
Abstract
Study Design:
Retrospective cohort study.
Objective:
To determine the rate of early failures (readmission or reoperation for new or recurrent pain/neurological symptoms) within 30 days after lumbar discectomy and identify associated risk factors.
Methods:
A retrospective cohort study was conducted of patients undergoing lumbar discectomy in the National Surgical Quality Improvement Program database between 2013 and 2017. Rates of readmission for new or recurrent symptoms or reoperation for revision discectomy or fusion within 30 days postoperatively were measured and correlated with risk factors.
Results:
In total 62 690 patients were identified; overall rate of readmission within 30 days was 3.3%, including 1.2% for pain or neurological symptoms. Populations at increased risk of readmission were those with 3 or more levels of treatment (2.0%, odds ratio [OR] 2.8%, P < .01), age >70 years (1.8%, OR 1.6, P < .01), class 3 obesity (1.5%, OR 1.4, P = .04), and female gender (1.4%, OR 1.2, P = .02). The overall rate of reoperation within 30 days was 2.2%, including 1.2% for revision decompression or lumbar fusion surgery. Populations at increased risk of reoperation were revision discectomies (1.4%, OR 1.7, P < .01) and females (1.1%, OR 1.4, P < 0.01). Extraforaminal discectomies were associated with lower rates of readmission (0.7%, OR 0.6, P = 0.02) and reoperation (0.4%, OR 0.4, P = .01).
Conclusions:
Early failures after lumbar discectomy surgery are rare. However, certain subpopulations are associated with increased rates of early failure: obesity, multilevel surgery, females, and revision discectomies.
Keywords
Introduction
Lumbar discectomy is one of the most commonly performed surgical procedures in the United States. 1 In 2002 to 2003, the rate of lumbar discectomy or laminectomy was 1.1 per 1000 Medicare enrollees. 1 The postoperative complication rates after lumbar discectomy surgery has been described as being low compared with lumbar fusion surgery. 2 -4 However, very early failure (within 30 days after the initial surgery) after lumbar discectomy due to inadequate decompression or recurrent herniation, requiring readmission or reoperation, remains a complication that has not been extensively studied.
In one series of over 1000 patients undergoing primary discectomy, 1.1% of patients suffered a recurrent herniation within 1 year. 5 However, this series did not focus specifically on failures during the very early postoperative period and many actually had good initial symptomatic improvement postoperatively. In another large series of over 1300 patients undergoing lumbar discectomy, the overall rate of immediate failure requiring reoperation was 2.8%, with the most common reason being inadequate discectomy or reherniation. 6 However, the authors did not determine risk factors for reherniation or identify subpopulations at higher risk for early failure. Finally, one large series of over 20 000 discectomy patients found a 2.6% rate of readmissions in the early postoperative phase. 7 However, this did not analyze reoperations due to early failures.
The current study aims to determine rates of very early failure (within 30 days postoperatively) after lumbar discectomy surgery and risk factors based on patient characteristics and the type of discectomy procedure performed. As there are different types of lumbar disc herniation, such as posterolateral and far lateral herniations, it is important for both patients and surgeons who are counseling them preoperatively to understand relative early failure rates between procedures. This analysis utilized the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database with large sample size allowing measurement of significant differences in this relatively rare complication.
Materials and Methods
Study Design
A retrospective cohort study of patients undergoing lumbar discectomy was conducted in the NSQIP database.
Setting
All patients undergoing lumbar discectomy from 2013 to 2017 were identified in the NSQIP database. NSQIP is a clinical registry of surgical data from participating US hospitals, both community and private. Trained data reviewers collect complication, readmission, and reoperation data on all included patients for 30 days postoperatively using medical charts and home telephone calls.
Participants
Patients undergoing lumbar discectomy surgery between 2013 and 2017 were determined using Current Procedural Terminology (CPT) codes 63 030, 63 035 (primary discectomy), 63 042, 63 044 (revision discectomy), 63 056, and 63 057 (far lateral discectomies). Exclusion criteria were a preoperative diagnosis of infection, fracture, or neoplasms; patients undergoing simultaneous spinal fusion or cervical spine surgery; and patients undergoing lumbar corpectomy, spinal osteotomy, or vertebral column resection for correction of spinal deformity were excluded. Simultaneous cervical spine surgery was excluded due to the additional risks or readmission and reoperation associated with either anterior or posterior cervical spine surgery and the extended operative time compared with lumbar discectomy.
