
Abstract
Study Design
Retrospective cohort analysis.
Objective
Identify demographic and clinical predictors for revision discectomy and compare postoperative complications between primary microdiscectomy (MD) and revision discectomy.
Methods
Patients who underwent one-level primary lumbar MD and subsequent one-level revision discectomy for lumbar disc herniation were identified using the PearlDiver national database. Multivariate regression analysis was performed to identify predictors of revision discectomy, assess 30-day postoperative complications and opioid use, and assess the likelihood of future lumbar fusion.
Results
Of 52,310 patients undergoing primary lumbar MD, 4536 (7.98%) required revision. Independent predictors included smoking (aOR: 1.72), obesity (aOR: 1.44), lateral disc herniation (aOR: 1.69), coagulopathies (aOR: 1.34), CAD (aOR: 1.62), anemia (aOR: 1.38), diabetes (aOR: 1.47), hypertension (aOR: 1.63), peripheral vascular disease (aOR:1.33), preoperative opioid use (aOR: 2.06), postoperative opioid use (aOR: 1.80), and depression (aOR: 1.73) (all, P < 0.01). Revision discectomy was associated with higher risks of infection (aOR: 1.78), AKI (aOR: 1.41), VTE (aOR: 1.46), dehiscence (aOR: 2.32), neurological injury (aOR: 1.48), durotomy (aOR: 2.19), epidural hematoma (aOR: 2.61), I&D (aOR: 2.32), opioid use (aOR: 1.73), and increased fusion rates (all P < 0.05).
Conclusion
Several patient-related factors increase the risk of revision MD, which is associated with additional short- and long-term complication risks relative to the index procedure. These findings inform expectations for disease progression and postoperative outcomes in revision MD. Revision discectomy should be avoided when possible.
Keywords
Introduction
Lumbar microdiscectomies constitute a principal treatment strategy for management of lumbar disc herniations, representing the most commonly utilized spine procedure within the United States (US). 1 Although highly efficacious, a subset of patients incur disc reherniations postoperatively, a proportion of which require additional surgery.2,3 While previous literature has sought to identify potential modifiable risk factors which may be implicated in greater reherniation risks such as smoking and increased body mass index (BMI), predictors for undergoing revision discectomy along with their unique risk profiles are less clearly defined.4-6
Nonetheless, patients undergoing revision procedures are generally predisposed to suboptimal outcomes given the inherent challenges assumed with postoperative scarring and adhesions. Impaired visualization arising from post-surgical anatomy inherently increases the risk of intraoperative complications such as dural tears and nerve root injuries, which subsequently extends operative duration, hospital length of stay (LOS), and postoperative narcotic use.7,8 While these risks are commonly assumed with revision surgery overall, complications specific to undergoing revision discectomy warrant further investigation to help inform the selection of optimal management strategies in consideration of patients’ individualized clinical presentations.
Therefore, the current study utilizes a large national database to comprehensively characterize the demographic and clinical features of patients who underwent primary lumbar microdiscectomy (MD), along with those subsequently treated with revision discectomy for lumbar disc reherniation. In doing so, the present analysis aims to (1) identify independent predictors for requiring revision discectomy, and to (2) compare the postoperative complication profiles between primary MD and revision discectomy.
Methods
Patients who underwent one-level primary lumbar microdiscectomy (MD) and one-level revision discectomy between 2010 and Q3 of 2022 (January to October 2022) were identified using the PearlDiver Mariner Database (PearlDiver Technologies, Fort Wayne, IN). This database comprises over 41 billion HIPAA-compliant inpatient and outpatient records across the United States, encompassing data on patient demographics, diagnoses, and procedures from both major private and public insurance providers. Relevant demographic and procedural data for patients undergoing primary lumbar MD and revision discectomy were collected using International Classification of Disease, 9th and 10th edition (ICD-9 and ICD-10) and Current Procedural Terminology (CPT) codes. Lumbar microdiscectomies were defined using CPT codes for open discectomies (CPT-63030) with CPT-69990 to denote use of a surgical microscope, to ensure this cohort strictly included microdiscectomies rather than open discectomies, as equivalent code sets are commonly used to document both procedures in clinical practice in association with insurance reimbursement policies. 9 Revision discectomies were separately defined using CPT-63042. ICD codes were then used to identify patients who underwent microdiscectomy for a diagnosis of disc herniation or disc degeneration. Exclusion criteria for this study included two-level discectomy and patients with surgical indications for cauda equina syndrome, trauma, infection, or malignancy. Informed consent and institutional review board (IRB) approval were not required as all patient data for this study was de-identified.
