
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To assess how the thoracic kyphosis affects the ability of the fulcrum bending radiograph (FBR) to predict the coronal thoracic curve correction.
Methods:
A retrospective study of prospectively collected data was conducted of 107 consecutive patients with thoracic adolescent idiopathic scoliosis (AIS) treated with a standard screw-fixation protocol. Radiographic variables were assessed preoperatively and at 2-year follow-up. Curve flexibility was determined based on the FBR and the Fulcrum Bending Flexibility Index (FBCI). Radiographic variables included preoperative Cobb angle, T5-T12 kyphosis, T12-S1 lordosis, sagittal vertical axis, list, T1-T12 length, truncal shift, and radiographic shoulder height. Patients were also categorized as hypo-, normo-, or hyperkyphotic.
Results:
Based on multivariate modeling, an increase in FBR Cobb angle and thoracic kyphosis were significantly associated with an increase in FBCI (increased mismatch between the FBR and postoperative Cobb angles) at 2-year follow-up (P < 0.001). In patients with hyperkyphosis, a longer instrumented length existed despite similar curve size and shorter curve length than the hypo- and normokyphotic groups. Based on these findings, we developed a new predictive postoperative curve correction index, known as the Multiprofile Flexibility Index (MFI).
Conclusions:
Our results show that an increase in preoperative thoracic kyphosis is associated with an increased difference between the preoperative coronal curve flexibility and the postoperative coronal curve correction. Our findings broaden the understanding of curve flexibility and indicate that selection of fusion levels may need to take into consideration the sagittal profile to improve clinical decision making and optimize outcome.
Keywords
Introduction
Surgical management of adolescent idiopathic scoliosis (AIS) should aim to achieve a sustained coronal curve correction while maintaining a balanced spine. AIS has long been recognized as more than a 2-dimensional deformity and the surgical coronal curve correction appears to be associated with the preoperative sagittal profile as studies show that failure to restore normal postoperative thoracic kyphosis may be due to stiffness of the spine in the coronal plane. 1 Additionally, several studies have shown that curve correction is better in hypokyphotic patients. 1,2 Thoracic kyphosis ranges are between 20° and 33° in normal subjects 3 but AIS is characterized by a broader range of kyphosis and often hypokyphosis is seen. 4
Assessment of curve flexibility is essential in preoperative planning as it provides information about the extent of structural change, selection of fusion levels, screw strategy, the amount of correction that can be safely achieved, and whether fusion of the secondary curve is indicated. 5,6 Flexibility is traditionally understood as a 2-dimensional parameter that solely addresses the potential curve correction in the coronal plane. However, Luk et al 7 showed that a coupled mechanism exists between coronal curve correction on FBR and sagittal “self-normalization” of the thoracic kyphosis. However, this coupling mechanism is not yet fully understood and whether the sagittal profile of the curve may affect the flexibility has not been examined. Most centers use the bending radiograph primarily to decide which curves to include in the fusion and to identify patients that may require osteotomies. The specific fusion selection is often based on the standing AP radiograph with the lower end of the instrumentation typically at the “stable minus one” vertebra in Lenke type 1 and 2 curves. 8 Curve flexibility ranges substantially between patients and choosing the fusion level without addressing the flexibility can result in a longer fusion resulting with higher operative costs and risk of complications. 9,10
Flexibility can be visualized through various techniques, whereby the most commonly accepted are lateral bending, traction, push-prone or fulcrum bending radiographs (FBRs). The FBR has shown to be the most predictive with regard to thoracic AIS. 11 The FBR has shown a strong positive correlation with the surgical curve correction in thoracic curves for both hook and all-pedicle screw constructs. 9,10 In a recent Delphi Survey by the AOSpine Knowledge Forum on deformity, 75% of participants worldwide noted the FBR to be a well-accepted technique used in clinical practice to assess curve flexibility. 12
The Fulcrum Bending Flexibility Index (FBCI) was developed as an alternative to the traditional curve correction index to better assess curve correction based on the preoperative curve flexibility. The FBCI, has shown good correlation with the fulcrum flexibility 6,13 but studies show that FBCI ranged from 75% to 208%, thereby indicating that, in some cases, the surgical curve correction substantially exceeded the correction predicted by the FBR. 9 There are clearly factors affecting the predictability of the FBR; however, the nature of these factors remains largely unknown. A reduced deformity correction results in poor patient-reported outcomes in terms of reduced self-image and dissatisfaction with treatment. 14,15 As such, it is of value to know the potential for correction prior to surgery to be able to differentiate the surgical treatment and to manage patient expectations prior to surgery with involvement of families in the clinical decision-making process.
The objective of the study was 2-fold: (1) to assess how the thoracic kyphosis affects the ability of the FBR to predict the coronal thoracic curve correction and (2) to introduce a novel prediction index for postoperative curve correction.
Materials and Methods
Following approval by The University of Hong Kong and Queen Mary Hospital Institutional Review Board, a prospective radiographic study was conducted. Written informed consent was obtained from all patients. We included consecutive patients surgically treated for Lenke type 1, 2, or 3 AIS 5 between January 2006 and December 2010 at a single institution. All patients underwent single stage posterior fusion with alternate-level pedicle screw instrumentation. 16
Assessment of curve flexibility was based on the FBR, which has been previously described. 11 In short, each patient was positioned in the lateral decubitus position. A padded bolster (fulcrum) was placed on the convex side of the curve at the level of the rib corresponding to the apex of the curve. The fulcrum was positioned so that the shoulder and the pelvis were lifted off the table.