Variables and Data Sources
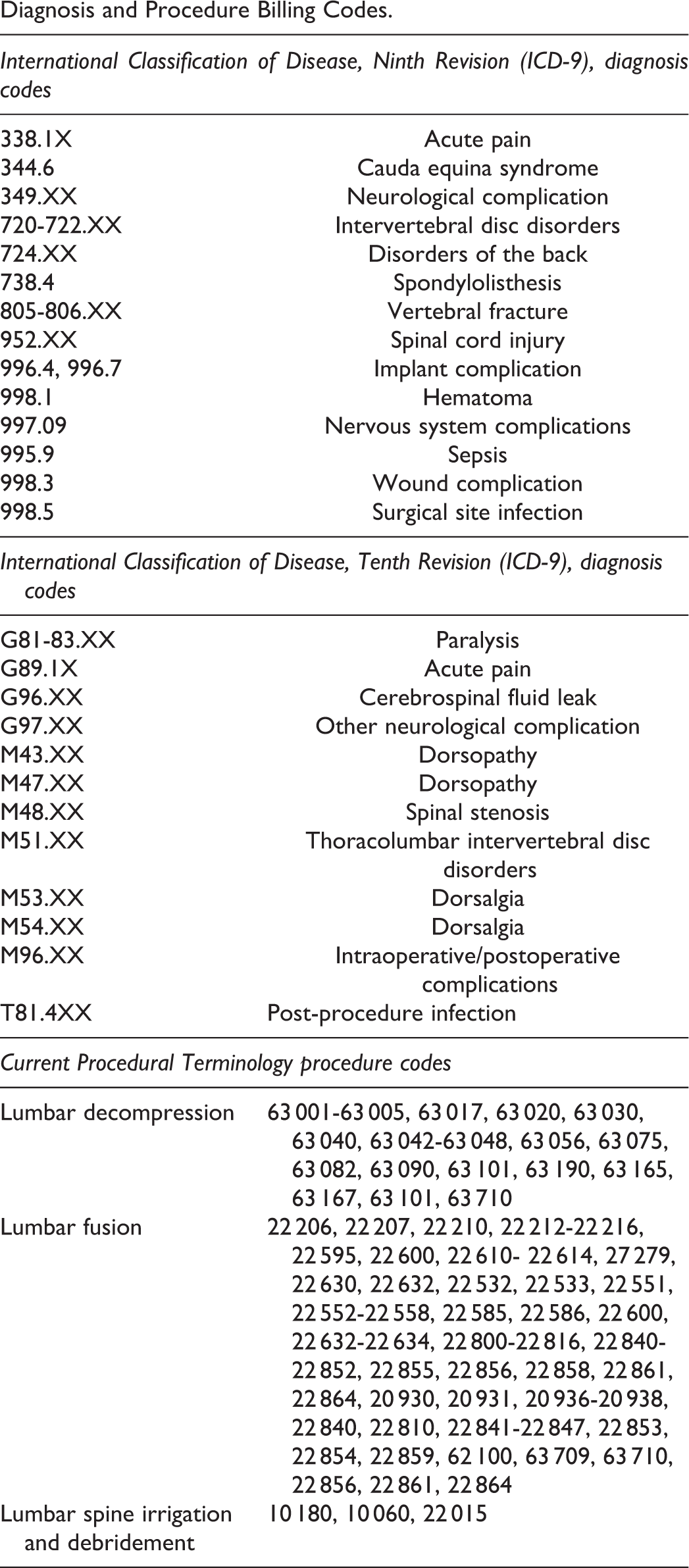
The primary outcome measures analyzed were any surgery-related 30-day readmissions due to new or recurrent pain or neurological symptoms and including infection or surgery-related 30-day reoperation for revision lumbar spine decompression or lumbar spinal fusion. Surgery-related readmissions due to new or recurrent pain, neurological symptoms, or surgical site infection were determined based on International Classification of Disease, Ninth Revision (ICD-9), and International Classification of Disease, Tenth Revision (ICD-10), diagnosis codes on readmission. Included ICD-9 and ICD-10 codes can be found in the appendix. Patients readmitted for revision lumbar decompression or fusion surgery, as defined below, were also included.
Reoperations for revision lumbar discectomy or fusion were determined based on CPT procedural codes for the revision procedure or ICD-9/ICD-10 diagnosis codes. The same ICD-9/ICD-10 codes described above were included. CPT codes for revision discectomy, lumbar fusion surgery, and lumbar spine irrigation and debridement can be found in the appendix.
The primary experimental variables were patient risk factors. Risk factors included patient sex, age, body mass index (BMI), current smoking status, number of levels of discectomy/laminotomy, revision discectomy, far lateral discectomy. Sex, age, BMI, and current smoking status are reported in NSQIP as discrete variables based on clinical data reviewer chart review. Number of levels of discectomy/laminotomy, revision discectomy, and far lateral discectomy were determined based on CPT procedure coding.
Statistical Methods and Bias
First the rate of early readmissions due to spine-related reasons and early reoperations for lumbar decompression or fusion were determined for the overall populations and for the subpopulations. Next, a multivariate logistic regression model was used to find the association of risk factors with early readmission for postoperative pain or neurological symptoms and with reoperation for revision decompression or lumbar fusion, after controlling for other patient factors (age, sex, BMI). Multivariate regression modeling was used to control for possible confounding factors related to readmission or reoperation after lumbar discectomy. In addition, 4 interaction terms were included in the regression model in order to determine any mixed effect of obesity: (1) obesity and multilevel surgery, (2) obesity and revision surgery, (3) older age and multilevel surgery, and (4) older age and multilevel surgery. Statistical tests were performed with Stata version 13.0 statistical software (StataCorp LP). All statistical tests were made 2-tailed, and an α level of .05 was considered statistically significant.
