
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To determine the incidence of index level fusion following open or minimally invasive lumbar microdiscectomy.
Methods:
We conducted a retrospective review of 174 patients with a symptomatic single-level lumbar herniated nucleus pulposus who underwent microdiscectomy via a mini-open approach (MIS; 39) or through a minimally invasive dilator tube (135). Outcomes of interest included revision microdiscectomy and the ultimate need for index level fusion. Continuous variables were analyzed with independent sample t test, and χ2 analysis was used for categorical data. A multivariate regression analysis was performed to identify predictive factors for patients that required index level fusion after lumbar microdiscectomy.
Results:
There was no difference in patient demographics in the open and MIS groups aside from length of follow-up (60.4 vs 40.03 months, P < .0001) and body mass index (24.72 vs 27.21, P = .03). The rate of revision microdiscectomy was not statistically significant between open and MIS approaches (10.3% vs 10.4%, P = .90). The rate of patients who ultimately required index level fusion approached significance, but was not statistically different between open and MIS approaches (10.3% vs 4.4%, P = .17). Multivariate regression analysis indicated that the need for eventual index level fusion after lumbar microdiscectomy was statistically predicted in smokers and those patients who underwent revision microdiscectomy (P < .05) in both open and MIS groups.
Conclusions:
Our results suggest a low likelihood of patients ultimately requiring fusion following microdiscectomy with predictors including smoking status and a history of revision microdiscectomy.
Keywords
Introduction
Lumbar microdiscectomy is the most commonly performed procedure in the United States for patients suffering from back or radicular pain as a result of a herniated disc. 1,2 Many studies have found lumbar microdiscectomy to be a particularly efficacious procedure, with high patient satisfaction with regard to restoration of function and elimination of pain. 3 –5 While the results are generally successful, the most common reported complication following lumbar microdiscectomy remains recurrent disc herniation. The reported incidence of recurrent disc herniation ranges from 3% to18%. 6 –10 Obesity, smoking, and persistence of weight lifting after surgery have been identified as potential risk factors. 10 –12
Since the advent of the lumbar discectomy in 1934 by Mixter and Barr, the technique has undergone a number of modifications including the introduction of the operative microscope allowing for an open microdiscectomy. Beginning with Foley et al, the first minimally invasive (MIS) tubular microdiscectomy was performed. 13 Multiple studies have since demonstrated the efficacy of MIS microdiscectomy, with results that are equal to or better than those performed via a traditional open approach. 14 –18 In spite of the excellent results, the overall rate of reherniation has not been demonstrated to be significantly less than the open approach. 15,18
While the rate of reherniation requiring revision discectomy is well established, the rate of spinal fusion after microdiscectomy has not been addressed in the literature. For many surgeons, spinal fusion is a viable option after recurrent disc herniation. A recent survey study by Mroz et al found that surgeons in practice for 15+ years were more likely to select revision microdiscectomy for a reherniation compared with less experienced surgeons who were more likely to select revision microdiscectomy with PLIF (posterior lumbar interbody fusion)/TLIF (transforaminal lumbar interbody fusion) (P < .001). 19 However, there are no published studies detailing the likelihood or rate of those patients with recurrent herniated nucleus pulposus who ultimately require an index level fusion.
The purpose of this study is to detail the rate of patients that undergo index level fusion following lumbar microdiscectomy in patients treated with a MIS or open approach. Furthermore, risk factors for both revision microdiscectomy and fusion will be identified.
Methods
A consecutive series of 174 patients who underwent an open or minimally invasive (MIS) microdiscectomy by a single surgeon between December 2008 and December 2012 at a single institution were retrospectively analyzed after institutional review board approval. The initial 39 patients underwent a traditional open lumbar microdiscectomy. The following 135 patients underwent an MIS lumbar microdiscectomy with the use of a 16 mm dilator tube and operative microscope. There was no overlap in the groups, as the change to MIS microdiscectomy represented a shift in the operative technique of the primary surgeon.
All patients underwent an initial trial of nonoperative care including activity modification, physical therapy, anti-inflammatory medications, opioid analgesics, or epidural injections for at least 3 months. Diagnostic inclusion criteria included radicular pain below the knee, positive straight leg raise, or a corresponding neurological deficit. All patients had a magnetic resonance imaging–confirmed disc herniation corresponding to the appropriate side and level of their clinical presentation.