Statistical Analysis
Differences in patient demographics and comorbidities were assessed using Chi-squared test for categorical variables and the student’s t-test for continuous variables. Demographic characteristics are presented as means ± standard deviation (SD) for continuous variables and proportions for categorical variables.
Multiple logistic regression was utilized to identify independent predictors for revision discectomy while accounting for confounding variables, including age, gender, and Elixhauser Comorbidity Index (ECI). Predictors assessed included age, gender, ECI, tobacco use, obesity, lateral disc herniation, alcohol abuse, coagulopathy, coronary artery disease (CAD), anemia, dementia, depression, diabetes, hypertension, peripheral vascular disease (PVD), pre-operative opioid use, and post-operative opioid use.
A similar model that additionally controlled for tobacco use was then utilized to assess risk of 30-day postoperative complications and opioid use, and lumbar fusion surgery up to 10 years postoperatively. Complications included infection, acute kidney injury (AKI), venous thromboembolism (VTE), dehiscence, neurological injury, durotomy, epidural hematoma, and the need for incision and drainage (I&D). All statistical analyses were conducted with Rstudio (Version 4.4.2). A P-value less than 0.05 was considered statistically significant.
Results
Patient Demographics and Clinical Features
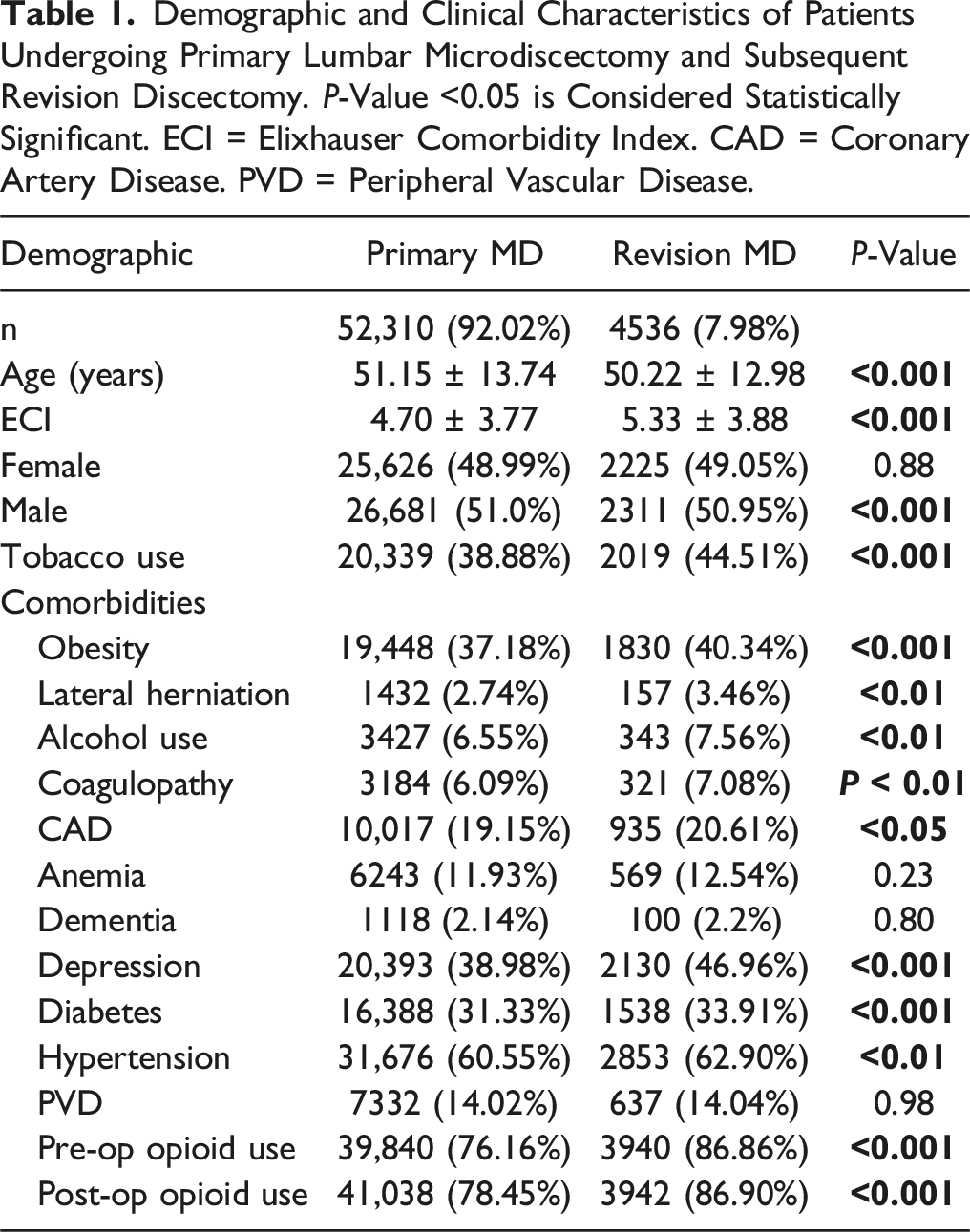
Demographic and Clinical Characteristics of Patients Undergoing Primary Lumbar Microdiscectomy and Subsequent Revision Discectomy. P-Value <0.05 is Considered Statistically Significant. ECI = Elixhauser Comorbidity Index. CAD = Coronary Artery Disease. PVD = Peripheral Vascular Disease.
Predictors of Revision Discectomy
Univariate and Multivariate Analyses of Risk Factors for Revision Discectomy. Covariates Include Age, Gender, and ECI. P-Value <0.05 is Considered Statistically Significant. ECI = Elixhauser Comorbidity Index. CAD = Coronary Artery Disease. PVD = Peripheral Vascular Disease.
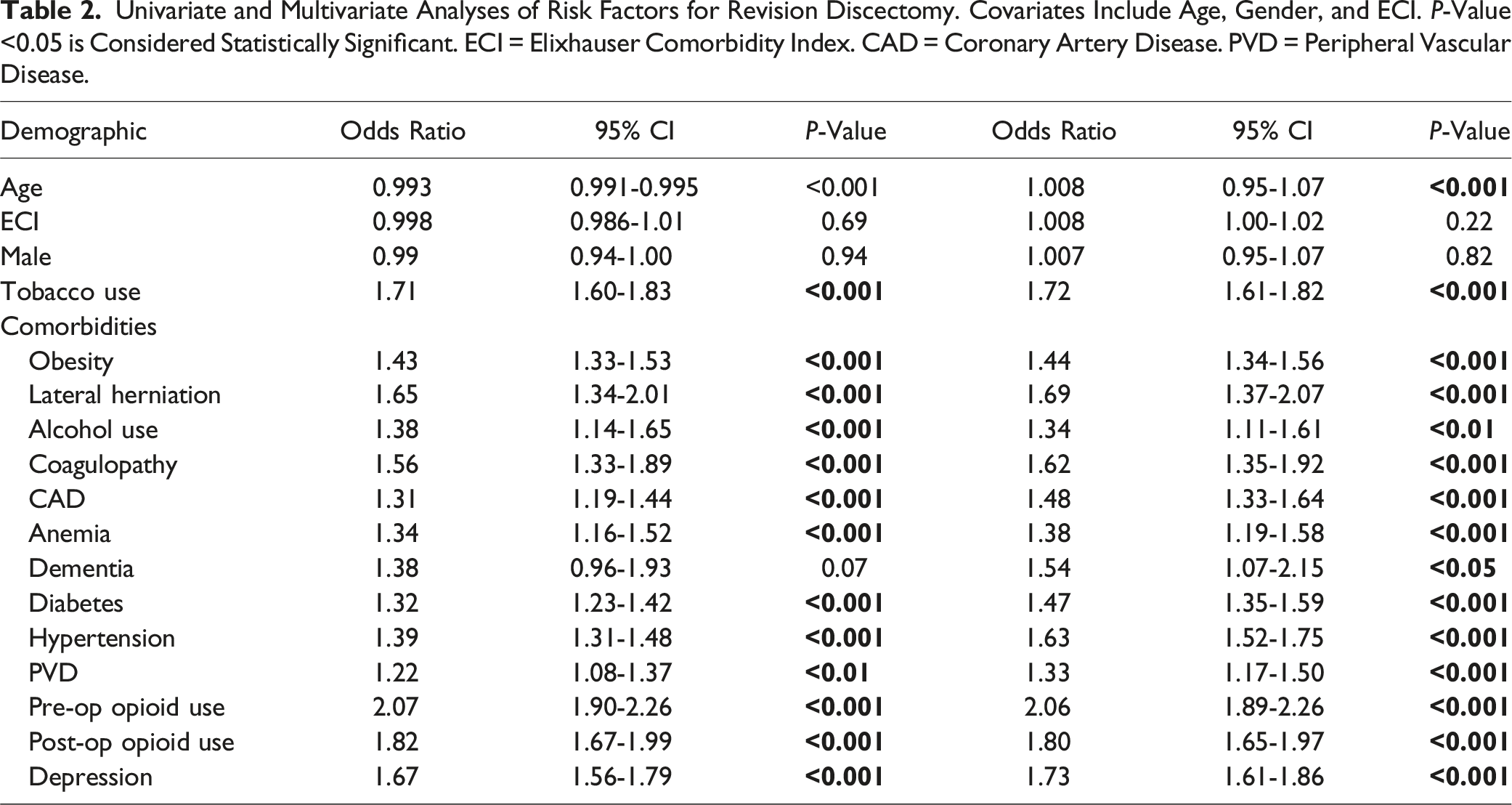
Multiple logistic regression subsequently identified the following predictors: smoking (aOR: 1.72 [1.61-1.82]), obesity (aOR: 1.44 [1.34-1.56]), alcohol use (aOR: 1.34 [1.11-1.61], P < 0.01), lateral herniation (aOR: 1.69 [1.37-2.07]), alcohol use (aOR: 1.34 [1.11-1.61]), coagulopathies (aOR: 1.62 [1.35-1.92]), CAD (aOR: 1.48 [1.33-1.64]), anemia (aOR: 1.38 [1.19-1.58]), dementia (aOR: 1.54 [1.07-2.15], P < 0.05), diabetes (aOR: 1.47 [1.35-1.59]), hypertension (aOR: 1.63 [1.52-1.75]), PVD (aOR: 1.33 [1.17-1.50]), preoperative opioid use (aOR: 2.06 [1.89-2.26]), postoperative opioid use (aOR: 1.80 [1.65-1.97]), and depression (aOR: 1.73 [1.61-1.86]) (all P < 0.001 unless otherwise specified) (Table 2). Corresponding odds ratios for each demographic and clinical features are illustrated as a forest plot in Figure 1. Forest plot of predictors of revision discectomy.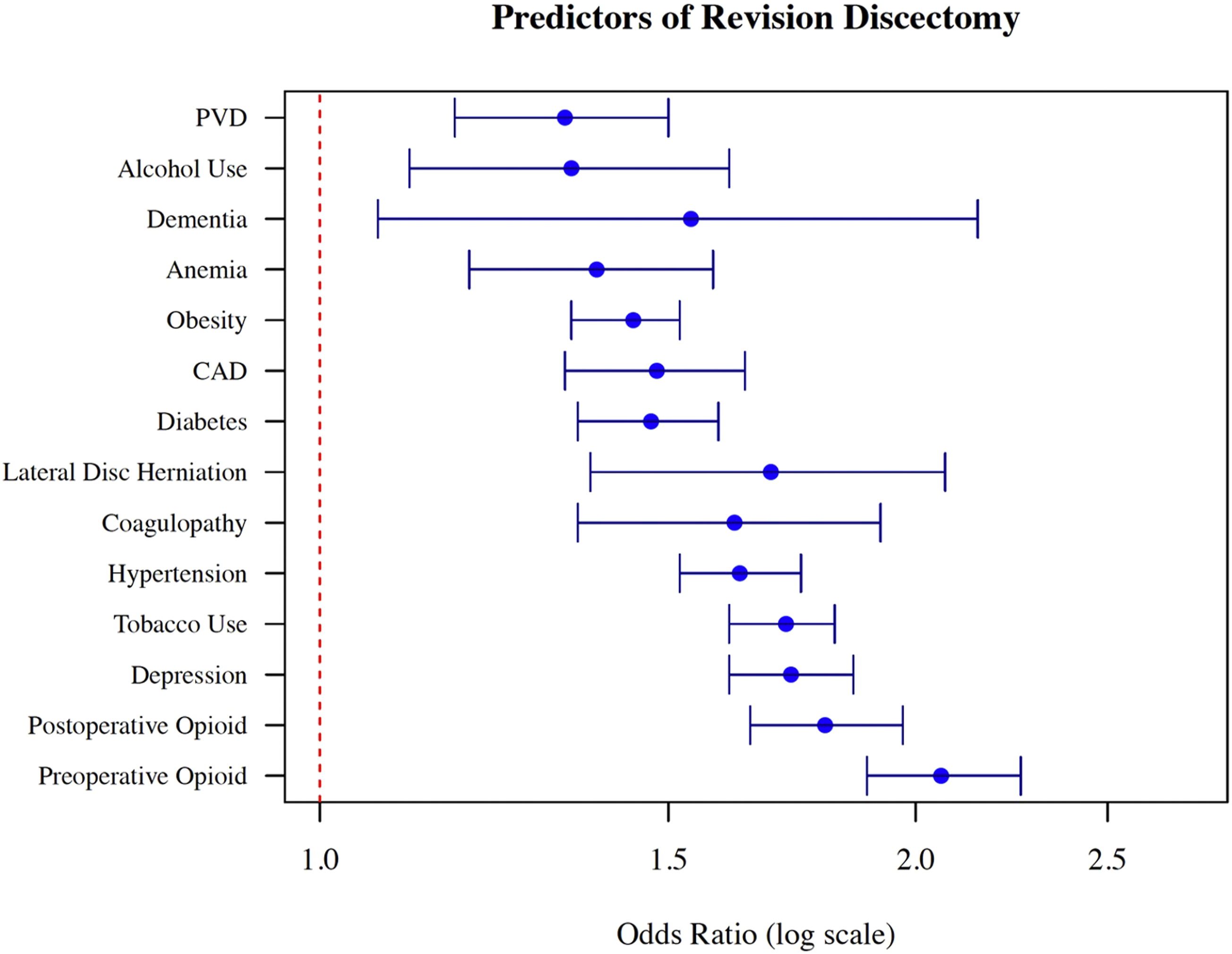
