
Abstract
Study Design
A retrospective cohort utilizing the PearlDiver Patient Claims Database.
Objective
Cervical disc arthroplasty (CDA) is accepted treatment for cervical radiculopathy; however, it may also be safe and effective in myelopathy. Thus, we compared clinical characteristics and outcomes in patients undergoing CDA and anterior cervical discectomy and fusion (ACDF) for degenerative cervical myelopathy (DCM) specifically.
Methods
Patients undergoing CDA or ACDF between 2015-2019 were identified with follow-up through 2021. Univariate and multivariable analyses were performed to identify factors associated with either procedure. Reoperation rates were compared using propensity-matched analysis.
Results
We identified n = 2391 CDA and n = 50 845 ACDF procedures for DCM. Factors favoring CDA included: female sex, younger age, lower CCI, lower incidence of obesity, osteoporosis, diabetes, or smoking (P ≤ .001); remaining significant after multivariable logistic regression except for sex (P = .06). Single-level surgery was more predictive for undergoing CDA. CDA patients had lower 90-day readmissions, complications, and lower opioid utilization. The overall reoperation rate was 5%. Predictors of reoperation included: male sex, younger age, greater CCI, obesity, osteoporosis, diabetes, smoking, and multi-level surgery; all remaining significant after multivariable analysis except for diabetes (P = .23) and CCI (P = .05). After propensity-matching CDA and ACDF patients (n = 2391), there was no difference in re-operation rates (P = .47).
Conclusions
CDA patients were healthier (less obesity, smoking, diabetes, better CCI) and represented 4.5% of anterior procedures for DCM. In univariate analysis, readmission rates, medical complications, and opioid use were lower in CDA patients, despite a similar reoperation rate. Considering these findings, CDA might be used very selectively for DCM.
Introduction
Degenerative cervical myelopathy (DCM) represents a set of nontraumatic degenerative forms of spinal disease including cervical spondylotic myelopathy, degenerative disc disease, and ossification of either the posterior longitudinal ligament or the ligamentum flavum, with degenerative changes leading to spinal canal stenosis, compression of the spinal cord, and eventually myelopathy-based disability. 1 Both static and dynamic forces are at play in the pathophysiology.1,2 Detailed descriptions of DCM, including epidemiology, pathophysiology, and treatment has recently been reviewed and published.1,2 DCM from cord compression often results in neck pain, hyperreflexia, paresthesia, balance difficulties, loss of fine motor control, bladder dysfunction, falls, and hand clumsiness. 3 The RECODE-DCM effort aims to improve research regarding DCM by developing a MeSH index term, minimum dataset (ie, core outcomes set), and determining research priorities. 3
Given that DCM is the leading cause of spinal cord dysfunction in adults, treatment is aimed at minimizing permanent disability and improving quality of life. 2 Surgical treatment options for DCM consist of either anterior or posterior spine surgery, with anterior cervical discectomy and fusion (ACDF) typically the gold standard. However, ACDF results in loss of motion across the fused segments, with pseudarthrosis and acceleration of adjacent segment disease (ASD) posing risks4-6; thus, cervical disc arthroplasty (CDA) offers an alternative, preserving motion. As the number of fused levels increases, the potential negative impact that loss of motion has on quality of life becomes increasingly important.
CDA has been FDA-approved for pathology at 1-2 contiguous levels, between C3-C7, and for treatment of cervical myelopathy and/or radiculopathy, but specific indications remain device-specific. 7 Data from outside the US indicate that CDA may also be safe and effective in patients with mild myelopathy,8,9 but appropriate patient selection, sufficient decompression, and proper positioning of the device are key. 10 Data for cervical radiculopathy indicates that CDA is at least comparable to ACDF with respect to outcomes and complications; superiority remains debated however. 11 Aside from motion preservation, CDA may also reduce the incidence of adjacent segment disease and patients are less likely to require surgical treatment of ASD.6,12-16 Contraindications to the use of CDA include infection, trauma, hypermobility/instability, osteoporosis, severe facet arthropathy, and axial neck pain without radiculopathy or myelopathy. 7 The complications related to CDA include: migration of the implant, insertion problems/failures, neck pain, heterotopic ossification, and radiculopathy, 17 and recurrent/persistent stenosis. 18 In addition to mechanical failure, 19 there may be worse dysphagia in long-term follow-up. 20
Limited studies have evaluated the use of CDA in the treatment of DCM only specifically - most were performed outside the US or are device IDE trials21-27; whereas the majority of general CDA-related studies utilized a combined cohort of cervical radiculopathy, myelopathy, or myeloradiculopathy, and even fewer compared ACDF vs CDA directly for DCM only. 28 Thus, we focused on comparing clinical characteristics and outcomes between ACDF and CDA for degenerative cervical myelopathy using a large national insurance claims database to establish a possible equivalency between these treatment modalities, utilizing both univariate and multivariable analyses. To reduce bias from confounding variables and to ensure equivalency between groups, we utilized propensity score matching, which allows balancing baseline covariates using logistic regression in order to minimize their impact and reanalyze the data for treatment effects. 29
Materials and Methods
All aspects of this study were approved by the Oregon Health & Science University Institutional Review Board # STUDY00024370. Given that de-identified information was utilized, the study was exempt from requiring informed consent. This retrospective study was conducted utilizing the PearlDiver Mariner Patient Claims Database (PearlDiver Technologies).30,31 This is a national insurance database of commercial, Medicare, Medicaid, government, and cash payers containing 157 million distinct patient records from 2010-2021 with longitudinal follow-up that can be searched using International Classification of Diseases (ICD) Ninth and Tenth Revisions and Current Procedural Terminology (CPT) codes. Claims data is collected from all fifty United States and its territories and includes over 260 insurers. Patient data is de-identified, HIPAA compliant, and tracked longitudinally using a unique, encrypted identifier regardless of insurer.
We identified all patients with an ICD-10 code for cervical myelopathy from 2015-2021, since the ICD-10 coding system was implemented in 2015, and to allow for sufficient follow-up in the database post-operatively. Using CPT codes, we further identified patients undergoing CDA and ACDF from 2015-2019 with a diagnosis of cervical myelopathy, which comprised the two cohorts (Supplementary Tables 1 and 2).
