
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Total disc replacement (TDR) has been introduced in order to preserve segmental motion and thus reduce adjacent segment disease (ASD) as seen after spinal fusion. However, it is uncertain whether these presumed beneficial effects remain. The aim of this study was to evaluate the long-term incidence of ASD and residual-mobility in relation to clinical outcome.
Methods:
A total of 210 patients treated with lumbar TDR for degenerative disc disease were invited for follow-up. ASD was reported in case of severe degeneration in an adjacent disc at latest follow-up, or if an increase in disc degeneration was observed in these adjacent segments as compared to direct postoperative radiographs. Residual-mobility of the TDR was defined as a minimal rotation of 4.6° on flexion-extension radiographs. Patient-reported outcome measures were obtained.
Results:
Fifty-seven patients (27.1%) were lost to follow-up. In 32 patients (15.3%) a revision by spinal fusion had been performed. In 20 patients this revision had occurred ≥5 years after TDR and were included. Consequently, 141 patients were available for analysis (mean follow-up of 16.7 years). Residual-mobility was noted in 38.0%. No significant associations were observed between residual-mobility and the occurrence of ASD, or with clinical outcome. In addition, ASD and clinical outcome were not related either.
Conclusions:
It appears that long-term preservation of motion after TDR is met for only a third of patients. However, residual-mobility is not associated with the occurrence of ASD, and both residual-mobility and ASD do not appear to be related to long-term clinical outcome.
Introduction
Fusion of a symptomatic lumbar spinal motion segment is the most commonly used operative treatment for patients with degenerative disc disease (DDD), unresponsive to nonoperative care. 1 Total disc replacement (TDR) has been introduced in order to preserve motion at the affected level and mimic the morphology of the intervertebral disc, 2,3 aiming to prevent the occurrence of adjacent segment disease (ASD) as seen after lumbar fusion, and thus a presumably better long-term outcome. 4 -7
The predicted reoperation rate of ASD after spinal fusion ranges between 9.9% and 22.2% at 10-year follow-up. 4,6,7 Studies reporting on the incidence of ASD after TDR with a minimal follow-up of at least 10 years are scarce. Those available report an incidence of ASD as determined on plain radiographs of the lumbar spine between 2% and 17% at mean follow-up of 10 to 17.3 years. 8 -10 A systematic review by Wang et al 11 showed a pooled risk of clinical ASD that needed revision surgery of 1.2% and 7.0% in the TDR and fusion groups, respectively, after maximum of 5 years follow-up. A randomized controlled trial of Zigler et al, 12 comparing TDR with lumbar fusion, indicated that TDR has a protective effect against ASD, 5 years after the index surgery.
Multiple studies with a follow-up of 2 to 11 years have shown that range of motion (ROM) was preserved or even improved after TDR. 3,9,10,13 None of these studies evaluated residual-mobility in relation to the occurrence of ASD and clinical outcomes.
The purpose of this study was to evaluate residual-mobility and the long-term incidence of ASD after TDR. Additionally, an assessment was made whether ASD and residual-mobility were related to clinical outcome.
Methods
Patient Selection
The current study was approved by the medical ethics committee METC-Z (16-N-22) and registered at the Dutch Trial Registry (NTR5710). The medical records of all patients who received a lumbar TDR using an SB Charité III between 1994 and 2000 at the Zuyderland Medical Centre, Sittard, the Netherlands, were reviewed.
TDR had been performed for the treatment of patients with lumbar DDD causing predominant axial low back pain. Nerve root compression and/or spinal stenosis was considered as a contraindication for TDR. Preoperatively, all patients had undergone fluoroscopically guided provocation discography to confirm a painful disc. No facet joint injections were performed. Patient characteristics are listed in Table 1.
Summary of Subgroup Patient Demographic and Surgical Data.