Revision Outcomes
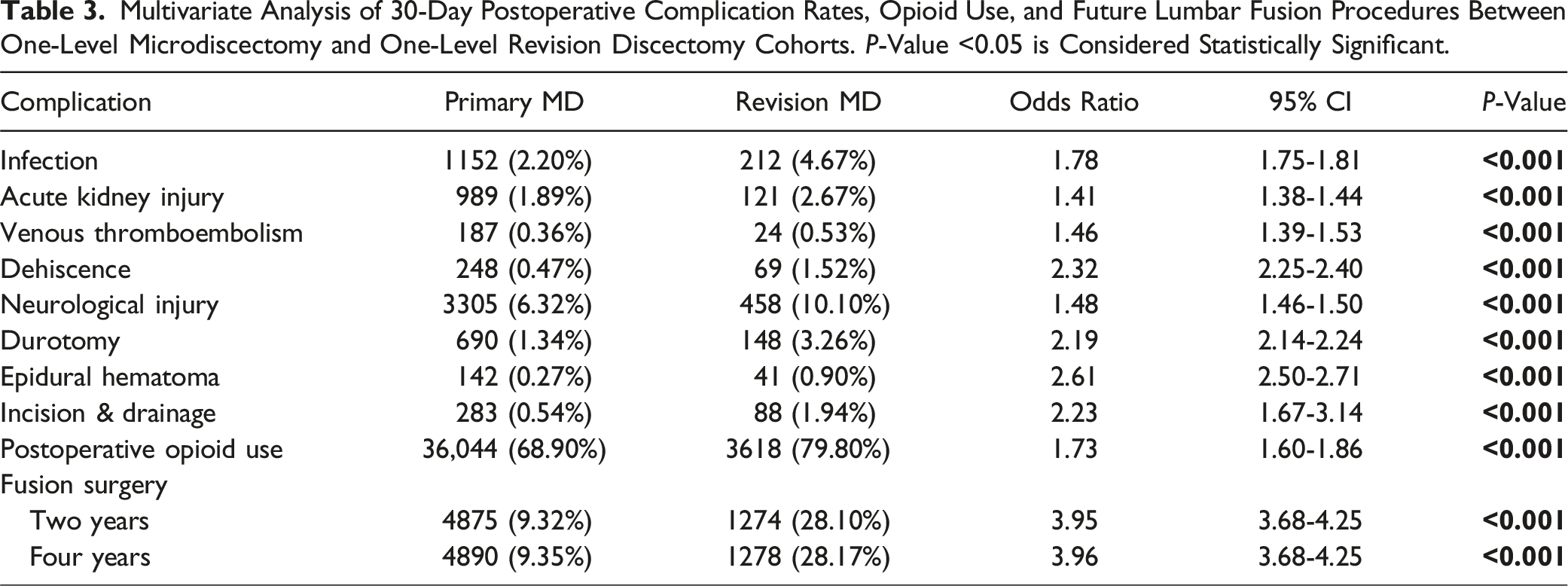
Multivariate Analysis of 30-Day Postoperative Complication Rates, Opioid Use, and Future Lumbar Fusion Procedures Between One-Level Microdiscectomy and One-Level Revision Discectomy Cohorts. P-Value <0.05 is Considered Statistically Significant.
Discussion
The present study identifies independent predictors and complication profiles associated with primary lumbar microdiscectomy and revision discectomy. With a total cohort of 56,846 patients, this represents the largest analysis to date, enabling a comprehensive evaluation of the risks and complications associated with revision discectomy. Several patient-related independent factors were identified, including obesity, lateral disc herniation, alcohol use, coagulopathies, CAD, anemia, dementia, diabetes, hypertension, PVD, preoperative opioid use, postoperative opioid use, and depression. The prevalence of these clinical features among patients requiring revision cases aligns with prior studies, which have consistently reported higher rates of smoking, alcohol use, and obesity in this population.6,10-16 Independent risk factors such as depression, prolonged postoperative opioid use, and smoking corroborate findings from previous research.17,18