Clinical data collected included: age, sex, obesity, smoking status, osteoporosis status, Charlson Comorbidity Index (CCI),32,33 1- vs multi-level surgery, cervical spine reoperations, 90-day readmissions, medical complications, and opioid usage as measured using morphine milligram equivalents (MME). For the cohorts identified, no missing data were present for the data variables collected. The PearlDiver database does not include data on implant details.
Statistical Analysis
Predictors of Arthroplasty vs ACDF for Degenerative Cervical Myelopathy Diagnosis: Univariate Analysis.
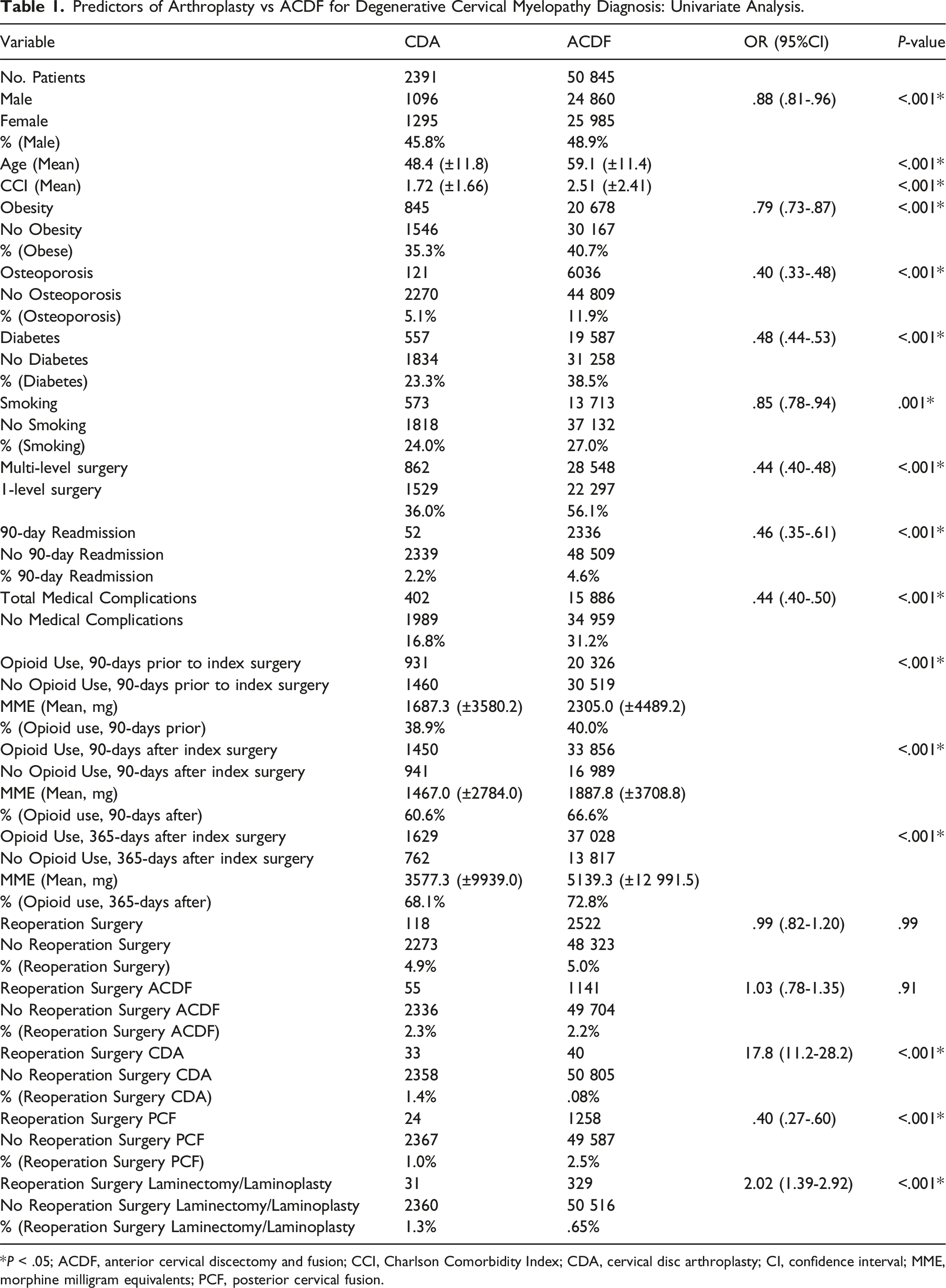
*P < .05; ACDF, anterior cervical discectomy and fusion; CCI, Charlson Comorbidity Index; CDA, cervical disc arthroplasty; CI, confidence interval; MME, morphine milligram equivalents; PCF, posterior cervical fusion.
Predictors of CDA vs ACDF for Degenerative Cervical Myelopathy (Multivariable Logistic Regression Analysis).
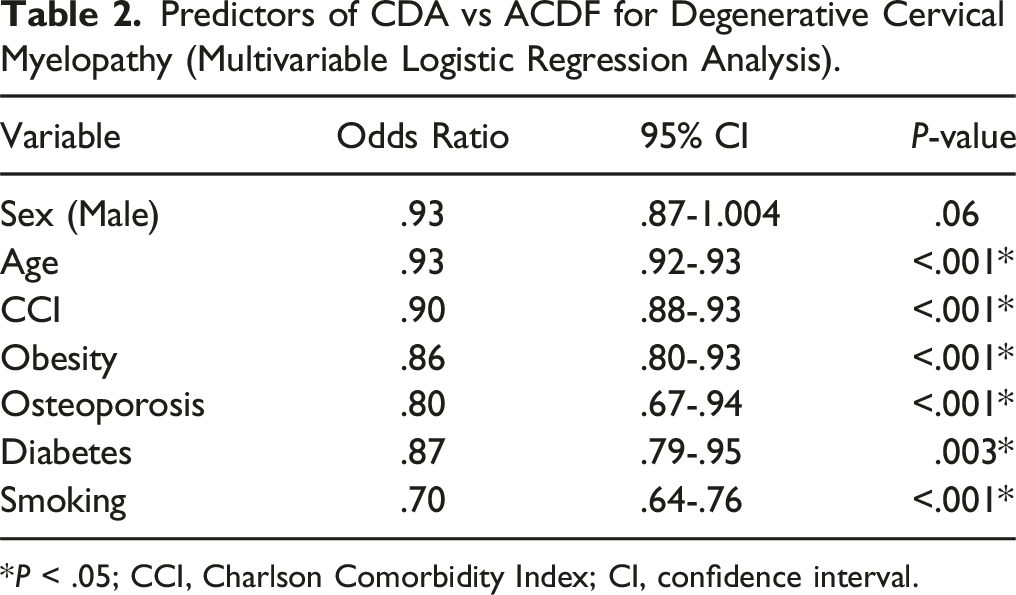
*P < .05; CCI, Charlson Comorbidity Index; CI, confidence interval.