Selection of fusion levels was based on the protocol reported by Luk et al. 6 In short, a line was drawn parallel to the inferior endplate of the estimated distal instrumented vertebra (DIV). From the line above the center of the DIV, a perpendicular line was drawn, termed the center line (CL). After the estimated proximal instrumented vertebra (PIV) was identified, a line is drawn parallel to the superior endplate. The Cobb angle was determined based on DIV and PIV. If the shift from the PIV was greater than 20 mm from the CL, the next caudal vertebra was chosen as the DIV. If the shift was less than 20 mm but the Cobb angle was greater than 20°, then the next cranial vertebra was chosen as the estimated PIV. All patients were operated using an alternate-level screw strategy by 1 of 3 surgeons all with more than 15 years of experience. The inferior articular process was removed to locate the pedicle screw entry point in the thoracic spine. No Ponte osteotomy or direct vertebral rotation was performed for any case. Intraoperative correction is standardized in our department with the concave rod engaged and rotated first, with intersegmental distractions. The convex rod is under bent and anchored followed by intersegmental compressions. All rods were of titanium alloy. Prone anteroposterior radiograph was taken intraoperatively to make sure the fusion block shift was within accepted limits (<20°). 17
All patients had preoperative standing posteroanterior (PA) and lateral radiographs as well as FBR, and all patients had immediate (within 1 week) and 2-year radiographic follow-up with PA and lateral radiographs. From the preoperative PA radiograph the following were determined: Cobb angle of the major curve, truncal shift, radiographic shoulder height (RSH), truncal height (from the superior endplate of T1 to the inferior endplate of T12), and list (distance from the C7 plumb line to the central sacral vertical line). From the FBR, the Cobb angle was determined and from the preoperative sagittal radiograph, the following were determined: T5-T12 kyphosis, T12-S1 lordosis, and sagittal vertical axis (distance from the C7 plumb line to the supero-posterior corner of S1) (SVA). Postoperative coronal Cobb angle was measured at the immediate and 2-year follow-up. These radiographic parameters have shown good to excellent intraobserver reliability. 18 -22 All radiographs were analyzed by a single surgeon with several years of experience in radiographic and clinical assessment of AIS patients. Assessment of intraobserver reliability was not the focus of this study and was not performed. Additional variables included preoperative curve length (number of vertebrae in the main curve) and instrumentation length (number of vertebrae instrumented and included in the fusion).
The following parameters were calculated (Figures 1 and 2):
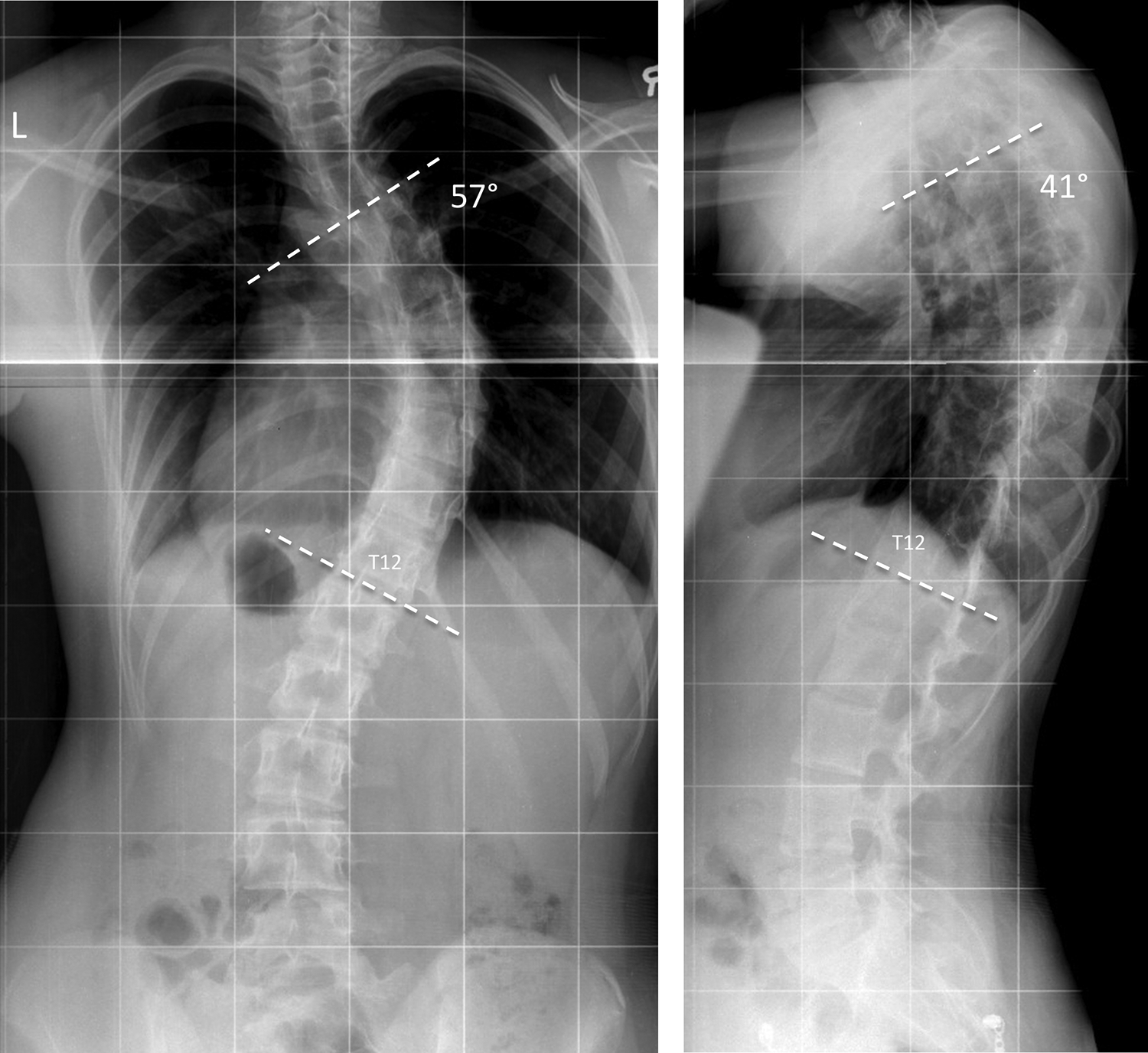
(Left) Anteroposterior radiograph of a Lenke 1A type curve with a preoperative Cobb angle of 57°. (Right) Corresponding lateral radiograph showing a preoperative thoracic kyphosis of 41°.