Patients with multiple herniated levels requiring operative treatment or patients requiring procedures other than microdiscectomy were not included in the analysis. Additional exclusion criteria included early lumbar surgery, cauda equina syndrome, spondylolisthesis, and spine infection or tumor. Patient age, gender, smoking status, length of symptoms, body mass index (BMI), medical comorbidities, operative complications, insurance status, and adjacent segment degeneration were recorded. Indications for fusion after lumbar microdiscectomy included failed revision microdiscectomy, evidence of spondylolysis or spondylolisthesis, or segment instability.
Lumbar fusion following the index microdiscectomy was performed in the following patients: symptomatic reherniation with evidence of spondylosis, spondylolisthesis, or segmental instability. Additionally, if the patient had already undergone a revision microdiscectomy and was presenting with a recurrent herniation, these patients were also indicated for lumbar fusion. All risks and benefits of an additional operation were discussed at length with each patient considering revision. Severity of patient symptoms, potential for improvement, and the desire of the patient to undergo an additional procedure were taken into consideration before an agreement was made between the surgeon and patient to undergo reoperation. To the best of the treating surgeon’s knowledge, none of the patients sought treatment at another institution.
Statistical Analysis
Graphpad Prism v6.5 (La Jolla, CA) was utilized for statistical analysis with independent sample t test for continuous variables and χ2 analysis for categorical data. A multivariate regression analysis was performed to identify those patient factors that are predictive of fusion after lumbar microdiscectomy. Kaplan-Meier survivorship curves were created using the Mantel-Cox analysis (log-rank) to model survivability after microdiscectomy for both revision microdiscectomy and fusion. A P < .05 was used to denote statistical significance.
Results
Patient Characteristics and Demographics
Patient characteristics and demographics can be found in Table 1. There were 39 patients that underwent open lumbar microdiscectomy with an average follow-up of 60.4 months; 135 patients underwent MIS microdiscectomy with an average follow-up of 40.03 months (P < .001). The average patient age was 43.97 years in the open group and 42.12 years in the MIS group (P = .46). There were no significant differences in the percentage of females in each group, with 30.8% of the open group and 38.5% of the MIS group being female (P = .38). Five patients in the open group and 11 patients in the MIS group were active smokers at the time of surgery (P = .37). The BMI of the patients was significantly higher in the MIS group, 27.21 versus 24.72 (P = .03). There was not a statistically significant difference in operations at L2-3 and L3-4. There were a significantly higher percentage of operations performed at L4-5 and L5-S1 in the MIS group.
Demographics and Patient Characteristics of Open and MIS Microdiscectomy.
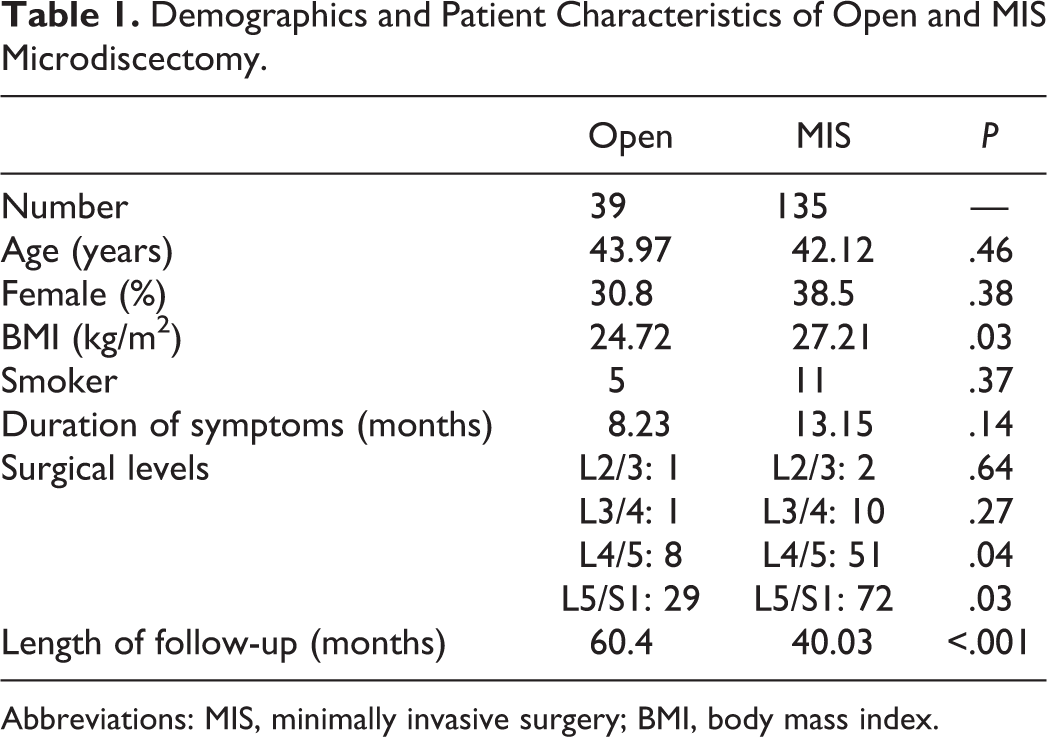
Abbreviations: MIS, minimally invasive surgery; BMI, body mass index.