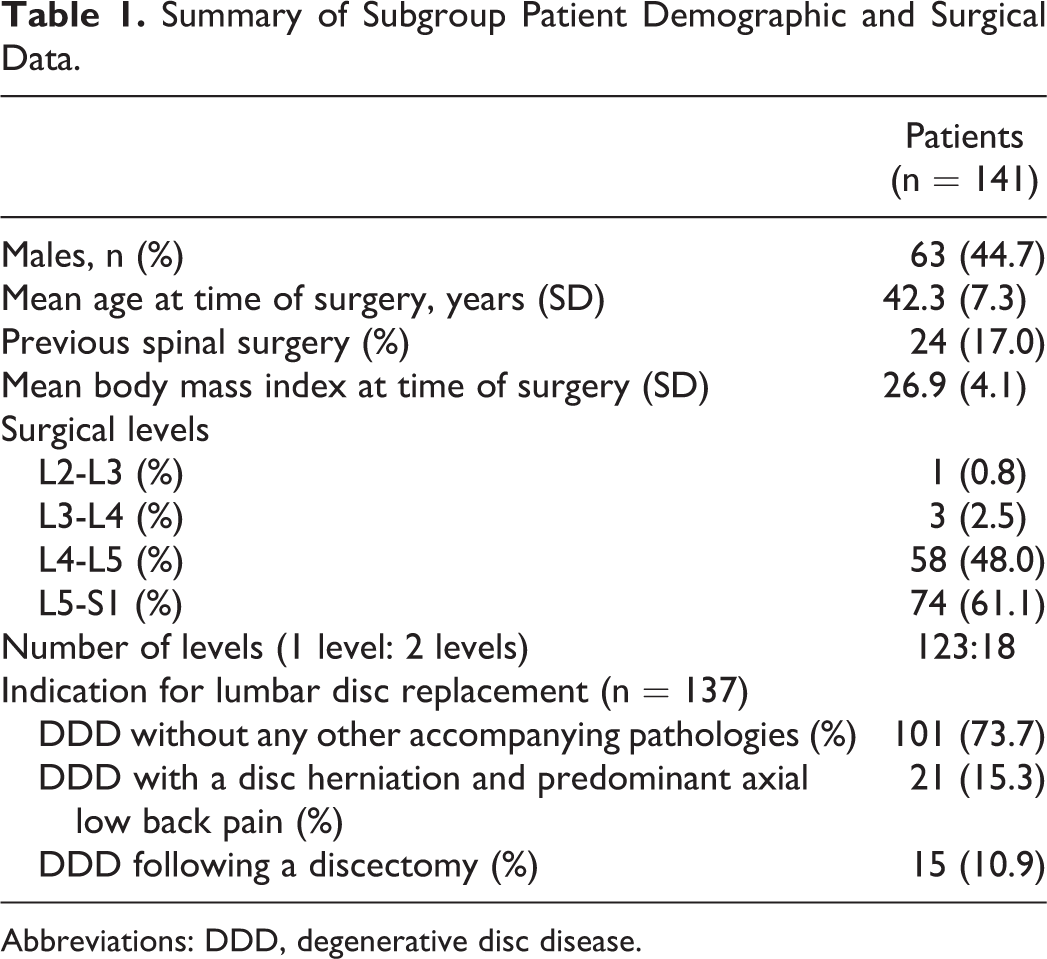
Abbreviations: DDD, degenerative disc disease.
Radiological Analysis
The radiographic grading system of Wilke et al 14 was used to determine the degree of intervertebral disc degeneration (Figure 1). This grading system covers 3 radiographic signs of disc degeneration: “height loss,” “osteophyte formation,” and “diffuse sclerosis.” On standing anteroposterior and lateral radiographs these 3 variables were graded individually on a scale from 0 to 3. Based on the sum of these 3 scores, the overall degree of degeneration was assigned to each disc on a 4-point scale from grade 0 (no degeneration, 0 points) to grade 3 (severe degeneration, 7-9 points). 14
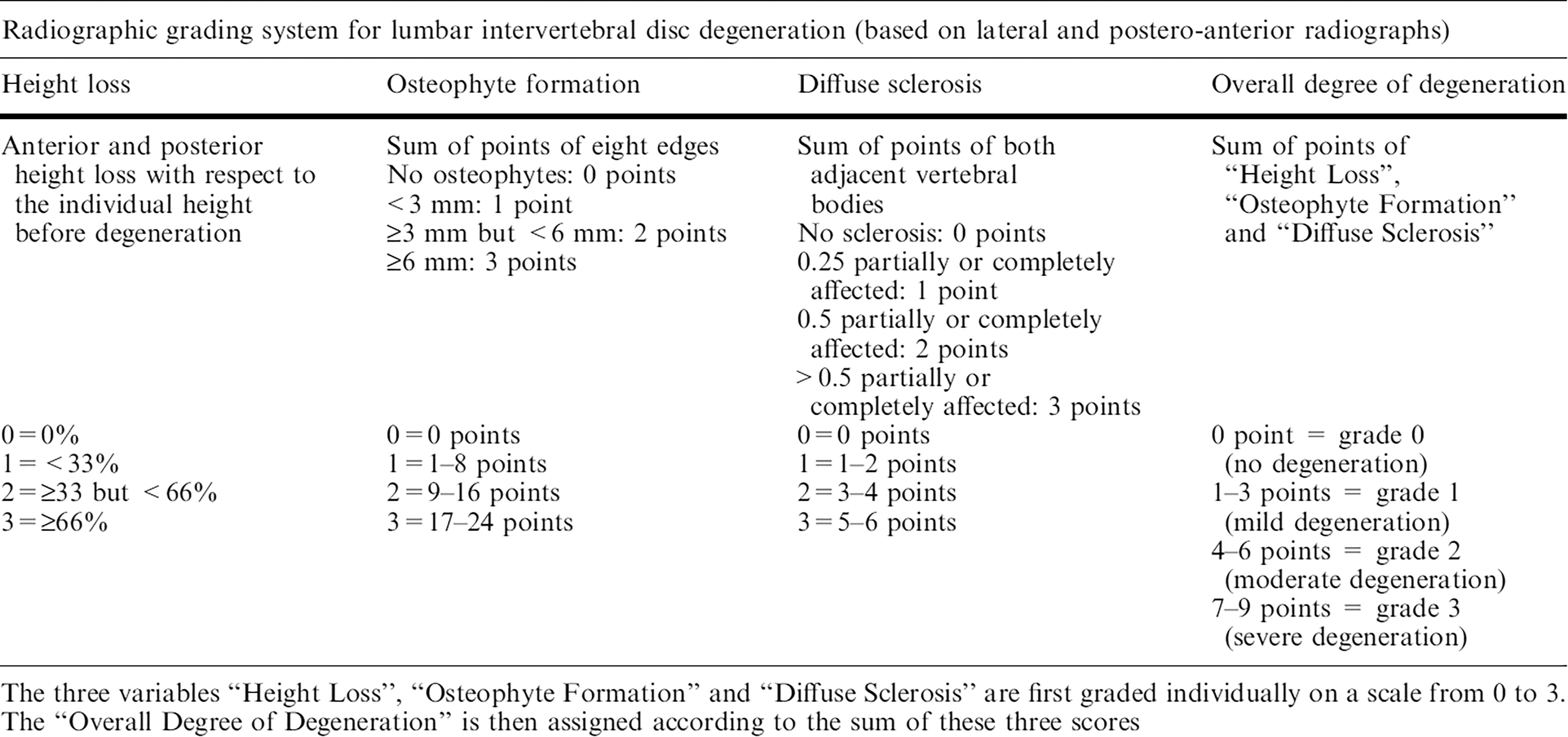
Radiographic grading-system by Wilke et al 14 to determine the degree of intervertebral disc degeneration.
