
Abstract
Study Design
Biomechanical testings and finite element analysis.
Objectives
This study aims to investigate how annulus fibrosus (AF) incision size (RIS, Ratio of incision width to AF height) and shape affect intervertebral disc (IVD) biomechanics.
Methods
A validated finite element model of lumbar spines simulated various incisions in the middle-right posterior region of the AF, with different sizes and shapes. Simulations included axial compression, flexion, extension, bending, and rotation. Parameters assessed included stability, re-herniation, and IVD degeneration by analyzing stress, height, Intradiscal pressure (IDP), and the range of motion (ROM).
Results
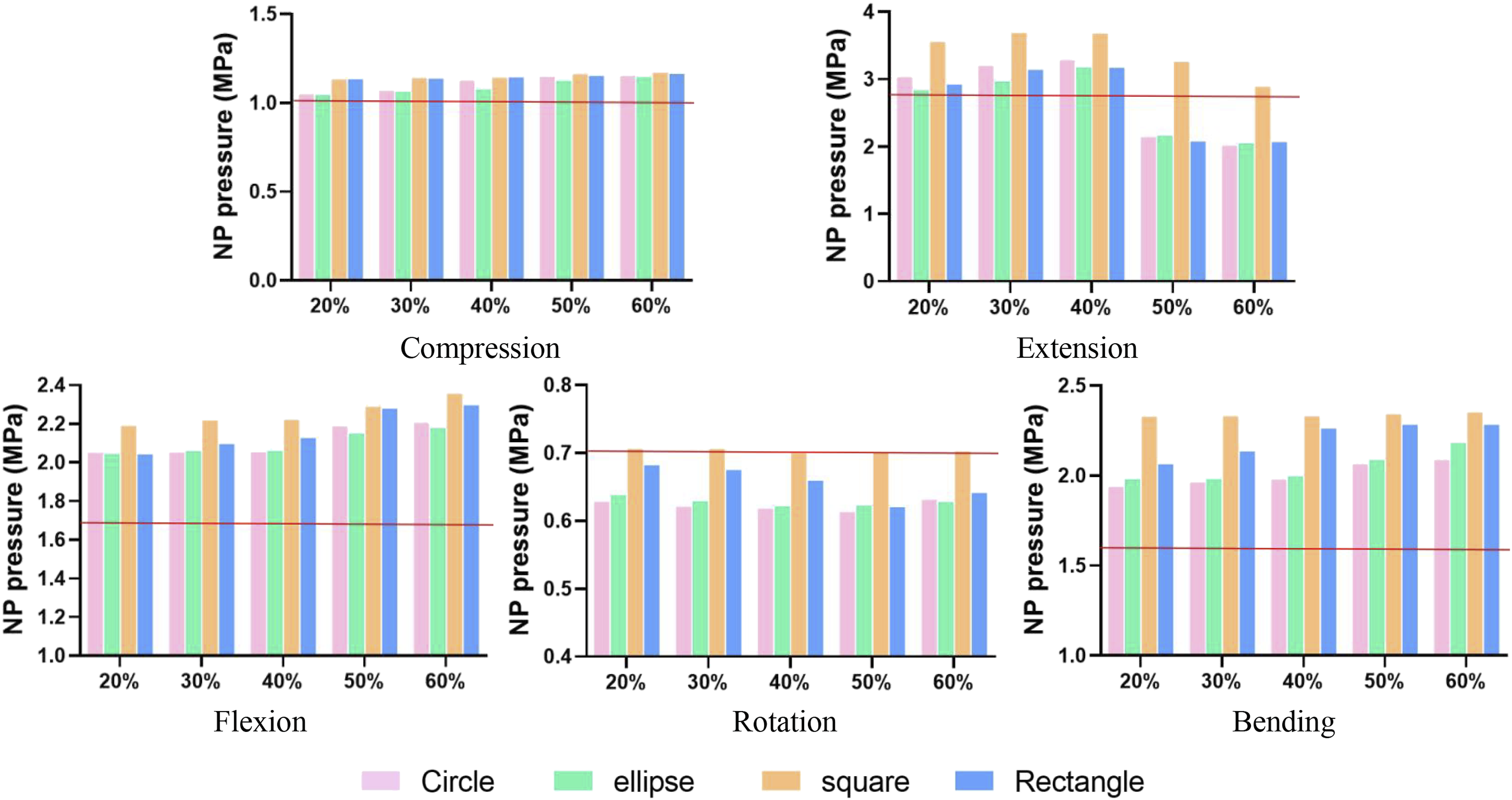
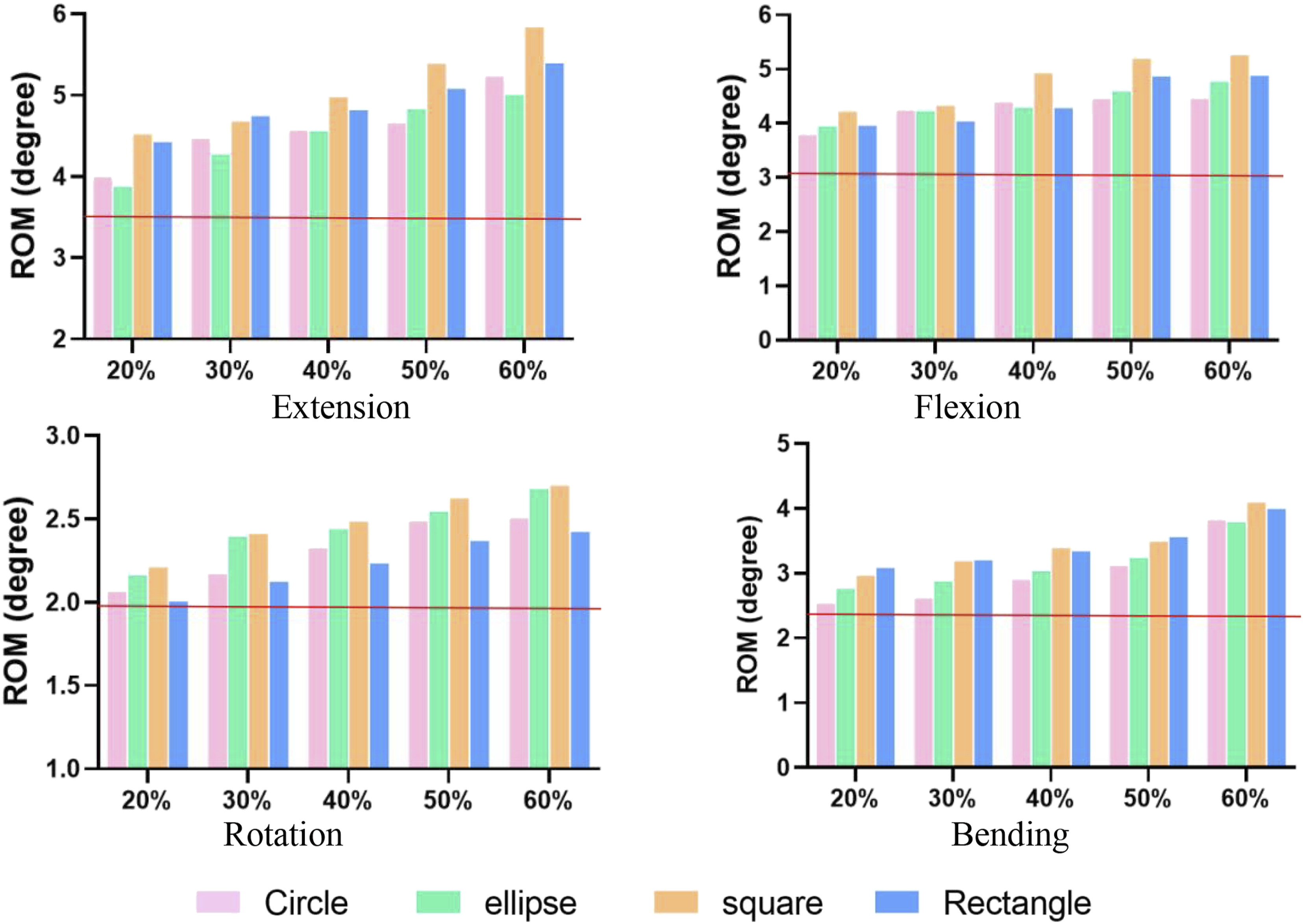
Incision increased AF stress and ROM under 3 Nm moment, with values rising as RIS increased. RIS exceeding 40% resulted in a 20% AF stress increase during compression and extension, while RIS over 50% led to over 20% AF stress increase during other motions. Incision stress also increased with higher RIS, particularly surpassing 50% RIS. IDP rose across all incision shapes. Endplate stress increased (9.9%-48.9%) with larger incisions, with average increases of 12.8%, 12.7%, 30.5%, and 22.8% for circular, oval, square, and rectangular incisions. Compression and rotation minimally affected NP pressure (<15%), while flexion (19.8%-38.8%) and bending (18.5%-43.9%) had a more pronounced effect. ROM increased with RIS (20.0% ∼ 77.4%), especially with an incision RIS exceeding 40%.
Conclusions
AF injury elevates AF stress, reduces spine stability, heightens degeneration risk with increasing RIS. Reherniation risk rises when RIS exceeds 40%. Circular or oval incisions maintain spine biomechanics better than square or rectangular ones.
Introduction
Intervertebral discs (IVDs) are pivotal components of the human vertebral column and are crucial for maintaining both mobility and stability. IVDs consist of two main structures: the nucleus pulposus (NP) and the annulus fibrosus (AF). Under axial compression, the AF, characterized by its high stiffness, restrains the NP from herniating. 1 Nevertheless, the aging process or injury can damage the AF and allow nuclear substrates to escape, which can lead to the onset of chemical radiculitis, accompanied by persistent back and/or leg pain. 2
