
Abstract
Study Design:
Retrospective cohort study.
Objective:
Elucidate negative sagittal balance following adult spinal deformity surgery.
Methods:
We conducted a retrospective review of adult spinal deformity patients who underwent long fusion (>5 levels) to the sacrum by a single surgeon at a single institution between 2011 and 2015. Patients were divided into cohorts of postoperative sagittal vertical axis (SVA) <−10 mm, between −10 and +10 mm, or >+10 mm, denoted as groups 1, 2, and 3, respectively. Univariate analysis compared preoperative factors between the groups, and a multivariable logistic regression model was used to determine independent risk factors for developing a negative sagittal balance (SVA<−10 mm) following adult spinal deformity correction.
Results:
We reviewed 8 patients in group 1, 9 patients in group 2, and 25 patients in group 3. The average postoperative SVA for group 1, group 2, and group 3 were −30.99, +3.67, and +55.56 mm, respectively. There was a trend toward higher upper-instrumented vertebra (UIV) in group 1 (T2) compared with group 2 (T10) and group 3 (T9) (P = .05). A trend toward lower preoperative SVA in groups 1 and 2 compared with group 3 was also seen (+53.36 vs +71.73 vs +122.80 mm) (P = .06). Finally, we found a trend toward lower body mass index in group 1 compared with groups 2 and 3 (24.71 vs 25.92 vs 29.33 kg/m2) (P = .07). Based on multivariable regression, higher UIV was found to be a statistically significant independent predictor for developing a postoperative negative sagittal balance of <−10 mm (P = .02, odds ratio = 0.67).
Conclusions:
Our results demonstrate that a higher UIV may predispose patients undergoing adult spinal deformity correction to have a postoperative negative sagittal balance.
Keywords
Introduction
Adult spinal deformity comprises a number of disorders affecting alignment of the spine in the axial, coronal, and sagittal planes. 1,2 Sagittal deformity of the spine has gained increasing attention for its correlation to negative health-related quality of life and disability. 3 -5 A commonly utilized metric to define global sagittal alignment is the sagittal vertical axis (SVA). In general, if the SVA is greater than +5 cm, a patient is considered to have a global sagittal imbalance. 3 The negative impact of an elevated SVA on clinical symptoms and outcomes has been well studied. 3,5 -7
Contrarily, the effect of a negative SVA, and therefore, a negative global sagittal balance, has not been well characterized. Similarly, factors that influence the development of a postoperative negative sagittal balance following adult deformity correction have not been previously explored. Given the strong relationship a positive sagittal balance has with poor patient symptoms and disability, it may be that negative sagittal balance affects such outcomes as well.
Our objective with this retrospective cohort study was to elucidate the concept of postoperative negative sagittal balance and to determine what, if any, demographic, radiographic, and operative characteristics served as risk factors for developing a postoperative negative sagittal balance after adult spinal deformity correction.
Methods
Patient Cohorts
The institutional review board approved this retrospective radiographic review of patients who underwent long spinal fusion (>5 levels) to the sacrum for adult spinal deformity correction by a single surgeon at a single academic institution (2011-2015). Patients undergoing primary or revision surgeries were included. Pediatric patients (<18 years) were excluded. Patients with a primary sagittal deformity as well as primary coronal/axial deformity were included in the study. Sagittal deformities included diagnoses of thoracolumbar kyphoscoliosis, positive sagittal imbalance syndrome, and flat back deformity, and coronal deformities included only degenerative scoliosis. All patients had at least 1 year of follow-up and those who did not were excluded. All demographic, radiographic, and operative information was obtained through the electronic medical record.
Coronal and sagittal measurements were performed with a dedicated spine measurement tool (Surgimap, Nemaris Inc, New York, NY, USA), a validated software, on the most recent preoperative and two week postoperative standing radiographs. 8 Patients were divided into 3 cohorts: group 1 (negative) had a postoperative SVA <−10 mm, group 2 (neutral) had a postoperative SVA between −10 and +10 mm, and group 3 (positive) had a postoperative SVA >+10 mm (Figure 1).