Notably, while depression, lateral disc herniation, and sustained postoperative opioid use have not been conclusively established as independent predictors, their associations with suboptimal postoperative outcomes are well-documented in the literature.19-22 More specifically, the observed association between postoperative opioid use and an increased risk of revision discectomy is likely due to patients with more severe preoperative disc herniations requiring more extensive discectomy. This results in higher postoperative pain and a greater need for pain management, including opioid use. Patients with more severe disc herniations are more likely to experience higher rates of subsequent discectomy. Prior research has shown that larger annular defects are associated with a higher risk of reherniation, placing this patient population at increased risk for revision procedures. 23 Additionally, the association between lateral disc herniation and an elevated risk of revision discectomy is supported by prior studies demonstrating higher recurrence risk with extraforaminal herniations. In a retrospective study of 1214 microdiscectomy patients, Gulensoy et al identified lateral disc herniation type as a significant predictor of recurrence, further emphasizing its clinical importance. 24
Postoperative Outcomes
In assessing postoperative outcomes, our multivariate regression analysis of one-level procedures revealed that patients who underwent revision discectomy were at significantly greater risk for various complications—both short- and long-term—compared to those who underwent primary lumbar microdiscectomy. Across perioperative outcome measures, revision discectomy patients incurred substantially higher rates of neurological injury, epidural hematoma formation, durotomy, and all short-term complications collectively. Similarly, Tafazal et al reported a 3.5% incidence of durotomy during primary microdiscectomy, compared to a 13.2% incidence in revision cases. 25 Heightened prevalence of perioperative complications observed within the revision cohort likely reflects altered postoperative anatomy commonly preceding surgical intervention.26,27 Peridural scarring has been widely established as an inherent process of wound healing following lumbar spine surgery, 28 wherein replacement of mobile epidural fat by taut fibrotic tissue can tether and compress the dura and nerve roots against surrounding structures to precipitate new-onset postoperative pain. 29 In a multi-phase, prospective observational survey study of 422 patients, Mancuso et al demonstrated significant associations between undergoing revision lumbar spine procedures and higher postoperative pain scores 30 ; the authors also found that improvement following revision surgery was additionally tempered relative to patients who underwent an index procedure.