Discectomy is a widely practiced surgical intervention for treating disc herniation, effectively alleviating the associated painful symptoms. 3 An incision may be created by a surgeon to remove nuclear substrates from compressing surrounding nerves, thereby achieving decompression. A study examining nearly 900 patients undergoing discectomy revealed that 39% of patients already had a large AF incision, a figure that increased to 77% after surgery. 4 While surgical intervention provides relief, patients with annular incisions face a notable risk of symptomatic recurrence and reoperation, with reported rates ranging from 2% to 25%. 5 Consequently, proactive measures are imperative to reduce the incidence of postoperative complications.
An AF incision, as performed during the treatment of symptomatic lumbar disc herniation, would alter the biomechanical properties of the affected disc. 6 However, even when the same surgical techniques are used to repair the AF, the outcomes are inconsistent, possibly due to a lack of standardized definitions for the AF incision. Various publications have proposed different incision sizes, ranging from 3 mm to 6 mm, 7 but none have garnered substantial consensus for use in clinical practice. Moreover, considering individual differences in the IVD height, using the relative incision size (RIS, Ratio of incision width to AF height) may be a better parameter for defining an incision. In addition, Thanikachalam et al. 8 found that the effectiveness of incision closure was influenced by the incision shape, but this factor is often overlooked in clinical practice. Surgeons often use a variety of instruments to disrupt the AF to remove the protruding NP, resulting in incisions that are square, rectangular, circular, or oval in shape. 9 Different incision shapes might have different effects on the pressure-volume characteristics of the involved disc, yet there is no standard shape for AF incisions in surgery. Therefore, it is meaningful to investigate the influence of incision shape on disc behavior.
The purpose of this study is to assess how the AF incision size and shape affects the IVD stability and flexibility, which can impact the risk of NP reherniation and disc degeneration. A finite element model of porcine lumbar spines was constructed from MRI scans and a discectomy was simulated with different incisions. It was hypothesized that larger and non-circular incisions would increase the risk of NP reherniation and disc degeneration following discectomy.
