
Abstract
Study Design:
Retrospective cohort study.
Objective:
Overcorrection in adult spinal deformity (ASD) surgery may lead to proximal junctional kyphosis (PJK) because of posterior spinal displacement. The aim of this paper is to determine if the L1 position relative to the gravity line (GL) is associated with PJK.
Methods:
ASD patients fused from the lower thoracic spine to sacrum by 4 spine surgeons at our hospital were retrospectively studied. Lumbar-only and upper thoracic spine fusions were excluded. Spinopelvic parameters, the L1 plumb line (L1PL), L1 distance to the GL (L1-GL), and Roussouly type were measured.
Results:
One hundred fourteen patients met inclusion criteria (63 patients with PJK, 51 without). Mean age and follow up was 65.51 and 3.39 years, respectively. There was no difference between the PJK and the non-PJK groups in baseline demographics, pre-operative and immediate post-operative pelvic incidence-lumbar lordosis mismatch, sagittal vertical axis, or coronal Cobb. The immediate postoperative L1-GL was -7.24 cm in PJK and -3.45 cm in non-PJK (P < 0.001), L1PL was 1.71 cm in PJK and 3.07 cm in non-PJK (P = 0.004), and PT (23.76° vs 18.90°, P = 0.026) and TK (40.56° vs 31.39°, P < 0.001) were larger in PJK than in non-PJK. After univariate and multivariate analyses, immediate postoperative TK and immediate postoperative L1-GL were independent risk factors for PJK without collinearity.
Conclusions:
A dorsally displaced L1 relative to the GL was associated with an increased risk of PJK after ASD surgery. The postoperative L1-GL distance may be a factor to consider during ASD surgery.
Introduction
Adult spinal deformity (ASD) correction surgery has been shown to improve both radiographic and clinical outcomes, but proximal junctional kyphosis (PJK) can significantly detract from both the surgeon’s and patient’s opinion of an otherwise successful surgery.1,2 The incidence of PJK ranges widely from 5% to 46%, with most studies reporting rates between 20% and 40%.3-5 Multiple factors such as postoperative spinopelvic parameters, magnitude of sagittal correction, and bone density have been reported as risk factors for PJK following ASD surgery.1,6-8 Powerful instrumentation and techniques using osteotomies have allowed surgeons to induce tremendous amounts of lordosis and to change position of the spine, but overcorrection is a phenomenon that is observed clinically. However, quantification of the effects of overcorrection is rare. We sought to evaluate if the position of L1—representing the extent of overcorrection of the lumbar spine—is associated with PJK.
It has been shown that the sagittal vertical axis (SVA) of less than 5 cm is protective against the development of PJK.9,10 However, the C7 vertebral body can be obscured by the shoulders and in patients with an L5-S1 fusion, the posterior superior endplate of S1 is can be unclear, leading to measurement error. Moreover, although the SVA is commonly used, 11 Yagi et al found a discordance beteween the SVA and ground reaction forces (GRF); instead, they found a concordance of the GRF and the gravity line (GL), which may better define the virtual center of gravity (COG). 12
Overcorrection and extreme lordosis of the lumbar spine may result in PJK, as patients will instinctively re-balance themselves to keep their head over their feet, resulting in a kyphotic angulation above the upper instrumented vertebrae (UIV). We sought to evaluate if the position of L1 relative to the GL is associated with PJK, with the hypothesis that overcorrection of the lumbar spine with resultant dorsal displacement of the L1 plumb line may result in PJK.
Materials and Methods
Patient Cohort
A retrospective study of patients who undergoing ASD correction from the lower thoracic (LT) spine (T9 to T12) to S1 at the University of California San Francisco from 2008 to 2018 by 4 spine surgeons was performed. The study was approved by Institutional Review Board of University of California San Francisco (IRB:13-12 087) and patient consent was not necessary for this retrospective research. Inclusion criteria were age ≥ 18 years, radiographic diagnosis of ASD (defined as at least one of the following: coronal Cobb angle ≥ 20°, SVA ≥ 5 cm, pelvic tilt (PT) ≥ 25°), UIV at T9 to T12, lower instrumented vertebra (LIV) to the sacrum, and at least 1-year post-operative follow up with radiographs and records. Diagnoses included adult idiopathic scoliosis, adult degenerative scoliosis, and flat back deformity. Patients were excluded if they had tumor, trauma, or infection. Data collected were demographics such as age, gender BMI, PJK, and radiographic parameters. Spinopelvic parameters were compared pre- and post-operatively, and the magnitude of change was analyzed. Data was collected and analyzed by 2 neurosurgeons, 3 orthopedic surgeons, and 2 researchers.