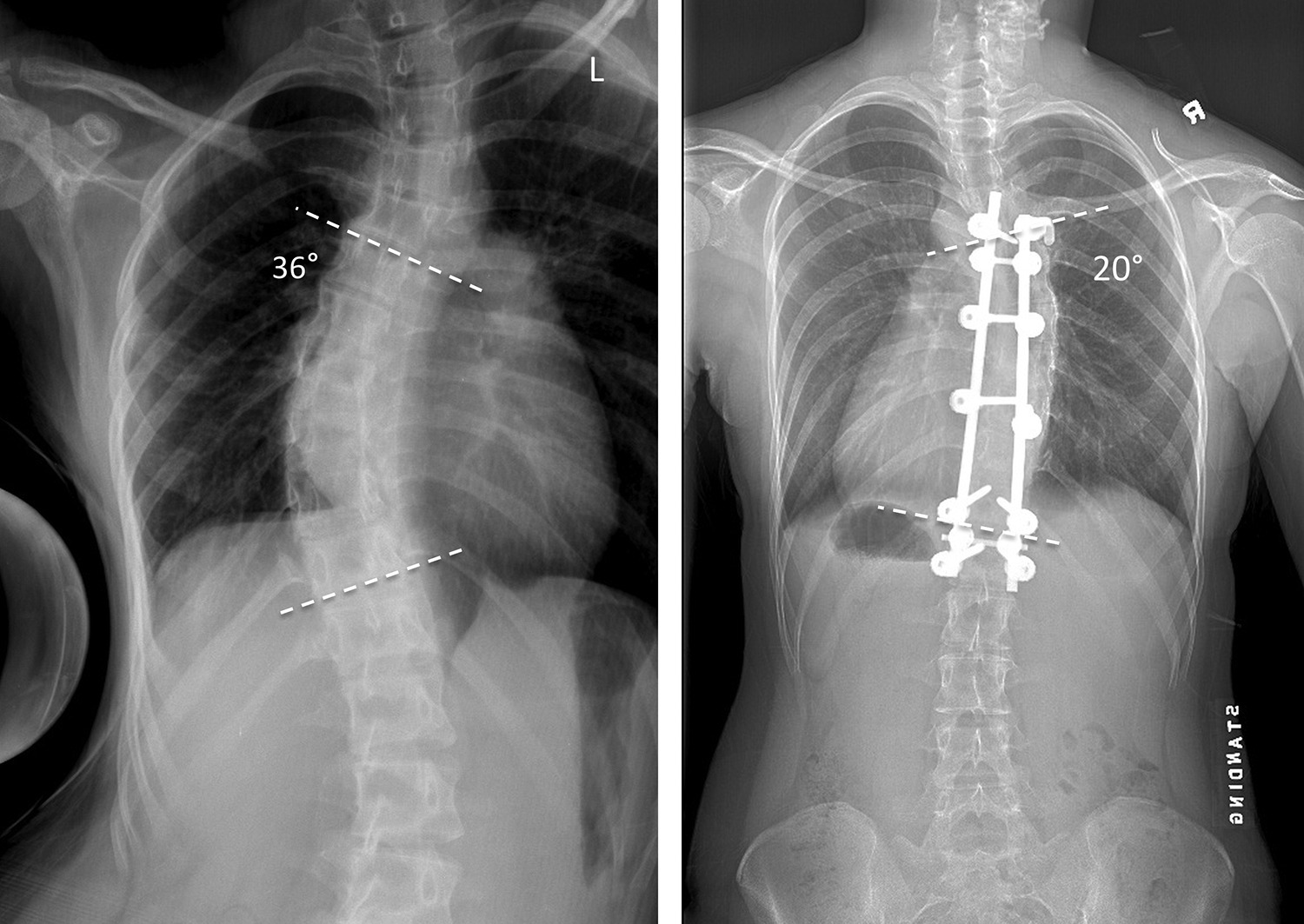
(Left) Fulcrum bending radiograph of the patient from Figure 1 showing a Cobb angle of 36° corresponding to a flexibility of 37%. (Right) Postoperative (2-year follow-up) anteroposterior radiograph showing a Cobb angle of 20° corresponding to a correction rate of 65% and a Fulcrum Bending Flexibility Index (FBCI) of 175%.



Statistical Analyses
All statistical analyses were performed using R version 3.1.3 (R core team, 2014, Vienna, Austria). Data was reported as proportions (%), mean ± standard deviation (SD) and data distribution was assessed by histograms. Parametric data was compared using unpaired, 2-tailed t test or 1-way analysis of variance (ANOVA) and post hoc analysis was performed in cases of significant difference with Tukey’s post hoc test. Correlation between parametric data was analyzed using Pearson’s correlation.
Univariate and multivariate linear regression analyses were performed to analyze the factors associated with an increase in FBCI based on commonly used radiographic descriptors of the coronal and sagittal profile of the spine. 23 -26 The main endpoint, and dependent variable, was FBCI at 2-year follow-up. An increase in FBCI was understood as an increased difference between the potential correction suggested by the FBR and the postoperative Cobb angle. Covariates selected for the multivariate model depended on the univariate analyses as well as a priori knowledge of relevant factors based on the reported literature. Assumptions for linearity were tested using residual plots and quantile-quantile plots. Likelihood ratio test was used to determine the effect on the model fit of adding other predictors. A P value less than .05 was considered statistically significant. Using the coefficients from the multivariate regression as well as the results from the likelihood ratio test, an equation for a novel flexibility index, called the Multiprofile Flexibility Index (MFI), was developed.