Method
Specimen Preparation
Twelve spines from 1-year-old pigs weighing 150-200 kg were purchased from a slaughterhouse. Specimens were stored at 20°C until the day prior to use, then thawed overnight (<24 hours) at room temperature. Before experimentation, the L5-L6 segment from each porcine lumbar spine was divided with a bone cutter with the cutting surface flush with the edge of the adventitia disc, and all adjacent soft tissues, spinous, transverse processes and muscles were removed keeping the anterior/posterior ligaments intact. The spines were maintained at 4°C to allow full hydration before mechanical testing (Figure 1A). (A) Experimental samples of porcine lumbar. (B) Finite element model of porcine lumbar. (C) Schematic representation of axial compression with L5-L6 specimens. (D) Force-displacement diagram for 5 cycles of axial compression.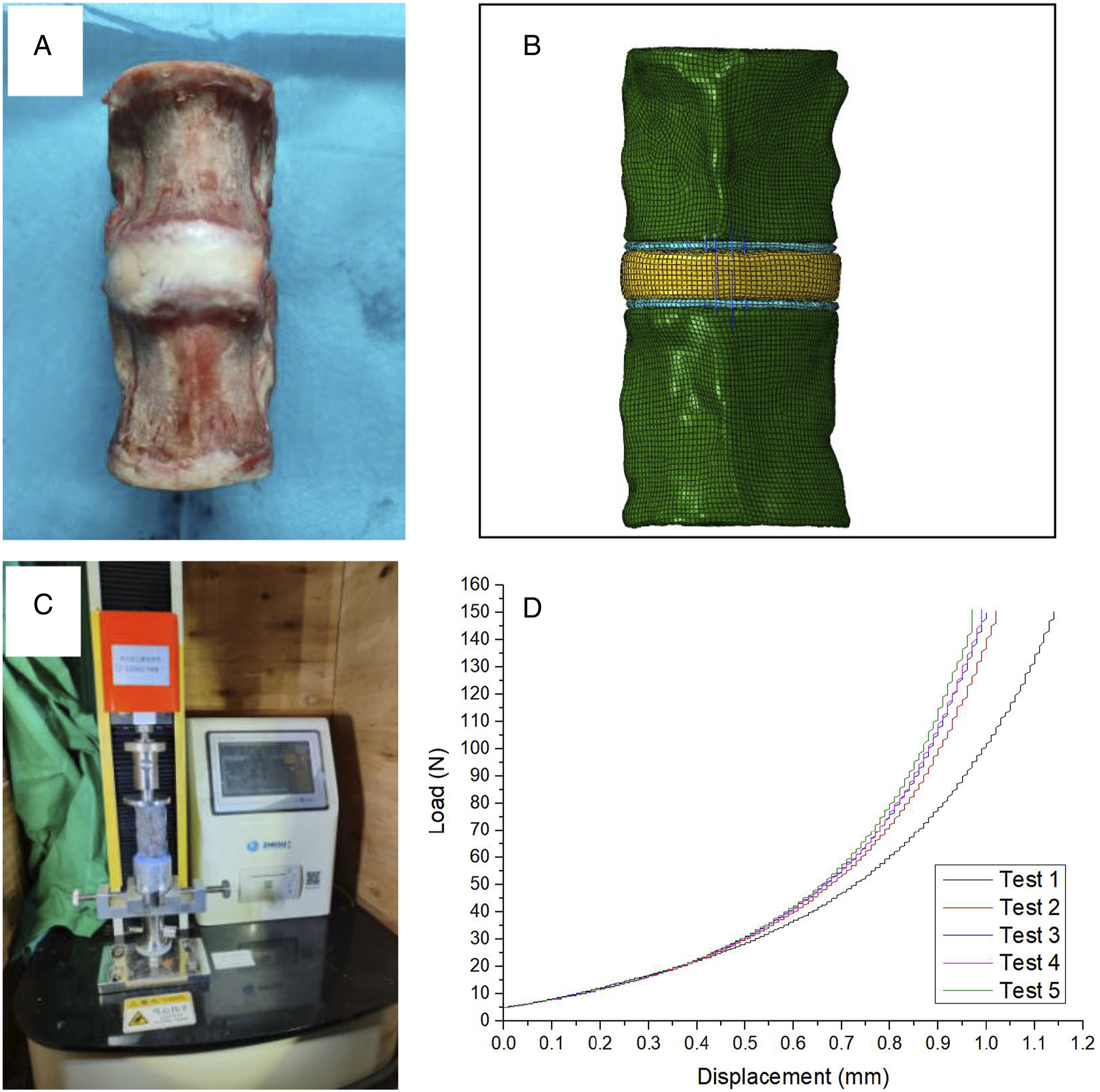
Model Reconstruction
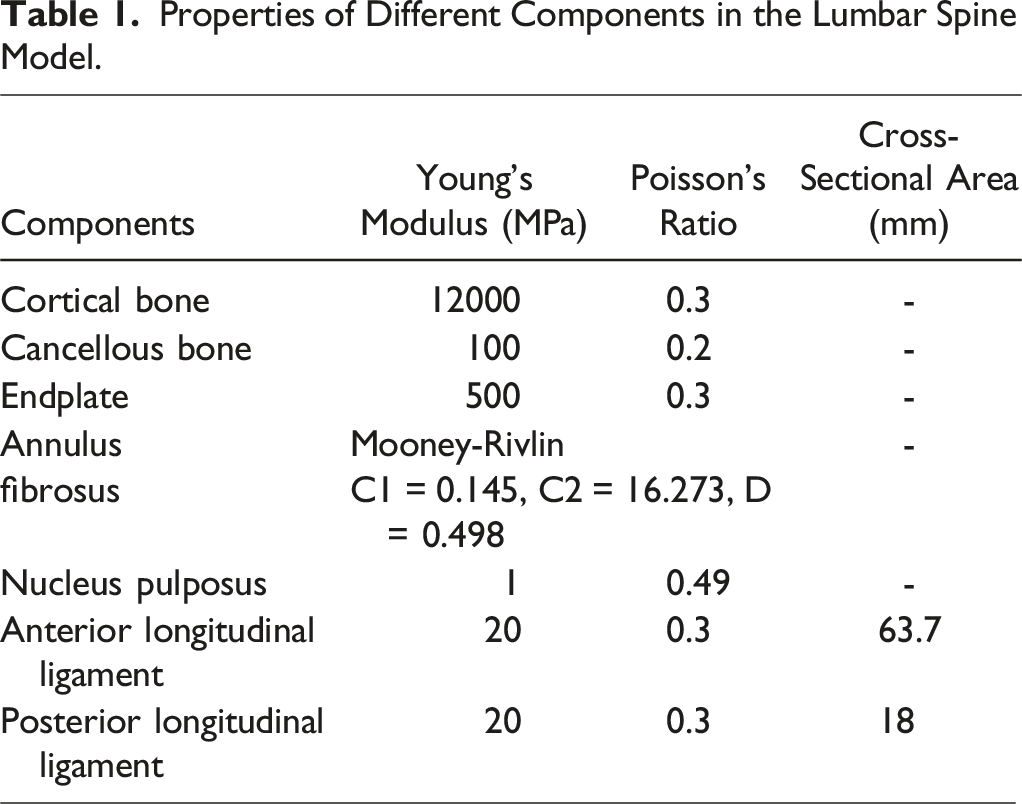
The lumbar vertebrae underwent MRI scanning (SIEMENS MAGNETOM Skyra, Germany) at 0.2 mm resolution at Shanghai Ninth People’s Hospital. MRI images were screened for degeneration absence, and differentiation of bone, endplate, annulus fibrosus (AF), and nucleus pulposus (NP) was conducted using Amira 6.7 (Thermo Fisher Scientific, Waltham, MA, USA). A three-dimensional lumbar model consisting of the L5–L6 functional spinal unit was reconstructed in Amira using the average values of the anatomical parameters measured from the MRI scans of the twelve porcine spines. The model incorporated 1 mm thick cortical bone, and ligament insertion locations referenced from anatomical attachment points. Built with hexahedral elements, the model (Figure 1B) included the cortical bone, cancellous bone, endplate, NP, AF, anterior longitudinal ligament and posterior longitudinal ligament.
Properties of Different Components in the Lumbar Spine Model.