The American College of Surgeons regularly conducts internal data audits of NSQIP collected data to ensure accuracy and reduce the amount of missing data for discrete data elements. The reported rate of data collection errors within NSQIP is low compared to other large national datasets, with an overall interrater disagreement rate below 2%. 8 NSQIP also conducts regular quality control audits of participating hospitals and excludes institutions with disagreement greater than 5%. However, we do expect some degree of missing data for variables abstracted from ICD-9 or CPT codes.
Sources of Funding
No funding was received for this study.
Results
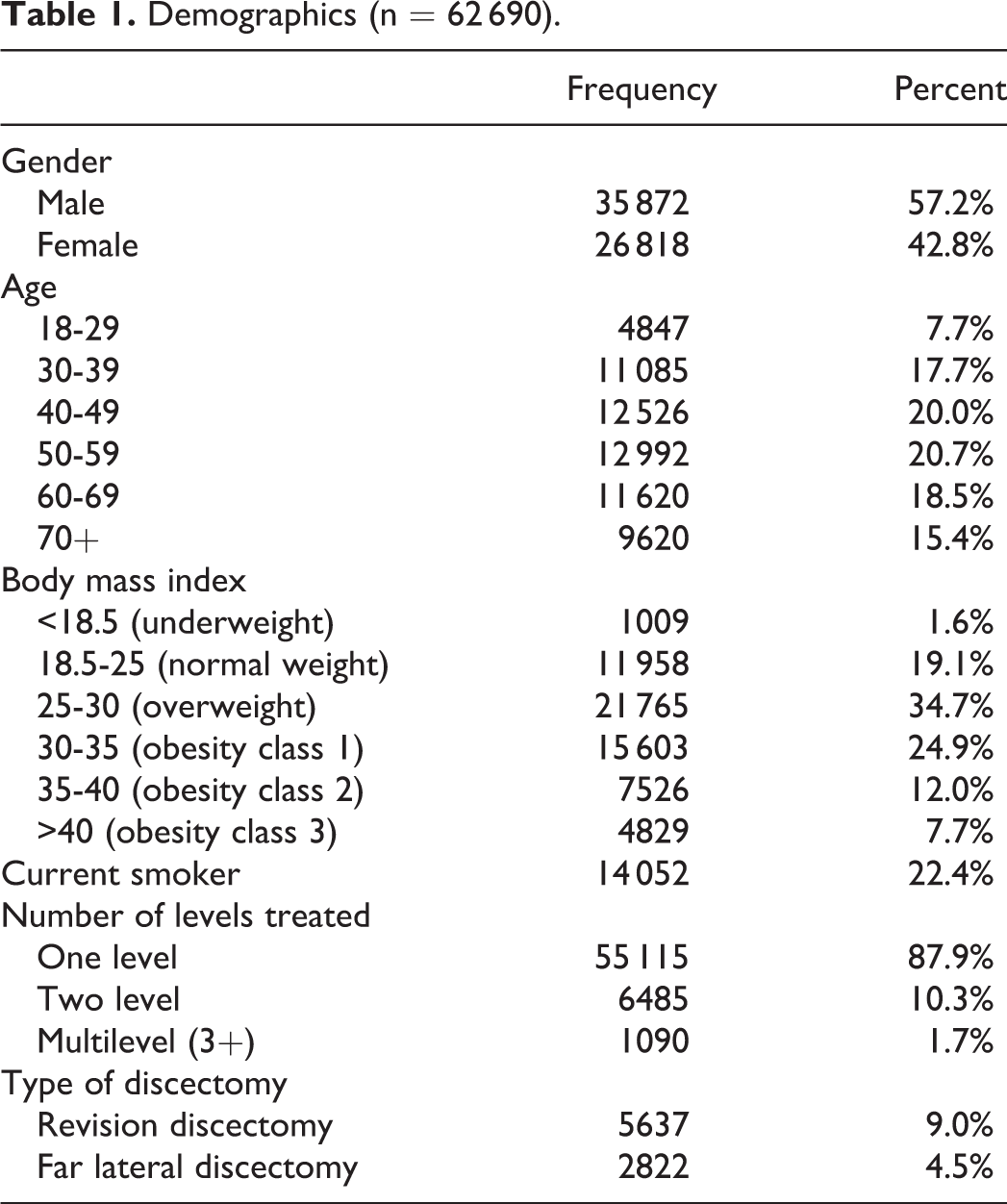
A total of 62 690 patients who underwent lumbar decompression surgery between 2013 and 2017 were identified (Table 1). Of those patients, 55 115 (87.9%) underwent a single-level discectomy, 5637 (9.0%) underwent revision discectomy, and 2822 (4.5%) underwent a far lateral discectomy.