Radiographic Measurements
All patients had standing 36-inch standing anteroposterior and lateral spinal radiographs preoperatively, postoperatively within 3 months, and at last follow-up. Standard measurements included sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), lumbar lordosis (LL), PI-LL, thoracic kyphosis (TK) (T5 to T12), SVA, central sacral vertical line (CSVL), coronal scoliosis Cobb angle, and T1 pelvic angle (TPA). Also measured were: the L1 pelvic angle (L1PA), defined as the angle subtended by a line from the L1 centroid to the femoral heads and a line from the femoral heads to the center of S1; the L1 plumb line (L1PL), defined as the distance from a plumb line drawn from the L1 centroid to the posterior superior corner of the S1 endplate, with positive numbers anterior and negative numbers posterior; the L1 to gravity line distance (L1-GL), defined as the distance from the L1 centroid to the gravity line (GL), which is measured as a plumb line from the ear canal on long cassette radiographs (Figure 1), 12 and the Roussouly type. 13 The proximal junctional angle (PJA) was defined as the sagittal Cobb angle between the inferior endplate of the UIV to the superior endplate of 2 vertebrae above (UIV+2) (Figure 1). Radiographic PJK was defined as PJA ≥ 10° and a PJA ≥ 10° compared to the preoperative measurement.8,14
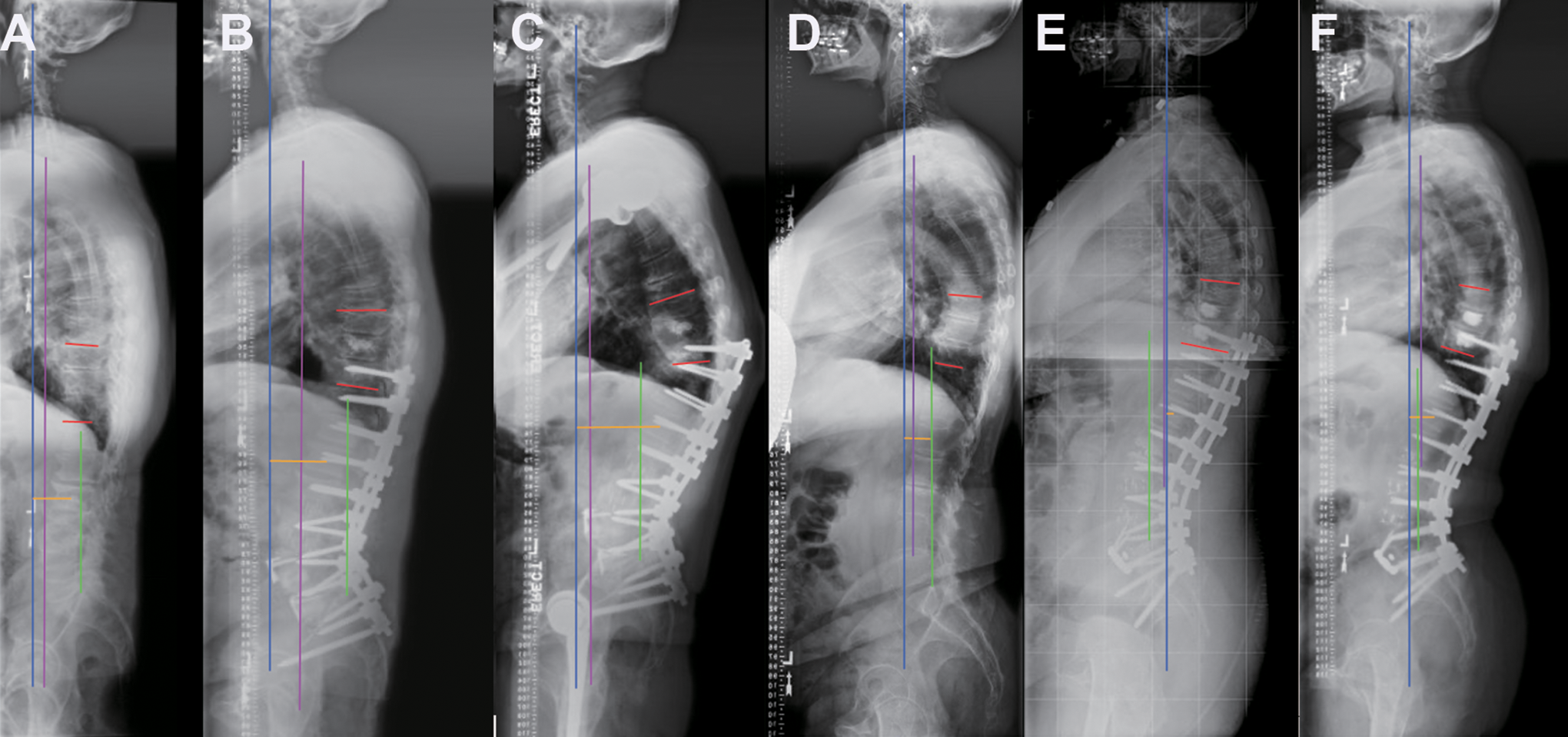
The measurement of the L1-GL distance (yellow line), the gravity line (a vertical blue line from the ear canal) and the angle of proximal junction (PJA, red lines) in PJK patient (A: preoperative, B: immediate postoperative, C: at last follow-up) and in a non-PJK patient (D: preoperative, E: immediate postoperative, F: at last follow-up). Green line: a vertical line from posterior superior corner of the S1 endplate; Purple line: the C7 plumb line.