Model Validation
After MRI scanning, specimens underwent in vitro testing. Six lumbar vertebrae were randomly selected to explore force-displacement curves, mitigating cadaveric swelling bias. Approximately one third of each vertebral body was fixed in quick-hardening plaster and secured in a custom biomechanical test apparatus (Precision Instruments, ZHIQU, China) (Figure 1C). Specimens underwent five load–unload cycles at 5 mm/min, corresponding to a moment of 150 N. 11
Michalek et al. 12 found that disc height and torsional stiffness were the most sensitive properties to annular injury. Therefore, axial compression and torsional loading was placed on the lumbar spine in this study. Axial compression with a rate of 5 mm/min up to 400 N and torsional loading with a rate of 0.25°/s up to 3 Nm were applied at six lumbar vertebrae to assess spine response to injury. Compression stiffness, torsional angle and stiffness were recorded. In vitro experiments were replicated in Abaqus and compared to validate the finite element model.00
Effect of Incision Shape and Size on Reherniation and Degeneration
Four types of annular incisions (Figure 2) were made in the right postero-lateral quadrant at the annulus midsection of the model
13
to evaluate the effect on reherniation and disc degeneration, including circular, oval, square and rectangular shapes. All incisions had the same center point and area, but varied in size of 20%, 30%, 40%, 50%, and 60% of the AF height (Figure 2). One intact model and twenty injury models were ultimately reconstructed. A 3 Nm moment was applied in various directions to simulate flexion, extension, lateral bending, and axial rotation. Additionally, a 400 N compression force was applied to simulate gravitational effects. The main variables included spinal segment range of motion (ROM), intradiscal pressure (IDP), IVD height, and the maximum von Mises stress on the endplates, AF, and incisions. Results are presented as median values with confidence intervals (CI). The left column shows incisions of different shapes (RIS of 40%) and the right column shows circular incisions of different sizes.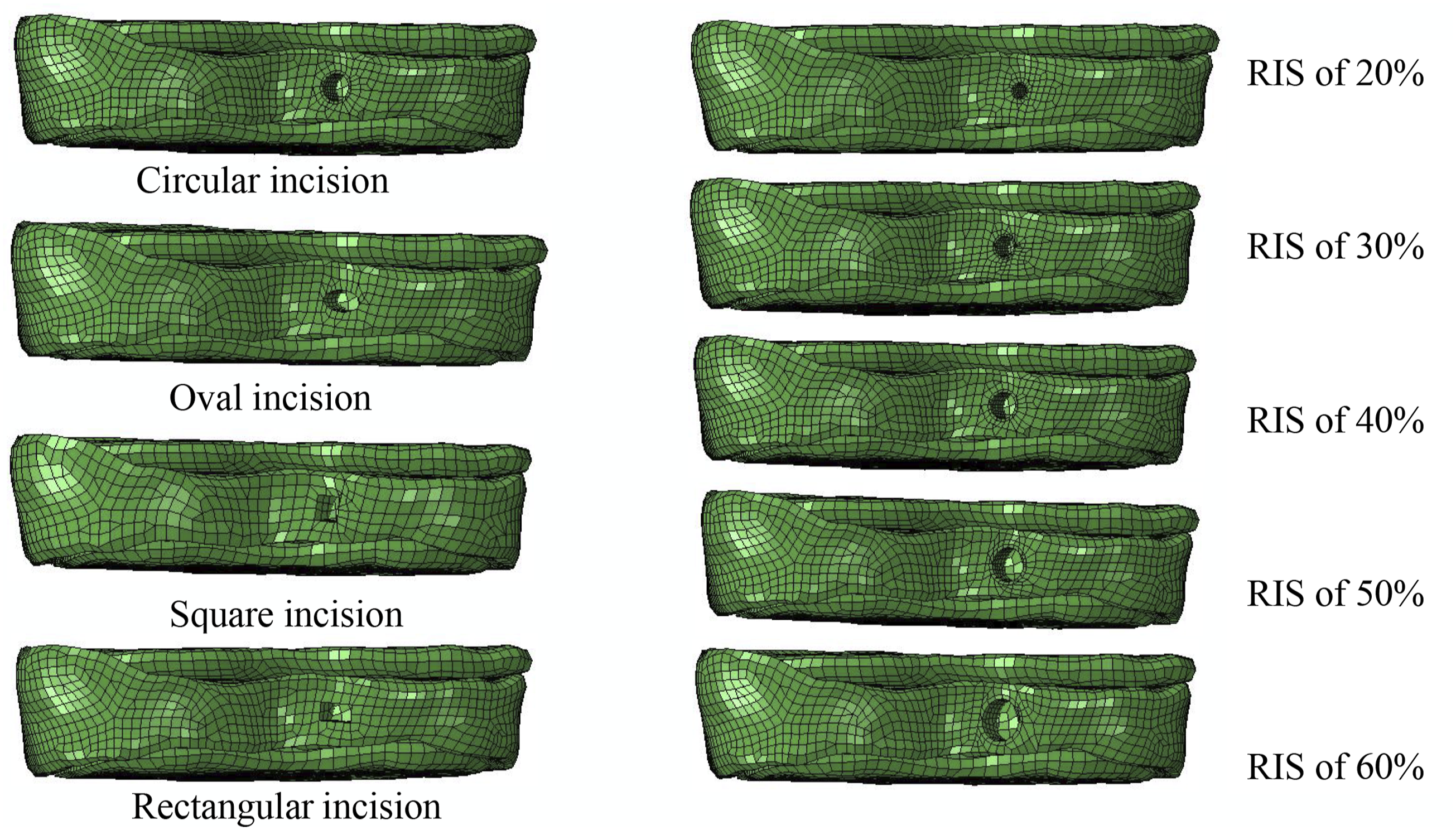
Results
Validation of the Intact Lumbar Finite Element Model
The Change Magnitude in Compressive Stiffness Relative to the Previous Model.
