
Abstract
Study Design:
Meta-analysis.
Objective:
Proximal junctional kyphosis (PJK) is a complication of surgical management for adult spinal deformity with a multifactorial etiology. Many risk factors are controversial and their relative importance are not fully understood. We aimed to identify the surgical, radiographic, and patient-related risk factors associated with PJK and proximal junctional failure (PJF).
Methods:
A systematic literature search was performed using PubMed, Cochrane Database of Systematic Reviews, and EMBASE. The inclusion criteria included prospective randomized control trials and prospective/retrospective cohort studies of adult patients with radiographic evidence of PJK, which was defined as a proximal junctional sagittal Cobb angle ≥10° and at least 10° greater than the preoperative measurement. Studies required a minimum of 10 patients and 12 months of follow-up.
Results:
A total of 14 unique studies, including 1908 patients were included. The pooled analysis showed significant differences between the PJK and non-PJK groups in age (weighted mean difference [WMD] −3.80; P = .03), prevalence of osteopenia/osteoporosis (odds ratio [OR] 1.99; P = .0004), preoperative sagittal vertical axis (SVA) (WMD −17.52; P = .02), preoperative lumbar lordosis (LL) (WMD −1.22; P = .002), pedicle screw instrumentation at the upper instrumented vertebra (UIV) (OR 1.67; P = .02), change in SVA (WMD −11.87; P = .01), fusion to sacrum/pelvis/ilium (OR 2.14; P < .00 001), change in LL (WMD −5.61; P = .01), and postoperative SVA (WMD −7.79; P = .008).
Conclusions:
Our meta-analysis suggests that age, osteopenia/osteoporosis, high preoperative SVA, high postoperative SVA, low preoperative LL, use of pedicle screws at the UIV, SVA change/correction, LL change/correction, and fusion to sacrum/pelvis/iliac region are risk factors for PJK.
Keywords
Introduction
Adult spinal deformity (ASD) comprises a wide scope of disorders. Surgical management for ASD frequently involves long fusion constructs with osteotomies to mobilize spinal segments and achieve appropriate sagittal and coronal balance. Complications after ASD surgery can be separated into immediate or delayed onset. One of the more common delayed onset complications is proximal junctional kyphosis (PJK). Glattes et al 1 defined the proximal junction as being between the caudal endplate of the upper instrumented vertebra (UIV) and the cephalad endplate of the vertebra that is 2 levels above the UIV (ie, UIV+2). 1 PJK is defined as a proximal junctional sagittal Cobb angle ≥10° and at least 10° greater than the preoperative measurement. The reported incidence of proximal junctional kyphosis ranges from 20% to 40%. 1 PJK can lead to a progression of worsening sagittal alignment, vertebral collapse, and neurologic injury. Inferior clinical outcomes from PJK have spurred surgeon efforts to develop techniques and strategies to prevent PJK.
There has also been increasing interest in proximal junctional failure (PJF), which is becoming recognized as one of the most common reasons for reoperation following ASD surgery. 2 PJF is defined as a proximal junctional sagittal Cobb angle ≥15° with the presence of structural failure and mechanical instability, which distinguishes it from PJK. Structural failure in PJF can present as vertebral body fracture at the UIV or UIV+1, implant pullout or breakage, or disruption of the posterior ligamentous complex. 2,3 Compared with PJK, PJF has been associated with increased morbidity, spinal instability, and neurologic deficits. 2
PJK has a multifactorial etiology, with proposed mechanisms, including extensive paraspinal muscle dissection, disruption of the posterior ligamentous tension band, UIV selection, choice of surgical approach, proximal disc degeneration, degree of correction, compression fracture at or around the UIV, facet violation, and patient factors such as age, body mass index (BMI), and the presence of osteoporosis. 1,4,6 -14 To our knowledge, only one prior study has performed a systematic review or meta-analysis on the risk factors for PJK. 15 The purpose of this article was to perform a meta-analysis to analyze the surgical, radiographic, and patient-related risk factors associated with PJK and PJF.
Methods
Inclusion/Exclusion Criteria and Review Procedure
A systematic Medline literature search was performed using PubMed, Cochrane Database of Systematic Reviews, and EMBASE. The databases were searched for publication dates from January 2006 to September 2016. The searches were performed from Medical Subject Headings (MeSH) used by the National Library of Medicine, MeSH terms “proximal,” “junctional,” “kyphosis,” and “PJK” were used. The inclusion criteria included prospective randomized control trials or prospective/retrospective cohort studies, adult patients who had ASD with radiographic evidence of PJK, which was defined as a proximal junctional sagittal Cobb angle ≥10° and at least 10° greater than the preoperative measurement. Studies required a minimum of 12 months of follow-up, reported clinical outcomes and/or risk factors for PJK, and a minimum of 10 patients for a given study. Exclusion criteria included review papers, abstracts, case studies, and repeat data.