Patients were considered to have developed ASD if in one or more adjacent segments of the TDR a grade 3 disc degeneration was observed at latest follow-up (ASD-static). We confirmed that this grade 3 disc degeneration was not already present in the same segment at the direct postoperative radiographs. We also considered ASD to be present if an increase of 3 or more points was observed in the same adjacent segment when the direct postoperative radiographs were compared with those at latest follow-up (ASD-dynamic).
The Cobb method was used to calculate the sagittal alignment angles of the TDR in the flexion and extension radiographs. 15 A kyphotic angle was assigned a negative value, lordosis a positive value. According to a study by Lim et al, 15 it appears that in order to be sure with 95% certainty that a TDR has any sagittal motion, a ROM of at least 4.6° should be observed on standard flexion-extension lumbar spine radiographs. Consequently, residual-mobility was defined as a minimal change of 4.6° in the sagittal alignment angles. We used the method of Punt et al 16 to quantify radiographic subsidence in the current population.
Finally, the pelvic incidence (PI) was measured on the lateral radiographs. All measurements were performed by 2 independent observers, who were not involved in patient care (JK, TV). Mean values of their measurements were calculated. The interclass correlation coefficient was used to quantify agreement between the 2 observers.
Clinical Outcome Evaluation
Patient-reported outcome measures (PROMs) were obtained from all patients at their follow-up visit to the outpatient clinic. Back-pain and leg-pain intensity was recorded with a Visual Analogue Scale (VAS; 0 to 100 100 being “worst pain”). General and functional well-being was evaluated using the Short Form-36 survey (SF-36) and Oswestry Disability Index (ODI), respectively. In both a score of 0 is equivalent to no disability, and a score of 100 is equivalent to maximum disability. Quality of life was assessed using the EuroQol-5D (EQ-5D; 0 to 1, 1 indicates the best health state). Finally, patients were assigned to a success or failure group: A revision by spinal fusion or a reported VAS pain score ≥50 was classified as failure. 17
Data Analysis and Statistics
Baseline patient characteristics were described using mean and standard deviation or absolute number and percentage. The independent t test was used to test for differences in the means of radiological parameters and clinical outcome scores between patients with or without residual-mobility or ASD. Differences in categorical variables in the same groups were tested using the χ2 test. A multivariable logistic regression model was utilized to identify if there is an independent association between the occurrence of residual-mobility and ASD. Confounding variables that were used for the multivariable analysis are those listed in Table 1. Confounding variables were determined a priori, not by means of statistical testing. Corresponding estimates of adjusted odds ratios (OR) and 95% confidence intervals (CIs) were obtained. A P value of <.05 was considered statistically significant. All analyses were performed using IBM SPSS (Version 23.0).
Results
Study Population
Altogether 226 patients with a TDR were identified, and 16 patients had deceased (7.1%). The remaining 210 patients were contacted by mail and subsequently by phone, with the request to visit our outpatient clinic. A total of 57 patients (27.1%) could not be retrieved. In 32 patients a revision by spinal fusion had been performed prior to our study. We only included patients if the revision had occurred at least 5 years after the initial TDR, to be able to report on changes in the adjacent levels at long-term follow-up (n = 20, range 5-22 years). Consequently, 141 patients (67.1%) were included for analysis. Informed consent was acquired from all patients. A flowchart of the included and excluded patients is shown in Figure 2.
