior release with PCO. Segmental analysis performed with generalized linear mixed models (GLMM) were used to analyze the effect of release type on spine deformity correction with subjects as a random factor and level as repeated factor (utilizing the calculated change between pre-operative and first erect measures). Thresholds for anterior release were guided via classification and regression tree (CART) analysis with 10-fold cross validation. A threshold of 25 degrees of kyphosis was determined as acceptable minimum thoracic kyphosis and used as the primary outcome of the CART based upon data on mean thoracic kyphosis in AIS patients12,13 and prior literature defining this as an acceptable outcome in AIS surgery. 3 Statistical analysis was completed using BlueSky® statistical software (Commercial Server Version 7.10, BlueSky Statistics LLC, Chicago, IL, 2021). GLMM and CART analysis were performed with SPSS v28 (IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp).
Results
Baseline Patient Demographic Characteristics.
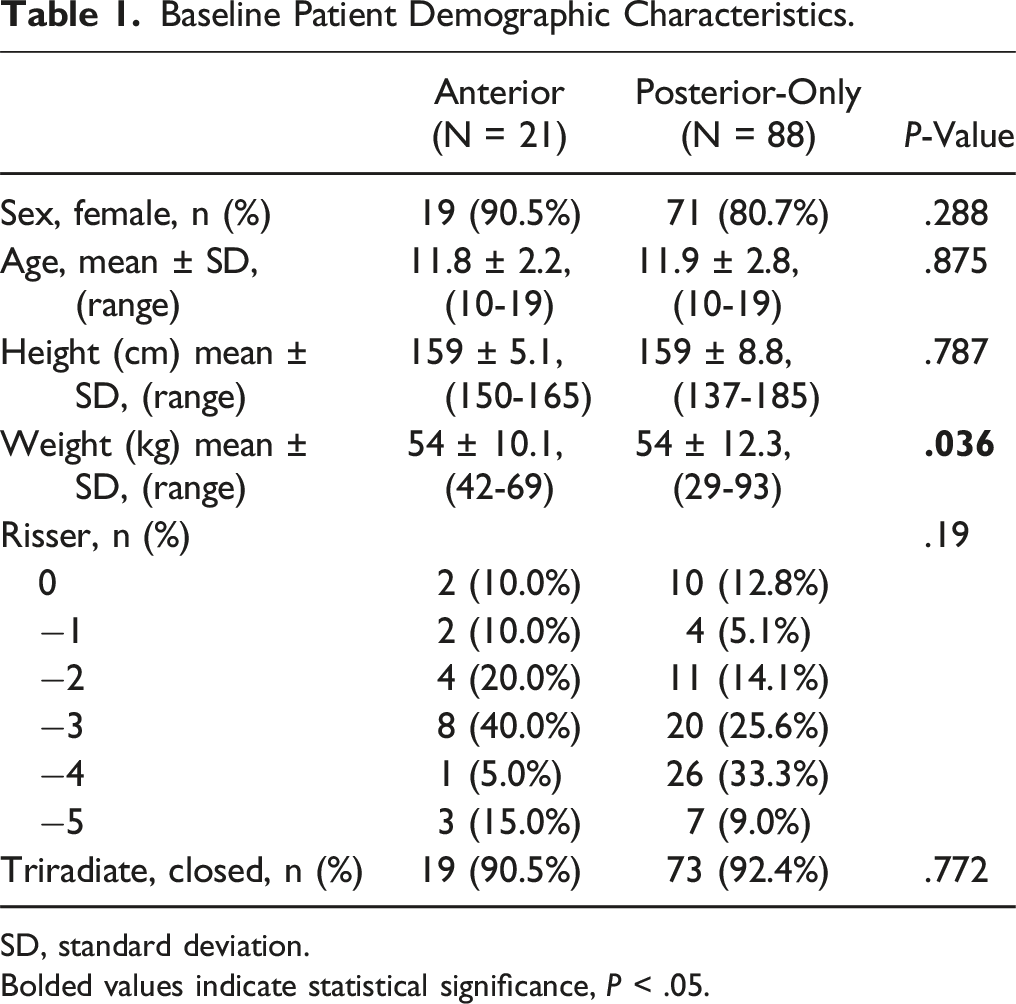
SD, standard deviation.