Statistical Analysis
Inter-observer and intra-observer reliability were assessed with an absolute agreement intraclass correlation coefficient (ICC) analysis using a 2-way random effects model. Agreement was classified as excellent with an ICC of >0.75. Categorical variables were presented as numbers, and continuous variables were presented as means with standard deviations. Normality of distribution was tested using Kolmogorov–Smirnov test. One-way ANOVA, independent samples t-tests, and chi-squared tests were used to evaluate differences. The receiver operating characteristic (ROC) curves established separation criteria between PJK and non-PJK groups. The most appropriate thresholds (cut-off value) of continuous variables with high sensitivity and specificity were also established using the ROC curve. In addition, univariate analyses of possible risk factors were performed by way of a Cox proportional hazards regression model. The variables that achieved a significance level of P < 0.05 were entered into multivariate analyses for screening as independent risk factors via the Cox model. Values of P < 0.05 were considered statistically significant, and statistical analyses were performed using SPSS version 23.0 software (IBM, Illinois, USA).
Results
A total of 114 patients met inclusion criteria, with a mean age of 65.51 ± 8.05 years (41 to 80 and 82 females). The mean follow-up was 3.00 ± 2.11 years (range 1 to 11 years). There were 63 out of 114 patients with PJK (55.3%). There was no significant difference in age (P = 0.208), gender (P = 0.332), body mass index (BMI, P = 0.929), and follow-up times between the 2 groups (P = 0.194) (Table 1).
Demographics of Patients With and Without Proximal Junctional Kyphosis.
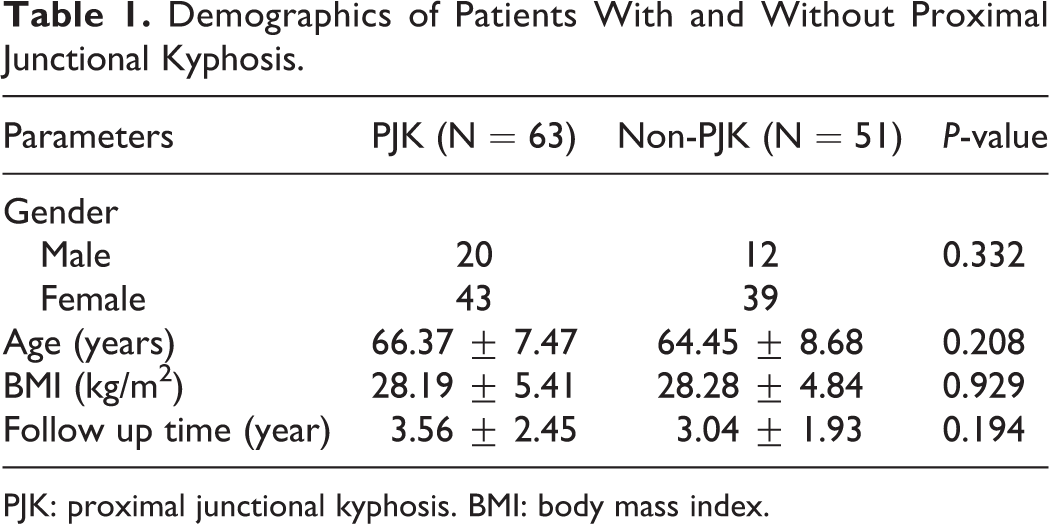
PJK: proximal junctional kyphosis. BMI: body mass index.
Radiographic Analysis
As shown in Table 2, there were no significant differences between the PJK and non-PJK groups in SS (P = 0.201), PT (P = 0.061), PI (P = 0.566), LL (P = 0.458), PI-LL (P = 0.990), SVA (P = 0.151), CSVL (P = 0.094), L1PA (P = 0.640), and coronal Cobb angle (P = 0.189) preoperatively. The preoperative TK was 28.18 ± 15.39° in PJK group and 18.29 ± 13.79° in non-PJK group (P = 0.001), and the preoperative TPA was 28.52 ± 9.71° in PJK group and 24.52 ± 9.75° in non-PJK group (P = 0.034). The preoperative L1PL was 1.41 ± 2.96 cm in PJK and 2.60 ± 2.86 cm in non-PJK (P = 0.033). The preoperative L1-GL was -10.39 ± 5.43 cm in PJK and -5.54 ± 3.16 cm in non-PJK (P < 0.001). There was no collinearity between preoperative TK and preoperative L1-GL (P = 0.197).