Two independent authors reviewed abstracts of each article to determine which articles to include in the study. The review of articles was performed as suggested by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and a flowchart of the review process is outlined in Figure 1. The authors jointly reviewed the full text of the articles meeting the inclusion criteria based on the abstract to determine agreement on the inclusion of the studies. In case of a discrepancy, a third author participated until a consensus was reached.
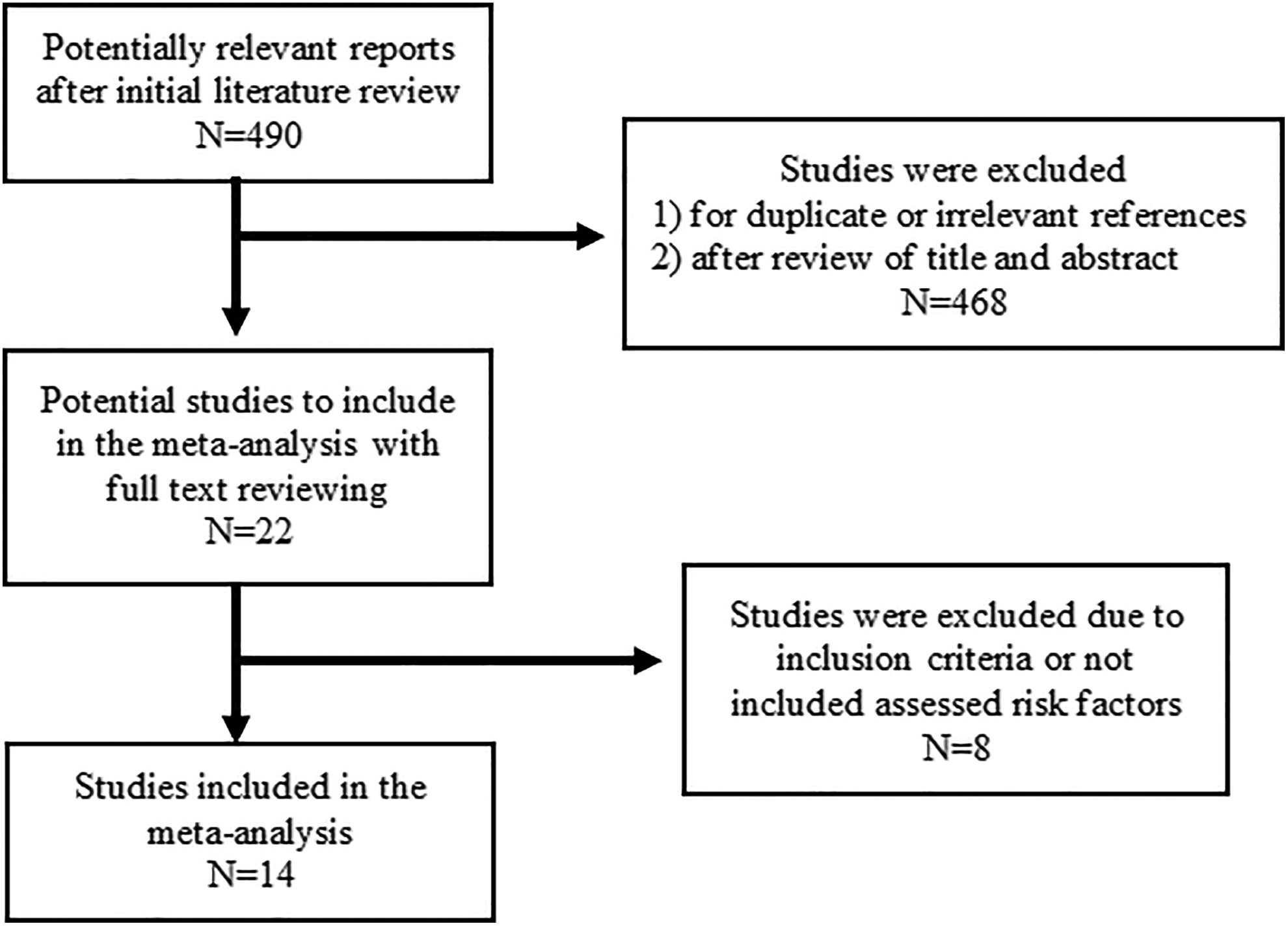
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study selection.