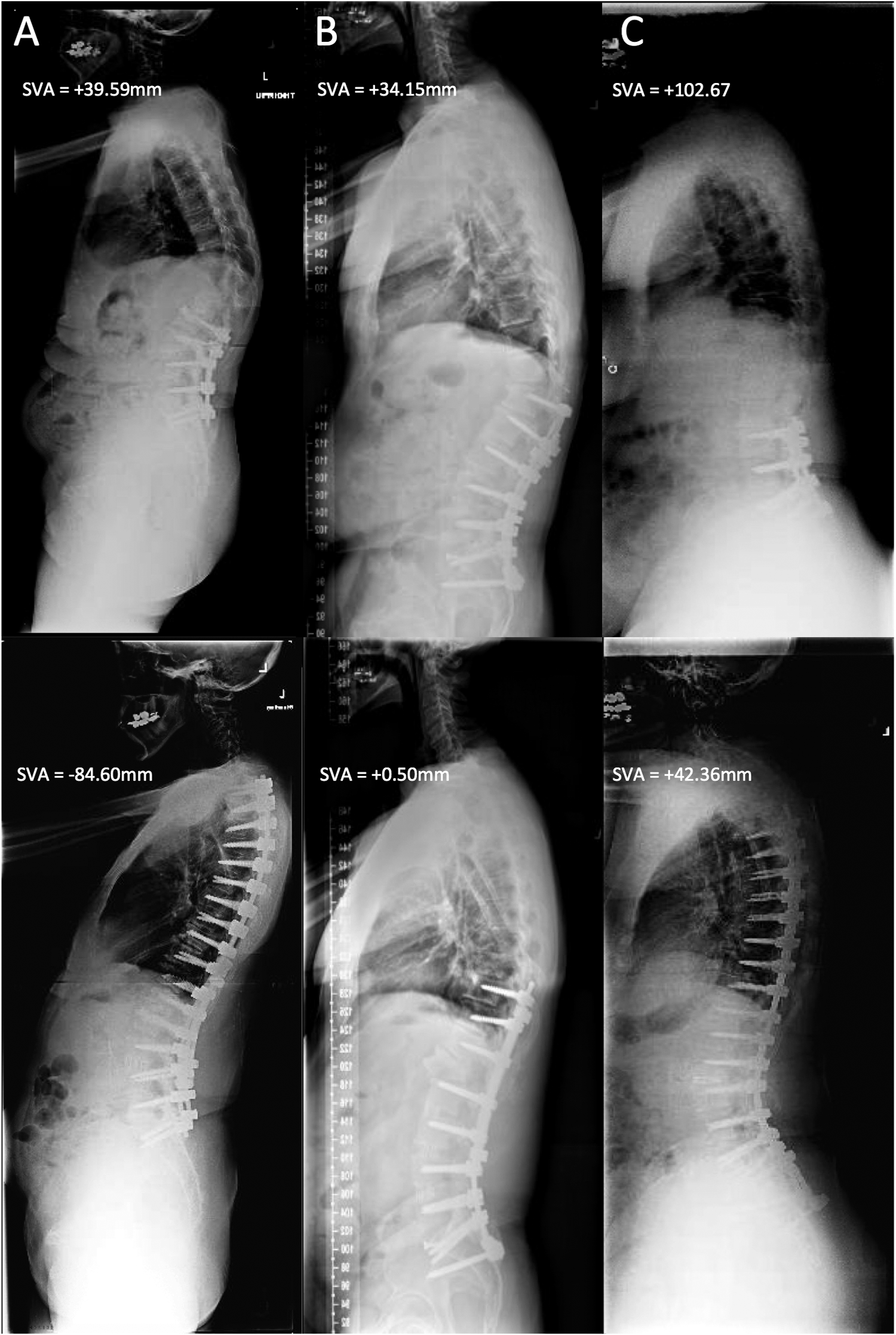
Representative standing, lateral radiographs taken preoperatively (top row) and postoperatively (bottom row). (A) Patient in group 1 (negative), with a postoperative sagittal vertical axis (SVA) <−10 mm. (B) Patient in group 2 (neutral), with a postoperative SVA >−10 mm and <+10 mm. (C) Patient in group 3 (positive), with a postoperative SVA >+10 mm.
All cases were performed by a single senior surgeon and assisted by a spine fellow or orthopedic surgery resident. The posterior approach was used for every case, and ponte or pedicle subtraction osteotomies were performed where appropriate as indicated in Table 1. Morcellized local autograft and recombinant human bone morphogenetic protein–2 (rhBMP-2) was used in all cases with the average quantity of rhBMP-2 reported in Table 1. All cases were instrumented with 5.5 mm radius titanium or cobalt chromium rods.