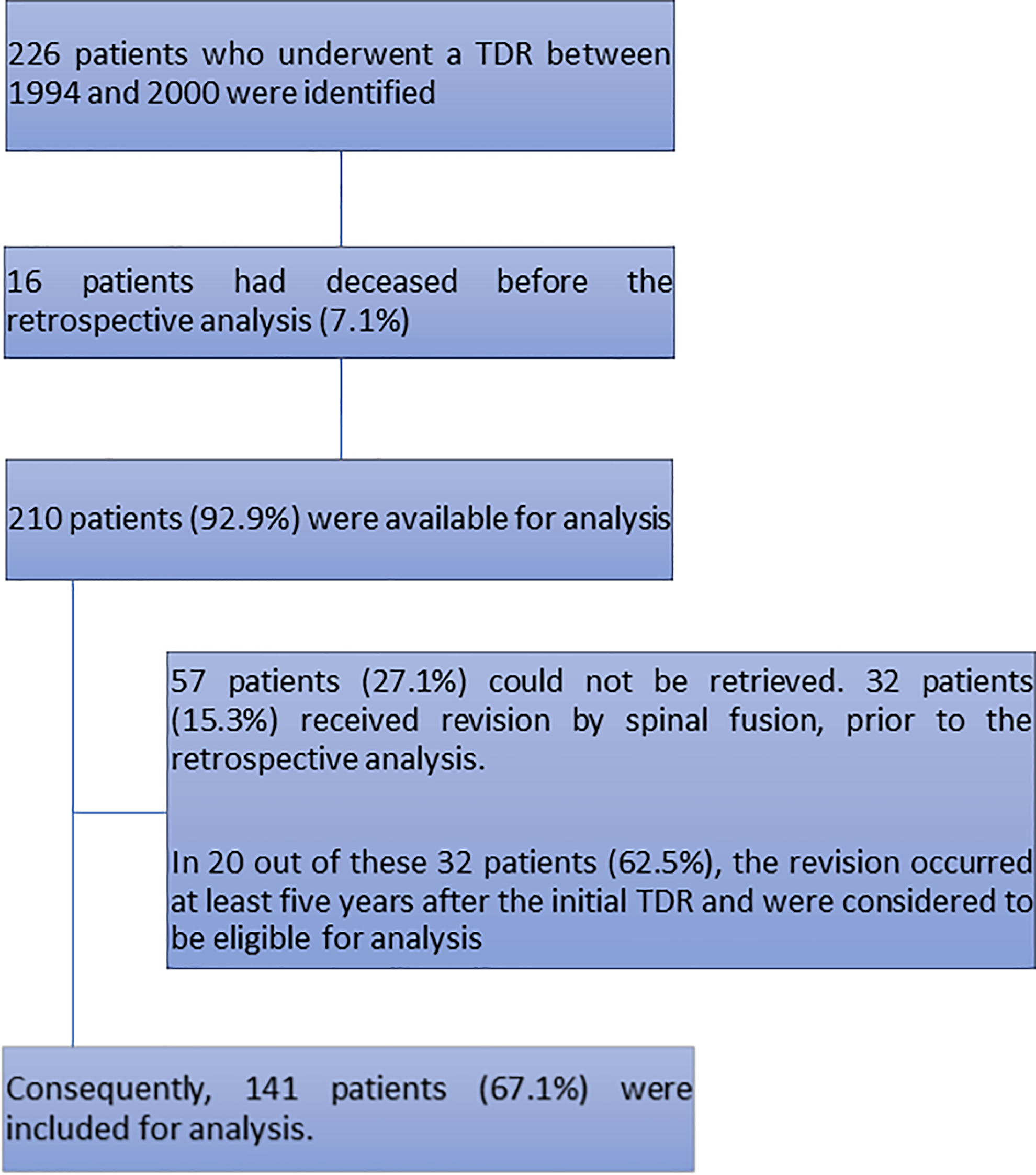
Reasons for exclusion.
Mean follow-up after implantation for the 121 TDR patients without revision fusion was 16.7 years (median 16.5, range 13.6-23.0 years). In 15 patients a TDR had been placed at 2 or more levels. In 18 out of the 121 patients without a revision, the direct postoperative radiographs were not available. In addition, patients with a revision by spinal fusion were eligible for analysis if both the radiographs direct postoperative and before their spinal fusion were available (n = 8). Consequently, in 111 patients the development of ASD after TDR could be determined.
Incidence of Residual-Mobility and ASD
As shown in Table 2, only 46 out of 121 TDR patients (38.0%) had a residual-mobility of ≥4.6° at latest follow-up. The mean ROM in the present study was 4.3° (range: 0° to 15.6°). High interclass correlation coefficients between the 2 observers were found (R ≥ 0.899, P < .01). In 55 patients a grade 3 disc degeneration (7-9 points) was scored in one or both the adjacent levels at latest follow-up. In 4 patients this degeneration was already present, in the same adjacent level on the direct postoperative radiographs. Consequently, ASD-static occurred in 51 out of 107 patients (47.7%, one level n = 38, both levels n = 13). As to ASD-dynamic, in 28 out of the 111 patients (25.2%) an increase of 3 or more points in one (n = 14) or both (n = 14) of the same adjacent segments was observed. No significant differences were seen for the occurrence of residual-mobility and ASD when the results were corrected for monosegmental versus bisegmental TDR.
Patient Characteristics in Relation to Residual-Mobility.