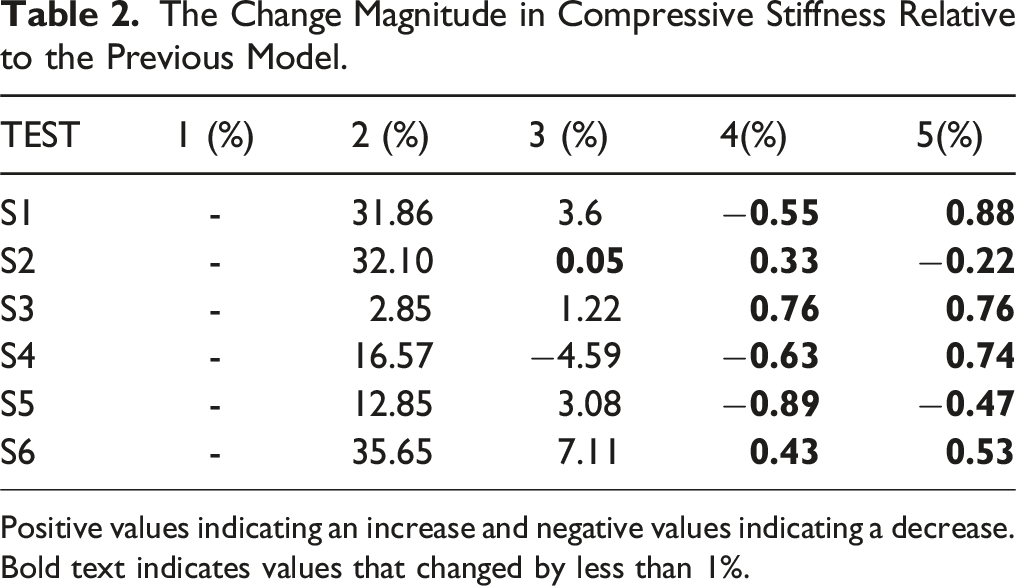
Positive values indicating an increase and negative values indicating a decrease.
Bold text indicates values that changed by less than 1%.
During compression testing, axial displacement ranged from 0.90 to 1.45 mm, with compression stiffness between 239.4 and 363.3 N/mm. Under a torque of 3 Nm, torsion angles varied from 2.46° to 5.67°, with torsional stiffness ranging from 1.44 to 3.17 Nm/°. In the intact lumbar spine model, axial displacement measured 1.07 mm, compression stiffness was 267.4 N/mm, torsional angle was 3.76°, and torsional stiffness was 1.85 Nm/°. Finite element simulation results aligned with in vitro experimental data, indicating satisfactory agreement between experimental and numerical models.
Biomechanical Properties of Different Types of AF Incisions
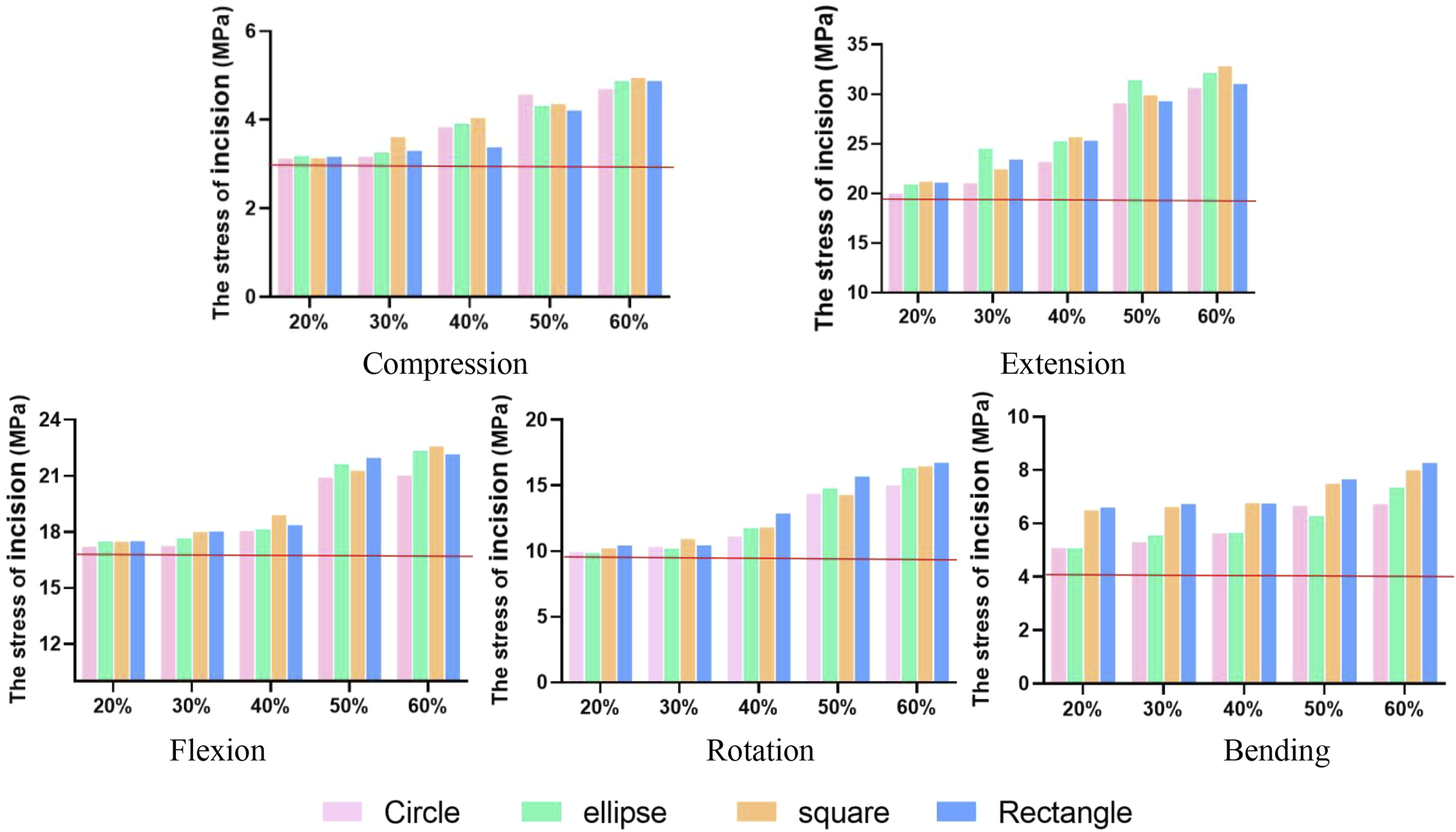
Figures 3 and 4 depict that incisions with RIS > 40% caused over a 20% rise (21.2%-120.0%) in AF stress during compression and extension compared to intact models. RIS over 50% led to 22.3%-74.3% increase in AF stress during flexion, bending, and rotation. Incision stress increased by 22.8%-102.4% for RIS > 50%. Specifically, increasing RIS from 40% to 50% resulted in a 14.0-33.8% increase in AF stress and a 10.0-33.8% increase in incision stress, more pronounced with square and rectangular incisions vs circular and oval shapes. The annulus fibrosus stress under 400N compression or 5Nm moment. The red horizontal line indicates the value for the intact model. The stress of incision under 400N compression or 5Nm moment. The red horizontal line indicates the value for the intact model.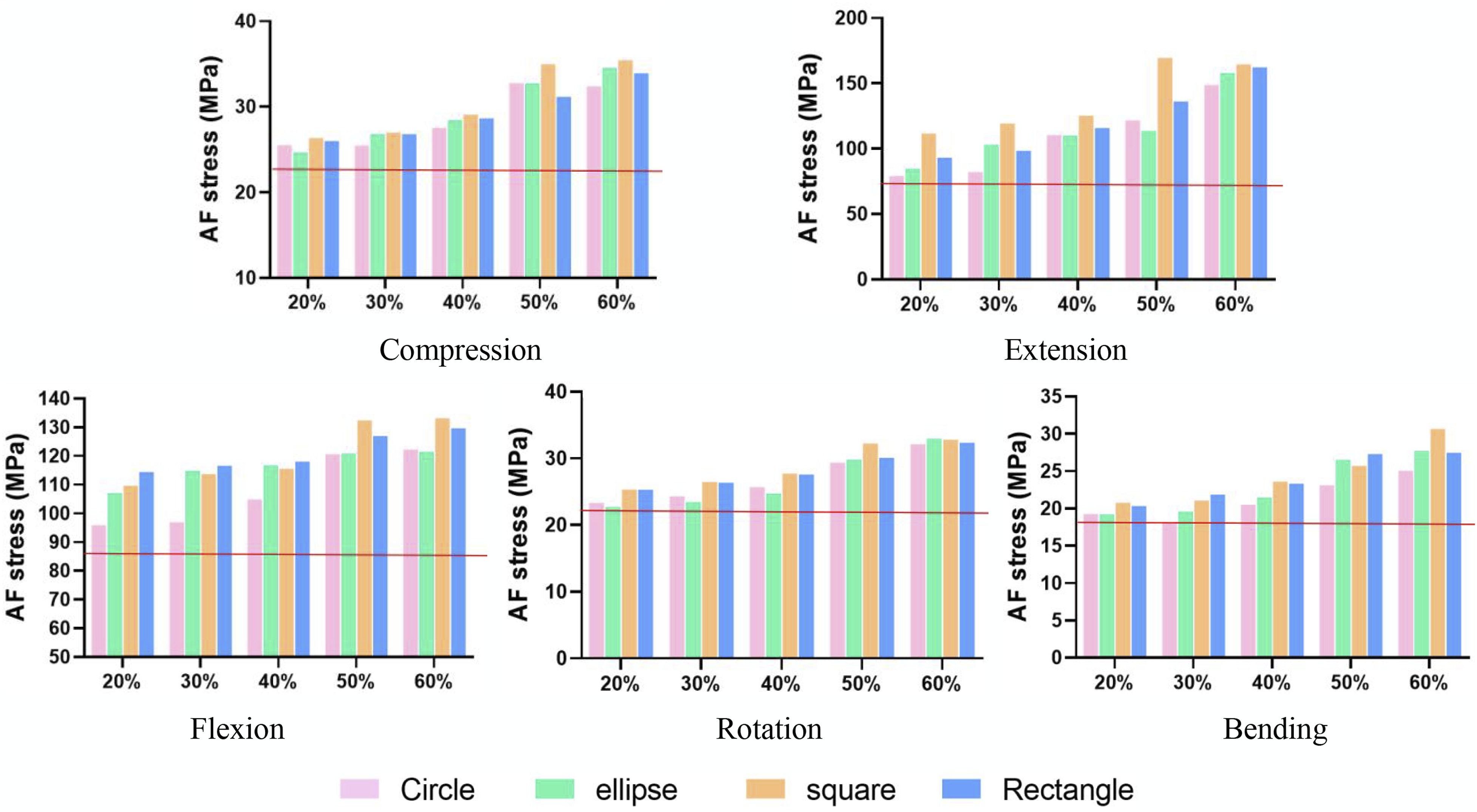