Demographic and Operative Features of Patients in Group 1 (Postoperative SVA <−10 mm), Group 2 (Postoperative SVA Between −10 mm and +10 mm), and Group 3 (Postoperative SVA >+10 mm).
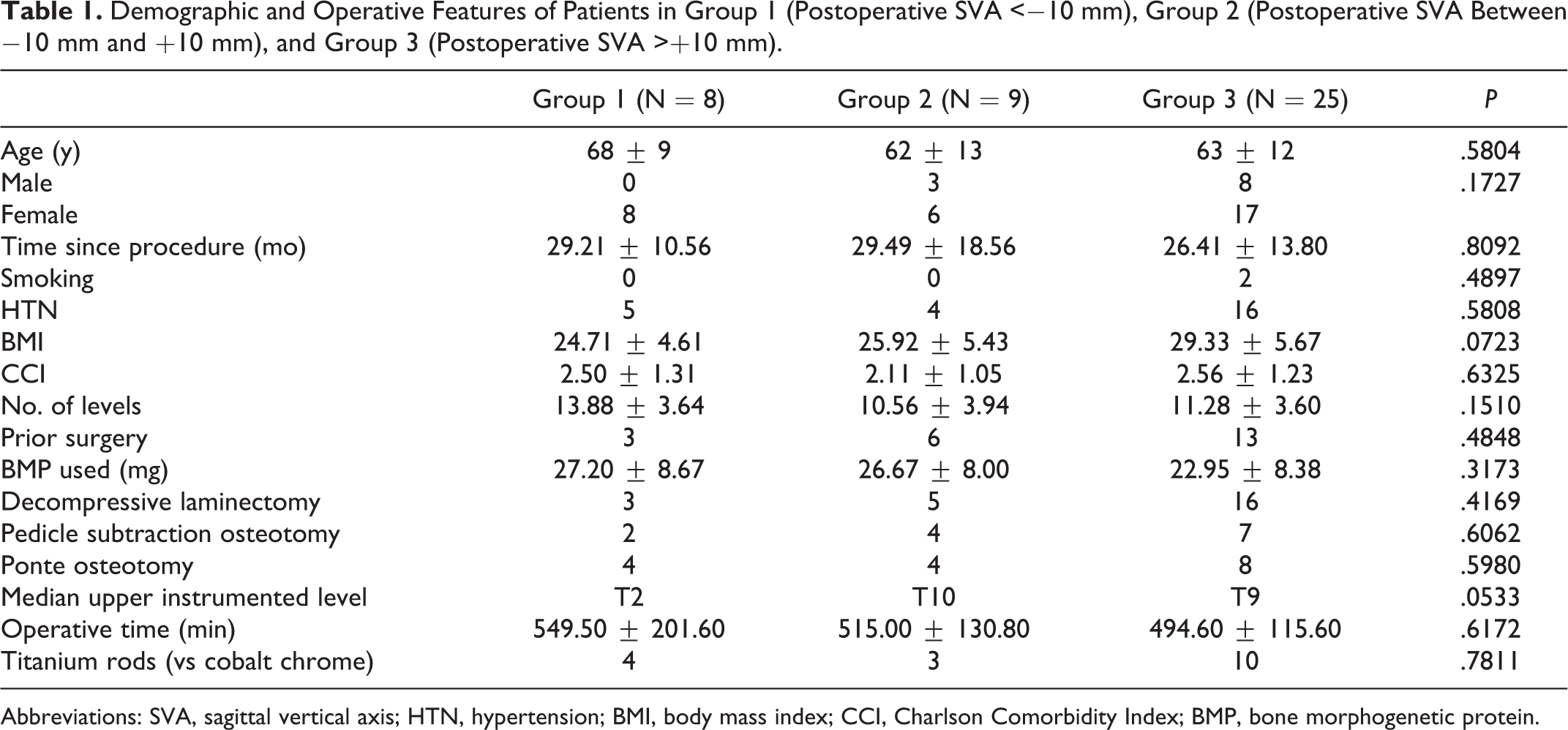
Abbreviations: SVA, sagittal vertical axis; HTN, hypertension; BMI, body mass index; CCI, Charlson Comorbidity Index; BMP, bone morphogenetic protein.