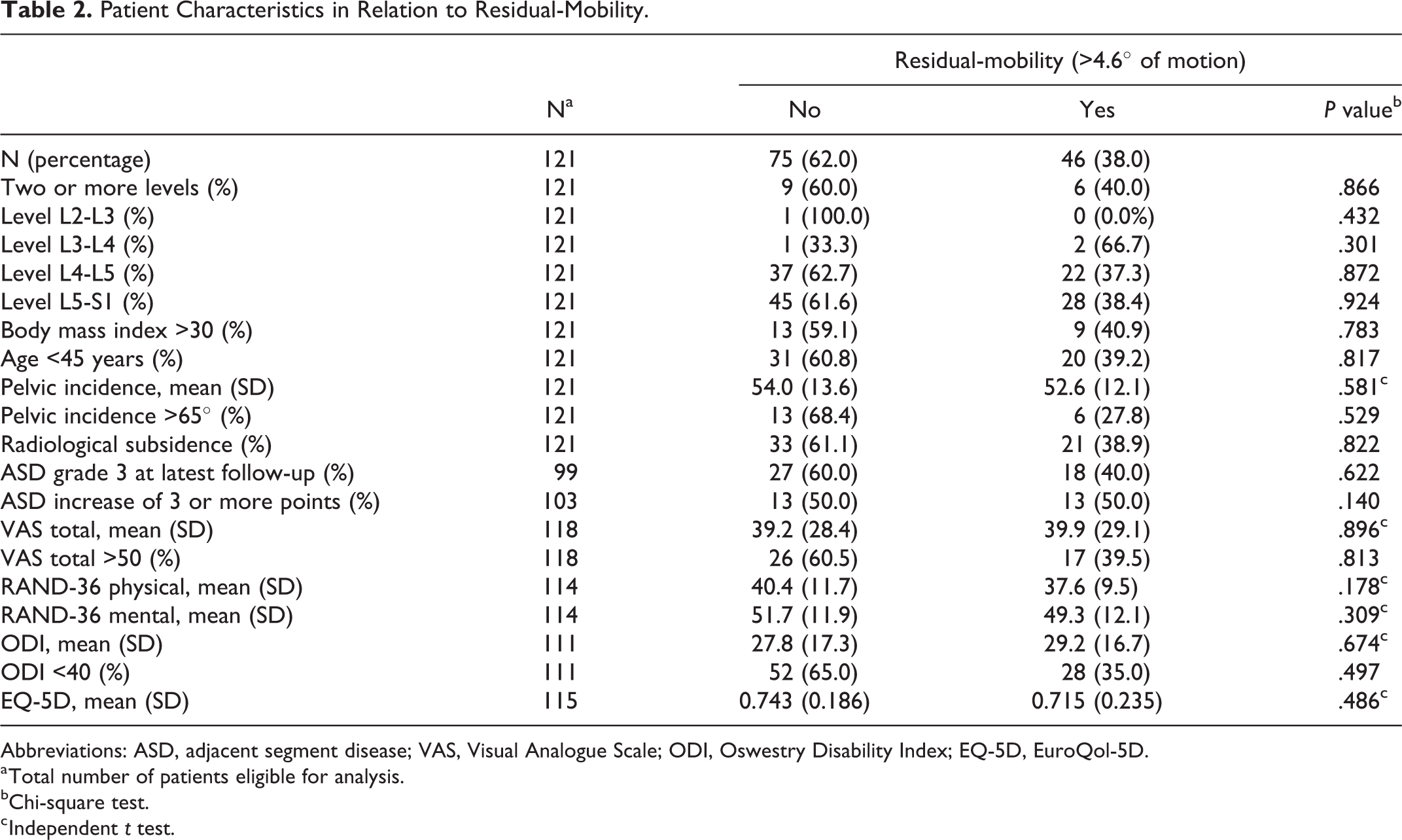
Abbreviations: ASD, adjacent segment disease; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; EQ-5D, EuroQol-5D.
a Total number of patients eligible for analysis.
bChi-square test.
c Independent t test.
Residual-Mobility Versus Patient Characteristics, ASD, and Clinical Outcome
No significant associations were found between the different patient- or procedure-related characteristics such as the level of placement or multilevel TDR, and the occurrence of residual-mobility (Table 2). Additionally, no significant associations were found for the VAS, SF-36, EQ-5D, or ODI score and the occurrence of residual-mobility. Finally, no significant changes were observed when the occurrence of residual-mobility and those of ASD-static or ASD-dynamic were compared. The latter was confirmed in a multivariable logistic regression analysis, with an OR of 0.85 (CI 0.34-2.08, P = .713) for ASD-static and 0.46 (CI 0.17-1.21, P = .113) for ASD-dynamic (Table 3). All potential confounders were included in the analysis, besides a TDR at L2-L3 or L3-L4 because of too few events to estimate the OR.
Multivariable Logistic Regression Model Between the Occurrence of Residual-Mobility and ASD With Potential Confounders.
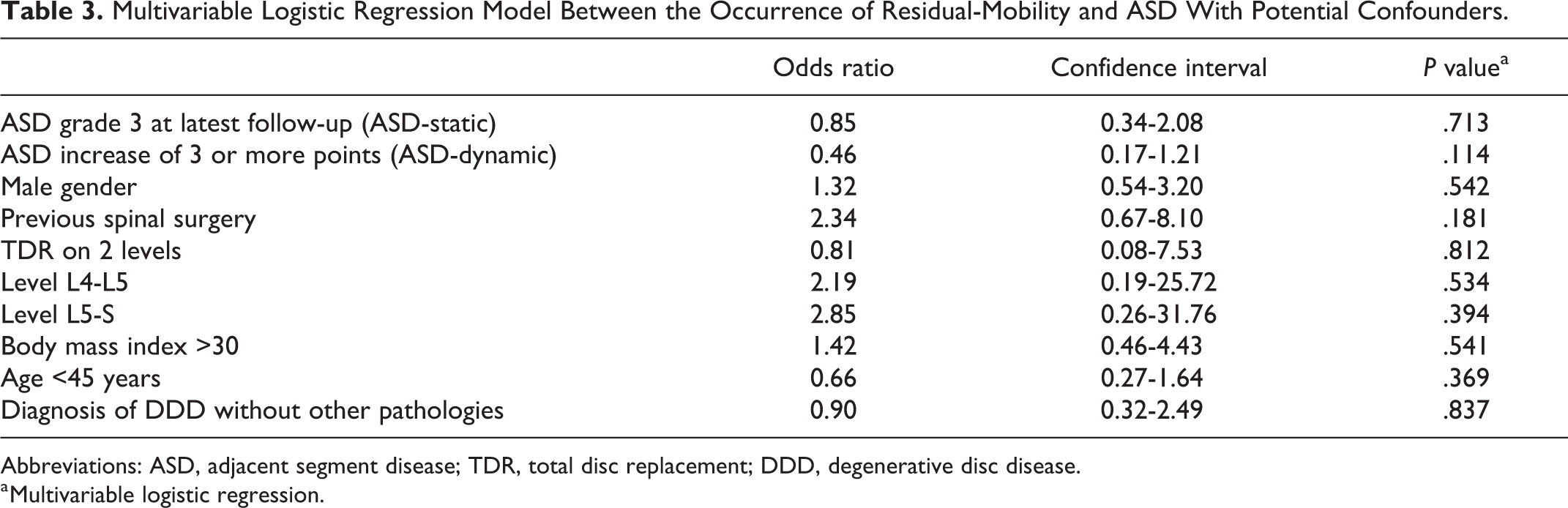
Abbreviations: ASD, adjacent segment disease; TDR, total disc replacement; DDD, degenerative disc disease.