Bolded values indicate statistical significance, P < .05.
Comparison of Perioperative Patient Outcomes.
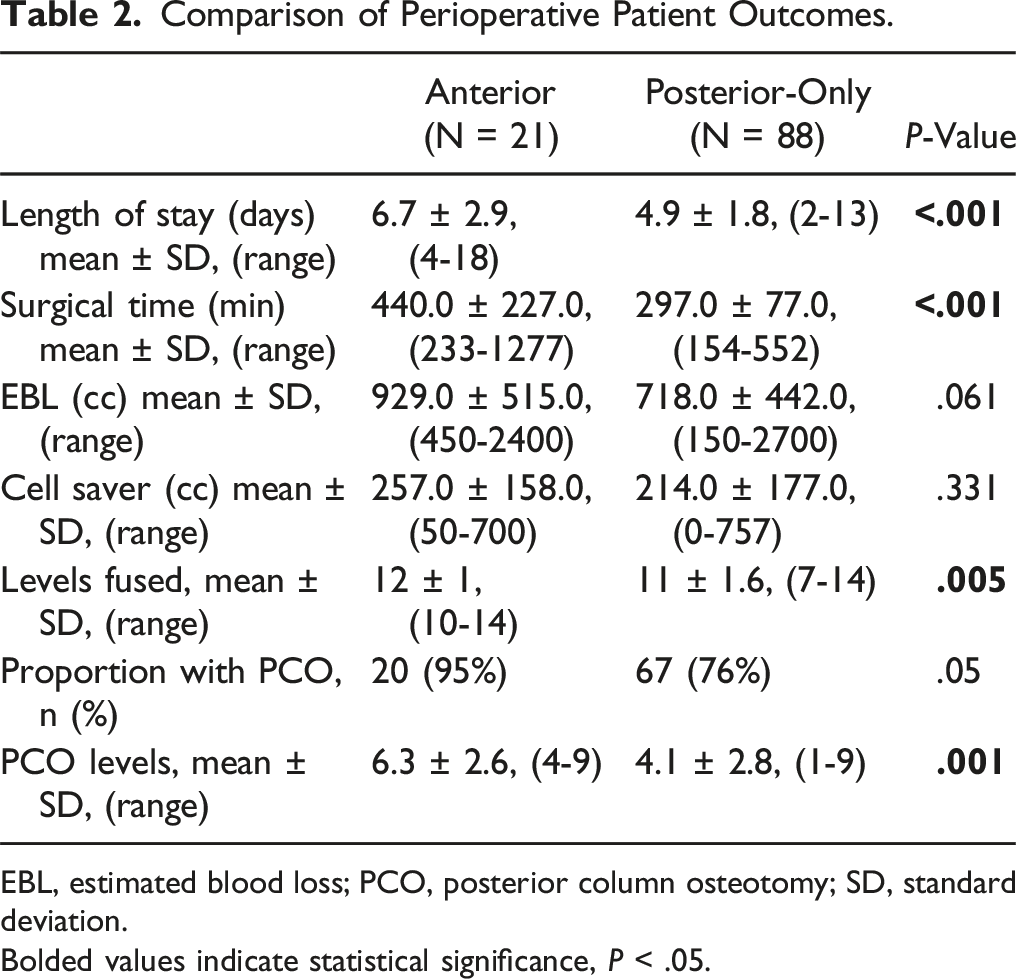
EBL, estimated blood loss; PCO, posterior column osteotomy; SD, standard deviation.
Bolded values indicate statistical significance, P < .05.
Pre-Operative and First Erect (FE) Post-Operative Radiographic Outcomes.