Demographics (n = 62 690).
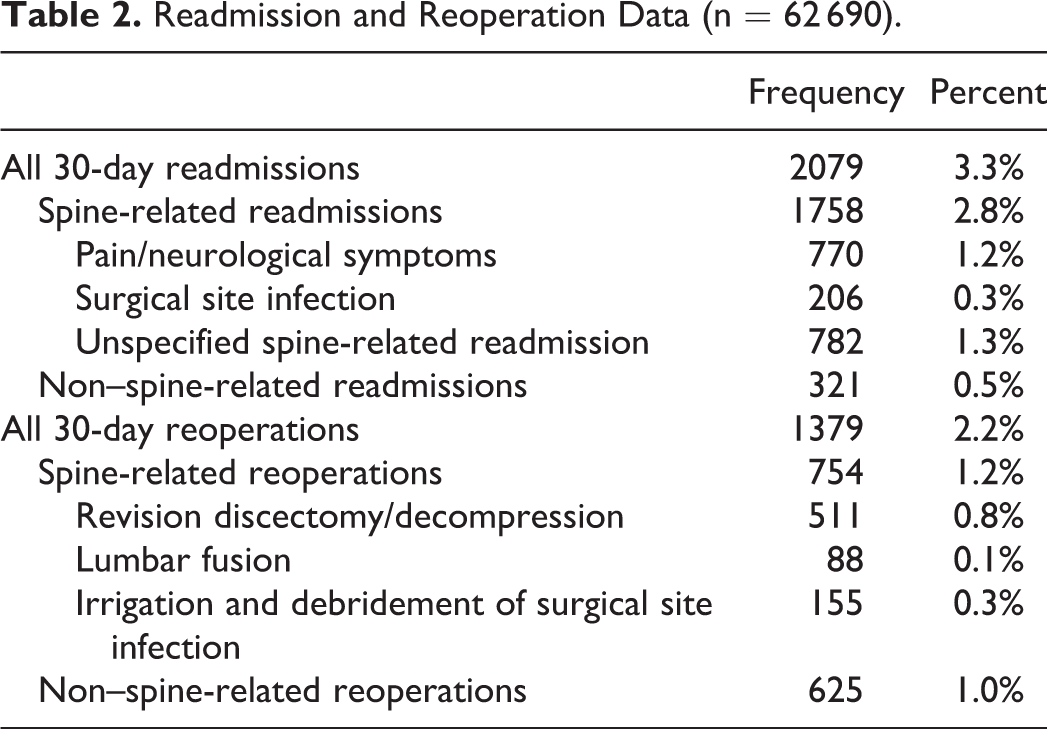
There were a total of 2079 patients (3.3%) that were readmitted to the hospital within 30 days of surgery (Table 2). Of those, 1758 (2.8%) were spine-related readmissions, including 770 (1.2%) for pain or neurological symptoms, and 206 (0.3%) for postoperative infection. In multivariate analysis (Table 3), populations at increased risk of readmission for pain or neurological symptoms were those with 3 or more levels of treatment (2.0%, odds ratio [OR] 2.8, P < .01), the interaction between obesity and revision surgery (3.3%, OR 1.9, P = .01), age >70 years (1.8%, OR 1.6, P < .01), class 3 obesity (1.5%, OR 1.4, P = .04), class 1 obesity (1.3%, OR 1.3, P = 0.02), and female gender (1.4%, OR 1.2, P = .02). Far lateral discectomies were associated with lower rates of readmission (0.7%, OR 0.6, P = .02).
Readmission and Reoperation Data (n = 62 690).