a Multivariable logistic regression.
As previously mentioned, a sagittal motion of at least 4.6° should be observed, in order to be sure with 95% certainty that a TDR has any ROM. However, this does not exclude motion in those patients who do not meet this threshold. If we look more closely to these patients, their median sagittal motion is 2.2°. If this value is applied as a cutoff for ankylosis, 50.3% of the patients without residual-mobility may have some degree of motion. Therefore, we adjusted the threshold for residual-mobility (4.6°) in steps of 0.5° from 0 to the maximum measured sagittal ROM, to test if this affected our results. Similarly, no significant associations were observed between the different thresholds for residual-mobility and the occurrence of ASD or clinical outcome.
ASD Versus Patient Characteristics, Pelvic Incidence, and Clinical Outcomes
As for residual-mobility, we found no significant associations between the different patient- or procedure-related characteristics and the occurrence of ASD-static or ASD-dynamic (Table 4). Remarkably, in all 4 TDRs that were placed at a level cranial of L4-L5, ASD-static was observed (n = 4, P = .025). Pelvic incidence was not significantly associated with the occurrence of ASD. No significant associations were found for the VAS, SF-36, EQ-5D, or ODI score and the occurrence of ASD-static or ASD-dynamic (Table 4). Finally, no significant differences were found between the success and failure group for the occurrence of ASD-static or ASD-dynamic (Table 5).
Patient characteristics in relation to ASD.
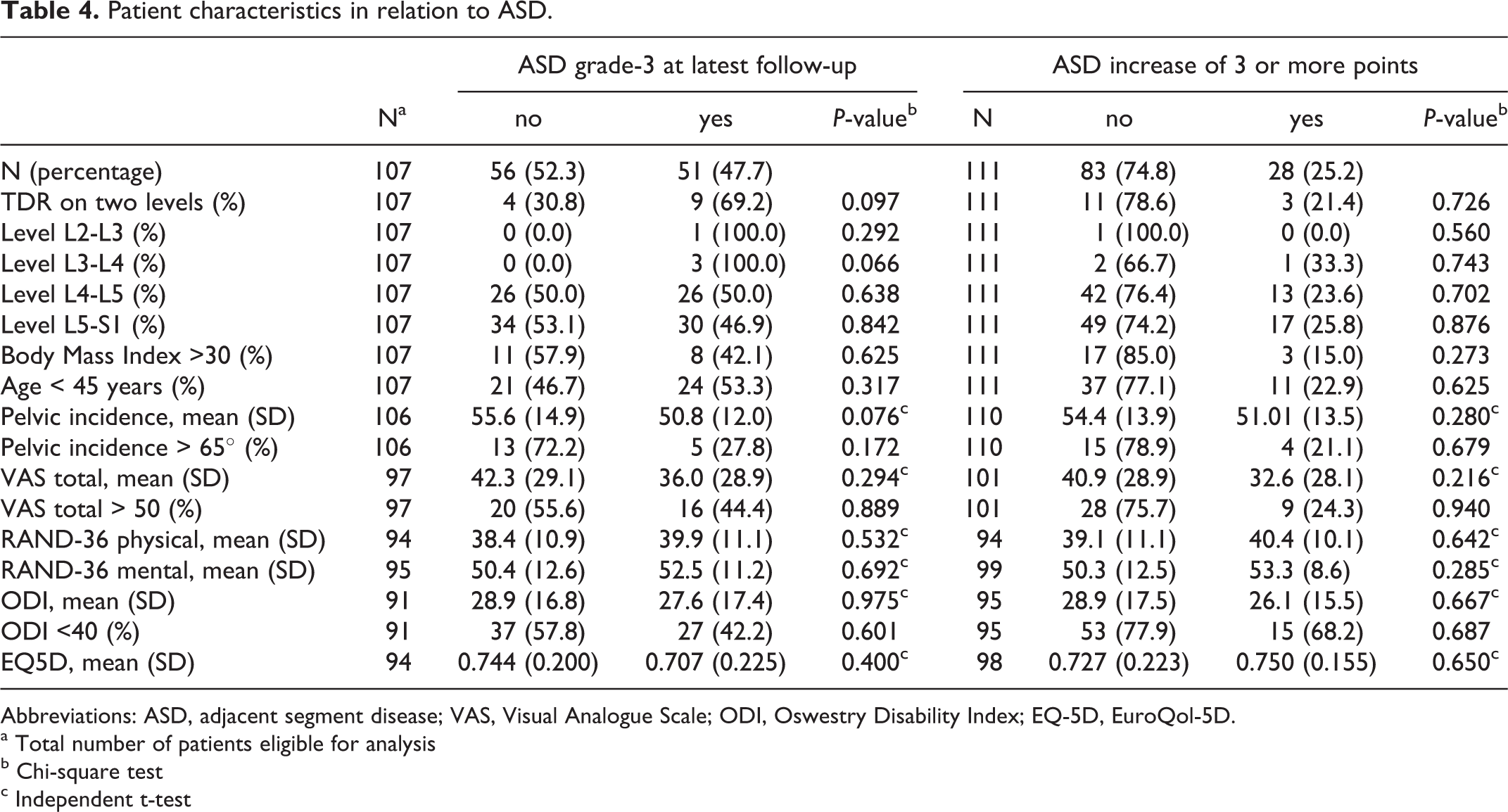
Abbreviations: ASD, adjacent segment disease; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; EQ-5D, EuroQol-5D.