Comparison of Radiographic Parameters in the Patients With and Without Proximal Junctional Kyphosis.
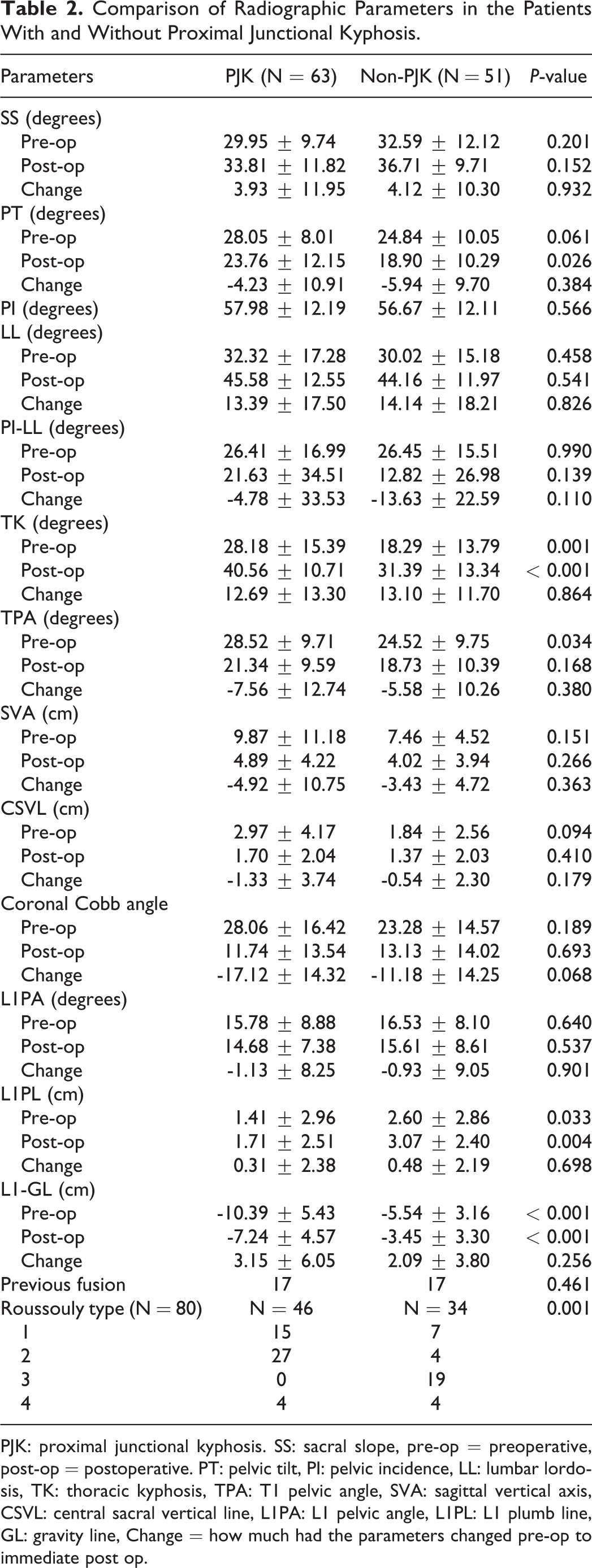
PJK: proximal junctional kyphosis. SS: sacral slope, pre-op = preoperative, post-op = postoperative. PT: pelvic tilt, PI: pelvic incidence, LL: lumbar lordosis, TK: thoracic kyphosis, TPA: T1 pelvic angle, SVA: sagittal vertical axis, CSVL: central sacral vertical line, L1PA: L1 pelvic angle, L1PL: L1 plumb line, GL: gravity line, Change = how much had the parameters changed pre-op to immediate post op.
Postoperatively, there were no significant differences in SS (P = 0.152), LL (P = 0.541), PI-LL (P = 0.139), TPA (P = 0.168), SVA (P = 0.266), CSVL (P = 0.410), L1PA (P = 0.537), and coronal Cobb angle (P = 0.693). The immediate postoperative PT (23.76 ± 12.15°) and TK (40.56 ± 10.71°) were larger in the PJK group than in the non-PJK group (PT: 18.90 ± 10.29°, P = 0.026, TK: 31.39 ± 13.34°, P < 0.001). The immediate postoperative L1PL was 1.71 ± 2.51 cm in the PJK group and 3.07 ± 2.40 cm in the non-PJK group (P = 0.004). The immediate postoperative L1-GL was -7.24 ± 4.57 cm in the PJK group and -3.45 ± 3.30 cm in the non-PJK group (P < 0.001) (Table 2). There was no collinearity between immediate postoperative TK and L1-GL (P = 0.254).