Results
A total of 107 patients were included in the study. Mean age was 15.2 ± 3.4 years and 88 patients (82%) were female. The mean Cobb angle was 56° ± 9° with a mean flexibility of 59% ± 15%. Immediate postoperative Cobb angle was 16° ± 7° corresponding to a mean curve correction of 72% ± 11% with a mean FBCI of 128% ± 28%. At 2-year follow-up, the mean Cobb angle was 19° ± 7° corresponding to a mean correction of 67% ± 12% with a mean FBCI of 120% ± 28% (Table 1). The preoperative thoracic kyphosis showed a significant correlation with preoperative flexibility (r = 0.5, P < .001). SVA showed no correlation (r = −0.14, P = .146) and for lumbar lordosis the correlation was weak although statistically significant (r = 0.21, P = .026). Univariate linear regression showed that an increase in FBR Cobb angle, preoperative Cobb angle, and preoperative thoracic kyphosis were significantly associated with an increase in FBCI at 2-year follow-up (P < .001). However, in the adjusted multivariate analysis, only FBR Cobb angle and preoperative thoracic kyphosis were significant predictors (P < .01, R2 = 0.62; Table 2, Figure 3). Preoperative and postoperative thoracic kyphosis was not significantly different between Lenke curve types (P ≥ .415).
Pre- and Postoperative Results of Radiographic Parameters.
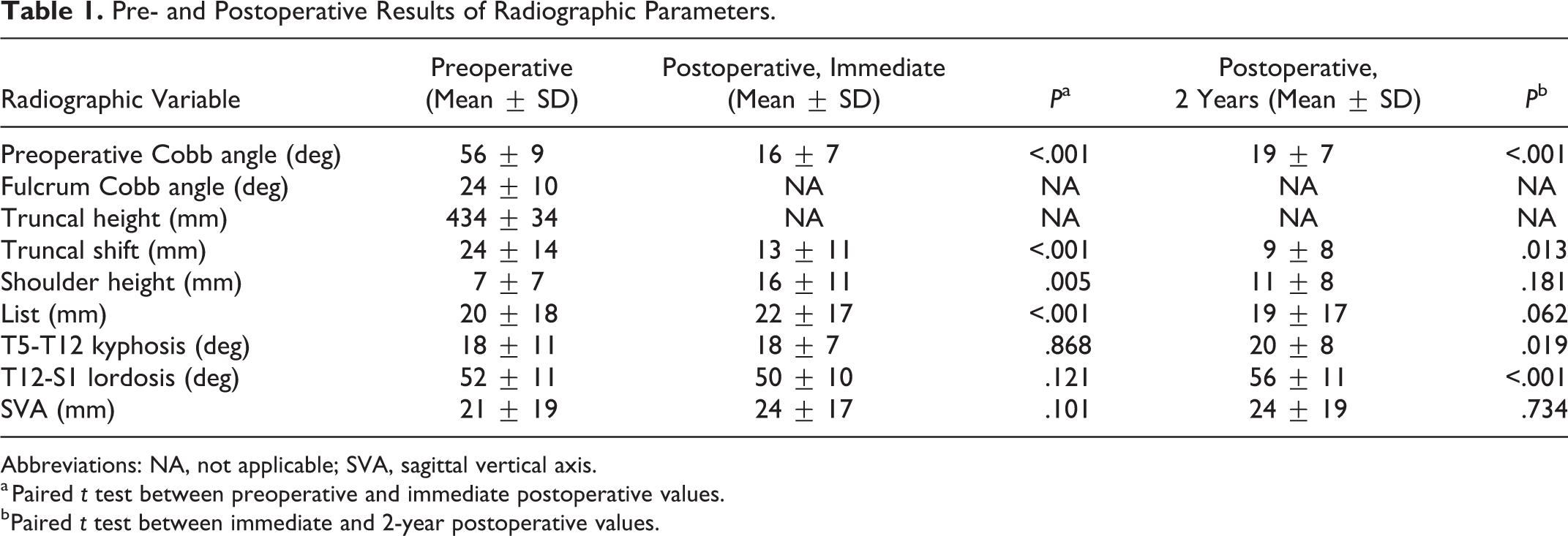
Abbreviations: NA, not applicable; SVA, sagittal vertical axis.
a Paired t test between preoperative and immediate postoperative values.
b Paired t test between immediate and 2-year postoperative values.
Univariate and Multivariate Linear Regression Analysis.
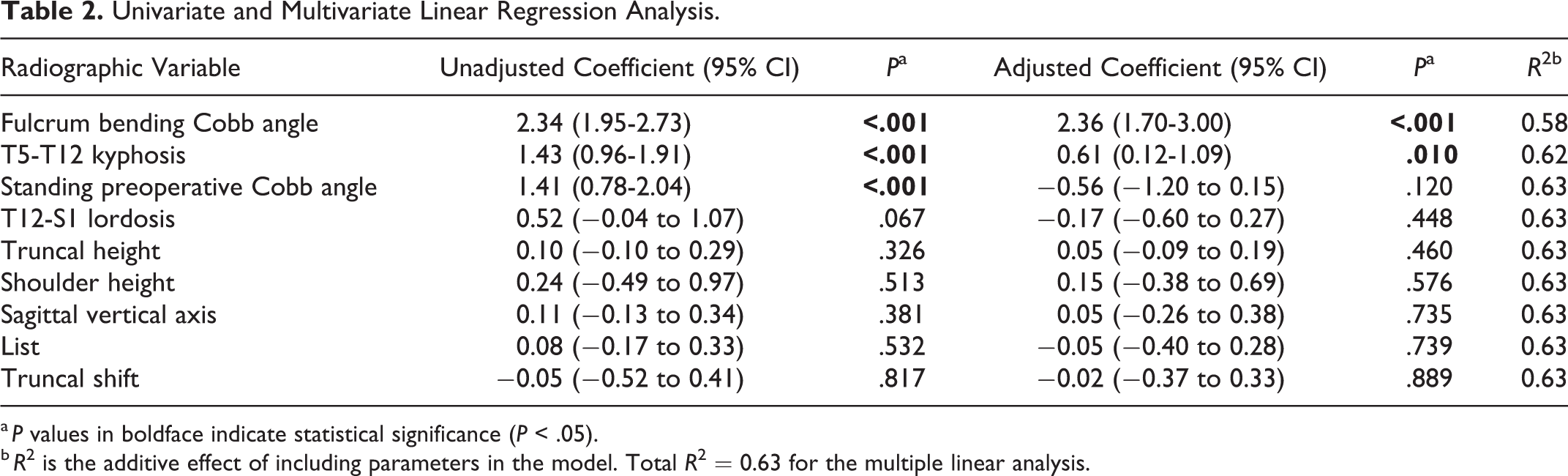
a P values in boldface indicate statistical significance (P < .05).
b R 2 is the additive effect of including parameters in the model. Total R 2 = 0.63 for the multiple linear analysis.