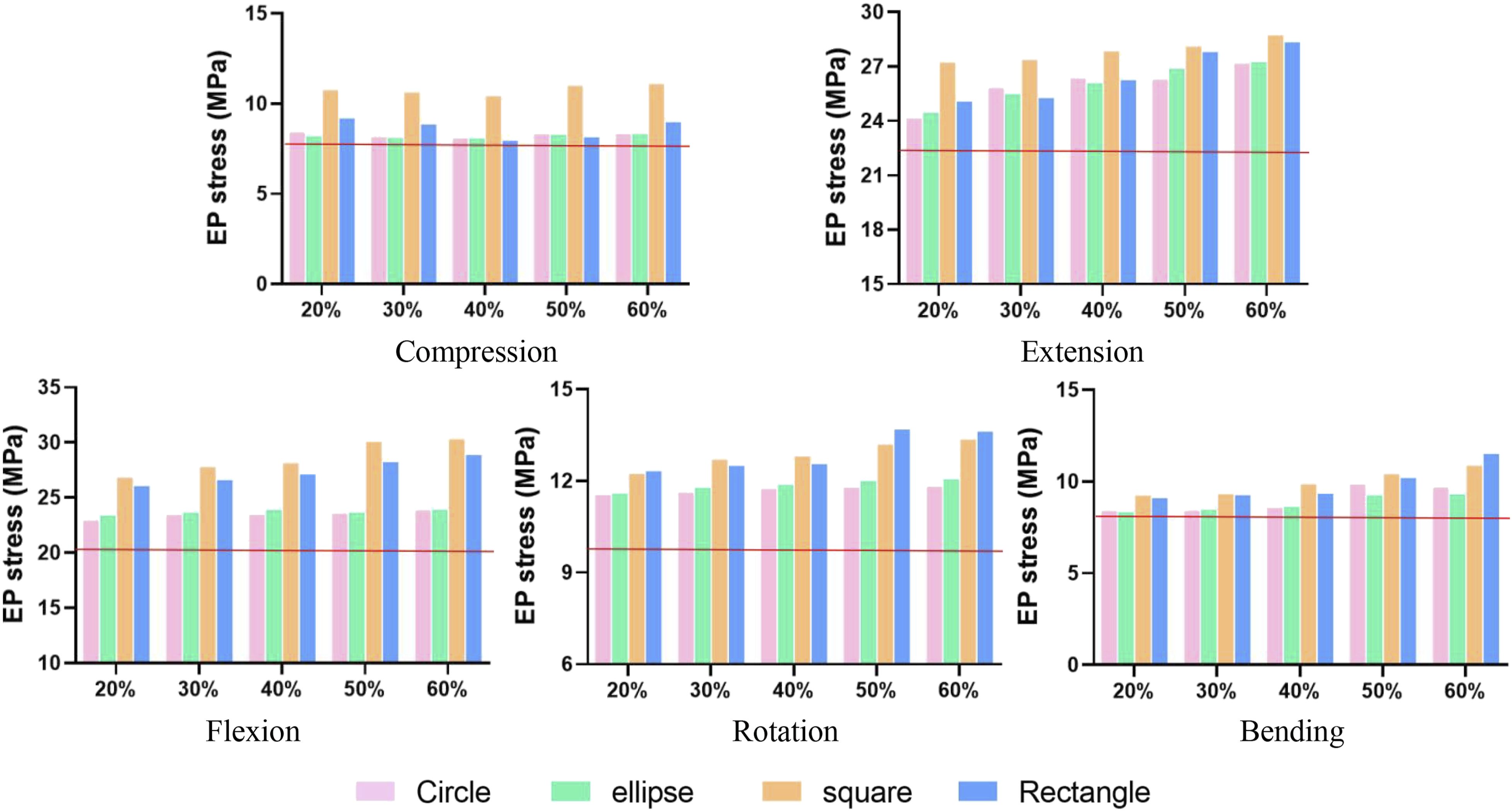
Increased displacement percentages for circular, oval, square, and rectangular incisions were 3.3% (IC: 2.4%, 5.0%), 4.0% (IC: 2.9%, 5.9%), 12.1% (IC: 11.3%, 14.5%), and 12.8% (IC: 10.0%, 14.2%) (Figure 5). EP stresses and NP pressure were essentially unchanged in compression. Under a 3 Nm moment, EP stress rose noticeably, with growth rates of 15.2% (CI: 9.8%, 15.7%), 15.7% (CI: 9.0%, 15.0%), 30.7% (CI: 27.1%, 34.0%), and 24.8% (CI: 17.9%, 27.7%) for circular, oval, square, and rectangular incisions (Figure 6). NP pressure continuously increased, but with incisions exceeding 40%, NP pressure dropped significantly below intact levels, indicating potential leakage (Figure 7). As incision size increased, ROM increased during flexion, extension, and bending by 20.0%-77.4% over the intact model, with increments of 27.2% (IC: 21.7%, 36.0%), 30.7% (IC: 25.9%, 38.8%), 46.5% (IC: 33.2%, 50.9%), and 36.4% (IC: 27.4%, 44.5%) for circular, oval, square, and rectangular incisions (Figure 8). The displacement of intervertebral disc under 400N compression or 5Nm moment. The red horizontal line indicates the value for the intact model. EP stresses in the intervertebral disc under 400N compression or 5Nm moment. The red horizontal line indicates the value for the intact model. NP pressure in the intervertebral