Revision Discectomy
The rate of revision microdiscectomy in the open group was 10.3% (4/39), with the average time until discectomy of 9.25 months. The rate of revision microdiscectomy in the MIS group was 10.4% (14/135), with an average time to revision discectomy of 8.74 months. The time to revision discectomy was not found to be statistically different between the 2 groups (P = .90). There was no statistical difference in the rate of revision discectomy between the open and MIS groups (P = .99). The Mantel-Cox test of survivability found no statistical difference between the open and MIS groups (P = .80; Figure 1). A summary of the results of revision discectomy can be found in Table 2.
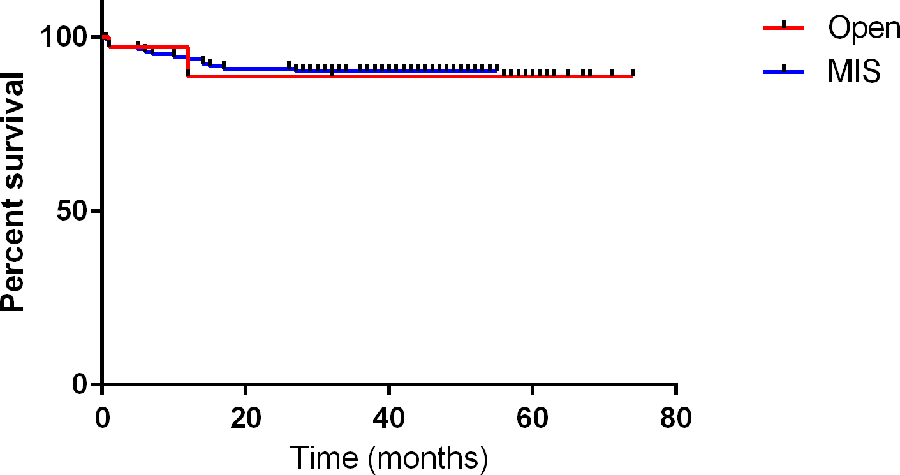
Kaplan-Meier revision discectomy survivorship curve shows percent survival of index lumbar microdiscectomy without undergoing revision microdiscectomy at index level in the y-axis with time (months) in the x-axis for both open and minimally invasive approaches.
Summary of Results for Revision Microdiscectomy and Fusion in the Open and MIS Groups.
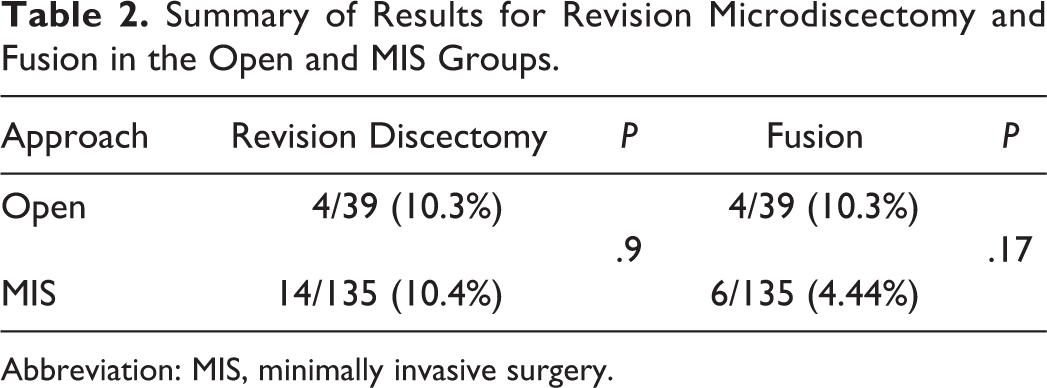
Abbreviation: MIS, minimally invasive surgery.