Predictors of Reoperation Cervical Surgery for Patients With Degenerative Cervical Myelopathy Diagnosis who Underwent Anterior Surgery, ie Anterior Surgery = ACDF or CDA (Univariate Analysis).
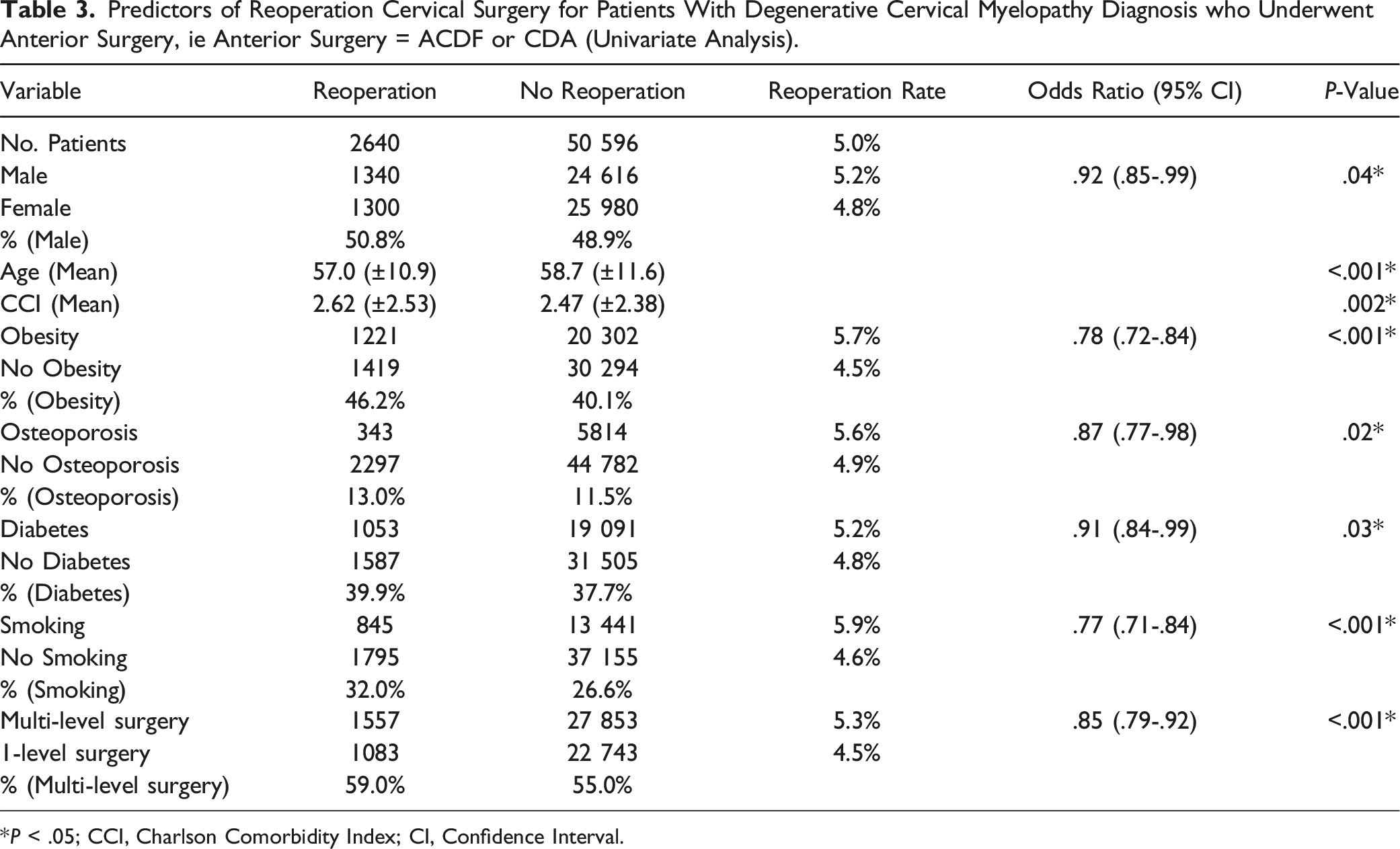
*P < .05; CCI, Charlson Comorbidity Index; CI, Confidence Interval.
Predictors of Reoperation Cervical Surgery for Patients With Degenerative Cervical Myelopathy Diagnosis who Underwent Anterior Surgery, ie Anterior Surgery = ACDF or CDA (Multivariable Logistic Regression Analysis).