Statistical Analysis
Statistical analysis was performed with SPSS (IBM, Armonk, NY, USA). Univariate analysis was carried out among the 3 cohorts with a 1-way analysis of variance with post hoc Tukey test for multiple comparisons. Unpaired t tests were performed on any groups that were different in order to obtain P values. Contingent variables were compared with a chi-square test. Any variables with a trend toward a difference (P < .1) or that were statistically different between the groups were chosen for analysis using a multivariable logistic regression model. The regression model treated negative sagittal balance (SVA<−10 mm) as a binary outcome. Upper instrumented vertebra (UIV) was defined as an ordinal variable, with the highest vertebral level being T1. This was given a value of 1, and each vertebral level below was numbered as T2 = 2, T3 = 3 and so on. Therefore, a higher UIV on the spine was coded with a lower numerical value. Statistical significance was taken at P < .05.
Results
Patient Characteristics
We reviewed a total of 42 patients with 8 in group 1 (SVA <−10 mm), 9 in group 2 (SVA −10 mm and <+10 mm), and 25 in group 3 (SVA > +10 mm). Table 1 summarizes the demographic and operative characteristics among the groups. There were 4 patients with a sagittal deformity and 4 patients with a coronal deformity in group 1. There were 5 patients with a sagittal deformity and 4 patients with a coronal deformity in group 2. There were 14 patients with a sagittal deformity and 11 patients with a coronal deformity in group 3. The proportion of sagittal versus coronal deformities among the 3 groups was not statistically different (P = .95). The 2 pedicle subtraction osteotomies (PSOs) in group 1 were performed at L3. Of the 4 PSOs in group 2, 2 were performed at L3, 1 at L1, and 1 at L4. Of the 7 PSOs done in group 3, 1 was done at T11, 3 at L2, and 3 at L3. There was a trend toward a lower body mass index (BMI) (P = .07) and higher median UIV (P = .05) in group 1.
Preoperative and Postoperative Coronal and Sagittal Measurements
Table 2 summarizes the preoperative coronal and sagittal measurements among the 3 groups. There was a trend toward difference in preoperative SVAs of group 1 (+53.36 mm), group 2 (+71.73 mm), and group 3 (+122.80 mm) (P = .06).
Preoperative Coronal and Sagittal Measurements Between Patients in Group 1 (Postoperative SVA <−10 mm), Group 2 (Postoperative SVA Between −10 mm and +10 mm), and Group 3 (Postoperative SVA >+10 mm).
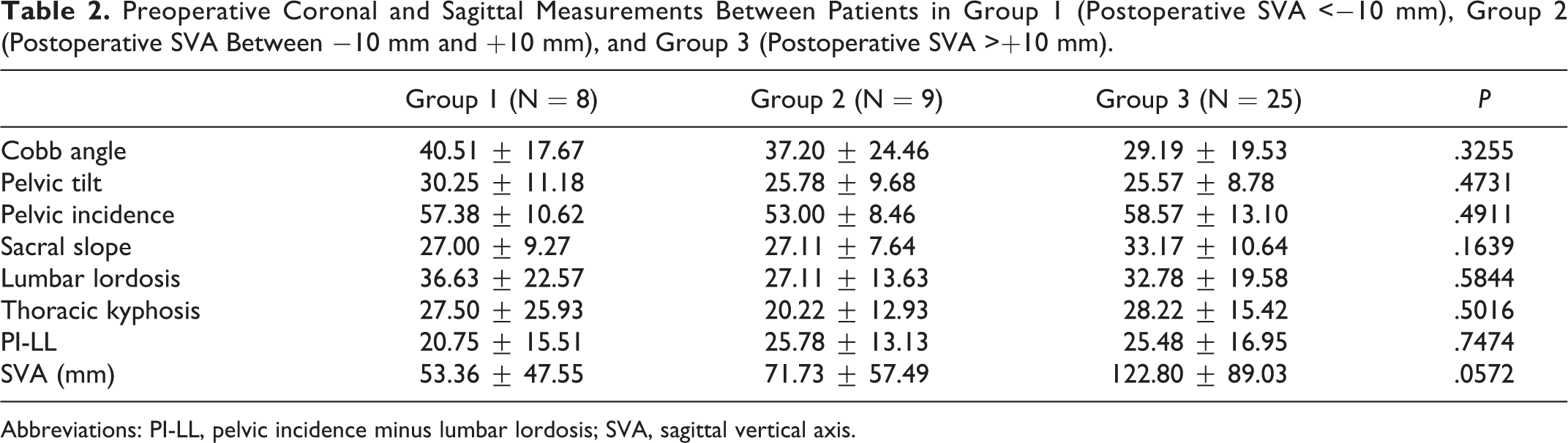
Abbreviations: PI-LL, pelvic incidence minus lumbar lordosis; SVA, sagittal vertical axis.