Revision Fusion
The rate of patients that went on to require an index level fusion following open microdiscectomy was 10.3% (4/39), with an average time after the initial discectomy until eventual fusion of 20.5 months. The rate of index level fusion following microdiscectomy in the MIS group was 4.44% (6/135), with an average time to fusion of 19.6 months. The time to fusion was not found to be statistically different between the 2 groups (P = .88). There was no statistical difference in the rate of fusion after discectomy between the MIS and open groups (P = .17). The Mantel-Cox test of survivability found no statistical difference between the open and MIS groups (P = 0.12; Figure 2). A summary of the results of those patients requiring index level fusion following microdiscectomy can be found in Table 2.
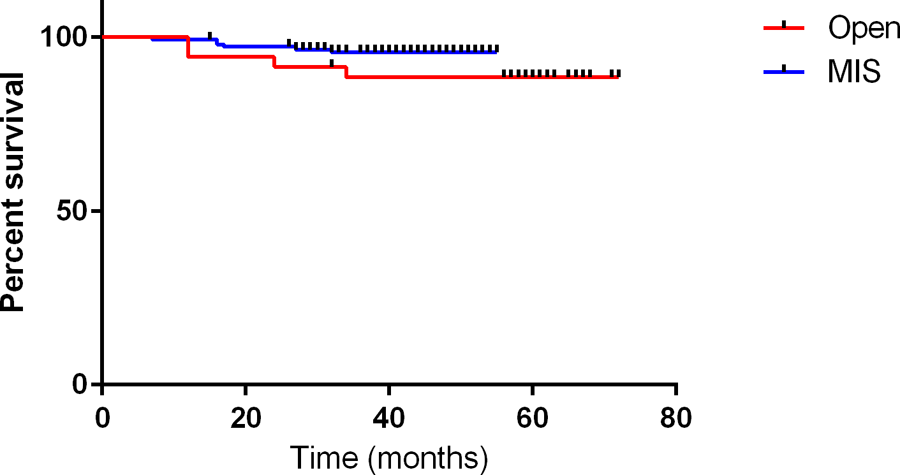
Kaplan-Meier fusion survivorship curve shows percent survival of index lumbar microdiscectomy without undergoing revision fusion at index level in the y-axis with time (months) in the x-axis for both open and minimally invasive approaches.
Multivariate Regression Analysis
A multivariate regression analysis was conducted to evaluate the factors that are predictive for patients ultimately requiring index level fusion after microdiscectomy. Patient age, gender, smoking status, length of symptoms, BMI, medical comorbidities, operative complications, insurance status, and adjacent segment degeneration were recorded. Basic descriptive statistics and regression coefficients are shown in Table 3. The results of the regression analysis indicated that 2 predictors (deep vein thrombosis and infection) explained 40.1% of the variance in the model. A significant regression equation was found (F[13,163] = 5.41; P < .00001). The overall model fit was R 2 = 0.27. Patients who ultimately progressed to fusion were significantly predicted by both smoking at the time of the initial microdiscectomy (β = 0.12, P = .04), as well as having undergone a revision microdiscectomy (β = 0.34, P < .0001). Insurance status, medical comorbidities, and presence of adjacent disc degeneration were not predictive of requiring eventual index level fusion (P > .05).
Multivariate Regression Analysis for Variables Predictive of Fusion After Lumbar Microdiscectomy.