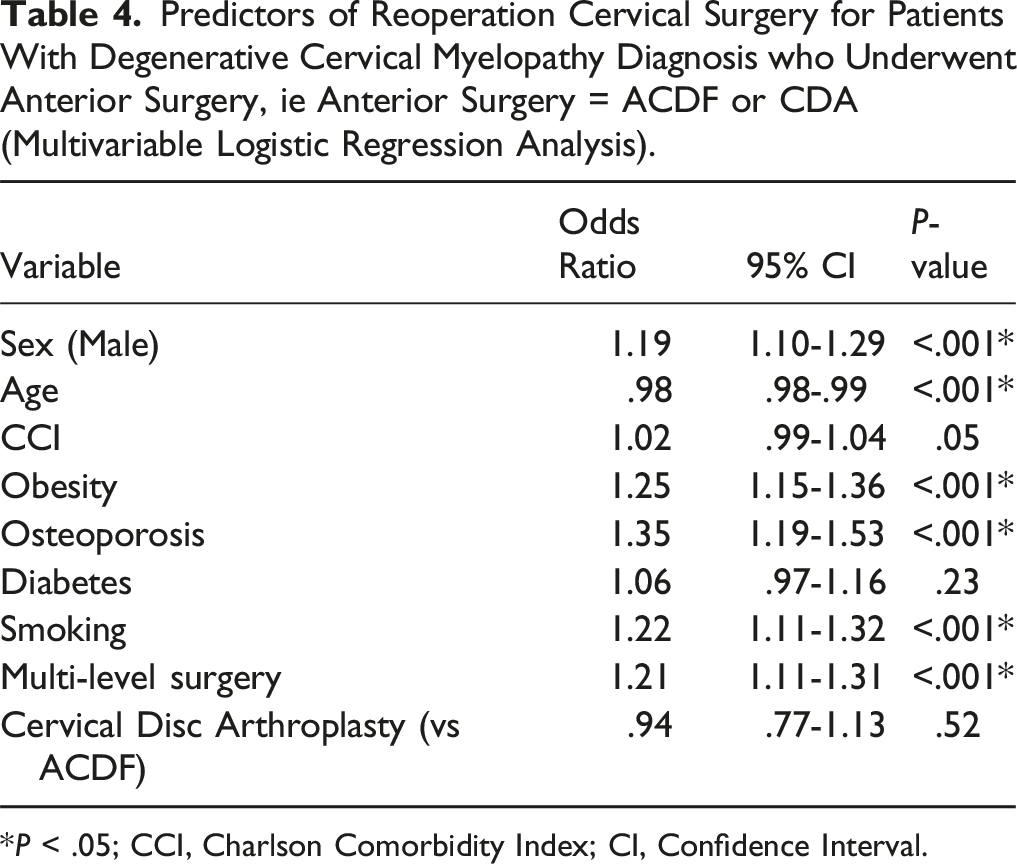
*P < .05; CCI, Charlson Comorbidity Index; CI, Confidence Interval.
Results
Patient Characteristics
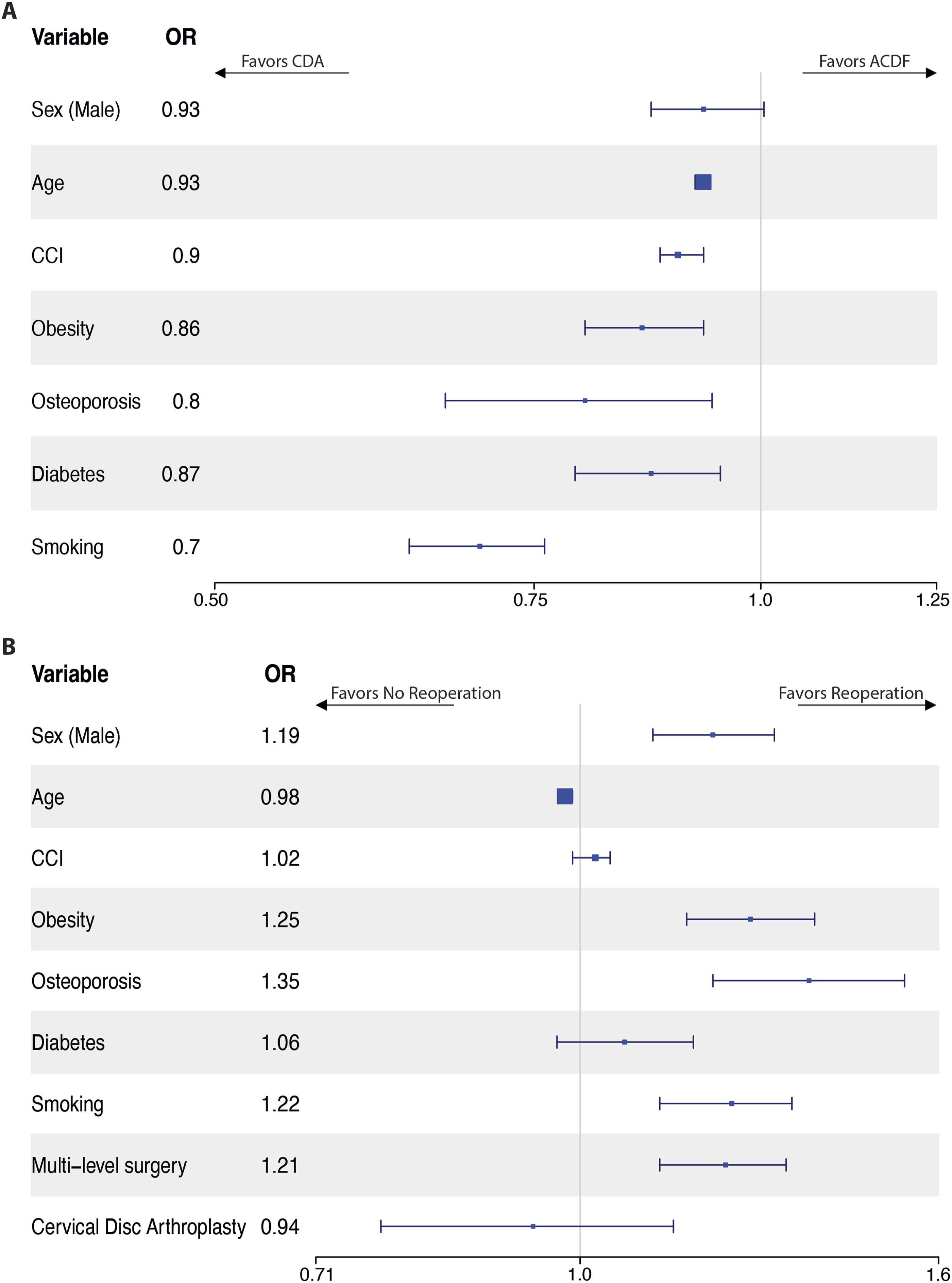
From the PearlDiver Mariner Patient Claims Database, we identified 2391 patients who underwent CDA for myelopathy (45.8% male) and 50 845 patients who underwent ACDF for myelopathy (48.9% male) (Figure 1) (Table 1). Univariate analysis identified that CDA patients were less likely to be male (OR .88, P < .001), more likely to be younger (48.4 years vs 59.1 years, P < .001) with lower CCI (1.72 vs 2.51, P < .001), less likely to smoke (OR .85, P = .001), less obese (OR .79, P < .001), and were less likely to have a diagnosis of osteoporosis (OR .40, P < .001) or diabetes (OR .48, P < .001) than patients undergoing ACDF. After multivariable logistic regression analysis: age, CCI, obesity, osteoporosis, diabetes, and smoking all remained significant independent predictors of CDA over ACDF (P ≤ .003), with female sex as a trend favoring CDA (P = .06) (Table 2 & Figure 2A). Selection schema of CDA and ACDF patient cohorts from the PearlDiver database. (A) Forest plot of predictors of CDA vs ACDF for degenerative cervical myelopathy (multivariable logistic regression analysis), and (B) of predictors of reoperation for degenerative cervical myelopathy patients who underwent either CDA or ACDF anterior surgery (multivariable logistic regression analysis).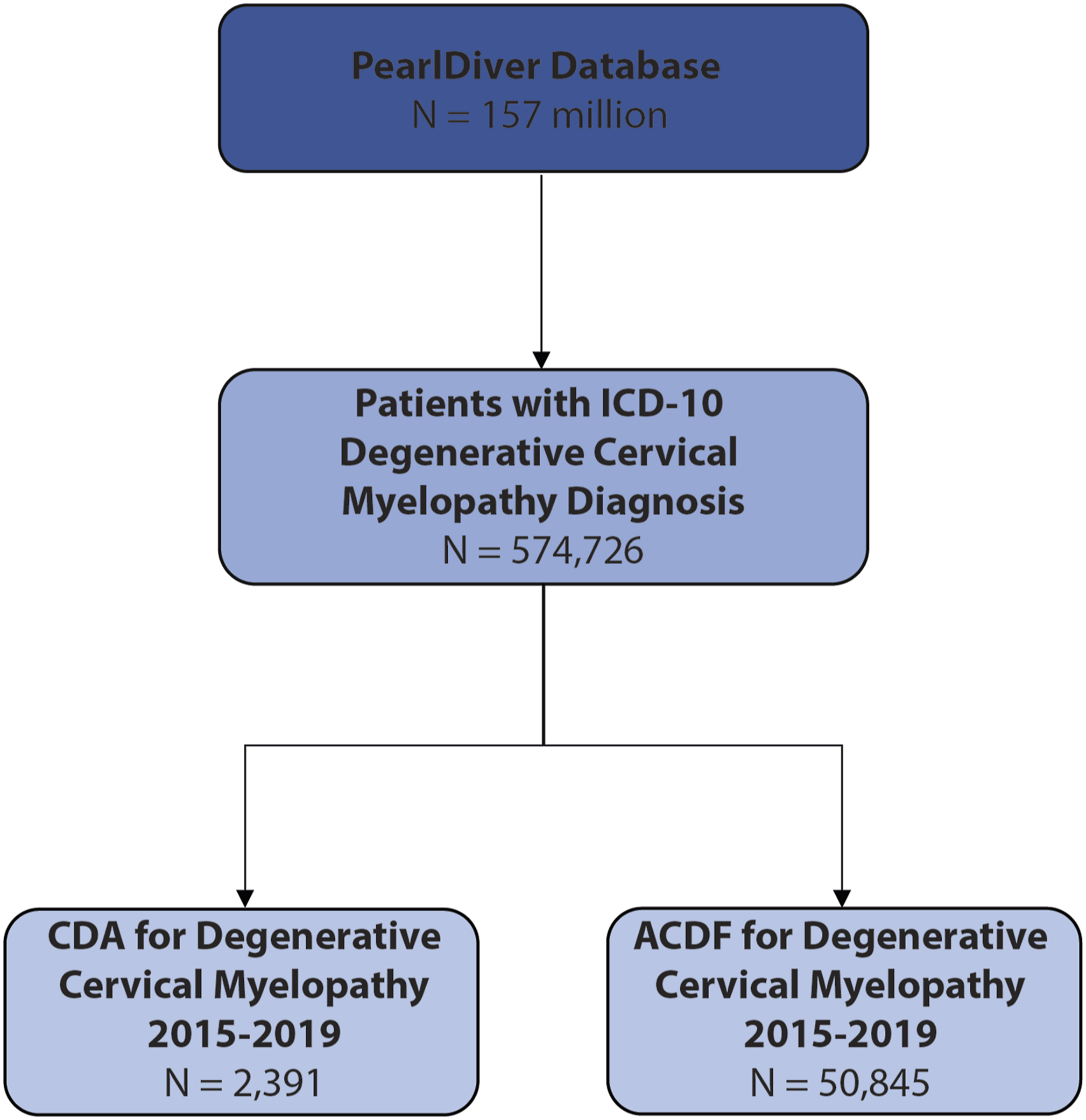
Postoperative Outcomes