Postoperative measurements among the 3 groups are summarized in Table 3. The only statistically significant difference in postoperative alignment among the groups was for SVA, which was −30.99 mm for group 1, +3.67 mm for group 2, and +55.56 mm for group 3. Multiple comparisons revealed that groups 1 and 2 had a statistically smaller postoperative SVA than group 3 (P < .0001, P = .0008, respectively). The postoperative SVA for the negative balance group ranged from −84.60 to −11.40 mm. The range for the neutral and positive balance groups was −3.42 to +8.80 mm and +10.56 to +166.00 mm, respectively. There was a trend toward significant difference in postoperative thoracic kyphosis (TK) measurements among the groups, with the negative balance group having the lowest TK (P = .09).
Postoperative Coronal and Sagittal Measurements Between Patients in Group 1 (Postoperative SVA <−10 mm), Group 2 (Postoperative SVA Between −10 mm and +10 mm), and Group 3 (Postoperative SVA >+10 mm).a
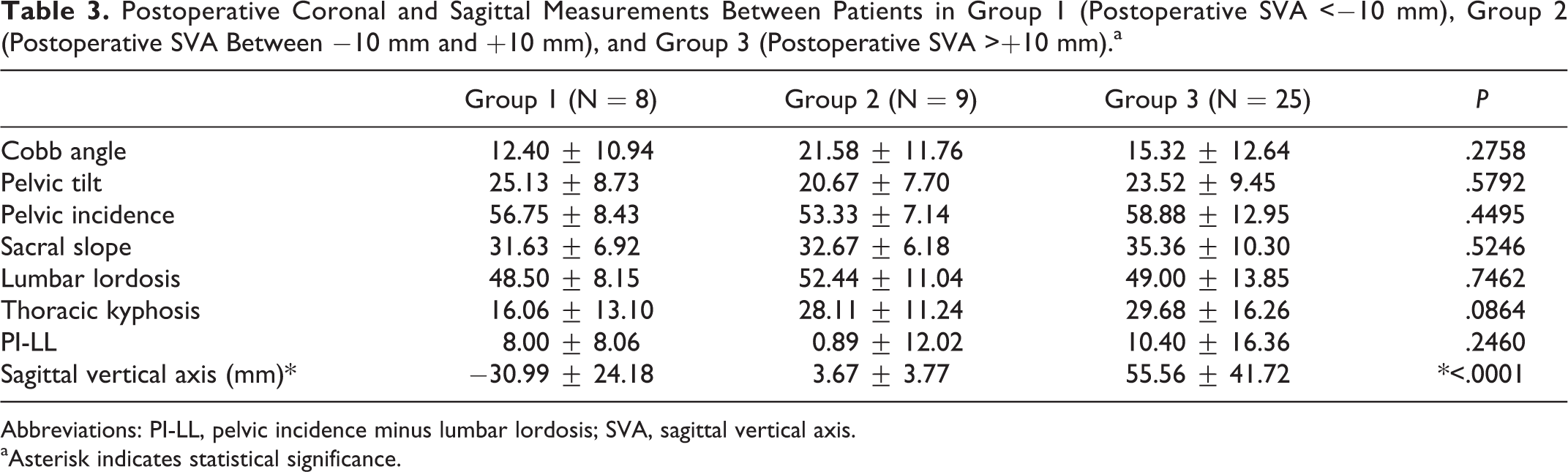
Abbreviations: PI-LL, pelvic incidence minus lumbar lordosis; SVA, sagittal vertical axis.
aAsterisk indicates statistical significance.
When examining the magnitude of change in regional alignment from preoperative to postoperative, the only measurements that were statistically different among the groups were Cobb angle and TK. The negative balance group had a statistically greater magnitude of change in Cobb angle pre- to postoperatively than the positive balance group (P = .008). The negative balance group also had a statistically greater change in thoracic kyphosis pre- to postoperatively compared with the neutral balance group (P = .01). There was no difference between the groups with respect to magnitude of change in pelvic tilt.