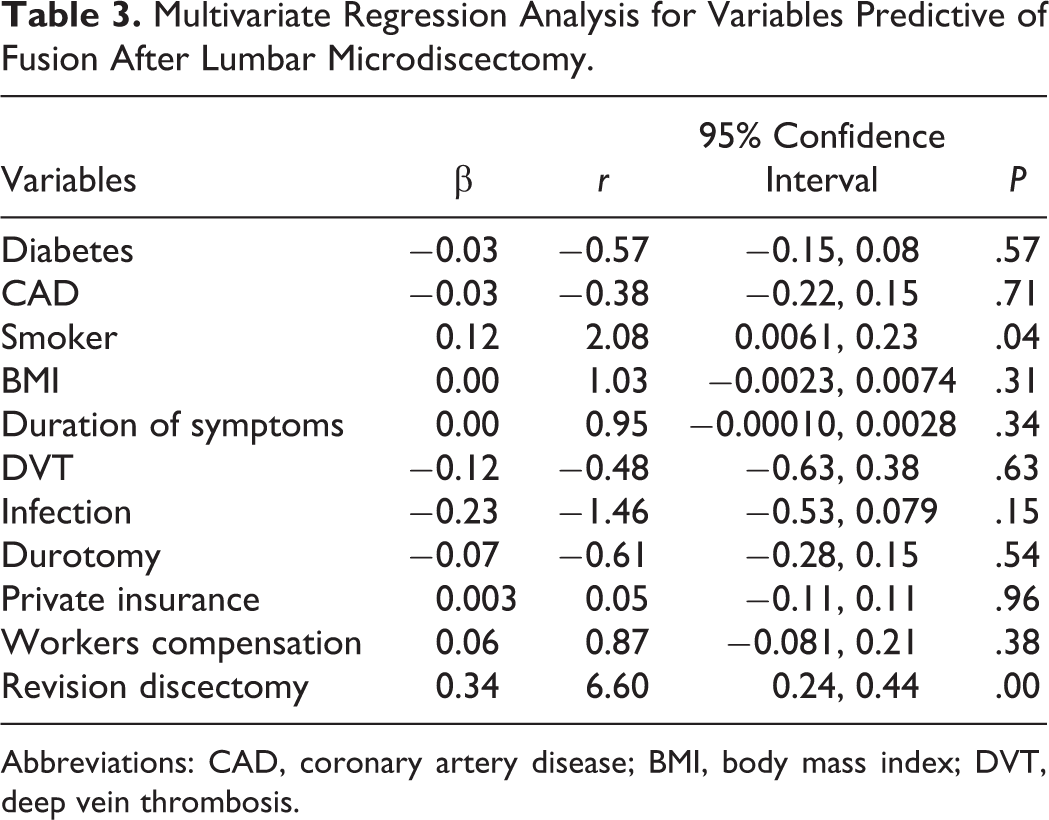
Abbreviations: CAD, coronary artery disease; BMI, body mass index; DVT, deep vein thrombosis.
Discussion
Lumbar microdiscectomy is the most commonly performed spinal procedure for the treatment of symptomatic herniated nucleus pulposus resulting in back pain or leg pain that is refractory to conservative measures. Clinical outcomes following lumbar microdiscectomy are generally excellent with 76.2% of patients returning to work by 1 year. 2 The most common complication following microdiscectomy remains a clinically significant reherniation, which occurs in 3% to 18% of cases. The rate of reherniation has not been shown to be different between open and MIS techniques, which paralleled the results of our study as well. The rate of patients that remain symptomatic after an index microdiscectomy and ultimately require index level fusion is a clinically relevant topic that has not been fully addressed within the literature up until this point.
This study is a retrospective review of 2 independent cohorts of patients that underwent either a standard open microdiscectomy or a tubular MIS microdiscectomy. Thirty-nine patients underwent a microdiscectomy with an open approach and 135 patients with an MIS approach. There were no significant differences between the 2 cohorts with respect to patient age, percentage of females, or smoking status. The length of follow-up was greater in the open cohort (60.4 vs 40.03 months), which was statistically significant. This coincides with the senior author’s transition to performing tubular microdiscectomies. Additionally, the BMI was found to be statistically higher in the MIS group (P = .03). This is not explainable by the transition and does not represent a predilection for the surgeon to perform tubular discectomies in patients with higher BMIs, as all patients after a certain date underwent a tubular approach. The average BMI in the open group was normal, while the BMI in the MIS group was slightly overweight (24 vs 27). BMI remains a clinically relevant patient variable as several authors have noted that increased BMI is a factor that may be predictive of reherniation or revision microdiscectomy. 12,20 –22 In our study, BMI was not predicative of either revision microdiscectomy or need for eventual fusion.