Data Extraction
A meta-analysis database was created from the included studies with the following categories: (1) study ID to include author, journal, and year of publication; (2) reference; (3) study type and level of evidence; (4) study inclusion/exclusion criteria; (5) number of patients; (6) male-to-female ratio; (7) patient age; (8) length of follow-up; (9) patient-related risk factors (smoking, BMI, osteoporosis); (10) preoperative spinopelvic measurements; (11) postoperative spinopelvic measurements; (12) approach; (13) type of instrumentation (hook, pedicle, hybrid constructs); (14) level of correction; (15) patient outcome scores (Scoliosis Research Society instrument [SRS-24], Oswestry Disability Index [ODI]).
Methodological Quality Assessment
Methodological quality assessment was accomplished using the Downs and Black checklist. The total cumulative score is composed of a profile that measures quality of reporting, internal validity, and external validity. According to Downs and Black, the performance results of the checklist showed a high internal consistency (Kuder-Richardson formula 20 = 0.89) and test-retest (r = 0.88) and interrater (r = 0.75) reliability. 16 The checklist consists of 27 items for which a “yes” answer is scored 1 and “no” or “unable to determine” answer is scored 0.
Meta-Analysis
The odds ratio (OR) and weighted mean difference (WMD) were used as the summary statistics. Both fixed- and random-effect models were tested. In the fixed-effects model, it was assumed that treatment effect in each study was the same, whereas in a random-effects model, it was assumed that there were variations between studies. Chi-square tests were used to study heterogeneity between trials. I2 values were used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values greater than 50% considered as substantial heterogeneity. I2 can be calculated as I2 = 100% × (Q – df)/Q, with