With regard to change of pre-operative to post-operative spinopelvic parameters (Table 2), there were no significant differences between the PJK group and the non-PJK group in SS (P = 0.932), PT (P = 0.384), LL (P = 0.826), PI-LL (P = 0.110), TK (P = 0.864), TPA (P = 0.380), SVA (P = 0.363), CSVL (P = 0.179), L1PA (P = 0.901), coronal Cobb angle (P = 0.068), L1PL (P = 0.698), and L1-GL (P = 0.256). After excluding previous fusion cases in order to accurately assess Roussouly type (comparable numbers, P = 0.461), there were 46 patients in the PJK group and 34 patients in the non-PJK group. The PJK group had more Roussouly Type 1 and Type 2 patients, but the non-PJK group had more Type 3 and Type 4 patients (P = 0.001) (Table 2).
Univariate Analysis
In the univariate analysis, risk factors for PJK were analyzed including preoperative and immediate postoperative parameters. The variables that achieved a significance level of P < 0.05 were identified. They were preoperative SVA (P = 0.030), PT (Pre-op, P = 0.011, immediate post-op, P = 0.016), preoperative LL (P = 0.042), TK (Pre-op, P = 0.008, immediate post-op, P < 0.001), TPA (Pre-op, P = 0.022, immediate post-op, P = 0.002), L1PL (Pre-op, P = 0.009, immediate post-op, P = 0.001), and L1-GL (Pre-op, P = 0.008, immediate post-op, P < 0.001), (Table 3). The above parameters are all risk factors for PJK, and those parameters with P < 0.05 went into the multivariate analysis. Immediate postoperative SVA (P = 0.058) and immediate postoperative PI-LL mismatch (P = 0.209), did not reach significance as factors for PJK.
Univariate and Multivariate Analysis of Risk Factors for Proximal Junctional Kyphosis.
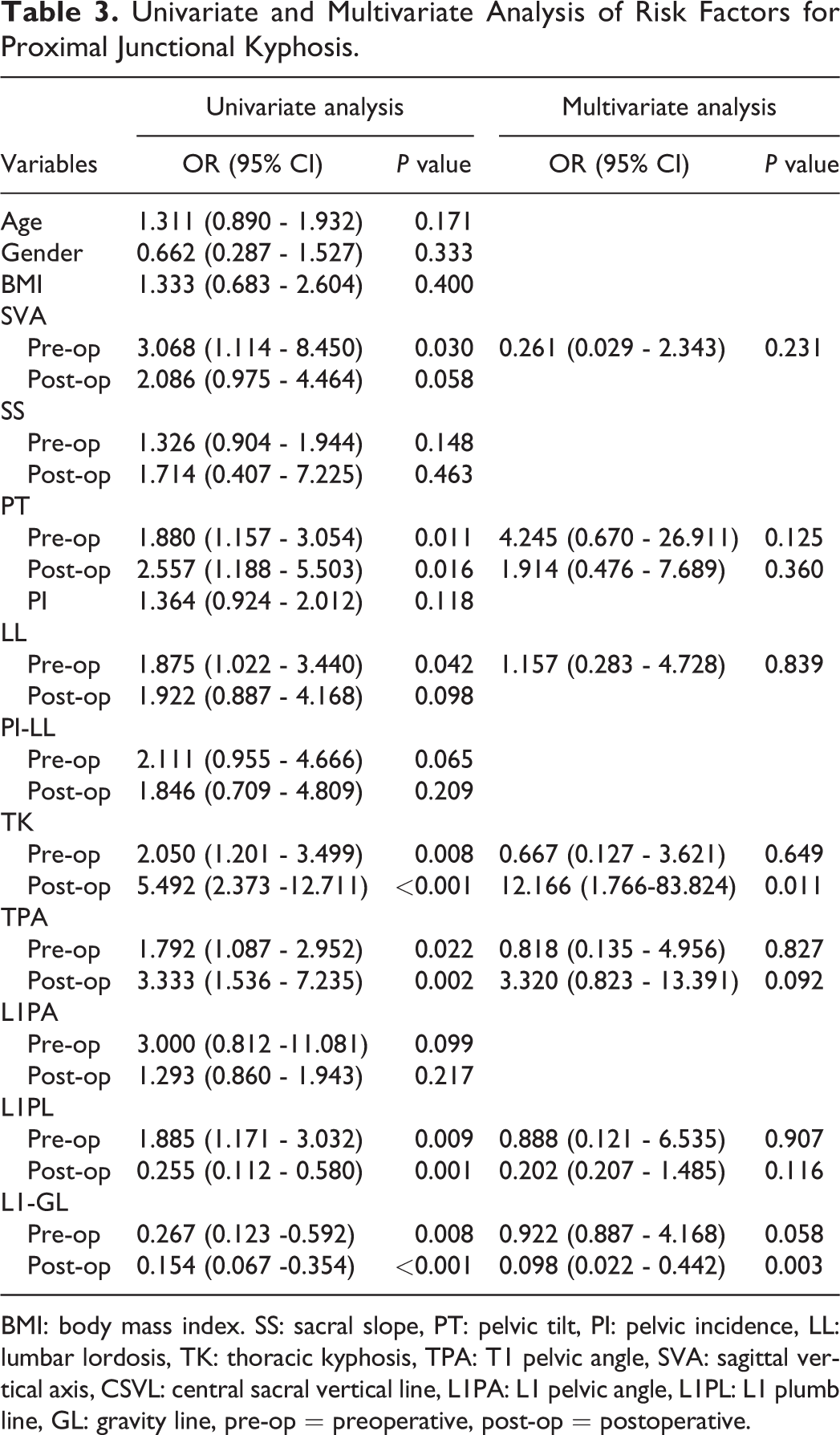
BMI: body mass index. SS: sacral slope, PT: pelvic tilt, PI: pelvic incidence, LL: lumbar lordosis, TK: thoracic kyphosis, TPA: T1 pelvic angle, SVA: sagittal vertical axis, CSVL: central sacral vertical line, L1PA: L1 pelvic angle, L1PL: L1 plumb line, GL: gravity line, pre-op = preoperative, post-op = postoperative.