a Total number of patients eligible for analysis
b Chi-square test
c Independent t-test
Patient Characteristics and the Occurrence of ASD in Relation to the Success and Failure Groups.
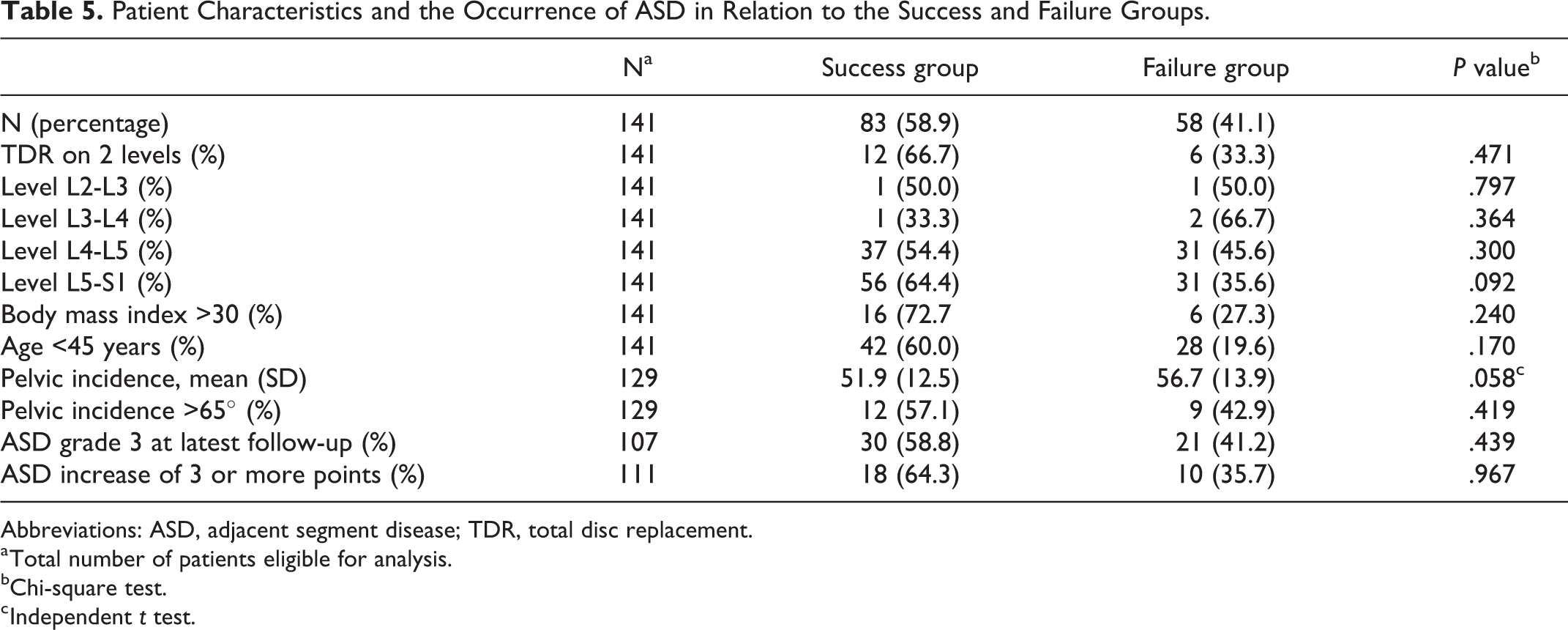
Abbreviations: ASD, adjacent segment disease; TDR, total disc replacement.
a Total number of patients eligible for analysis.
bChi-square test.
c Independent t test.
Discussion
This study represents a long-term follow-up of patients who received a lumbar TDR for the treatment of symptomatic DDD. Residual-mobility was noted in one third of our patients at latest follow-up. No significant associations were observed between residual-mobility and the different patient- or procedure-related characteristics, clinical outcomes, or the occurrence of ASD. We found no significant associations between ASD and clinical outcomes.