Q defined as Cochrane’s heterogeneity statistics and df defined as degrees of freedom. If there was substantial heterogeneity, the possible clinical and methodological reasons were explored qualitatively. The results using the random-effects model were presented to take into account the possible clinical diversity and methodological variation between studies. Specific analyses considering confounding factors were not possible because raw data was not available. All P values were 2-sided. All statistical analysis was conducted with Review Manager Version 5.3.2 (Cochrane Collaboration, Software Update, Oxford, UK). Sensitivity analysis was performed by varying the assumptions used in the meta-analysis and by single elimination of the studies. Funnel plots of effect size versus standard error were assessed by visual inspection to determine publication bias.
Results
Search Strategy
A total of 490 references were identified through electronic database searches (Figure 1). After exclusion of duplicate or irrelevant references and detailed evaluation of references, 22 potential studies remained. After applying the selection criteria, 14 studies were finally selected for analysis.
Baseline Characteristics and Quality Assessment
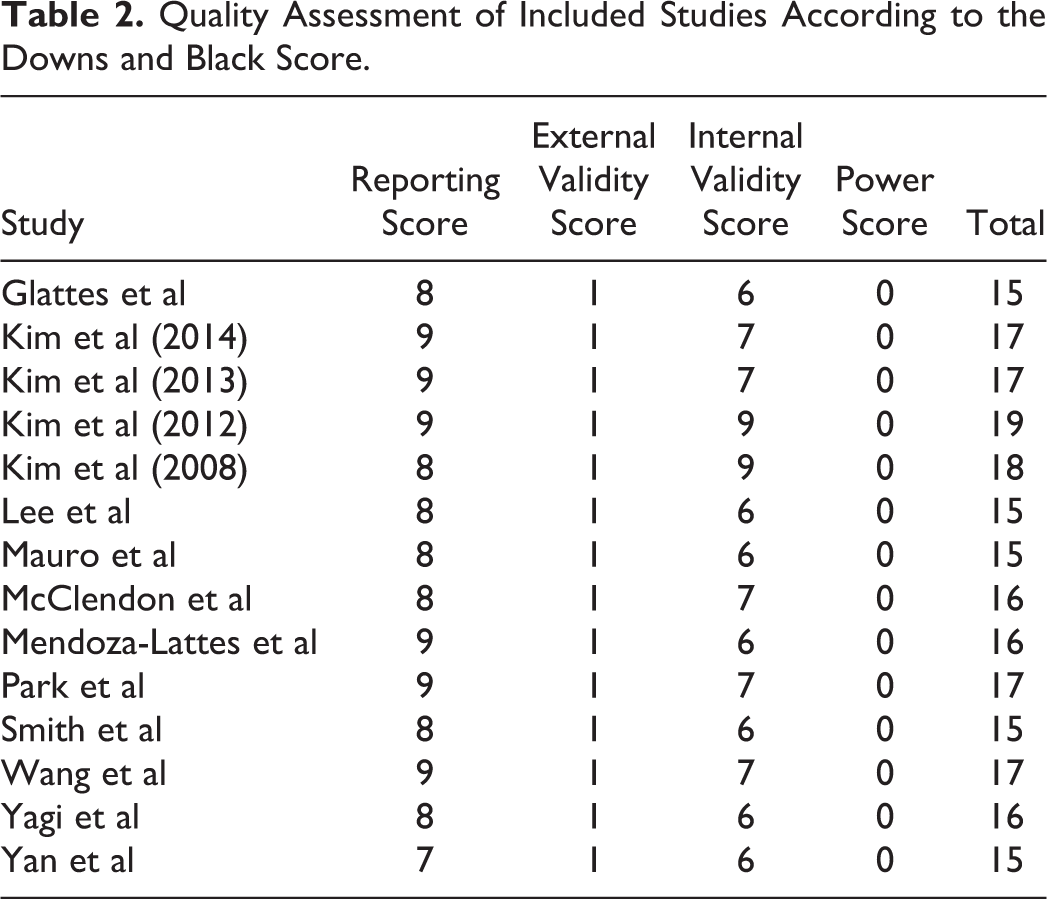
The main characteristics of the included studies are summarized in Table 1. The sizes of the studies ranged from 27 to 364 patients. A total of 530 patients had PJK and 111 patients had PJF after ASD surgery. As most studies included were retrospective, we used the Downs and Black scale to assess the quality of each study (Table 2). We found that the majority of included studies were of moderate quality.
Characteristics of the Included Studies.
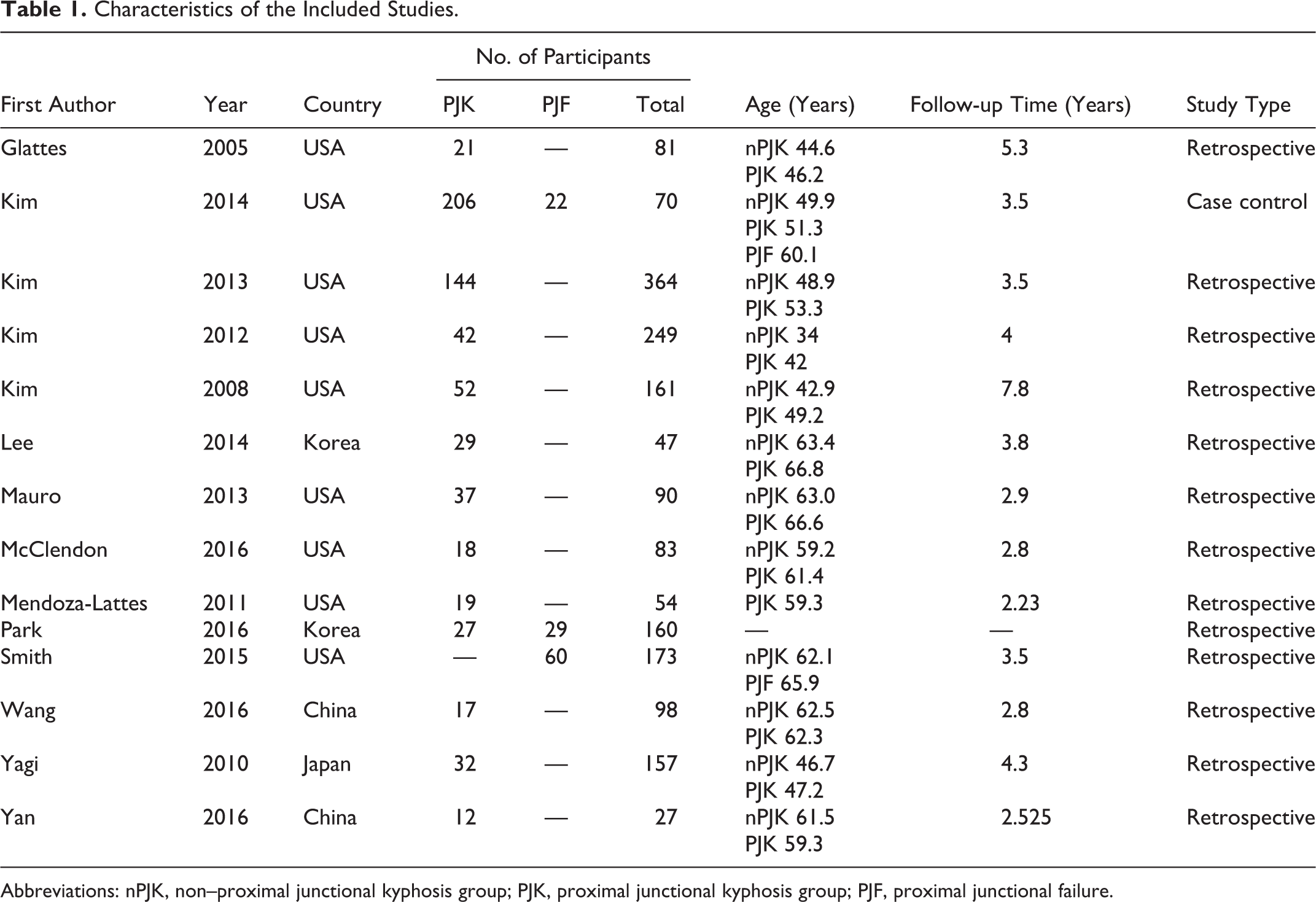
Abbreviations: nPJK, non–proximal junctional kyphosis group; PJK, proximal junctional kyphosis group; PJF, proximal junctional failure.