Multivariate Analysis of Risk Factors for Early Readmission for New or Recurrent Pain and Neurological Symptoms.a
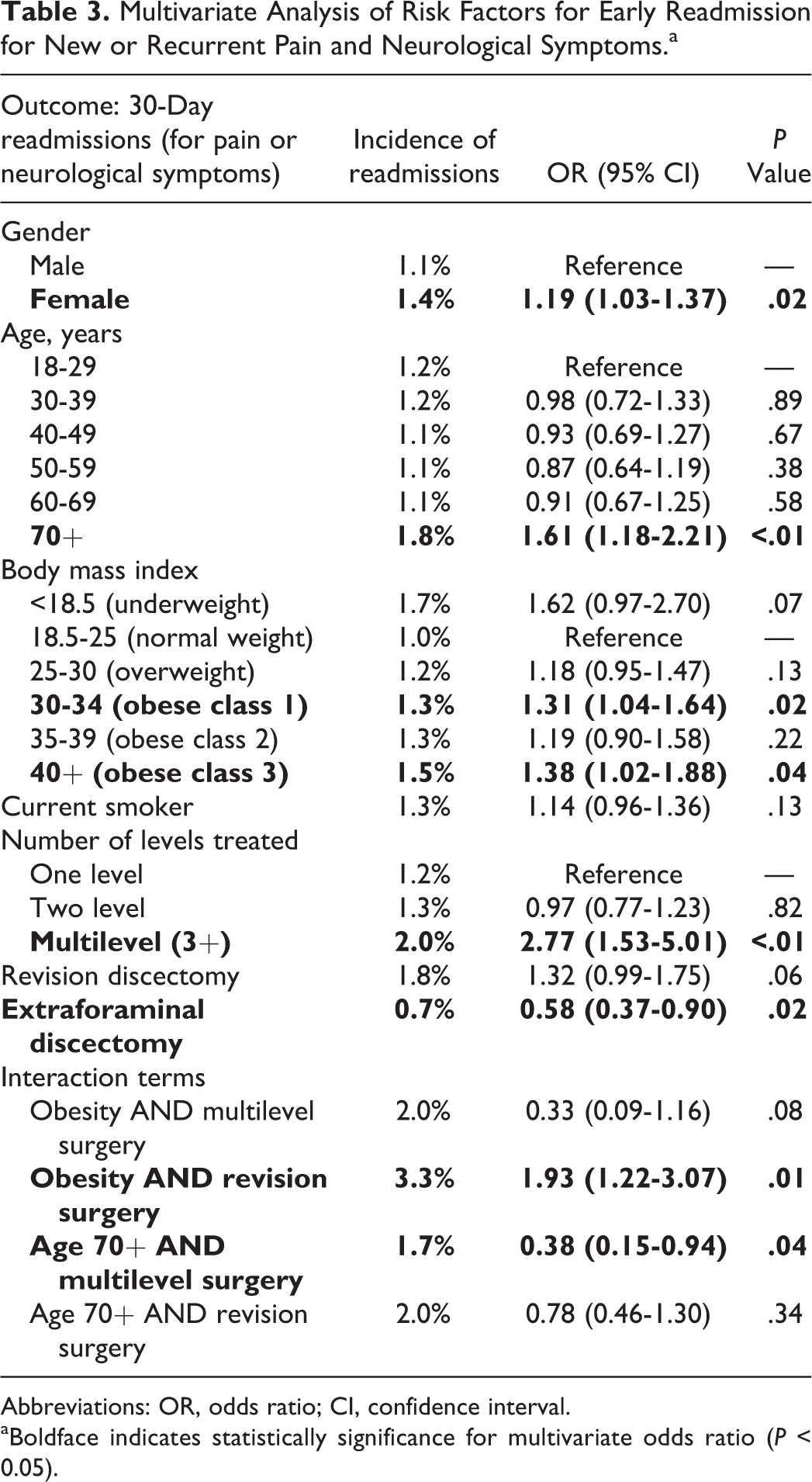
Abbreviations: OR, odds ratio; CI, confidence interval.
aBoldface indicates statistically significance for multivariate odds ratio (P < 0.05).
A total of 1379 patients (2.2%) underwent a reoperation within 30 days (Table 2). Of those, 754 (1.2%) were spine-related reoperations, including with 511 (0.8%) for revision lumbar discectomy, 115 (0.3%) for irrigation and debridement of an infection, and 88 (0.1%) for lumbar fusion. In multivariate analysis (Table 4), populations at increased risk of reoperation for revision decompression or lumbar fusion were revision discectomies (1.4%, OR 1.7, P < .01) and females (1.1%, OR 1.4, P < .01). Far lateral discectomies were associated with lower rates of reoperation (0.4%, OR 0.4, P < .01).
