
Abstract
Study Design:
Longitudinal cohort.
Objective:
It is unclear if patients with a recurrent disc herniation benefit from a concurrent fusion compared with a repeat decompression alone. We compared outcomes of decompression alone (D0) versus decompression and fusion (DF) for recurrent disc herniation.
Methods:
Patients enrolled in the Quality and Outcomes Database from 3 sites with a first episode of recurrent disc herniation were identified. Demographic, surgical, and radiographic data including the presence of listhesis and extent of facet resection on computed tomography or magnetic resonance imaging prior to the index surgery were collected. Patient-reported outcomes were collected preoperatively and at 3 and 12 months postoperatively.
Results:
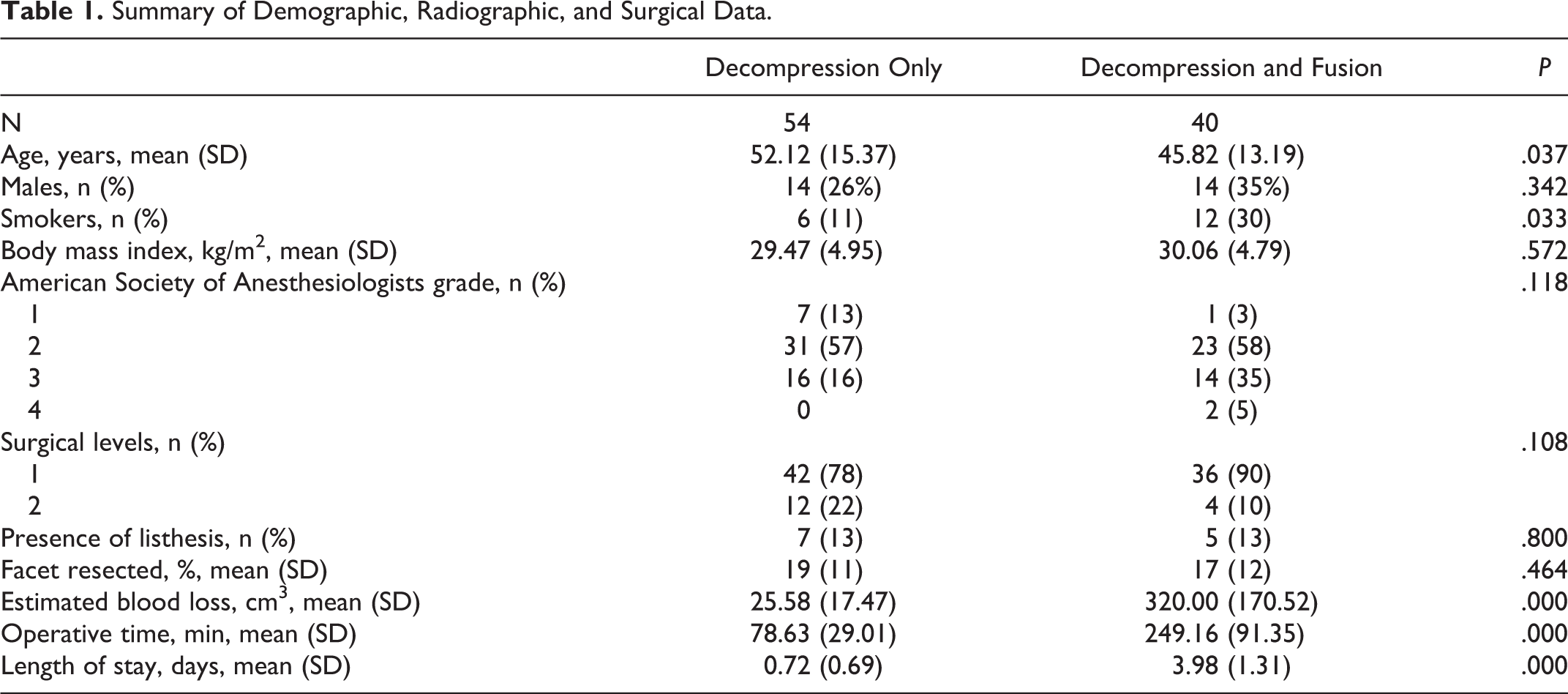
Of 94 cases identified, 55 had D0 and 39 had DF. Patients were similar in age, sex distribution, smoking status, body mass index, American Society of Anesthesiologists grade and surgical levels. Presence of listhesis (D0 = 7, DF = 5, P = .800) and extent of facet resection (D0 = 19%, DF = 16%, P = .309) prior to index surgery were similar between the 2 groups. Estimated blood loss (D0 = 26 cm3, DF = 329 cm3, P < .001), operating room time (D0 = 79 minutes, DF = 241 minutes, P < .001) and length of stay (D0 <1 day, DF = 4 days, P < .001) were significantly less in the D0 group. Preoperative and 1-year postoperative patient-reported outcomes were similar in both groups. Three patients in the D0 group and 2 patients in the DF group required revision. Regression analysis showed that presence of listhesis, extent of facet resection and fusion were not associated with the 12-month Oswestry Disability Index (ODI) score.