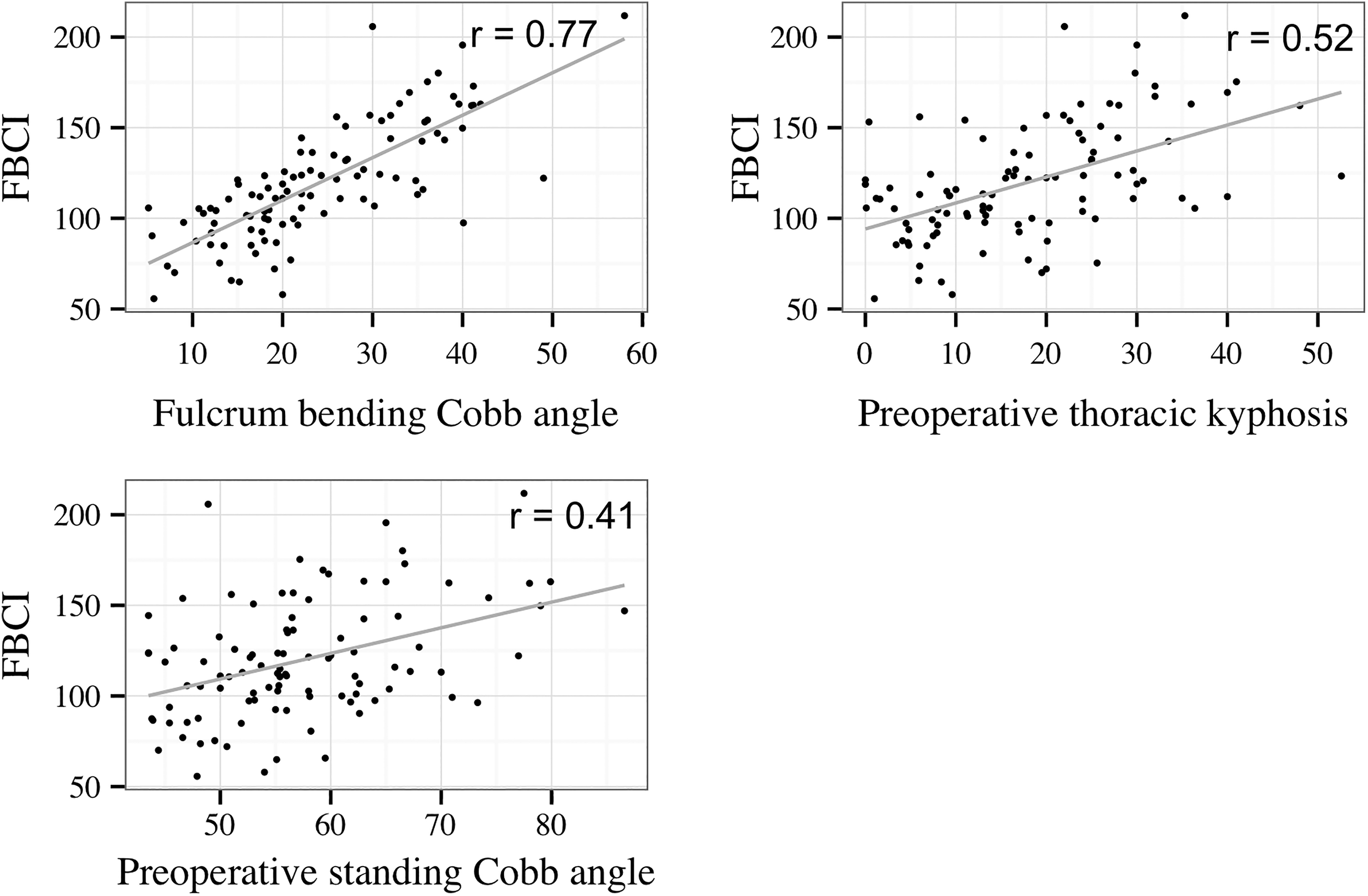
Univariate regression analysis for preoperative Cobb angle, fulcrum bending Cobb angle, and thoracic kyphosis with Fulcrum Bending Flexibility Index (FBCI) as the dependent variable.
Likelihood ratio test demonstrated that FBR Cobb angle and thoracic kyphosis significantly improved the model (P < .01) whereas changes in truncal height, truncal shift, RSH, list, lumbar lordosis, and SVA did not. Preoperative Cobb angle was hypothesized a priori as a predictor and was included in the prediction model (R
2 = 0.63). These findings were then incorporated into our new flexibility index (ie, MFI):
Pearson’s correlation between the MFI was 0.81 and 0.79 for immediate and 2-year FBCI, respectively (P < .001; Figure 4).