Multivariate Analysis of Risk Factors for Early Reoperation.a
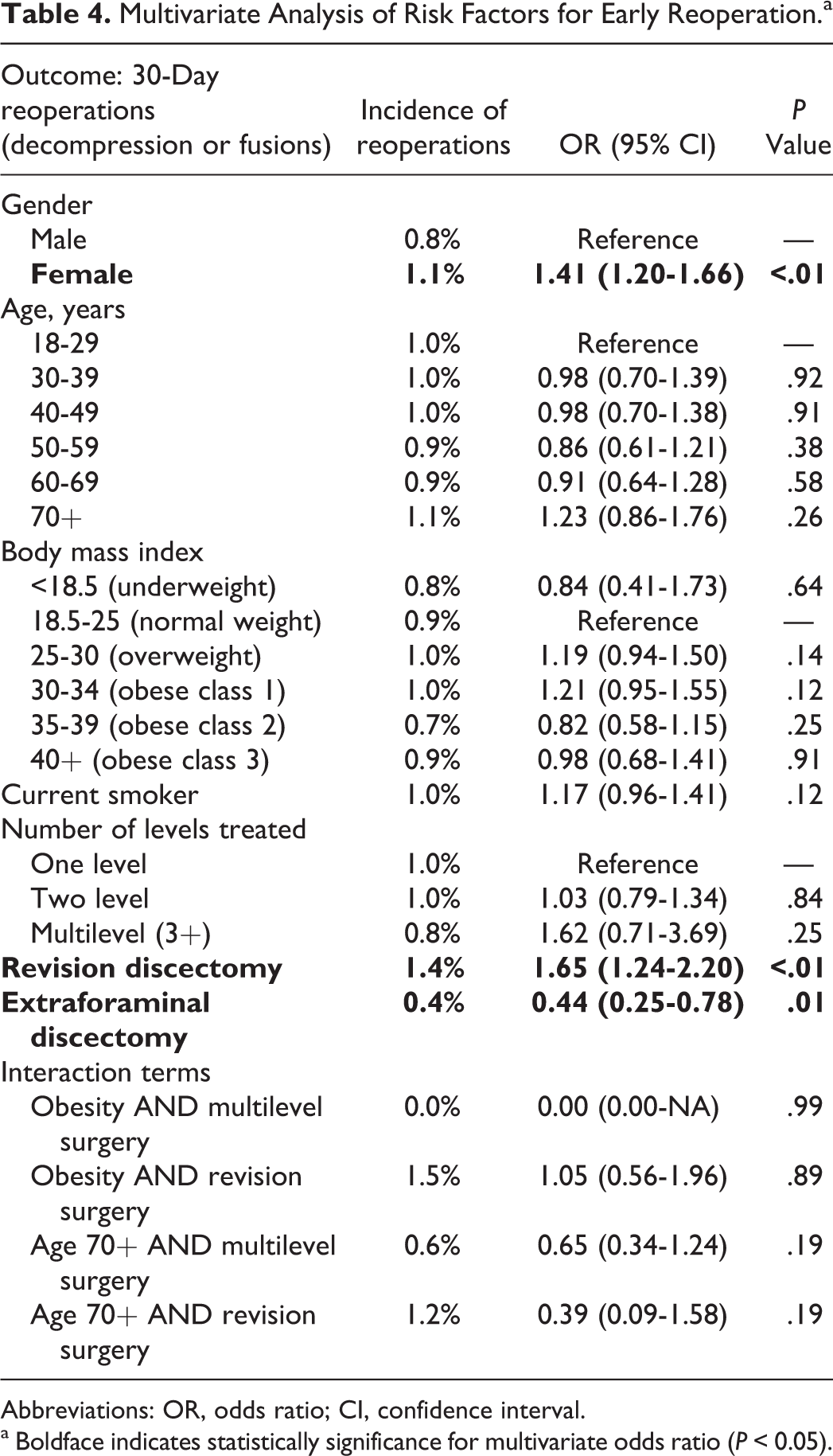
Abbreviations: OR, odds ratio; CI, confidence interval.
a Boldface indicates statistically significance for multivariate odds ratio (P < 0.05).
Discussion
Early failures after lumbar discectomy are a rare but significant complication resulting in increased health care costs and patient morbidity. 9 Excluding infections, early failures may occur due to reherniation, inadequate decompression, nerve root injury, or persistent postoperative back pain. The current study utilizes the NSQIP 2013 to 2017 database to demonstrate an overall low rate of both early readmission (3.3%) and early reoperation (2.2%) after lumbar discectomy surgery within 30 days postoperatively. There was also a lower rate of readmissions or reoperations specifically for spine-related pathology, at 2.8% and 1.2%, respectively. This is important knowledge for patient counseling and also for reimbursement purposes.
While previous studies have identified revision surgery, multilevel surgery, and obesity as risk factors reoperation after discectomy in the long term, the value of the current study is not identification of specific risk factors, but determination of the rate of early failures (within 30 days of surgery), a much more costly and unfortunate complication. This is the largest study to date to report the rate of and risks for early failures after lumbar discectomy at over 62 000 cases and 754 early spine-related reoperations in a national cohort. The only previous study to specifically describe early failures reported on approximately 1500 cases with 44 cases of early failure. This is also the first study to identify female sex and smoking status as risk factors for early failure within 30 days, the first to compares rates of failures between primary and revision procedures, and the first study to identify far lateral discectomies as having significantly lower rates of early failures.
The primary finding of the current study is that the overall rate of early readmission or reoperation after discectomy surgery is low. One previous large retrospective study of 1546 lumbar discectomy cases reported a 2.8% rate of early failure requiring reoperation, higher than reported in the current study. 6 In this study early failure was most commonly due to reherniation or inadequate decompression in 50% of patients (1.4% of overall study population), followed by battered root syndrome in 30% of patients (0.8% of overall study population), which was defined by the absence of any intraoperative findings during revision surgery. The current study reports a reoperation rate of 1.2% within the early 30-day postoperative period. This difference may be due to a more aggressive reoperation protocol in the former study, with 30% of cases demonstrating no pathology on reoperation. The authors of the former study did conclude that a trial of conservative management with anti-inflammatory medical therapy should be initiated first for persistent or recurrent symptoms prior to reoperation.