Conclusion:
For a first episode recurrent disc herniation, surgeons can expect similar outcomes whether patients are treated with decompression alone or decompression and fusion.
Keywords
Introduction
The incidence of recurrent disc herniation, defined as disc herniation at the same intervertebral level with a pain-free period of at least 6 months after a primary discectomy or decompression 1 has been reported to be between 0.5% and 25%. 2 Although not uncommon, it remains unclear if patients with a recurrent disc herniation benefit from a concurrent fusion compared with a repeat decompression alone. 3 -6
A recent systematic review on the treatment of recurrent disc herniation 7 concluded that there was not enough evidence to support either discectomy alone or discectomy with fusion. Although fusion is more expensive, has higher blood loss, longer operative times and longer length of hospital stays, some studies have shown greater improvements in pain compared with repeat decompression alone. 8 It is also unclear what patient and radiographic factors the surgeon considers in deciding to perform a decompression only or decompression and fusion. Interestingly, a study by Mroz et al 9 found that it is a surgeon characteristic that is associated with whether a decompression alone will be performed for recurrent disc herniation. The study reported that high-volume surgeons (>200 cases per year) that have been in practice longer (15-20 years) were more likely to do a fusion rather than a repeat decompression.
Although there are no guidelines to help surgeons determine which procedure is more appropriate to treat recurrent disc herniation, some authors recommend discectomy in patients with radiculopathy alone, 8,10 while fusion is recommended in the presence of lumbar instability, radiographic degenerative changes, and/or chronic low back pain. 8 The purpose of this study is to compare baseline patient and radiographic characteristics and 1-year patient-reported outcomes (PROs) in patients who had decompression only to patients who had decompression and fusion for recurrent disc herniation.
Methods
Patients enrolled in the Quality and Outcomes Database (QOD) 11 -13 from 3 tertiary spine centers with a first episode of recurrent disc herniation and 1- to 2-level surgery and complete baseline and 12-month follow-up data was identified. The QOD lumbar module is a prospective observational registry of demographic and surgical data, 30- and 90-day morbidity; and 3- and 12-month PROs. Six cases per site are enrolled each week on a rolling 6-day cycle. The first day of each 6-day week falls on each weekday with equal frequency creating a sampling method that prevents a disproportionate volume of enrollment on any one day of the week or from any one surgeon’s schedule at any one site, limiting potential enrollment bias.
The following baseline characteristics were collected: age, sex, body mass index (BMI), race, educational level, employment status, diagnosis, insurance status, Workers’ Compensation status, symptom duration, and American Society of Anesthesiologists (ASA) grade. 14 Numeric rating scales for back and leg pain, 15 Oswestry Disability Index (ODI) scores, 16,17 and EuroQOL-5D (EQ-5D) 18 scores were also collected preoperatively and at 3 and 12 months postoperatively. Additional radiographic data, confirming reherniation at the same intervertebral level, the presence of listhesis and the extent of facet resection on computed tomography or magnetic resonance imaging prior to the surgery for the recurrent disc herniation were also collected. The extent of resection was determined by comparing the width of the resected facet to the width of the contralateral facet to the width at the level of decompression (Figure 1). This was expressed as a percentage (width of the resected facet/width of the contralateral facet). Patients were divided into 2 cohorts, those who had a decompression and/or discectomy only (D0) and those who had a decompression and fusion (DF).

The extent of resection determined by comparing (a) the width of the resected facet to the (b) width of the contralateral facet at the level of decompression expressed as a percentage (width of the resected facet/width of the contralateral facet; a/b.
Statistical analysis was carried out with IBM SPSS software version 21.0. Statistical significance was set at P < .01. Independent t tests were used to determine differences in continuous variables, and Fisher’s exact test was used to determine differences in categorical variables between the 2 cohorts. Regression analysis was performed to determine associations between the presence of listhesis, extent of facet resection and type of surgery and the 12-month postoperative ODI score.
Approval from the institutional review board of the 3 participating institutions was received for both the QOD registry and the current analysis.