The rate of revision microdiscectomy was found to be 10.3% in the open group and 10.4% in the MIS group, which was not statistically significant (P = .99). The rates that we report are consistent with the existing literature for both approaches. Furthermore, survivorship analysis with the Mantel-Cox hazard ratio demonstrated that at 24 months, the open group had a survivorship of 88.57%, while the MIS group had a survivorship of 90.84%, which was not statistically significant (P = .80). Furthermore, the majority of clinically significant reherniations occurred in the first 12 months. It is possible to infer from this data that once a patient is 1 year from surgery, their risk of herniation is equivalent to that of the general population.
Lumbar fusion was indicated in our patient population after microdiscectomy if there was a symptomatic reherniation with failed conservative management and evidence of segmental spondylosis, spondylolisthesis, or instability. These criteria are similar to that of the general population with a virgin lumbar spine. The same criteria was used to indicate those who failed revision discectomy surgery. This is to say that the senior author did not have a different set of criteria for fusing a failed revision discectomy, regardless of the number of revisions. The surgical indications did not vary between the open and MIS groups. The rate of patients that required index level fusion following lumbar microdiscectomy was found to be 5.7% overall (10.3% in the open group and 4.44% in the MIS group; P = .17). There was no significant difference between the open and MIS groups in the time from initial microdiscectomy to eventual fusion (20.5 vs 19.6 months; P = .88). Furthermore, in the Mantel-Cox survivorship analysis there was a trend toward better survivability in the MIS group though this was not found to be statistically significant (P = .12). All of the fusions in both groups occurred within the first 30 months after microdiscectomy. Our model is not powered to predict the likelihood of long-term survival after microdiscectomy, with only a moderate time horizon of follow-up.
Accelerated disc degeneration at the microdiscectomy level has recently been a topic of interest in the literature. 23 The relationship between progressive disc degeneration following microdiscectomy and need for eventual fusion has not been established. Our results indicate that there is a low likelihood of fusion, about 5% after a primary microdiscectomy. In our regression model, active smoking status and a history of a revision microdiscectomy at the index level were predicative of patients that eventually required fusion. All other variables including adjacent segment disc degeneration at the time of index surgery, all medical comorbidities, and insurance status including workers compensation were not predictive of fusion.
The major limitations of this study are the retrospective nature and the unequal number of patients between the 2 cohorts. This was not a matched cohort study. Instead, this is a retrospective review of a single surgeon’s consecutive series of patients. Though there was a large disparity in the numbers between the 2 groups, there were no significant differences between the 2 groups with regard to age, medical comorbidities, insurance status, length of symptoms, or smoking status. The BMI was found to be significantly different between the 2 groups, with the MIS group being, on average, more overweight. This difference was not found to be clinically significant in our study, as BMI was not shown to be predictive of either revision discectomy or fusion.
Another potential limitation would be patients that chose to have a revision procedure with a different surgeon. All patients in this study were successfully contacted by phone or in person for follow-up. Patients were asked whether they had developed a reherniation requiring a secondary procedure at any time point after their index operation and when that occurred. A positive response was recorded and details were obtained on the revision procedure and included in the analysis. It also must be considered that there was a selection bias for choosing who underwent revision surgery and fusion after microdiscectomy. This was a retrospective study and the treating surgeon was not aware of a future comparison in rates of fusion after microdiscectomy between open and MIS approaches. Nonetheless, the possibility of selection bias cannot be ignored. Additionally, we did not have long-term follow-up.
Last, patient-reported outcome measures were not recorded. Despite finding no statistically significant difference in need for fusion following discectomy via the minimally invasive versus open approach, it is possible that patient-recorded outcomes could be different between the 2 approaches.
Conclusions
The results presented in our study represent the first report on the intermediate rate of patients whose disease progresses to ultimately require fusion following an index lumbar microdiscectomy. Our results indicate that there is a low likelihood of needing an index level fusion following microdiscectomy. Additionally, of those that went on to necessitate eventual fusion, most underwent fusion within the first 24 months after the index microdiscectomy. Predictors of those patients with recurrent symptoms leading to eventual fusion were found to be active smoking status and history of revision microdiscectomy. These results provide a substantial foundation with which we can counsel patients considering undergoing a lumbar microdiscectomy regarding their risk for needing an eventual fusion. Additionally, the results reinforce the efficacy of microdiscectomy whether employed via an open or tubular approach with low rates of reherniation and ultimate need for fusion, and no difference among type of approach utilized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.