Multivariate Analysis
After multivariate analysis, the immediate postoperative L1-GL (P = 0.003, OR = 0.098, 95%CI: 0.022-0.442) and immediate postoperative TK (P = 0.011, OR = 12.166, 95%CI: 1.766 - 83.824) were significant as independent risk factors for PJK (Table 3). The other variables were not independent risk factors for PJK (preoperative SVA, P = 0.231, preoperative PT, P = 0.125, immediate post-operative PT, P = 0.360, preoperative LL P = 0.839, preoperative TK, P = 0.649, preoperative TPA, P = 0.827, immediate post-operative TPA, P = 0.092, preoperative L1PL, P = 0.907, immediate post-operative L1PL, P = 0.116, and preoperative L1-GL, P = 0.058). After using a ROC curve to establish separation criteria of immediate postoperative L1-GL between PJK and non-PJK, the AUC was 0.877 (95% CI: 0.811-0.943), and the most appropriate threshold was -5.47 cm (sensitivity: 84.1%; specificity: 80.4%, Figure 2). A ROC curve for immediate postoperative TK was also established, with an AUC of 0.712 (95% CI: 0.614 - 0.810). The optimal immediate postoperative TK cut-off value determined by the Youden index is 32.5° (sensitivity, 80.6%; specificity, 56.9%).
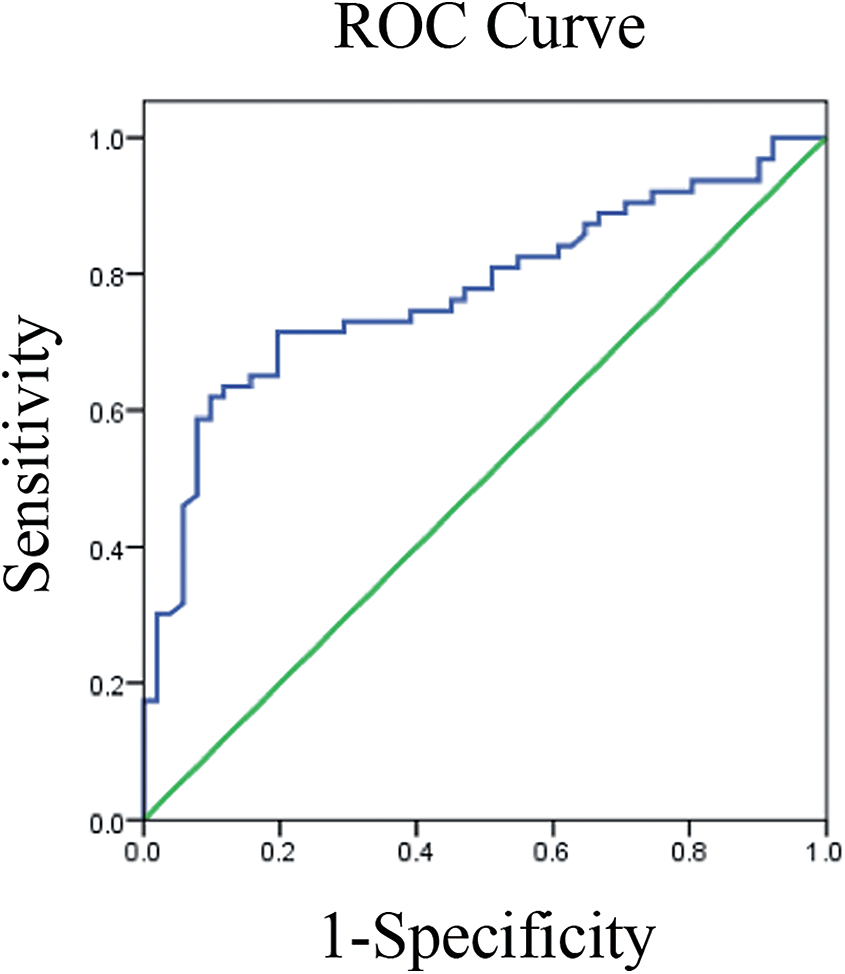
A receiver operator characteristic (ROC) curve for immediate postoperative L1-GL as a predictor for PJK was established, with an AUC of 0.877 (95% CI: 0.811-0.943). The optimal cut-off value of L1-GL determined by the Youden index is -5.47 cm (sensitivity, 84.1%; specificity, 80.4%).