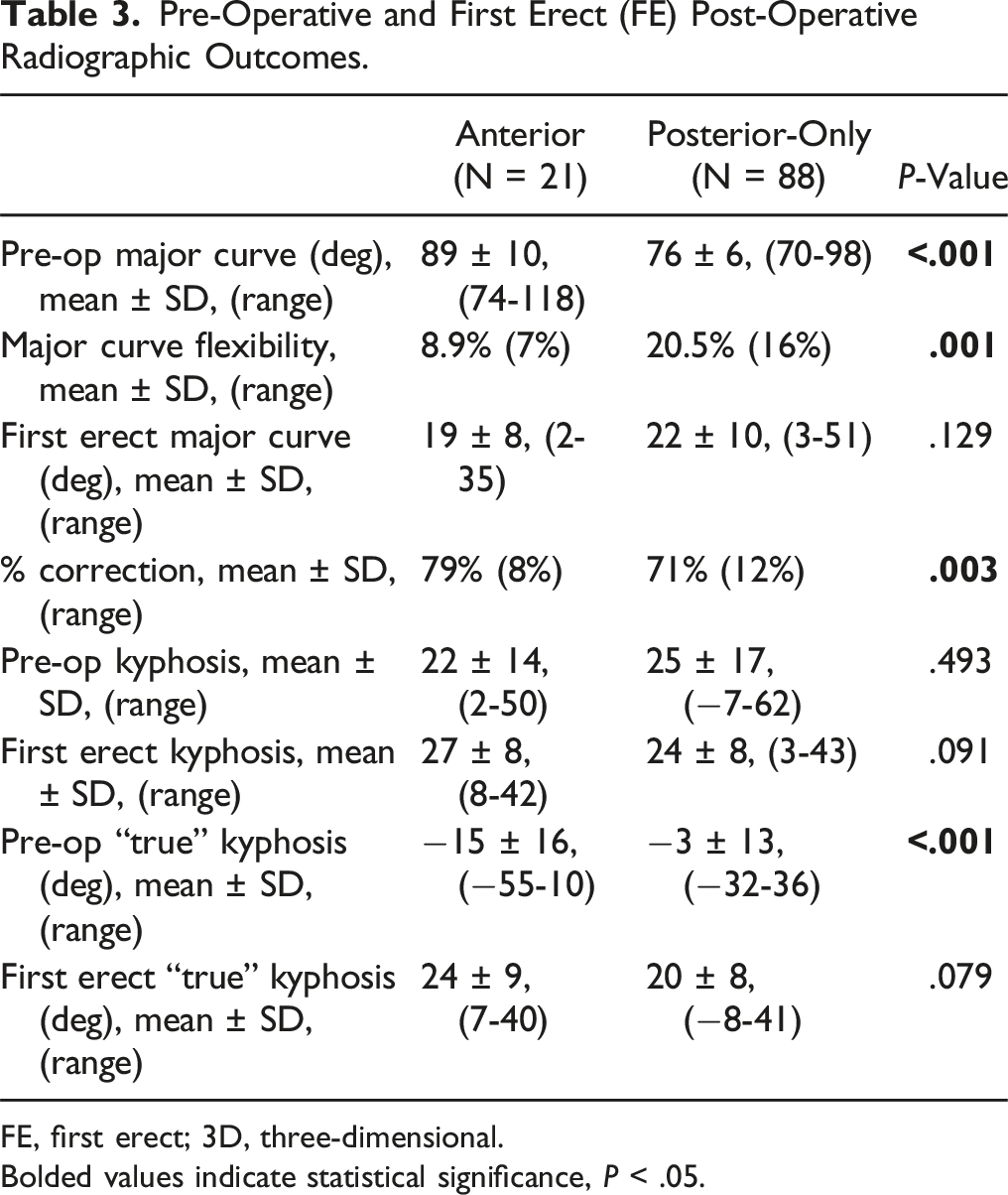
FE, first erect; 3D, three-dimensional.
Bolded values indicate statistical significance, P < .05.
Three-Dimensional, Segmental Radiographic Analysis Comparing by Type of Release.