Regarding outcomes, CDA patients were less likely to require multi-level surgery (OR .44, P < .001) and had a decreased likelihood of 90-day readmission (OR .46, P < .001), medical complications (OR .44, P < .001), opioid use in the 90 days preceding (1687.3 mg MME vs 2,305 mg MME, P < .001) and after surgery (1,467 mg MME vs 1887.8 mg MME, P < .001), and at 1-year post-surgery (3577.3 mg MME vs 5139.3 mg MME, P < .001).
The cervical reoperation rate was similar between the two cohorts (4.9% for CDA vs 5.0% for ACDF, P = .99) with an overall reoperation rate of 5% amongst the entire study population.
Factors Associated with Reoperation Following Anterior Surgery
In univariate analysis, factors predicting reoperation included male sex, younger age, greater CCI, obesity, osteoporosis, diabetes, smoking, and multi-level index surgery (all P ≤ .04) (Table 3). After multivariable logistic regression, male sex, age, obesity, osteoporosis, smoking, and multi-level index surgery remained significant (P < .001) predictors of reoperation surgery, with a trend for CCI (P = .05) (Table 4 & Figure 2B). The reoperation surgeries were more likely to be motion-preserving for CDA patients (for CDA reoperations: CDA 1.4% vs ACDF .08%, P < .001; for laminectomies or laminoplasties reoperations, CDA 1.3% vs ACDF .65%, P < .001), whereas the ACDF cohort was more likely to undergo posterior cervical fusion (CDA 1.0% vs ACDF 2.5%, P < .001), while both groups were equally likely to undergo an ACDF reoperation (CDA 2.3% vs ACDF 2.2%, P = .91).