A number of studies do report on long-term rates of readmission and reoperation after discectomy surgery. In the large multicenter prospective Spine Patient Outcomes Research Trial (SPORT), the overall rate of reherniation after discectomy was 9.1% at 8 years postoperatively, with 37.8% of these (3.4% of patients) occurring in the first year postoperatively. 10 In another series of over 1000 patients undergoing primary lumbar discectomy, 1.1% of patients suffered a recurrent herniation within 1 year. 5 Finally in a systematic review of over 21 000 patients the rate of recurrent disc herniation varied considerably from 0% to 23% and the rate of reoperation varied from 0% to 13%. 11 Again, in the current study the rate of reoperation was 1.2% within the first 30 days after surgery.
The large patient sample within NSQIP dataset used in this study allowed comparisons to be made between different subpopulations undergoing lumbar discectomy. Interestingly, we see increased rates of reoperation after revision discectomy and increased readmission with the combined effects of revision surgery in obese patients. Previous studies have compared early failures after primary and revision discectomies. 1,4,12,13 In one large analysis of 649 propensity-matched revision discectomy cases, revision discectomy showed similar rates of postoperative morbidity and 30-day complications compared to primary cases. 14 Another series of 227 consecutive cases demonstrated that, compared to primary cases, revision minimally invasive discectomy was associated with longer hospitalization and greater postoperative pain and narcotic use. 15 The current study supports these findings, suggesting that revision discectomies are more likely to require subsequent reoperation. This may be due to increased difficulty in confirming adequate decompression or increased likelihood for reherniation in the setting of an existing annulotomy.
This is also the first study to demonstrate lower rates of early readmission and reoperation with far lateral lumbar discectomies. This may be due to a more reliable ability to fully decompress the exiting nerve root through the extraforaminal far lateral approach. In comparison in the standard interlaminar approach for paracentral disc herniations, assessment of complete decompression may be difficult due to disc fragments hidden by the thecal sac centrally. There may also be a decreased anatomical propensity for reherniation from far lateral annular tear, compared with a paracentral tear. However, there is no existing evidence for this in the current literature.
Multilevel discectomy procedures were also associated with higher rates of early readmission, but not reoperation. From existing literature we know that early failures requiring revision are most commonly due to recurrent disc herniation and inadequate primary discectomy, usually treated with reoperation. 16,17 The lack of association of multilevel discectomy with reoperation surgery suggests that the increased readmissions may partially be due to increased postoperative pain or muscle spasm from the more extensive surgical dissection.
The current study also demonstrated a statistically significant association between female sex and both early readmissions and early reoperations. This association with sex was not seen in the large prospective SPORT trial of 810 discectomy patients. 10 However, 2 previous studies of over 10 000 patients undergoing lumbar discectomy surgery from the Swedish National Spine Surgical Register demonstrated that females had inferior postoperative outcomes after lumbar discectomy surgery due to inferior preoperative clinical status. 18,19 For example, females often had higher preoperative pain, worse walking ability, consumed more analgesic medication, and had worse preoperative ODI (Oswestry Disability Index). Another small series of 40 lumbar discectomy patients demonstrated worse ODI in female patients at long-term follow-up, which was statistically significant. 20 It remains to be seen whether there is any biological or societal reasoning for increased early postoperative failures in females after lumbar discectomies and whether this is related to worse preoperative clinical status.
Higher rates of early readmission were also seen with patients with obesity class 1, obesity class 3, and revision surgery in the setting of obesity. Previous studies have shown lower rates of minimal clinically importance difference in outcomes in obese patients undergoing lumbar decompression surgery at 6 months and 12 months. 21
Regarding optimal treatment for new or recurrent symptoms, the most common procedure in the current study was revision lumbar decompression in 511 patients, compared with only 88 patients undergoing lumbar fusion. In a previous study of 54 patients with post-discectomy pain syndrome, 15 patients underwent successful repeat discectomy while 6 failed repeat discectomy. 22 Twenty-seven patients underwent minimally invasive transforaminal lumbar interbody fusion with good outcomes. This suggests that fusion may be the optimal revision procedure in select revision cases, such as patients with instability, who may have initially benefited from a primary fusion. While the literature does support more durable outcomes after fusion for revision lumbar disc herniation, there remains no clear guideline for reoperation after failed discectomy. Due to the risk reherniation after a revision discectomy, surgeons may opt for either conservative treatment without discectomy versus lumbar fusion, in order to prevent recurrence.
The current study does have limitations that must also be considered inherent both to its retrospective nature and utilization of NSQIP. As a retrospective cohort study, the associations found in the current study cannot be assumed to be causative and the quality of data entered into the database must also be considered. In NSQIP, while postoperative readmission and reoperations are determined after an iterative, internally audited, chart review process by specialized clinical data reviewers, the sensitivity of diagnosis and procedure codes contained in the database and utilized for the current analysis are also known to be much lower. Previous investigation by the current group has demonstrated sensitivities as low as 5% to 25% for certain medical comorbidities. 23 Therefore, effect sizes may be underestimated in statistical comparisons between these subpopulations. In addition, NSQIP includes certain amounts of missing data. 24,25 However, the current group has also demonstrated that this missing data is primarily in preoperative laboratory values and that reoperation and readmission data is largely complete. Nevertheless, a significant percentage of patients did have an unspecified reason for readmission or reoperation, which does also limit the current study.