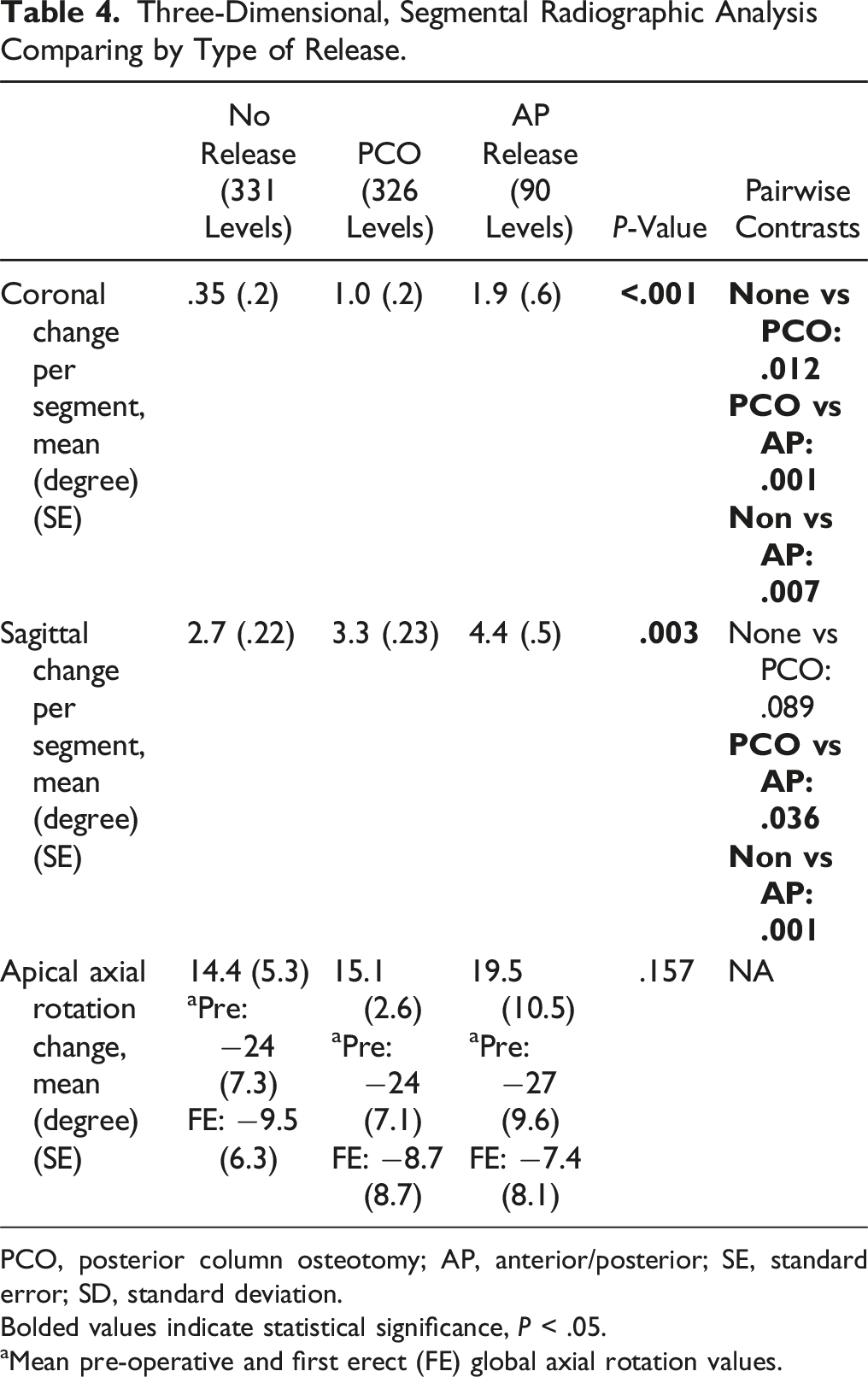
PCO, posterior column osteotomy; AP, anterior/posterior; SE, standard error; SD, standard deviation.
Bolded values indicate statistical significance, P < .05.
aMean pre-operative and first erect (FE) global axial rotation values.