Discusssion
Proximal junctional kyphosis (PJK) is a vexing problem after posterior fusion surgery in adult spinal deformity (ASD). One reason that PJK is difficult to eliminate is that its etiology is multi-factorial. Bone mineral density (BMD), high body mass index (BMI), fusion to the sacrum, circumferential spinal fusion, selection of the UIV, and use of pedicle screws have all been reported to be potential risk factors for PJK.1,8,15,16 Other papers have reported that SVA, TK >40°, postoperative LL, and PI-LL mismatch >30° were associated PJK.7,15,17,18 However, other studies have shown opposite evidence of these findings.6,19,20 When surgeons use spinopelvic parameters as goals of correction for ASD, lordosis is often induced either through facet releases, posterior column osteotmies, or 3-column osteotomies. However, even with powerful correction maneuevers and with knowledge of the ideal spiniopelvic alignment, PJK can still occur. One possible etiology of PJK in fusions to the lower thoracic spine is overcorrection or inducing too much lordosis. This can be manifested by a dorsally displaced L1 vertebral body relative to center of gravity of the body. With such a dorsally displaced L1, the remainder of the trunk and head may shift anteriorly to restore balance, leading to PJK. One method of measuring the center of gravity is by the use of the gravity line. Our research question was to assess if overcorrection of lumbar lordosis relative to the center of gravity—as manifested by the dorsal position of L1 relative to the gravity line—was associated with PJK. In our study, the rate of PJK was 55%, which is higher than most previously published papers, and there are probably some reasons for this observation. First is that because many patients were included in this study from over a decade ago, our awareness of bone density was probably not as prominent as it is currently. Many patients with either borderline bone density or even frank osteoporosis probably had surgery without bone health treatment. Such patients would probably undergo a bone density test before surgery and probably endocrinologist consultation with teriparatide treatment in the modern era. Also, another important reason is that all our patients had fusion to the sacrum, and it has been shown that long-segment fusions to the sacrum are associated with increased risk of PJK. 8 Finally, the UIV in our cases were instrumented with pedicle screws instead of hooks, and this method of UIV instrumentation may have contributed to the higher observed PJK rate.
Although spinopelvic parameters are traditionally used to measure sagittal and coronal alignment, the GL is an imaginary vertical line that passes through the whole-body center of mass. Le Huec et.al reported that the GL is located along a vertical line passing through the middle of the sacrum in the coronal plane and perpendicular to the ground, and it passes in the sagittal plane through a vertical line situated slightly to the rear of the femoral heads. 21 Hasegawa et.al reported that during standing, the GL coincides with the vertical plumb line from the ear canal on the lateral long cassette spinal radiograph. 22 In young healthy people, the C7 plumb line (C7PL) is generally dorsal to the GL, but in ASD patients, the GL and C7PL are discordant (GL to C7PL > 3 cm), even though there remains concordance between ground reaction forces (GRF) and GL. This means that in ASD patients, the GL should reflect the center of mass despite an abnormal SVA. 12 Thus, the GL may be a more accurate reflection of the patient’s overall body mass than the SVA, especially in ASD patients. In our study, we found that the distance from L1 to the GL (L1-GL) was longer in the PJK group than in the non-PJK group, potentially reflecting the effects excessive induction of lordosis and subsequent dorsal translation of L1 relative to the sacrum. This may also simply reflect the body’s adjustment to continually lean forward despite lordosis induction as is stated with the expression, “life is a kyphosing event.” After univariate and multivariate analyses, the immediate postoperative L1-GL distance was identified to be an independent risk factor for PJK. Combined with the ROC curve, we found that patients with an immediate postoperative L1-GL distance of more than 5.47 cm were 10.20 times more likely to develop PJK than patients with an immediate postoperative L1-GL of less than 5.47 cm (sensitivity, 84.1%; specificity, 80.4%). Thus, we found that the more dorsal L1 was relative to the gravity line, the more likely PJK would occur.