Risk Factors for Negative Sagittal Balance
Given that UIV, BMI, and preoperative SVA were the only preoperative characteristics with a trend toward statistical difference among the groups, we chose to analyze these factors as independent predictors of postoperative negative sagittal balance (SVA <−10 mm) by using a multivariable logistic regression. UIV was the only significant independent risk factor with an odds ratio of 0.67 (P = .02) (Table 4). Preoperative SVA had an odds ratio of 0.98, though this was not statistically significant (P = .07). Only 1 patient in group 1 currently has clinical symptoms of pain in the upper thoracic area, and none has required a revision surgery.
Multivariable Logistic Regression Analysis to Identify Risk Factors for Developing Postoperative Negative Sagittal Balance (SVA <−10 mm).a

Abbreviations: SVA, sagittal vertical axis; BMI, body mass index.
aAsterisk indicates statistical significance.
Revision and Complication Rates Among Groups
All patients had at least 1 year of follow-up. The mean follow-up time for the negative, neutral, and positive balance groups was 154.10 ± 46.78, 155.30 ± 82.21, and 141.60 ± 61.12 weeks, respectively. There was no statistically significant difference in the mean follow up time among the groups (P = .81).
The negative balance group experienced no intraoperative complications, the neutral balance group experienced 2 incidental durotomies requiring intraoperative repair, and the positive balance group experienced 2 incidental durotomies requiring intraoperative repair. The incidence of intraoperative complications was not statistically significant between the groups (P = .27).
The negative balance group experienced 3 complications that necessitated a return to the operating room, 2 symptomatic pseudarthroses and 1 deep vein thrombosis that required surgical intervention. The neutral balance group also had 3 adverse events that required a return to the operating room, 2 cases of pseudarthrosis and 1 infection that required a removal of hardware with irrigation and debridement. The positive balance group experienced 8 complications, 4 proximal junctional failures that required revision, 1 case of hardware loosening, 2 pseudarthroses, and 1 case of neurogenic bladder that required an emergent decompression. The overall incidence of complications that required a revision operation was not statistically different between the 3 groups (P = .96).
The deep vein thrombosis that occurred in the negative balance group, the infection that occurred in the neutral balance group, 2 of the proximal junctional kyphosis, 1 pseudarthrosis, and the neurogenic bladder that occurred in the positive balance group all occurred within 90 days of discharge. Apart from these complications, no patients were readmitted within 90 days of discharge for any other reasons in any of the groups.
Discussion
The importance of proper sagittal alignment has been well described, and positive sagittal imbalance has been correlated with pain and negative health-related quality of life outcome scores. 3 -5 We hereby introduced the concept of negative sagittal balance following long fusion to the sacrum for adult spinal deformity and identified risk factors that contributed to its development. Both careful preoperative planning and intraoperative execution are important to achieve ideal alignment postoperatively. As pedicle screw-based instrumentation provides the surgeon with powerful means to control the spine in all 3 planes, this study highlights the potential for overcorrection during surgery.
Of the demographic factors that we examined, only BMI trended toward significance, with lower BMI patients tending to have a postoperative SVA <−10 mm. Araujo et al 9 found that increasing BMI and central obesity were associated with an increased SVA. The group studied randomly sampled healthy adults and investigated spinopelvic alignment on standing radiographs. They further discovered that obesity and central adiposity were associated with nonneutral spinal position based on the Roussouly classification. 6 The authors suggested the biomechanical constraints obesity imposes on the spine produce a hypolordotic posture that leads to an anteriorly displaced SVA. We found increased BMI to trend toward positive postoperative sagittal alignment, and although our regression model did not determine increased BMI as having a significantly lower association with negative sagittal balance postoperatively, it did trend toward significance. These findings corroborate the results and postulates put forth by Araujo and colleagues. 9
The only operative characteristic that trended toward a significant difference among the 3 groups was UIV, and this was the only characteristic found to be independently associated with negative sagittal alignment based on multivariable logistic regression. The neutral and positive balance groups had median UIVs of T10 and T9, respectively, while the negative balance group had a median UIV of T2. The relationship between UIV and development of proximal junctional kyphosis has been well described, but it has not been reported on with regard to global sagittal alignment. 10,11 Our regression model coded T1 as “1,” T2 as “2,” and so on down the spine. The odds ratio was 0.668, indicating that with each increasing thoracic level relative to T1, and therefore, a lower UIV on the spine, patients were less likely to develop postoperative negative sagittal balance. This is important when taken in conjunction with postoperative radiographic findings. We found that group 1, the negative balance group, had not only a more posteriorly displaced SVA than the other 2 groups but also a smaller TK that trended toward significance. Similar to our observations, Blondel et al 12 demonstrated that lack of restoration of TK contributed to postoperative posterior sagittal alignment of <0 mm following lumbar osteotomy. This is a clinically important observation as TK can be significantly decreased surgically with modern instrumentation, and when the sagittal alignment is not positive preoperatively, TK ought to be maintained intraoperatively to maintain proper global alignment.