Results
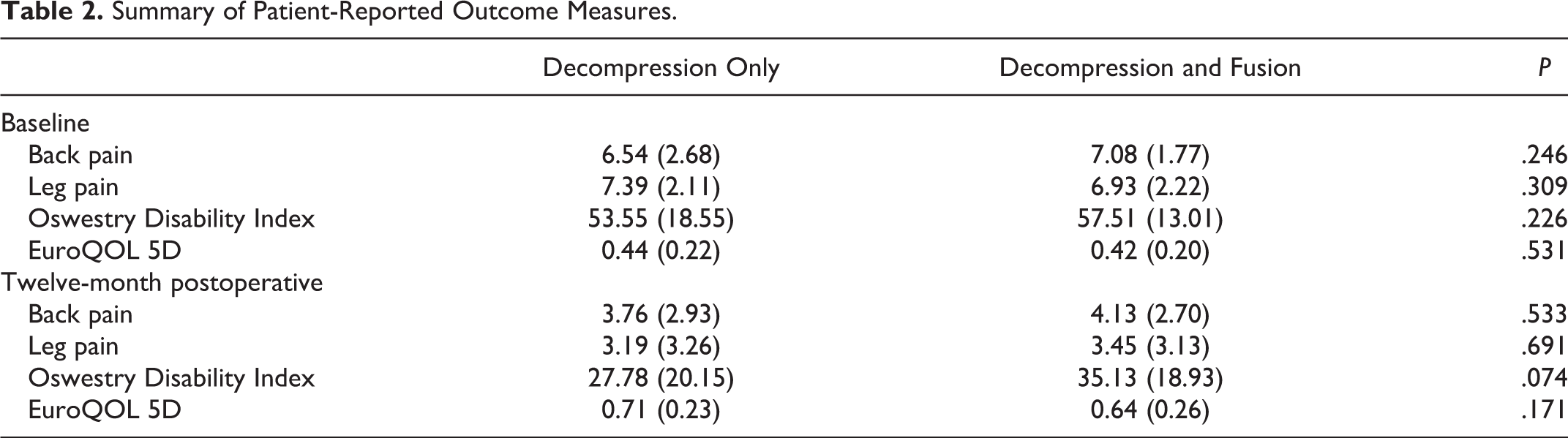
Of 94 cases identified, 55 had D0 and 39 had DF. The patients were similar in age, sex distribution, smoking status, BMI, ASA grade, and surgical levels (Table 1). In both groups, the majority of patients reported that leg pain was their dominant symptom (D0 = 67%, DF = 60%, P = .086). Presence of listhesis (D0 = 7, DF = 5, P = .800) and extent of facet resection (D0 = 19%, DF = 16%, P = .464) prior to index surgery were similar between the 2 groups. As expected, estimated blood loss (D0 = 26 cm3, DF = 329 cm3, P < .001), operative time (D0 = 79 minutes, DF = 241 minutes, P < .001), and length of hospital stay (D0 <1 day, DF = 4 days, P < .001) were significantly less in the D0 group. Preoperative and 1-year postoperative PROs were similar in both groups (Table 2). Three patients in the D0 group required revision, 2 for a second recurrence and 1 for foraminal stenosis. Two patients in the DF group required revision, 1 for nonunion and 1 for adjacent segment disease. None of the patients that had a revision had a listhesis prior to the surgery for the recurrent disc herniation. Regression analysis showed that presence of listhesis, extent of facet resection, and fusion were not associated with the 12-month ODI score.
Summary of Demographic, Radiographic, and Surgical Data.
Summary of Patient-Reported Outcome Measures.
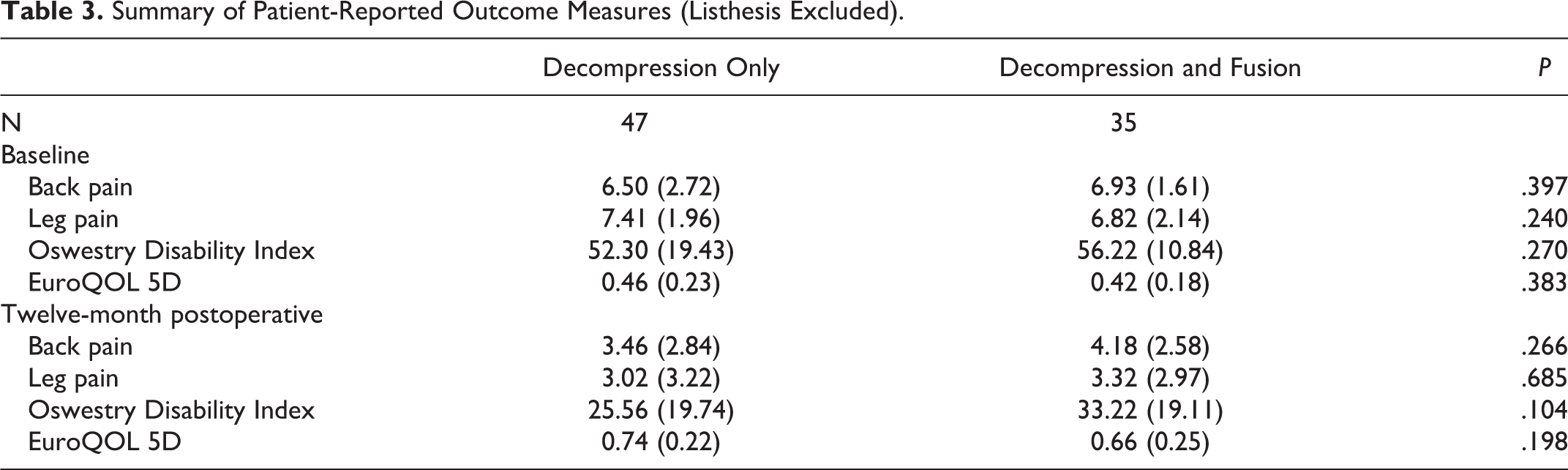
A subanalysis excluding patients with spondylolisthesis (Table 3) did not change the results of the study.