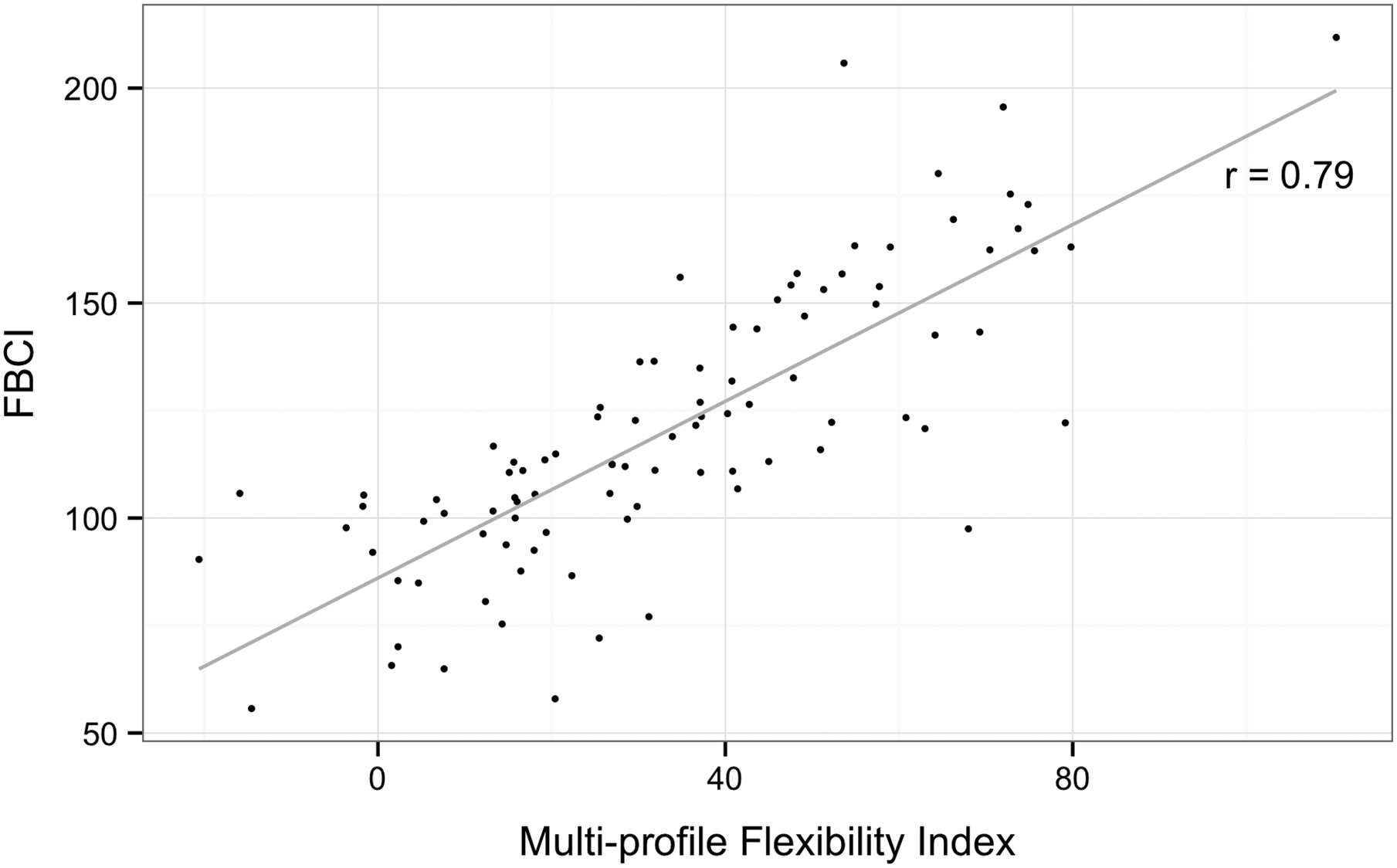
Correlation between the Multiprofile Flexibility Index and the Fulcrum bending flexibility index.
To study the effect of thoracic kyphosis on curve flexibility, patients were arbitrarily divided into hypokyphotic (<20°), normokyphotic (between 20° and 30°), and hyperkyphotic (>30°) groups (Table 3). No significant difference was found for preoperative Cobb angle or curve correction (P > .242) but the groups differed significantly in terms of length of the curve, flexibility, FBCI, and instrumentation length (P < .02). Post hoc analysis showed that the hypokyphotic group had significantly higher flexibility and a lower FBCI than both the normokyphotic and hyperkyphotic groups (P < .01) Also, instrumentation length was significantly longer in the hyperkyphotic group compared with the hypokyphotic group (P = .03) but similar to the normokyphotic group (P = .10). Pearson’s correlation between FBR Cobb angle and FBCI was 0.67, 0.68, and 0.90 for hypo-, normo-, and hyperkyphotic groups, respectively (Figure 5).
Characterization of Thoracic Kyphosis.