According to the CART analysis, our data suggested little benefit to an AP approach in achieving the target postoperative thoracic kyphosis of >25° if the pre-operative 3D kyphosis was >7°. While in contrast, no cases with pre-operative 3DTK of more than 18° of lordosis had a postoperative 3DTK value >25° without the use of an anterior release. For a preoperative 3DTK of between −18° and 7°, achieving the postoperative kyphosis goal was variable (Figure 3). Scatterplot of pre- and postoperative 3D kyphosis with indications for anterior release. Thresholds determined via classification and regression tree (CART) analysis.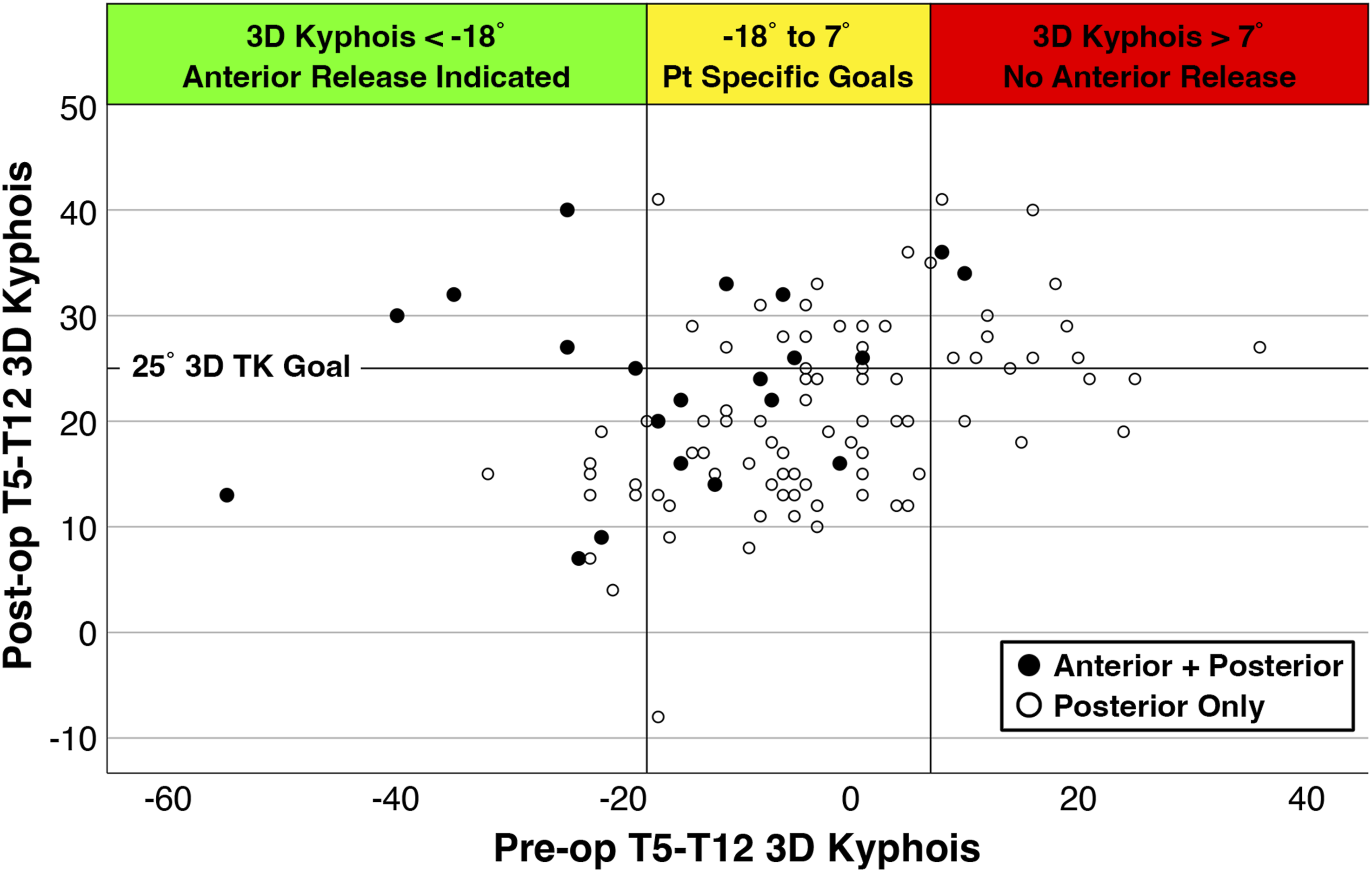
Discussion
Currently, the prevailing technique for the surgical management of AIS has become a posterior-only approach and anterior release is typically reserved for “severe or stiff” deformities. 5 However, the specific indications remain ill defined. Modern indications for anterior approaches are reported in the literature with conflicting conclusions.5,8,9 The present study shows anterior release can provide improved coronal and 3D sagittal correction in a select patient subpopulation of thoracic curves >70° that are also frankly lordotic more than 18° (as measured by the 3D summed segmental method). Additionally, we provide evidence for when an anterior release can be avoided; the posterior only approach in patients with >70° thoracic curves with 3DTK >7° provided no advantage in achieving sagittal thoracic kyphosis correction to >25°.