Incidence of Residual-Mobility and ASD
The number of long-term follow-up studies addressing the occurrence of residual-mobility after TDR is limited. 3,9,10,13 These studies reported a mean ROM between 7.7° and 10.3° at latest follow-up (mean 10-12 years). However, none of these studies defined residual-mobility. In the present study residual-mobility (ROM > 4.6°) at the index level of the TDR was found in only 38.0% of the patients (n = 46). The mean ROM was 4.3°, which is slightly lower than in the other studies, but may be explained by the fact that our follow-up duration was longer. In studies where ROM was monitored over time, a gradual decline of the device mobility was noted. 13,18 This, however, did not negatively affect the patient’s clinical outcomes in these studies. In the current study, the ROM was only available at latest follow-up.
Studies with long-term follow-up of lumbar TDR (mean 10-17.3 years) report an incidence of ASD-static as determined on plain radiographs between 2% and 17%. 8 -10 A prospective study by Meir et al 19 with a mean follow-up of 9 years (range 8-11 years) reported an incidence of ASD-static on magnetic resonance imaging of 68%. Based on plain radiographs we found an incidence of ASD-static of 47.7%, which seems consistent with the study of Meir, although not with the other studies. This could possibly be explained by the fact that these studies did not use a standardized scoring system for ASD. We used the grading system of Wilke et al, 14 who compared the radiographic scoring of DDD with the macroscopic grade of DDD and reported a kappa value of 0.713. Furthermore, the incidence of radiographic ASD seems to increase when long-term studies 8 -10,19 are compared with short-term studies. 12,20 However, this could also be part of the natural aging process. Two studies by Zigler et al showed that the risk of dynamic-ASD following TDR is significantly lower when compared with spinal fusion at 5-year follow-up. 12,20 However, the appearance of ASD does not seem to significantly increase revision surgery or deteriorate clinical outcome in these studies. 12,20
Residual-Mobility Versus Patient Characteristics, ASD, and Clinical Outcomes
In the present study, the different patient- or procedure-related characteristics did not have any influence on the occurrence of residual-mobility. To our knowledge only the retrospective study of Huang et al 21 reported an association between residual-mobility and clinical outcomes. In that study, patients (n = 32) with a residual-mobility of >5° had clinically modest but statistically significant lower ODI scores after a mean follow-up of 8.7 years. Our results showed no significant relationship between the occurrence of residual-mobility and the occurrence of ASD. This is similar to the results reported in the prospective study of Siepe et al 22 (n = 91) and a randomized controlled trial by Zigler et al 12 (n = 261), both with 4 to 5 years of mean follow-up.
Biomechanical studies have shown that the movement of a TDR differs from that of a normal disc in an intact spine. 23,24 These studies described an increase in rotational mobility at the index TDR level. Furthermore, in a study of Nunley et al 25 pressure effects on adjacent level discs after 2-level constructs, that is, fusion, hybrid, and TDR were compared. No significant differences were found between the different stabilization procedures. So maybe not so much the extent of motion (in degrees), but rather the quality of motion is the main factor in the occurrence of ASD.
Other biomechanical studies have demonstrated increased facet pressure and altered loading patterns with more sudden rather than gradual load increase in the facet joints after TDR. 26,27 It is not possible to make a reliable assessment of facet joint degeneration (FJD) on plain radiographs. Therefore, we could not investigate a possible association between FJD and the occurrence of residual-mobility or clinical outcome. Siepe et al 22 reported a significant increase of FJD at the index level after TDR and a significant decrease in ROM at the same level. The occurrence of FJD was associated with significantly lower VAS and ODI scores. This may explain why in our study, as in many other studies, 12,20,22 no significant associations were found between ASD and clinical outcome. FJD might be a stronger factor influencing clinical outcomes after TDR than ASD.
Study Limitations and Strengths
The current study’s main limitation is its retrospective nature. We were only able to report on the changes in residual-mobility and ASD between directly postoperative and at latest follow-up. TDR has been introduced in order to preserve motion and thus prevent or decrease the occurrence of ASD as seen after lumbar spinal fusion. 4 -7 Our study lacks a control group so evidently no direct comparison between TDR and fusion or between TDR and conservative treatment regarding the occurrence of ASD could be made.
We are aware that the radiographic measurements of residual-mobility are prone to error and a cutoff value of 4.6° may seem arbitrary. 15 However, a sensitivity analysis with different cutoff values led to the same results. To determine the degree of intervertebral disc degeneration, the standardized and validated radiographic grading system of Wilke et al 14 was used in order to obtain reproducible and accurate values.
We included 141 patients, which is more than in previously published long-term follow-up studies reporting on ASD or residual-mobility after TDR. 3,9,10,13 Our mean follow-up of 16.7 years is the longest available in the current literature on this subject and this might explain the substantial number of patients who were lost to follow-up, mainly due to patients who had died or could not be retrieved.
Conclusions
It appears that the initial goal of TDR, that is, long-term preservation of motion, is met for only one third of our patients. Residual-mobility is not associated with the occurrence of ASD. Both residual-mobility and ASD seem unrelated to long-term clinical outcome.
Footnotes
Authors’ Note
The current study was approved by the Medical Ethics Committee METC Z (16-N-22) and registered at the Dutch Trial Registry (NTR5710). Informed consent was acquired from all patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.