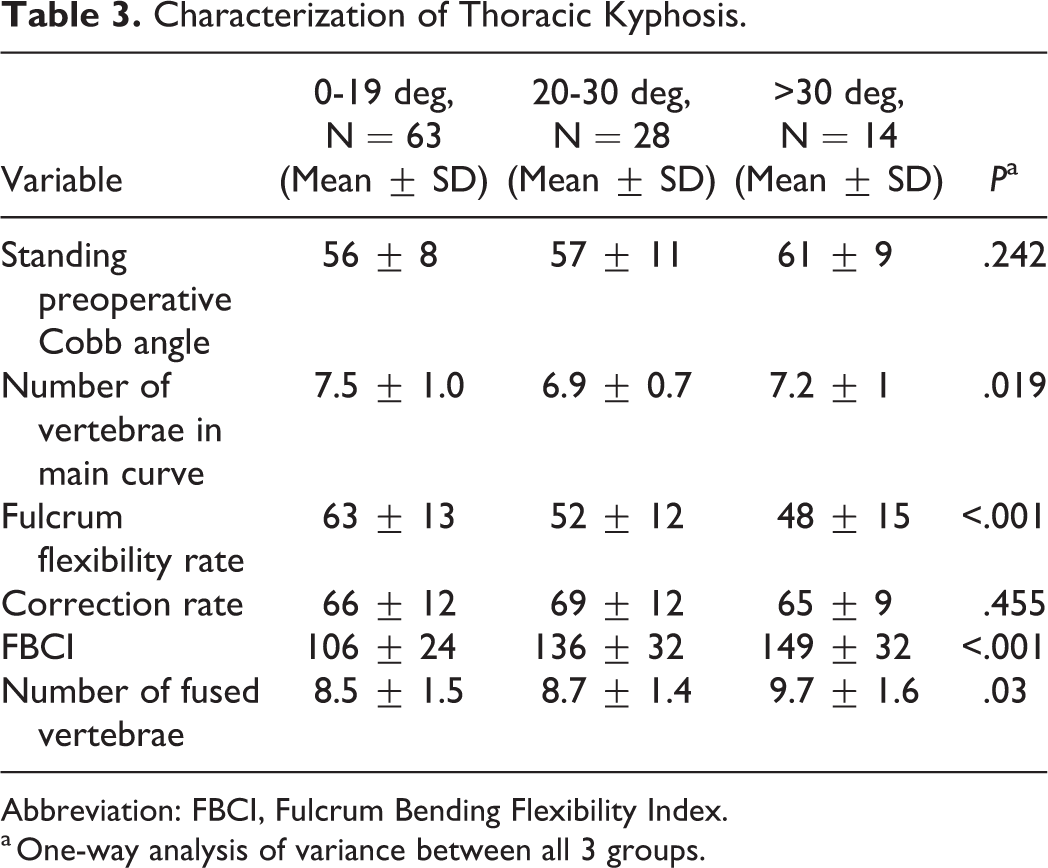
Abbreviation: FBCI, Fulcrum Bending Flexibility Index.
a One-way analysis of variance between all 3 groups.
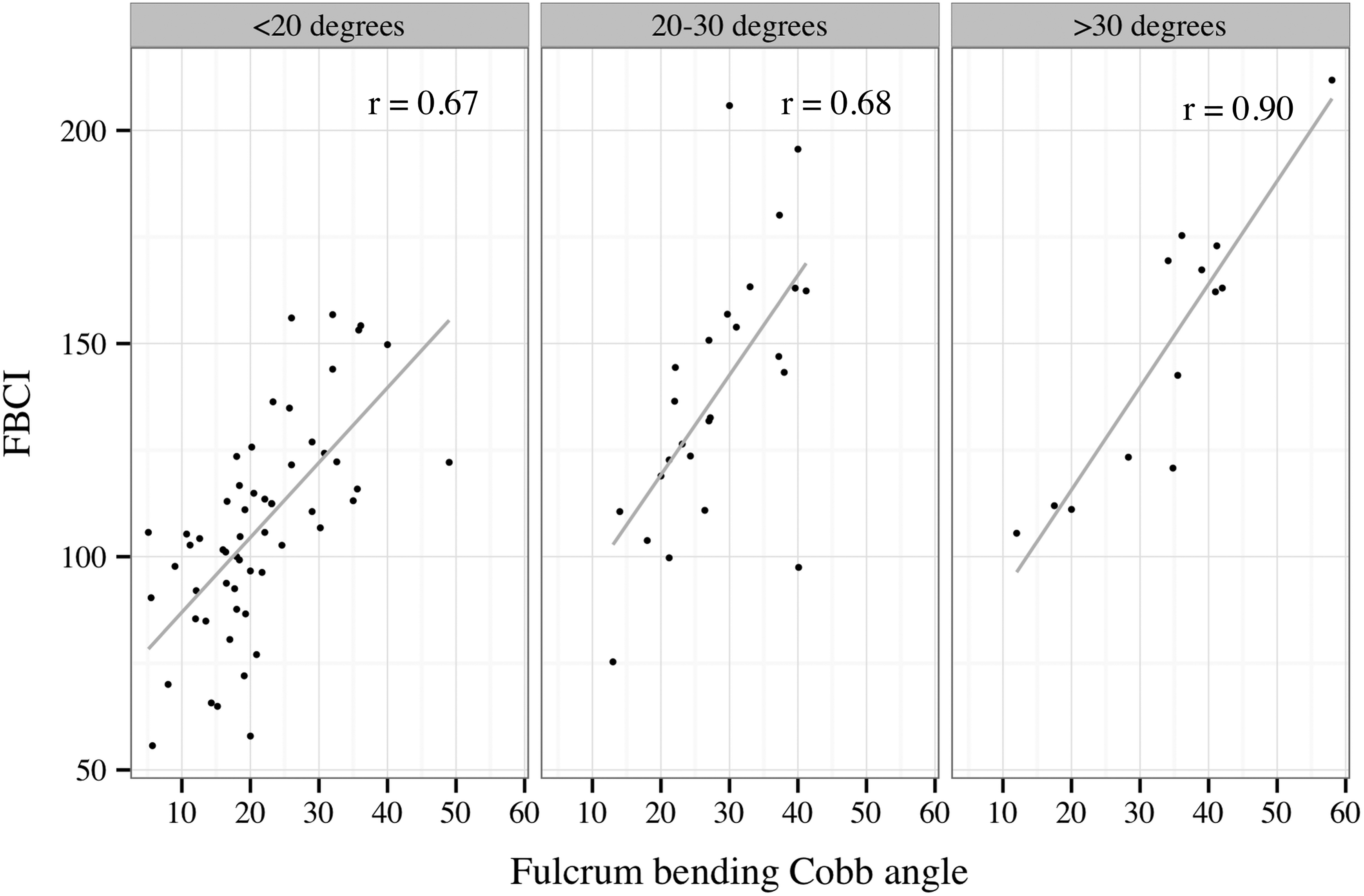
Correlation between the fulcrum bending Cobb angle and Fulcrum Bending Flexibility Index (FBCI) for hypo-, normo-, and hyperkyphotic groups.