As AIS is characterized by relative vs absolute anterior overgrowth associated with axial rotation and coronal displacement of the vertebrae,2,14 by not adequately addressing the anterior column, posterior-only approaches have been associated with residual thoracic hypokyphosis particularly in the era of powerful axial correction methods such as direct vertebral derotation/manipulation with segmental pedicle screws.15-17 The present study did not demonstrate a difference in apical vertebra axial plane correction between the methods of release (anterior/posterior vs posterior-only), although the study may be underpowered for this particular comparison. This may suggest it is “easier” to correct the axial plane, but at the expense of under correction of the sagittal plane if anterior column shortening is not achieved in patients who are more severely lordotic preoperatively. Under correction of thoracic kyphosis may affect the global alignment of the spine, as persistent thoracic hypokyphosis has been shown to be associated with reduced lumbar lordosis, which may further contribute to positive sagittal imbalance as the patient ages. 16
As Newton et al. demonstrated, virtual axial de-rotation and coronal correction of the spine utilizing 3D modeling uncovers hypokyphosis in the regions of scoliosis that is generally proportional to the magnitude of the scoliosis, and in more severe cases of scoliosis, there may be frank lordosis of the thoracic spine. 10 Axial plane rotation deformity is also present largely in proportion to the coronal deformity. Understanding of these concepts helps to illustrate how the 3 planes of deformity “compete” against each other during spinal deformity correction maneuvers. One study compared AIS patients categorized as either “high coronal correction” or “low coronal correction.” 17 Patients with maximal coronal plane deformity correction were found at 2 years to have significantly worse sagittal correction with more residual hypokyphosis. 17 While the high correction group may have had less post-operative major curve magnitude and less rib rotation, there was a loss in post-operative kyphosis of 3°. The low correction group had less correction of the curve magnitude, and more residual rib rotation, but notably had 8° increase in thoracic kyphosis. 17 This finding was in the early pedicle screw era and the finding may have been even more strikingly different had that analysis been done in 3D. Greater understanding of the true sagittal deformity has enabled more focused attention to the sagittal correction of AIS of late.
Our study demonstrates the ability of anterior release to significantly improve 3D deformity correction in a select AIS patient population. The coronal plane correction was marginally but statistically improved with percent correction 79% in those with an anterior release vs 71% in those treated posterior only. In addition, an anterior release allows one to shorten the anterior column, and in doing so, both de-rotate the spine and simultaneously restore thoracic kyphosis. Despite significantly larger, stiffer, and more hypokyphotic (“true” kyphosis) preoperative curves in the AP group compared to the posterior-only cohort, the 3D “true kyphosis” correction was significantly greater in the AP group with nearly twice the change from preoperative to postoperative time points (AP: 39° increase in 3DTK (−15° to 24°) vs P: 23° increase in 3DTK (−3° to 20°)). Additionally, this sagittal correction did not come at the expense of axial plane apical correction as there was no statistically significant difference with the AP group improving by 19.5° compared 15.1° for the posterior only group. This is particularly notable given changing the axial and sagittal planes are directly competing objectives and further establishes the efficacy of an anterior approach to allow for axial de-rotation without sacrificing correction in the sagittal plane and vice versa.
Additional support to the concept that anterior release allows greater correction was also provided from the 3D analysis of each individual motion segment in which we could compare the effect on coronal and sagittal motion changes after surgery, based on whether an anterior/posterior combined release, a posterior column only release or neither was performed. The findings, also based on 3D local plane analysis, demonstrated significant increases in correction of the coronal and sagittal planes when an anterior release was included in the surgical correction. Although the differences between and AP and P alone surgery are on average ∼1° per level in each plane, these differences vary and sum over numerous levels to result in the overall 3D correction of the procedure.