With respect to long-term outcomes, our findings describe substantially greater rates of fusion surgery following revision lumbar discectomy. Similarly, a retrospective study of 227 single-level lumbar MD performed by a single surgeon demonstrated significantly different reoperation rates of 14.5% and 31.7% in the primary and revision setting, respectively. 31 Overall, 11 of 12 patients in the revision group who required reoperation were treated with subsequent fusion. Heindel et al studied 13,654 patients receiving single-level lumbar discectomy, finding that 5.9% went on to lumbar spinal fusion within 4 years, while 38.4% of those requiring revision discectomy were ultimately fused within 4 years. 32 The collection of these findings similarly attests to our own results, wherein revision discectomy patients were substantially more likely to undergo subsequent fusion relative to their primary discectomy counterparts. This may be explained by the summative removal of aggregate disc material with progression to consequential segmental instability and eventual need for fusion. 33
Limitations
In evaluating the limitations of this study, it is imperative to acknowledge the inherent constraints associated with the utilization of the PearlDiver national database. Reliance on ICD and CPT coding systems inherently restricts the granularity of our analysis, as these systems provide a binary framework for data categorization. While intended to be uniform, the use of ICD and CPT coding is further subject to variability and potential inaccuracies across different institutions. The variability in coding practices, influenced by factors such as clerical errors, interpretation differences, annual updates to coding definitions, and noncoverage policies introduces an additional layer of complexity, particularly in the context of endoscopic approaches to lumbar discectomy. This heterogeneity underscores the importance of cautious interpretation of findings herein.
The retrospective design of our study moreover introduces the potential for confounding bias. To mitigate this, we restricted the analysis to one-level procedures and employed a multivariate regression analysis to account for known confounding variables. It is, however, crucial to recognize that such statistical controls cannot fully compensate for the limitations inherent in retrospective analyses.
Additionally, the PearlDiver database does not provide information on surgical variables such as differences in surgical techniques or surgeon experience, limiting the generalizability of our findings. Consequently, the incidence of revision discectomy and associated complications may vary by institution. Furthermore, we were unable to assess the severity of postoperative complications, which could have provided additional insights into clinical outcomes.
Conclusions
In conclusion, among microdiscectomy cases for disc herniation identified, 7.98% were revision cases. Several patient-related factors significantly increase the risk of undergoing revision MD, which is associated with additional short- and long-term complication risks relative to the index procedure. These findings help inform expectations regarding disease progression and postoperative outcomes in revision MD, and suggest that revision discectomy should be avoided. Future higher-level studies should be conducted to propose treatment algorithms for recurrent lumbar disc herniations, including indications for revision MD vs segmental fusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Andy Ton, Jane Han, Kevin Mertz, Henry Avetisian, Edward Shontz, Nicole Hang, Marc Abdou, Mirbahador Athari, and Will Karakash have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccentrial Robotics for lectures and presentations. Informed consent was waived due to the retrospective nature of the study and institutional review board (IRB) approval was not required as the database is de-identified.