Reoperation Rates for CDA vs ACDF Following Propensity-Score Matching
Pre- and Post-matched Propensity Variables: CDA Matched to ACDF Patients 1:1 by Variables Below.
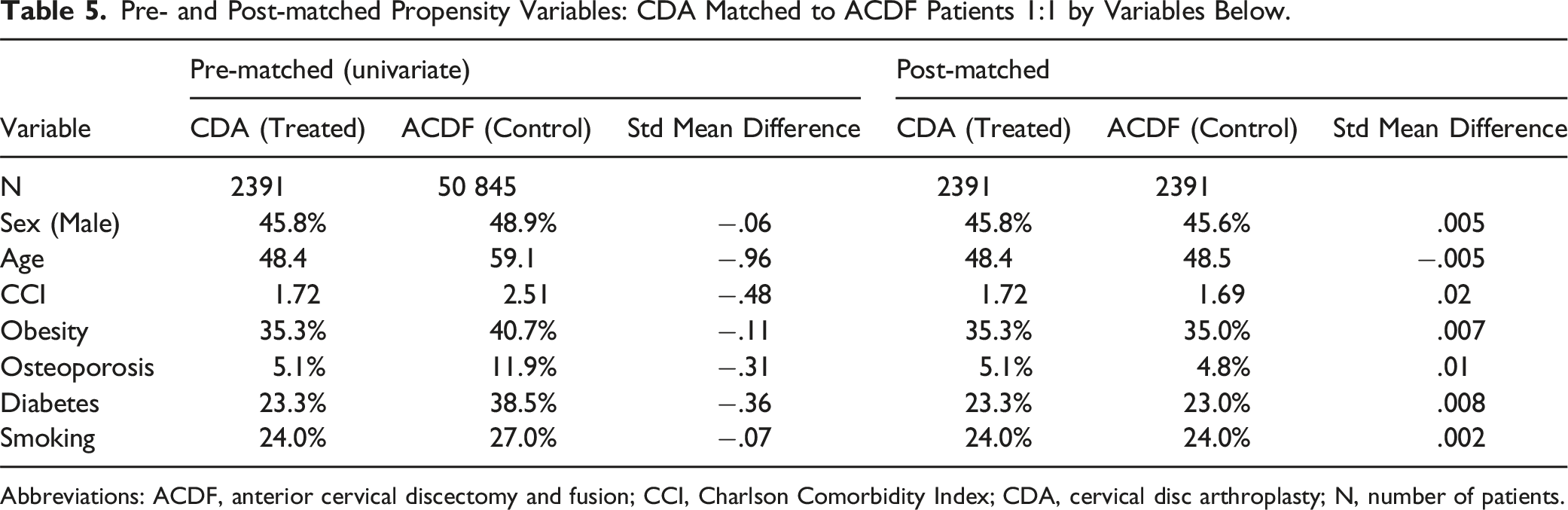
Abbreviations: ACDF, anterior cervical discectomy and fusion; CCI, Charlson Comorbidity Index; CDA, cervical disc arthroplasty; N, number of patients.
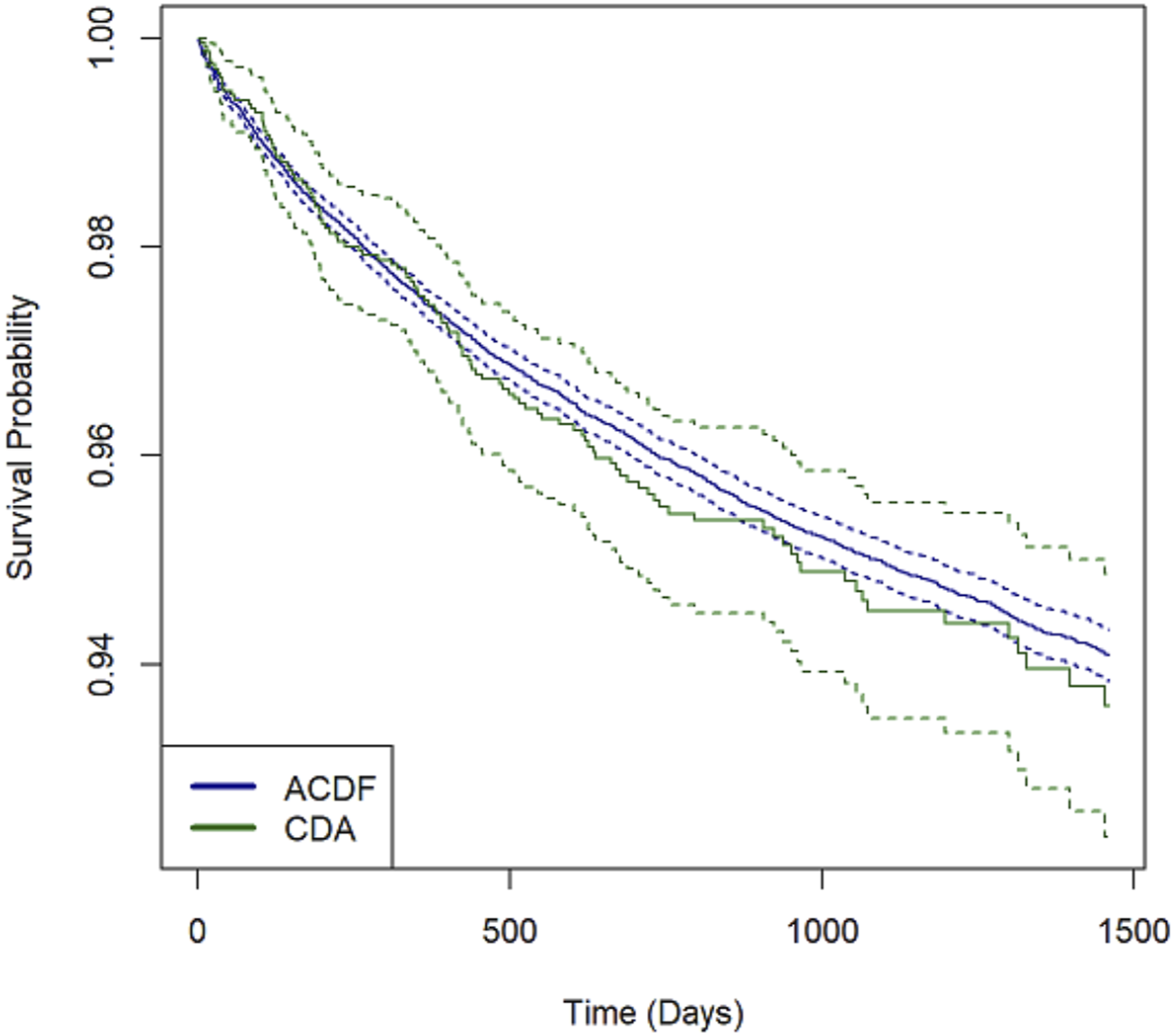
Evaluation of re-operation free survival between CDA and ACDF patients with diagnosis of degenerative cervical myelopathy. P = .5, indicating no differences in reoperation rates when comparing CDA to ACDF in the treatment of DCM.