disc under 400N compression or 5Nm moment. The red horizontal line indicates the value for the intact model. Range of motion of the intervertebral disc under 5Nm moment. The red horizontal line indicates the value for the intact model.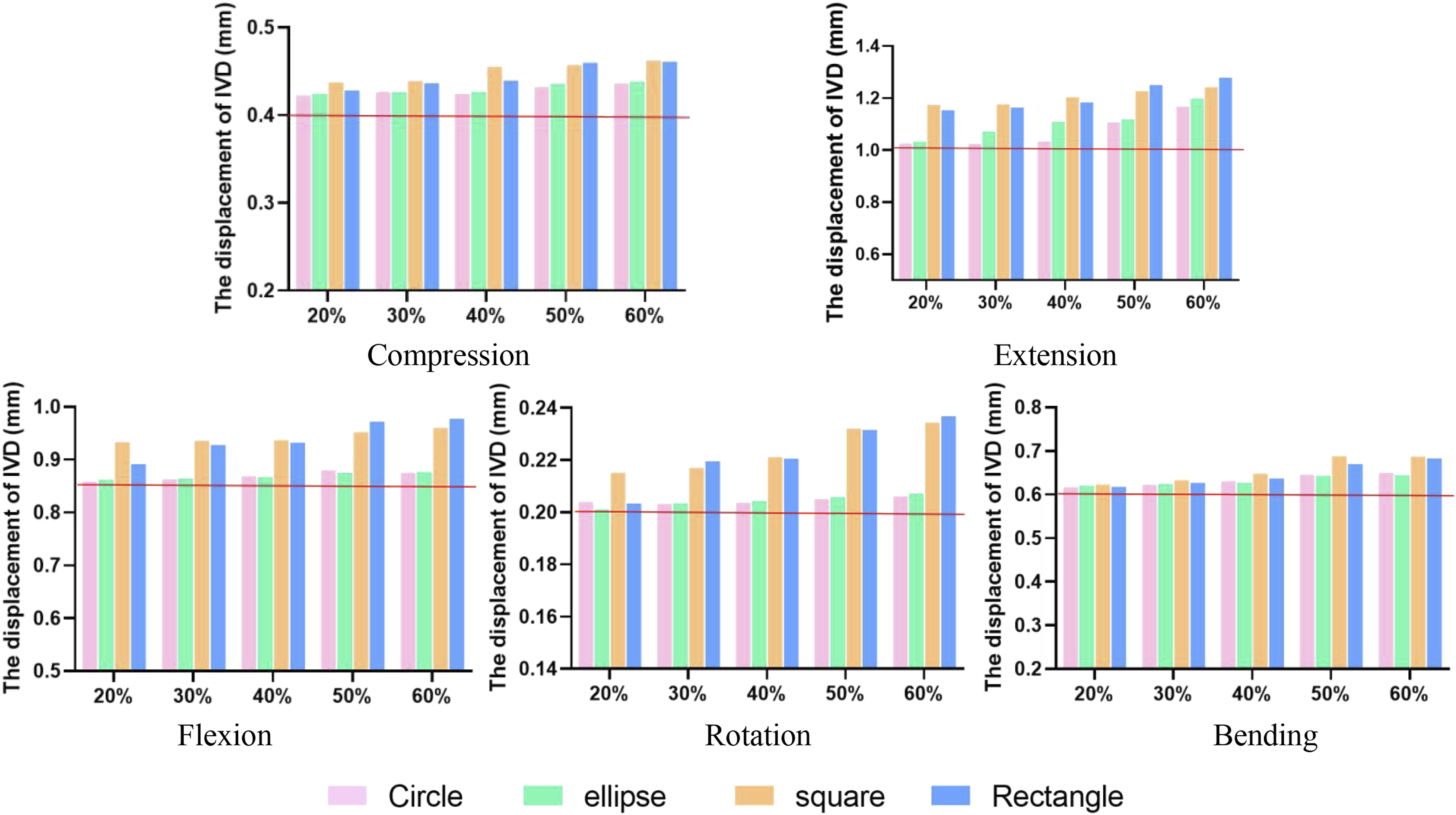
Discussion
NP herniation can occur due to natural disc rupture from trauma or intentional incisions, with varying shapes and sizes. Surgeons often need to modify AF injuries intraoperatively, yet standardized techniques for determining optimal incision size lack consensus. This study developed a validated three-dimensional finite element model of lumbar motion segments to investigate how incision size and shape affect the biomechanics. Incision RIS and shape are key factors influencing IVD mechanical properties. Compared to intact models, AF incisions increased IVD stress and compromised lumbar stability, with larger incisions decreasing stability and increasing degenerative risk. Notably, expanding incision RIS from 40% to 50% led to abrupt changes in AF stress and NP pressure, indicating elevated reherniation risk. Li et al. 14 also demonstrated that the disc stress changes mainly stemmed from AF tissue. Incision shape significantly impacted biomechanical changes, with circular or oval shapes better preserving stability and mobility than square or rectangular ones. These findings offer crucial clinical insights and guide surgeons in optimizing lumbar discectomy outcomes by selecting appropriate incision size and shape.