In our study, the distance from L1 to the posterior superior endplate of S1 (L1PL) was also a risk factor of PJK. One advantage of measuring the L1 position is its ease of visualization on plain radiographs; it is not obscured by the shoulders and is generally clear on routine lumbar spine views. Although there is very little literature on the position of L1 and fusion outcomes, Liang et al reported that the preoperative distance from L1 to S1 sagittal plumb line was found to be a potential risk factor for predicting symptomatic adjacent segment degeneration in the patients after lumbar spine fusion 18 . In our study, there were no statistical differences in age, gender, and BMI between the PJK and the non-PJK groups. Moreover, we tried to keep the groups as homogeneous as possible by only including patients with long-segment fusion to the lower thoracic spine (T9 to T12) to the sacrum; we did not include patients fused to the upper thoracic spine or patients with lumbar-only fusions. If upper thoracic spine patients or lumbar-only patients were also included, the compensatory abilities of the spine would not have been consistent; thus, only lower thoracic spine UIV patients were included. Consistent with the findings of the increased L1-GL distance in PJK patients, we found that TPA and TK were larger in the PJK group than in the non-PJK group. These findings are consistent with previous reports stating that a large TK and TPA was associated with increased PJK risk.8,23 Moreover, this makes sense in that an increased GL generally will be reflected in increase TK and TPA measurements. Consistent with known variables affecting PJK, we found that the preoperative SVA, pre- and immediate postoperative PT, preoperative LL, pre- and immediate postoperative TPA, and pre- and immediate postoperative L1PL were risk factors for PJK (P < 0.05); but they were not independent risk factors. A high immediate postoperative TK was an independent risk factor for PJK, and patients with postoperative TK > 32.5° was more likely to have PJK. This is consistent with previous reports reflecting that patients with increased TK were more at risk of PJK.24,25
Another interesting finding in our study is that more Roussouly types 1 and 2 patients had PJK compared to types 3 and 4 with the sub-analysis performed after exclusion of prior fusion patients. This may reflect overcorrection in types 1 and 2 lumbar spines that naturally need very little lordosis (sacral slope < 35°). Thus, these patients may be physiologically be adjusted to have very little lordosis at baseline, and induction of signficant lordosis in such patients can result in non-physiologic dorsal displacement of the L1 vertebral body, increasing the L1-GL distance.13,26 This increased posterior displacement of L1 results in further distance of the GL, potentially leading to PJK. Hey et al reported normal distances of L1 to the GL, and the average offsets of L1 to the GL in normal healthy adults were –4.6 cm and –4.3 cm in Roussouly types 1 and 2, respectively. 27 This is consistent with our finding that patients with more than -5.47 cm displacement had over 10 times the odds of developing PJK, reflecting our findings that the increased L1 to GL distances are not normal.
There are limitations to this study. First, this is a retrospective, single center study. A multi-center study with a larger sample size would have been more representative. The results of this study may not necessarily be generalizable to different regions and practices. Second, bone density is a factor associated with PJK, and this was not specifically measured. Unfortunately, pre-operative computed tomography to measure Hounsfield units and bone density test were not uniformly available in all patients, and thus, we could not accurately report on bone density. Third is that we did not correct for the different types of corrective tools used such as 3-column osteotomies, posterior column osteotomies, and interbody types. However, we tried to make the groups as homogeneous as possible by limiting the UIV to the thoracic spine and the LIV to the sacrum in all patients.
Conclusions
The position of the L1 vertebra relative to the gravity line appears to correlate with PJK after lower thoracic to sacrum fusions for ASD. Patients with an immediate postoperative L1-GL more than 5.47 cm behind the GL were 10.20 times more likely to develop PJK, also correlating with a supra-physiologic position of L1 relative to the GL by Roussouly type.
Footnotes
Disclosures
Zhuo Xi, MD; Minghao Wang, MD, Ping-Guo Duan, MD, Bo Li, MD, Hao-Hua Wu, MD, Jinping Liu, MD, Jeremy M.V. Guinn, BS and Joshua Rivera, BA: None. Praveen V. Mummaneni, MD: consultant: Depuy Synthes, Stryker, Globus. Royalties: Thieme Publishing, Springer Publishing, and DePuy Synthes. Research Support: NREF, ISSG and AO spine. Has purchased stock from Spinicity/ ISD. Shane Burch, MD: Consultant for Medtronic. Sigurd H. Berven, MD: Consulting: Medtronic, Stryker, Globus, Medicrea, Integrity Spine. Royalties: Medtronic. Research Support: NIH, AO spine. Dean Chou, MD: consultant: Globus, royalty: Globus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient consent was not necessary for this retrospective research. The study was approved by Institutional Review Board of University of California San Francisco (IRB:13-12 087).