Discussion
While cervical disc arthroplasty is an established and well-studied treatment for cervical radiculopathy, much less is known about its applicability in cervical myelopathy. We present the first large, national population database study investigating the role of CDA, specifically in degenerative cervical myelopathy, relative to ACDF, as well as factors associated with undergoing CDA. CDA was the treatment of choice in only 4.5% of DCM patients undergoing anterior surgery, similar to a MarketScan database study evaluating ACDF vs CDA for single-level cervical degenerative disc disease (2.7%). 34
Gornet et al 21 evaluated CDA vs ACDF for myelopathy vs radiculopathy in a small clinical trial and found that surgery times were longer, but adverse effects fewer, whereas measurements of success such as Neck Disability Index (NDI), neurological status, reoperation rates, and 2nd surgery failure demonstrated no difference at 2- or 7 years post-operatively. Given that we demonstrated reduced 90-day readmission rates, medical complications (almost half at 16.8% for CDA and 31.2% for ACDF), reduced short- and long-term post-operative opioid use, and overall similar reoperation rates, this combined argues for at least equivalency between CDA and ACDF for DCM. CDA may be a safer and better tolerated treatment option in these cases.
One challenge in utilizing CDA is that devices are generally utilized based upon their FDA-approved indications; requiring new trials or IDEs for expansion of indications would be costly and require significant effort. A recent study found significant differences in hospital characteristics related to CDA preference over ACDF – at the geographical level, as well as institutional level (ie, private vs public). 35 That study also indicated that younger age increased the odds of CDA, similar to our results. While complication rates were unchanged, CDA patients had shorter length of stay but at increased surgical cost. In our study, CDA patients were more likely to be female, younger, have lower CCI, and have lower rates of obesity, diabetes, osteoporosis, tobacco use, and multilevel surgery than patients undergoing ACDF. This suggests that during patient selection, surgeons may be more likely to propose CDA in patients that are generally healthier.
Opioid use remains a hot topic in spine surgery and it is difficult for clinicians to balance patient expectations and pain management. We found that opioid use decreased post-op to ∼¾ that of preoperative usage within the 90-day period. While a continued reduction was observed in both groups over time, opioid use at 1-year post-op was significantly less in the CDA group compared to the ACDF group; in fact, opioid use was nearly the same for ACDF patients at 1-year, as it was for CDA patients at 90-days (ACDF 1y = 14.1 MME/day vs CDA 90d = 16.3 MME/day and CDA 1y = 9.8 MME/day); although similar percentage-wise when comparing MME at pre-op 90-day vs post-op 1-year (52.3% of pre-op for CDA vs 55% for ACDF). Thus, both surgeries result in overall similar reductions in pain, but selection factors may bias ‘more painful’ patients to undergo ACDF instead.
CDA patients continued to prefer motion-preservation surgery in subsequent reoperations (eg, redo CDA, or laminectomies/laminoplasties). While ACDF patients were more likely to undergo fusion procedures (eg, posterior cervical fusion) for their reoperations, both groups were equally likely to undergo an ACDF reoperation. It remains unclear what influences this tendency to continue with either motion-preserving or fusion surgery – possibilities include: surgeon-related factors (patients returning to the same surgeon for reoperation or preferences to utilize the same technique), patient factors (either poor candidates for motion preservation surgery, or conversely prefer ‘motion-preservation’ and would rather reattempt it), co-factors of these such as institutional practices, insurance coverage, surgical costs, or other as-of-yet undetermined factors.
There were no differences in reoperation rates between CDA and ACDF patients, including after propensity score matching for sex, age, CCI, obesity, osteoporosis, diabetes, and smoking status. Although differences in reoperation rates have been previously reported, a 10-year follow-up study of patients in New York state who underwent CDA for either radiculopathy or myelopathy also showed similar reoperation rates when compared to ACDF 20 ; similarly there were no differences in reoperation rates in another single-surgeon study 36 and another database study found similar reoperation rates at 5 years post-procedure for cervical disc degenerative disease. 34 In contrast, one long-term follow-up analysis from IDE trials reported lower rates of reoperation for CDA 37 ; it is unclear where this discrepancy originates – possibly differences in the length of follow-up, variations in cohorts of patients or surgeons, or the use of CDA more broadly vs for cervical myelopathy only; however, it holds that the most conservative conclusion is that CDA does not increase reoperation rates. Overall, given the large size of our study population, this lends further support that CDA is appropriately indicated for very selective use in DCM.