Summary of Patient-Reported Outcome Measures (Listhesis Excluded).
Discussion
The optimum treatment, decompression alone or decompression with fusion, for first episode recurrent disc herniation continues to be controversial. Similar to previous studies, the current study showed that improvements in multidimensional patient reported outcomes are similar for patients treated with either approach. 1 -6 Only 1 comparative study has shown greater improvement in pain scores in patients who had a fusion. 8
As expected, estimated blood loss, operative time, and length of hospital stay was greater for patients who had a decompression and fusion. Interestingly, the rate of revision surgery was similar between the 2 cohorts. The reasons for reoperation were specific to the surgery that was performed, recurrent herniation and foraminal stenosis in the decompression only group; nonunion and adjacent segment disease in the fusion group. Longer term studies are needed to determine if the improvement in PROs are maintained in either group and if the prevalence of revision surgery is similar.
In an attempt to address the shortcomings of previous studies, we looked at radiographic findings that are generally thought to affect a surgeon’s decision making for patients with a first episode recurrent disc herniation. Our results show that the extent of facet resection and the presence of listhesis were similar in the cohort of patients who had a decompression compared with those who had a concomitant fusion. In addition, neither of these radiographic findings were associated with the 12-month ODI score. Excluding patients with listhesis did not change the results of the study.
Similarly, the current thinking that fusion should be recommended in patients whose symptoms are predominantly back pain are not borne out in this study. In both groups, leg pain was the predominant symptom in the majority of patients. Although not statistically significant, there were more smokers in the fusion group compared with the decompression only group. Thus, there would seem to be other factors that are not explicit, that make a surgeon decide to perform a fusion.
Based on this study, it remains difficult to put forward a treatment recommendation for patients with recurrent disc herniation. Conducting a randomized clinical trial would be ideal, but there may be barriers for funding and enrolling enough patients to achieve adequate. In addition, although it is widely accepted that the presence of instability is a clear indication for fusion, a valid definition of radiographic instability is lacking. The amount of motion of flexion-extension films that signifies instability is still open to discussion and altered by the prior discectomy; and an accurate and reliable method of determining the extent of facet resection is currently not available.
There are limitations to the study. Despite similarities in baseline demographic, PROs, and radiologic data, variables that lead a surgeon to choose decompression alone or decompression and fusion remain unknown and can lead to selection bias. The method to determine the extent of facet resection is done from a single axial cut using a linear dimension. The extent of facet resection in other planes may be underestimated. Other confounders such as the size and location of the disc herniation was not included in the analysis. Longer follow-up would have been ideal to determine if fusion results in a more lasting improvement or less revision surgery that decompression alone or does not add any benefit.
In conclusion, for a first episode recurrent disc herniation, surgeons can expect similar outcomes whether patients are treated with decompression alone or decompression and fusion. Further studies are needed to identify clear indications for fusion in patients with first episode recurrent disc herniation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SG and RRC have no relationships to disclose. LYC: AO Spine: Paid consultant, Editorial Advisory Board Spine, The Spine Journal: Editorial or governing board, Norton Healthcare: Employee, board or committee member, Spine Deformity: Editorial or governing board, Trips and Travel from Center for Spine Surgery and Research, University of Denmark: Other financial or material support, University of Louisville Institutional Review Board: Board or committee member. EFB: AANS Ethics, AANS/CNS Spine SPC: Board or committee member, Journal of Neurosurgery: Spine: Editorial or governing board, MiRus: Paid consultant, nView: Paid consultant; stock or stock options. EAP: AANS/CNS Joint Section on Disorders of the Spine and Peripheral Nerves: Board or committee member, Medtronic: IP royalties; paid consultant. SDG: K2M: Paid consultant, Medtronic: IP royalties; paid consultant, Scoliosis Research Society: Board or committee member. MEB, LYC, and SDG: Institutional research support from Pfizer, Lifesciences Corporation, IntelliROD, Cerapedics: Research support, Scoliosis Research Society, National Institutes of Health, Fischer-Owen Kotcamp Fund, International Spine Study Group, Texas Scottish Rite Hospital.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.