Discussion
This study describes the factors affecting the predictability of the FBR in assessing coronal curve flexibility and its relation with postoperative curve correction. We found that an increase in preoperative thoracic kyphosis was significantly associated with a decreased ability of the FBR to predict the postoperative Cobb angle (increase in FBCI). A new flexibility index—the MFI—was introduced incorporating preoperative thoracic kyphosis, standing Cobb angle and the fulcrum bending Cobb angle. This index was introduced to provide a better representation of the “true flexibility” in terms of predicting the postoperative coronal curve correction. The MFI showed a strong correlation with both immediate and 2-year FBCI and provides an assessment of preoperative flexibility, whereby each parameter is weighted according to the predictive effect on the surgical outcome.
Our results suggest that preoperative flexibility is influenced by the sagittal profile of the curve. This may be due to an inherent coupling between the coronal and sagittal deformity making hyperkyphotic curves less flexible or attributed to a decreased hinge effect of the fulcrum with increased kyphosis disguising the actual flexibility of the curve. To investigate the clinical implication of this finding, patients were arbitrarily grouped according to the degree of thoracic kyphosis. Curve flexibility was markedly higher in the hypokyphotic group while curve correction was similar. Correlation between FBR and FBCI differed substantially between kyphosis groups (Figure 5), stressing that the limitations of the FBR in predicting postoperative curve correction need to account for the sagittal profile. Additionally, we observed a significantly longer instrumentation in the hyperkyphotic group even though the preoperative curve length was actually significantly shorter than in the hypokyphotic group (Table 3). As such, a higher kyphosis may result in a less flexible curve, which would require recruitment of more vertebral levels when fusion-level selection is based on the FBR. Even in centers that do not use bending radiographs for fusion level selection, we would encourage that the lower instrumented vertebra may be chosen more conservatively in stiff, hyperkyphotic patients as a longer fusion may be required or that the surgical strategy should involve more aggressive soft-tissue release or even osteotomies in order to save fusion levels. We propose that the MFI may serve as an indicator for this approach and guide clinicians in optimizing surgical management. However, future studies should assess whether these risks of a more aggressive surgical approach outweigh the risk and costs of adding fusion levels.
The study included all main thoracic curves (Lenke 1, 2, and 3) to increase the clinical applicability of our findings. The Lenke classification is not routinely used for fusion selection in our center and only fusion of the main curve was performed in the current cohort. The T5-T12 kyphosis is typically within the upper- and lower limits of the main curve and neither pre- nor postoperative kyphosis differed between Lenke types. Hence, we suspect that our findings are relevant for all 3 curve types in cases of selective thoracic fusion.
Sun et al 16 noted that “extraneous” factors (ie, X-Factor Index) exist that may describe some of the variation between the flexibility of the curve and the FBCI. The authors proposed that these “X-factors” likely involved soft tissue release, surgical technique and strategy, stronger instrumentation and improved anesthetic technique. While these factors likely explain the systematic difference between flexibility and correction rate, they do not explain the large variation in the X-Factor Index (and FBCI) between patients in the same cohort who were operated by the same surgical team and similar screw strategy, fusion level selection and instrumentation. Our results indicate that part of the mismatch between the FBR and the postoperative results may be accounted for by addressing the sagittal profile of the curve.
While we consider our results to be of substantial clinical importance, we do acknowledge that the relationship between FBCI and thoracic kyphosis is not a perfectly linear one (Figure 3) and that our prediction model only explains 63% of the variation seen in FBCI (Table 2). Ultimately, curve correction is influenced by a number of surgical factors (eg, correction maneuvers and use of osteotomies) and the knowledge that hyperkyphotic curves may be underestimated in terms of flexibility is only one element of many to consider in the preoperative planning.
Patients were categorized as hypo-, normo-, or hyperkyphotic as these represented traditional clinical entities. However, thresholds were arbitrarily chosen based on the available literature as well as the current data material (Figure 3). There is no consensus regarding the “normal range” of kyphosis as this varies between studies and depends on a multitude of factors, for example, ethnicity, measurement level, and age. 22,27,28 We considered using a 40° upper threshold to deem patients as hyperkyphotic, but only three patients fell in this category making statistical analysis meaningless. The proposed categorization should be either validated or revised in future studies. Also, the hyperkyphotic group consisted of only 14 patients, which may explain why the MFI showed only a modest improvement in correlation with FBCI compared with FBR Cobb angle. Furthermore, the MFI needs to be validated in a different cohort to ensure the external validity of our findings.
As the current study was based on standard anteroposterior and lateral radiographs, we were not able to more thoroughly access the importance of the 3-dimensional coupling that exist between increased deformity in the coronal, axial, and sagittal planes. Newton et al 29 described the “lordo-scoliosis” (hypokyphosis) that is highly affected by the axial rotation of the curve and the authors hinted that idiopathic scoliosis without hypokyphosis may be a different clinical entity. We have previously shown that when the coronal deformity is reduced during FBR a coupled “normalization” is seen in the sagittal plane. 7 As more advanced imaging, such as biplanar slot scanners, becomes available, additional parameters may be incorporated into the multiprofile perspective; however, these scanning techniques are limited by an inability to access curve flexibility as patients cannot be placed in the supine position. Ultimately, these combined approaches may help identify different AIS phenotypes with different management requirements and surgical outcomes.
Regardless of the study’s limitations, our prospective study is one of the largest to utilize the FBR to describe the effects of the sagittal profile on curve flexibility and surgical outcome in AIS patients. Our work could provide the foundation for a new clinical and research platform to help refine the “outcome prediction profile” for curve correction.
Conclusion
In a large consecutive series of AIS patients we found that an increase in preoperative thoracic kyphosis was significantly associated with a decreased ability of the FBR to predict the postoperative Cobb angle. Furthermore, we reported a novel index, the MFI (ie, Multiprofile Flexibility Index), that may be used to more accurately access curve flexibility taking into account both the coronal and sagittal profile. The MFI can be adjusted to also account for sagittal flexibility, thereby enhancing its predictive utility by addressing flexibility in 2 planes. This study broadens the understanding of curve flexibility and may contribute to a more personalized approach toward the surgical management of AIS patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.