Regarding radiographic measurements, the only preoperative sagittal parameter investigated that trended toward a difference among the 3 groups was the SVA. This was expected given that an initial SVA that is low can lead to overcorrection and resultant negative sagittal balance. Our regression model confirmed this trend, though it failed to reach statistical significance. Based on our data, we recommend that either lower UIV (eg, T10) be chosen unless there are clinical and radiographic reasons to fuse to the proximal thoracic spine (eg, thoracic hyperkyphosis) or dial in proper TK to the rod to prevent overcorrection when preoperatively global balance (SVA) is not significantly positive. Fusing to a lower level in the thoracic spine may also have beneficial perioperative outcomes such as smaller incision, reduced blood loss, shorter hospital stay, and reduced implant cost. The surgeon should weigh the pros and cons of a shorter fusion construct, given that a UIV in the thoracolumbar region has been shown to correlate with an increased risk of proximal junctional kyphosis and increased incidence of compression fracture. 11,13 -16 We found no statistically significant difference in the incidence of complications among the 3 groups, suggesting that negative sagittal balance may not portend poor outcomes. Despite this, future studies must seek to further elucidate the clinical impact negative sagittal balance has on patient symptomatology and outcomes, which will help clarify the advantages and disadvantages of instrumenting to a lower thoracic vertebra.
Though we did not find statistical differences among the groups with regard to preoperative, postoperative, or magnitude of change in pelvic tilt, the negative balance group had the largest preoperative and postoperative pelvic tilt. This may suggest that the hip capsule or psoas musculature has been stretched from such an elevated preoperative pelvic tilt, limiting the patients’ ability to antevert the pelvis to compensate for a dorsally inclined spine even following proper restoration of lumbar lordosis-pelvic incidence match.
In summary, a higher UIV, lower BMI, and smaller preoperative SVA predisposed patients to a postoperative negative sagittal balance <−10 mm, though only UIV was statistically significant.
Limitations
A major limitation of our study was lack of outcome measures for the patients allocated to each group due to inconsistent collection of data. Though we only had anecdotal evidence that 1 of 8 patients in the negative balance group complained of persistent neck/upper back pain at the latest follow-up (2 years) and that there were no statistically significant differences in revision rates among the 3 groups, we could not accurately determine the clinical impact of negative sagittal alignment. Future studies should seek to clarify this relationship. Another major limitation of the study was the small sample size of heterogenous spinal deformities. We had only 8 patients with a negative postoperative negative sagittal balance. Because of our small sample size, we chose to include in our multivariable regression model only the variables that were statistically different, or very close to being statistically different, among our groups. A larger sample size would allow inclusion of more variables of interest in the multivariable regression without overfitting the model. Future studies should seek to expand on our concept with a larger sample size. We also did not take intraoperative X-rays, which would have helped to mitigate the difference in spinal alignment between patients. Finally, pedicle subtraction osteotomies were not performed at the same level, which may have had an effect on postoperative pelvic tilt. 17
Conclusion
UIV was the most significant risk factor for developing a postoperative negative sagittal alignment of less than −10 mm following adult spinal deformity surgery. BMI and preoperative SVA may be additional risk factors, but future studies are necessary to clarify this. These findings should be taken into account when assessing patients and planning surgical deformity correction to minimize overcorrection. The clinical impact of negative sagittal balance remains unclear and requires future exploration.
Footnotes
Authors’ Note
This research was approved by the institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.