Next, due to the multicenter, multisurgeon design of the current retrospective study, specific surgeon practices such as indications for fusion surgery and postoperative rehabilitation protocols were not available for review. This is certainly an important source of variability in the results as different surgeons may have different thresholds for subsequent fusion surgery. In addition, early rehabilitation protocols may be a potential source of early reherniations, although this remains to be studied prospectively. Finally, using ICD-9 diagnosis coding and CPT procedure coding, we are unable to determine the specific level of reoperation in patients. Therefore, we cannot distinguish between revision surgery at the index level of previous discectomy or at an adjacent level. Nevertheless, we believe the value of the current study is in identifying the overall rate of spine-related reoperations, and determining subpopulations at higher risk for these early failures. Further prospective study is warranted to determine the precise rates of early reherniation at an index level versus adjacent level.
In conclusion, early readmission or reoperation after lumbar discectomy surgery is a rare complication. However, in certain subpopulations the risk of early readmission or reoperation is significantly higher, such as with revision discectomies, current smokers, and female patients. Patients should be counseled about this increased risk of failure preoperatively.
Footnotes
Appendix
Diagnosis and Procedure Billing Codes.
| International Classification of Disease, Ninth Revision (ICD-9), diagnosis codes | |
|---|---|
| 338.1X | Acute pain |
| 344.6 | Cauda equina syndrome |
| 349.XX | Neurological complication |
| 720-722.XX | Intervertebral disc disorders |
| 724.XX | Disorders of the back |
| 738.4 | Spondylolisthesis |
| 805-806.XX | Vertebral fracture |
| 952.XX | Spinal cord injury |
| 996.4, 996.7 | Implant complication |
| 998.1 | Hematoma |
| 997.09 | Nervous system complications |
| 995.9 | Sepsis |
| 998.3 | Wound complication |
| 998.5 | Surgical site infection |
| International Classification of Disease, Tenth Revision (ICD-9), diagnosis codes | |
| G81-83.XX | Paralysis |
| G89.1X | Acute pain |
| G96.XX | Cerebrospinal fluid leak |
| G97.XX | Other neurological complication |
| M43.XX | Dorsopathy |
| M47.XX | Dorsopathy |
| M48.XX | Spinal stenosis |
| M51.XX | Thoracolumbar intervertebral disc disorders |
| M53.XX | Dorsalgia |
| M54.XX | Dorsalgia |
| M96.XX | Intraoperative/postoperative complications |
| T81.4XX | Post-procedure infection |
| Current Procedural Terminology procedure codes | |
| Lumbar decompression | 63 001-63 005, 63 017, 63 020, 63 030, 63 040, 63 042-63 048, 63 056, 63 075, 63 082, 63 090, 63 101, 63 190, 63 165, 63 167, 63 101, 63 710 |
| Lumbar fusion | 22 206, 22 207, 22 210, 22 212-22 216, 22 595, 22 600, 22 610- 22 614, 27 279, 22 630, 22 632, 22 532, 22 533, 22 551, 22 552-22 558, 22 585, 22 586, 22 600, 22 632-22 634, 22 800-22 816, 22 840-22 852, 22 855, 22 856, 22 858, 22 861, 22 864, 20 930, 20 931, 20 936-20 938, 22 840, 22 810, 22 841-22 847, 22 853, 22 854, 22 859, 62 100, 63 709, 63 710, 22 856, 22 861, 22 864 |
| Lumbar spine irrigation and debridement | 10 180, 10 060, 22 015 |
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Royalties: Globus Medical, Inc., Stryker K2M; Stock Ownership: Avaz Surgical, Vital 5 (past relationship); Consulting: Paradigm Spine, Globus Medical Inc., Stryker K2M; Scientific Advisory Board/Other Office: Association of Bone and Joint Surgeons, Cervical Spine Research Society, Healthgrades, International Society for the Advancement of Spine Surgery, ![]() Inc., Minimally Invasive Spine Study Group, North American Spine Society, Simplify Medical, Inc., Society of Minimally Invasive Spine Surgery, Spinal Simplicity, LLC; Editorial Board: Annals of Translational Medicine, Contemporary Spine Surgery; Honoraria: AMOpportunities, RTI Surgical Inc.; Speakers fees: Globus Medical Inc.
Inc., Minimally Invasive Spine Study Group, North American Spine Society, Simplify Medical, Inc., Society of Minimally Invasive Spine Surgery, Spinal Simplicity, LLC; Editorial Board: Annals of Translational Medicine, Contemporary Spine Surgery; Honoraria: AMOpportunities, RTI Surgical Inc.; Speakers fees: Globus Medical Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.