However, an anterior approach is not warranted in all cases, as an anterior approach does represent a more invasive surgery. Not surprisingly, the anterior approach patients had both longer hospital stays (6.7 vs 4.9 days, P < .001) and surgical times (440 vs 297 min, P < .001). Any difference in EBL that may exist did not reach statistical significance (929 vs 718 mL, P = .061), although the relatively limited number of AP patients may limit the statistical power. It stands to reason that an additional anterior approach would be a greater surgical insult, though the long-term effects were not within the scope of the present study and have been evaluated previously.18,19 While our study aimed to limit the patient population to more severe curves, there are still cases in our sample in which an anterior approach may not have been necessary based on our CART analysis. For the most severe sagittal deformities, with 3D thoracic kyphosis less than −18° (>18° of lordosis), an anterior approach appears to be necessary if restoration of kyphosis to more than 25° is the goal of the operation. The 25° threshold represents the minimum normal thoracic kyphosis and a goal greater than this may be appropriate for patients with a pelvic incidence in the upper end of the normal range. Similarly, patients with a 3DTK >7° did not routinely require an anterior approach to reach the kyphosis goal of 25o (Figure 3). In all cases the surgeon should determine some postoperative thoracic kyphosis target based on the preoperative assessment of global sagittal alignment which may include pelvic incidence as well as lumbar and thoracic pelvic angles. 20 The magnitude of the difference between the preoperative 3DTK and the postoperative target TK should help inform the decision regarding the benefit or lack thereof, in performing an anterior release in achieving the desired sagittal plane (and to a lesser extent the coronal plane) result.
Limitations of our study include the sample size, particularly in the AP cohort. Despite the sample size of 21 in the AP group, significant effects of anterior release were identified in several domains, suggesting a substantial effect size. Additionally, differences in surgical technique certainly exist both for the anterior (open vs thoracoscopic, extent of discectomy, etc.) and posterior (eg, adjunctive measures such as in-situ bending, variable de-rotation techniques, screw type or rod materials) procedures. All surgical decision making was at the discretion of the treating surgeon and thus surgeon preference (approach bias) and patient specific goals have contributed to variable patient selection regarding the procedures. We attempted to match the groups based on inclusion criteria of thoracic curve magnitude >70°, however, even in doing so the AP group had a larger preoperative coronal and 3D sagittal deformity. The inclusion of patients in the posterior-only group without any osteotomies may have confounded the results as many authors have argued for the use of PCOs to improve sagittal correction. However, in the 3D segmental analysis we were able to evaluate each motion segment individually and account for the type of release performed at each level and control for the use of PCOs. Table 4 demonstrates that there was no significant difference in sagittal change per segment between the levels with or without a PCO. Although, an anterior release had greater sagittal correction compared to no PCO or PCO alone. The primary objective of the study was to evaluate the immediate efficacy of anterior release on 3D spine deformity correction. As such we did not evaluate functional outcomes or address the durability of the correction as the radiographic outcomes at 2 years or greater were beyond the scope of our analysis, though it is an important question that should be addressed in future research. Additionally, while the “true” 3D thoracic kyphosis is a critical concept to understand the 3D spinal deformity, it is still not routinely integrated into clinical practice as it does require biplanar radiographs and specialized software to acquire this data.
Conclusion
In a cohort of thoracic AIS patients with a preoperative thoracic curve magnitude of >70° a 3D analysis comparing anterior release combined with posterior column osteotomies and instrumentation vs an isolated posterior only approach we found advantages to correction in the coronal and sagittal plane, but not the axial plane when an anterior release was included. Despite the anterior group tending to have larger, stiffer, more lordotic thoracic curves there was greater percentage coronal plane correction (79% vs 71%) and greater absolute change in 3DTK (1.7 times) when an anterior release was combined with posterior instrumentation that included PCOs compared to a similar posterior only approach. An anterior approach may be most advantageous in certain AIS patients with curves >70° and hypokyphosis, as measured by 3D thoracic kyphosis method, that is more than 18° of thoracic lordosis. In such cases a posterior only approach never achieved a postoperative thoracic kyphosis of >25° in our series.