In a herniated disc, the AF may or may not be ruptured prior to discectomy, but surgeons often create an AF incision by trimming the herniated area. The sizes and shapes of the incisions are determined by the surgeon based on patient condition and preferences. A compromised AF has limited intrinsic healing ability, while remaining tissue (undamaged AF or internal NP) may maintain load resistance. 9 However, Wang et al demonstrated that patients undergoing lumbar discectomy combined with annular repair had lower rates of recurrence and reoperation compared to those with discectomy alone, 15 highlighting the benefits of AF repair. Current repair results are controversial, with the definition of the AF incision requiring repair lacking standardized guidance.
The size of the AF incision post-lumbar discectomy have a substantial impact on patient outcome. Standardizing criteria for repairable annular incisions is crucial. Clinically, incision width is often assessed using a No. 1 Penfield probe (6 mm), with over 6 mm considered large in many studies, and one study reported a postoperative annular incision > 6 mm in 30% of patients after disc removal. 16 Carragee’s et al., 17 THOMé et al. 18 and Kim’s et al. 19 reported high recurrence rates of 27%, 25%, and 18%, respectively, after short-term follow-up (<2 years) for incisions of >6 mm. Miller et al. 16 found a 3-fold higher recurrence rate for incisions larger than 6 mm. However, Guterl et al. 20 noted incisions (>3 mm) with more inner annulus damage had higher recurrence risks. There are also some clinicians who consider >5 mm a large incision because they sometimes repaire AF with a 5 mm wide knife. 21 Studies suggest varied incision sizes due to clinician preference and training, contributing to different repair outcomes.
Previous studies proposed specific incision sizes (e.g., 3 mm, 5 mm, or 6 mm), but individual IVD sizes vary, making the relative incision size (RIS) a more consistent parameter. The results of this study show that increasing RIS destabilizes the IVD, increasing degeneration risk. Larger incisions compromise IVD structure, weakening its pressure resistance, potentially leading to NP re-protrusion and intervertebral height narrowing. Notably, when RIS increases from 40% to 50%, significant changes in AF stress, incision stress, NP pressure, and ROM occur, indicating possible IVD collapse. Elliott et al. 22 reported on how the relative needle diameter in puncture and sham injection animal models affects disc degeneration. They found no effect when the needle diameter was less than 25% of the disc height. For needle diameters of 25% to 40% of the disc height, the effect of needle puncture was inconsistent but not significant. When the needle diameter is greater than 40% of the disc height, mechanical changes in the disc are common. This is consistent with our findings and further suggests that when the incisional RIS is greater than 40%, some restorative measures should be taken in advance to prevent re-prominence and regression of the IVD. Our study observed maximum axial displacement near the incision site, and the incision appeared to be deformed after the application of force. The large increase in maximum principal motions caused by annular incisions can cause the matrix to fail.
Ahlgren et al. 23 compared the efficacy of straight transverse slit, cruciate incision, and window or box excision, noting that window or box excision had the highest re-prominence risk and yielded poor restorative outcomes. The amount of AF tissue removed significantly differed among the three incisions, with those preserving more tissue exhibiting stronger resistance to pressurization. However, in cases of substantial AF rupture, such as due to trauma, or when extensive NP removal is necessary, a large incision may be unavoidable. Given the heightened herniation recurrence risk with large incisions, understanding intraoperative incision preparation is crucial. Although Ahlgren et al. 23 documented varying effects of box excisions, straight transverse slits, and cruciate incisions on IVD, none explored the relationship between large incision size, shape, significant AF tissue loss, and resulting post-surgical biomechanical properties. This study compared circular, oval, square, and rectangular incisions of equal area, revealing rectangular and square incisions causing greater displacement, EP stress, and NP pressure than circular and elliptical ones. Reduced disc height and axial compliance signal IVD degeneration, with square and rectangular incisions posing higher risk of AF collapse, endplate fracture, and degeneration of the IVD. Circular and oval incisions, being more rounded, exhibit lower stress concentrations compared to their right-angled counterparts. Although both circular and oval incisions outperformed four-sided ones, the oval shape offers advantages in encapsulating various AF ruptures.
The results indicate lower NP pressure with larger incisions during extension and rotation. Reduced intradiscal pressure in the annulus decreases AF tension and may increase bulging, raising the risk of serial tears. 24 Incision shape or size did not impact transverse displacement, likely due to AF compensation. As shown in Figure 8, the change in NP pressure is small during compression, but large under torque. Previous in vitro have also found that compression alone often does not cause disc reherniation, but torsional loading is a risk factor. 25
The study has limitations. Firstly, it recognizes the inherent constraint of using animal models as substitutes for human subjects in experimental research, given logistical, ethical, and regulatory factors. While human clinical trials are preferred, preliminary investigations often rely on animal models. Despite anatomical differences, studies have shown the translational relevance of porcine lumbar spines to human physiology. Additionally, the study exclusively examined a single segment, disregarding neighboring segments. Due to the substantial number of experimental groups (21 groups), employing single-segment spinal functional units would be preferable. Additionally, our study did not include load-displacement data from experimental or finite element analysis (FEA) simulations. Our model focused on obtaining stress and strain results under predefined conditions rather than traditional load-displacement tests. While this allows precise analysis of specific parameters, it lacks comprehensive load-displacement curves that provide deeper insights into lumbar spine mechanics. Future research should include these tests for a more complete understanding and validation of the FEA model under dynamic loading conditions. Finally, this study focused more on the short-term results after repair and did not consider the long-term effects, which is another reason why only a single segment was considered, as the incidence of long-term complications such as neighboring segment disease is lower in that case, and therefore was not considered as a priority.
Conclusion
AF incision size and shape post-discectomy significantly affect IVD biomechanics. AF injury elevates IVD stress, reduces lumbar spine stability, and lager size increasing reherniation and degeneration risk. Circular or oval incisions better maintain lumbar biomechanics than square or rectangular ones. Surgeons should prioritize preserving annular tissue and consider to repair AF when the incision RIS is greater than 40%.
Footnotes
Acknowledgments
The research was conducted with support of the Engineering Research Center for Digital Medicine of the Ministry of Education. Mr. Colin McClean is acknowledged for his assistance with editing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Research Funds for the Central Universities (Grant numbers [AF0820060]).