Recent network meta-analysis using data from outside the US primarily further supports the use of CDA for spondylotic myelopathy – not only did CDA patients have better NDI scores, but also the fewest complications compared to ACDF, hybrid surgery, or anterior cervical corpectomy and fusion; but at the cost of increased operation times. 38
A more fundamental concern to widespread adoption of CDA in myelopathy is determination of the underlying pathophysiology– does spinal cord damage occur due to a ‘tethering’ phenomenon whereby the cord is stretched over the degenerative region? or is it the motion itself in the setting of circumferential stenosis that is the primary driver of damage? Both static and dynamic factors are likely contributing to myelopathy. Static factors would include degenerative changes and congenital spinal canal stenosis, ultimately leading to persistent compression and damage to neurons and glia. 39 The cord may also be tethered across the vertebra or intervertebral disc, leading to damage. 40 From a dynamic perspective, there is longitudinal distraction 40 which occur during the cardiac cycle causing oscillations and movement, in turn causing direct damage to the cord. 41 Thus, CDA may be more appropriate if static forces are thought to be causative, and cervical fusion if dynamic forces are prevailing.
Although exceedingly rare, some case reports of worsening myelopathy following CDA have been reported.42,43 While the specific factors in the cause of this rare complication are unclear, this remains an important consideration should patients re-present with myelopathic symptoms.
Limitations
This study is limited by its retrospective nature. There is undoubtedly bias of patient selection driven both by severity of disease and symptoms, comorbidities, surgeon preference and experience with each procedure, and perceived efficacy of the procedure. While we attempted to mitigate selection biases related to patient characteristics via propensity score matching, this remains a limitation. Importantly, the ‘predictors’ identified here for CDA vs ACDF are expert-driven selection criteria, rather than true predictors of success in surgical outcome. Hence, only a more detailed retrospective (or prospective) analysis of patient factors and outcomes for those undergoing CDA is likely to elicit which ‘predictors’ are indicative of surgical success.
Accurate documentation and coding are also critical for this analysis as we relied on ICD-10 and CPT coding for data collection; while there are likely coding inaccuracies in the PearlDiver dataset, we do not anticipate there to be any systematic errors which would greatly affect the outcome of these results. Another limitation of this database study is the inability to determine using ICD/CPT codes whether re-operations were index level revisions, or additional level surgeries.
The findings in this study are further limited by the lack of granular neurological status and exams; one addition would be the modified Japanese Orthopaedic Association (mJOA) score. 44 This could be utilized to stratify patients into mild, moderate, or severe myelopathy, which may impact surgeon’s choice of procedure. Coding limitations precluded evaluation of this in our study due to the lack of an ICD-10 code for severity of myelopathy. Furthermore, the perceived urgency of the procedure (ie, time from consult/contact to surgery) is also a potential confounder. Institutional experience with each technique and access to implants, surgical tools, and vendor-related limitations may also impact surgery choice. As previously stated, there are both international (eg, regulatory), regional (eg, wide variation in US regional utilization), and institutional (eg, private hospitals with greater financial resources) differences in the utilization of CDA. Such factors could be better studied prospectively at the multi-institutional level.
It is also important to consider that arthroplasty is primarily for motion preservation rather than motion restoration. Many of the factors favoring ACDF may also correlate with age to varying degrees, and thus age might serve as a proxy for determining CDA candidacy. Although CDA has lower rates of ASD, it would be important in future studies to ascertain whether this is primarily radiographic ASD or clinical/symptomatic ASD. 45 Similarly, heterotopic ossification may not demonstrate any clinical effects and thus require comprehensive evaluation using additional metrics such as the McAfee-Mehren classification. 46 Future studies will also evaluate the cost effectiveness of CDA vs ACDF. 47 Lastly, it remains critical to focus on long term outcomes, as differences could take as long as 5 years to become evident, as shown by Badhiwala et al. 48
Although our study did not evaluate the cost effectiveness of CDA vs ACDF, several others have attempted to do so, with the overall conclusion that generally CDA is as cost-effective, if not less expensive, than ACDF. To fully determine the cost-effectiveness would go beyond mere insurance claim data, as it would need to include long-term outcomes, including possible reoperations. For example, Qureshi et al 49 determined that if the CDA prosthesis lasts at least 11 years, CDA is more cost-effective than ACDF, assuming a lifetime of 20-year survival and evaluating quality-associated life years (QALYs). Another study used a Markov model to determine the long-term societal cost of CDA vs ACDF for cervical radiculopathy in a 45-65-year-old cohort, and found that CDA was significantly less expensive at $24,199 vs $31,178, permitting that CDA reoperation rates remain under 10.5% (generally reported around 2.5%, and in our study at 4.9%). 50 Similarly, a 5-year cost-effectiveness evaluation of 2-level ACDF vs CDA using a Markov analysis also determined CDR to be more cost-effective using $100,000/QALY willingness to pay, with an incremental cost effectiveness ratio for CDA at $62,133. 51 Lastly, Radcliff et al 52 reviewed the literature on cost-effectiveness for CDA compared to ACDF, and found that based on more recent prospectively collected data on utility scores, costs, and adverse events, CDA remains more cost effective over a time period of 7 years.
Conclusions
4.5% of patients undergoing anterior surgery for degenerative cervical myelopathy underwent CDA in a national population database. The data indicates that reoperation rates were similar when compared to ACDF, yet outcomes were seemingly better with respect to readmissions, complications, and opioid use. Therefore, carefully selected patients, especially those that are healthier, may be good candidates for CDA in cervical myelopathy, consistent with its FDA-approved indications. Application of CDA remains limited to appropriate anatomic and imaging findings, determination of how much motion is contributing to the pathophysiology, and achieving adequate decompression without compromising bone. Thus, not all DCM patients will be candidates for CDA and it is to be used very selectively. However, prospective studies utilizing more granular outcomes measurements would better discern the clinical benefits of CDA over ACDF, with preliminary data indicating CDA patients have no worse outcomes than ACDF patients when appropriately selected.
Supplemental Material
Supplemental Material - Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion in the Treatment of Degenerative Cervical Myelopathy: Patient Characteristics and Surgical Outcomes in a National Administrative Database
Supplemental Material for Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion in the Treatment of Degenerative Cervical Myelopathy: Patient Characteristics and Surgical Outcomes in a National Administrative Database by Charles N. de Leeuw, Won Hyung Andrew Ryu, Jung Yoo, and Josiah N. Orina in Global Spine Journal
Footnotes
Author Note
This material was presented as an oral abstract at the 2023 Annual Meeting of the Congress of Neurological Surgeons in Washington, D.C. on September 12, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.