Footnotes
Author Contributions
Conception or design of the work; or Acquisition, analysis, or interpretation of data for the work: Taylor J. Jackson, MD, Carrie E. Bartley, MA, Tracey P. Bryan, MA, Michael P. Kelly, MD, Suken A. Shah, MD, Stefan Parent, MD, PhD, Firoz Miyanji, MD, Harms Study Group and Peter O. Newton, MD. Drafting or critically revising the work: Taylor J. Jackson, MD, Carrie E. Bartley, MA, Tracey P. Bryan, MA, Michael P. Kelly, MD, Suken A. Shah, MD, Stefan Parent, MD, PhD, Firoz Miyanji, MD, Harms Study Group and Peter O. Newton, MD. Final approval of the version to be published: Taylor J. Jackson, MD, Carrie E. Bartley, MA, Tracey P. Bryan, MA, Michael P. Kelly, MD, Suken A. Shah, MD, Stefan Parent, MD, PhD, Firoz Miyanji, MD, Harms Study Group and Peter O. Newton, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grants to the Setting Scoliosis Straight Foundation in support of Harms Study Group research from DePuy Synthes Spine, EOS imaging, Stryker Spine, Medtronic, NuVasive, Zimmer Biomet and the Food and Drug Administration.
Harms Study Group Investigators
Aaron Buckland, MD; New York University. Ahmet Alanay, MD; Acibadem Maslak Hospital, Turkey. Amer Samdani, MD; Shriners Hospitals for Children—Philadelphia. Amit Jain, MD; Johns Hopkins Hospital. Baron Lonner, MD; Mount Sinai Hospital. Benjamin Roye, MD; Columbia University. Bob Cho, MD; Shriners Hospitals for Children, Pasadena, CA. Burt Yaszay, MD; Seattle Children’s Hospital. Caglar Yilgor, MD; Acibadem Maslak Hospital, Turkey. Chris Reilly, MD; BC Children’s Hospital. Dan Hoernschmeyer, MD; University of Missouri Health Care. Daniel Hedequist, MD; Boston Children’s Hospital. Daniel Sucato, MD; Texas Scottish Rite Hospital. David Clements, MD; Cooper Bone & Joint Institute New Jersey. Firoz Miyanji, MD; BC Children’s Hospital. Harry Shufflebarger, MD; Paley Orthopedic & Spine Institute. Jack Flynn, MD; Children’s Hospital of Philadelphia. Jean Marc Mac Thiong, MD; CHU Sainte-Justine, John Asghar, MD; Paley Orthopedic & Spine Institute. Josh Murphy, MD; Children’s Healthcare of Atlanta. Joshua Pahys, MD; Shriners Hospitals for Children—Philadelphia. Juergen Harms, MD; Klinikum Karlsbad-Langensteinbach, Karlsbad. Keith Bachmann, MD; University of Virginia. Kevin Neal, MD; Nemours Children’s Clinic, Jacksonville. Laurel Blakemore, MD; Pediatric Specialists of Virginia. Lawrence Haber, MD; Ochsner health center for children New Orleans. Lawrence Lenke, MD; Columbia University. Lori Karol, MD; Children’s Hospital, Denver Colorado. Mark Abel, MD; University of Virginia. Mark Erickson, MD; Children’s Hospital, Denver Colorado. Michael Glotzbecker, MD; Rainbow Children’s Hospital, Cleveland. Michael Kelly, MD; Washington University. Michael Vitale, MD; Columbia University. Michelle Marks, PT, MA; Setting Scoliosis Straight Foundation. Munish Gupta, MD; Washington University. Nicholas Fletcher, MD; Emory University. Noelle Larson, MD; Mayo Clinic Rochester Minnesota. Patrick Cahill, MD; Children’s Hospital of Philadelphia. Paul Sponseller, MD; Johns Hopkins Hospital. Peter Gabos, MD: Nemours/Alfred I. duPont Hospital for Children. Peter Newton, MD; Rady Children’s Hospital. Peter Sturm, MD; Cincinnati Children’s Hospital. Randal Betz, MD; Institute for Spine & Scoliosis. Stefan Parent, MD, PhD: CHU Sainte-Justine. Stephen George, MD; Nicklaus Children’s Hospital. Steven Hwang, MD; Shriners Hospitals for Children—Philadelphia. Suken A. Shah, MD; Nemours/Alfred I. duPont Hospital for Children. Sumeet Garg, MD; Children’s Hospital, Denver Colorado. Tom Errico, MD; Nicklaus Children’s Hospital. Vidyadhar Upasani, MD; Rady Children’s Hospital.