Quality Assessment of Included Studies According to the Downs and Black Score.
Assessment of Risk Factors for PJK and PJF
The PJK group (n = 333) was significantly older than the non-PJK group (n = 640) (WMD non-PJK vs PJK −3.74 years; 95% CI −5.09 to −2.40; I2 = 0%; P < .001) (Figure 2). The PJF group was also significantly older than the non-PJK group (WMD non-PJK vs PJF −3.80 years; 95% CI −7.33 to −0.27; P = .03).
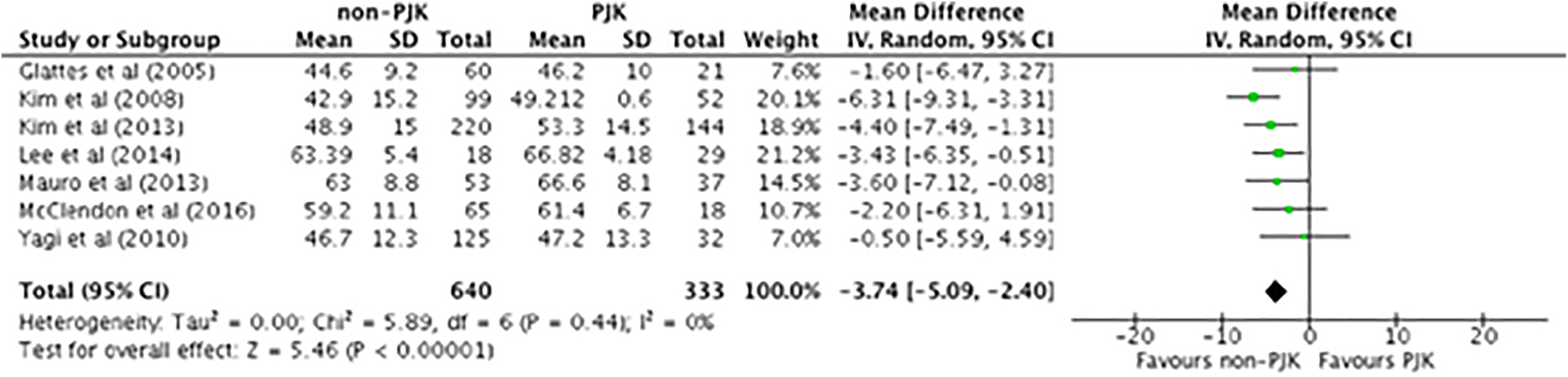
Weighted mean difference for age.
There was no significant difference in BMI between the non-PJK (n = 627) and PJK (n = 259) groups (WMD −0.15; 95% CI −1.44 to 1.14; I2 = 73%; P = .82). There was also no significant difference in BMI between the non-PJK (n = 136) and PJF (n = 22) groups (WMD −0.63; 95% CI −3.28 to 2.02; P = .64).
There was no significant difference in the proportion of smokers between the non-PJK (n = 469) and PJK (n = 250) groups (10.2% vs 11.2%; OR 1.02; 95% CI 0.58 to 1.80; I2 = 0%; P = .94). Similarly, in a pooled comparison of non-PJK patients (n = 249) versus PJF patients (n = 82), there was also no significant difference in the proportion of smokers (6.0% vs 8.5%; OR 1.28; 95% CI 0.50 to 3.26; I2 = 0%; P = .61).
The PJK group (n = 255) had a significantly higher prevalence of osteopenia/osteoporosis than the non-PJK group (n = 605) (31.0% vs 29.6%; OR 1.99; 95% CI 1.36 to 2.92; I2 = 0%, P < .001) (Figure 3).
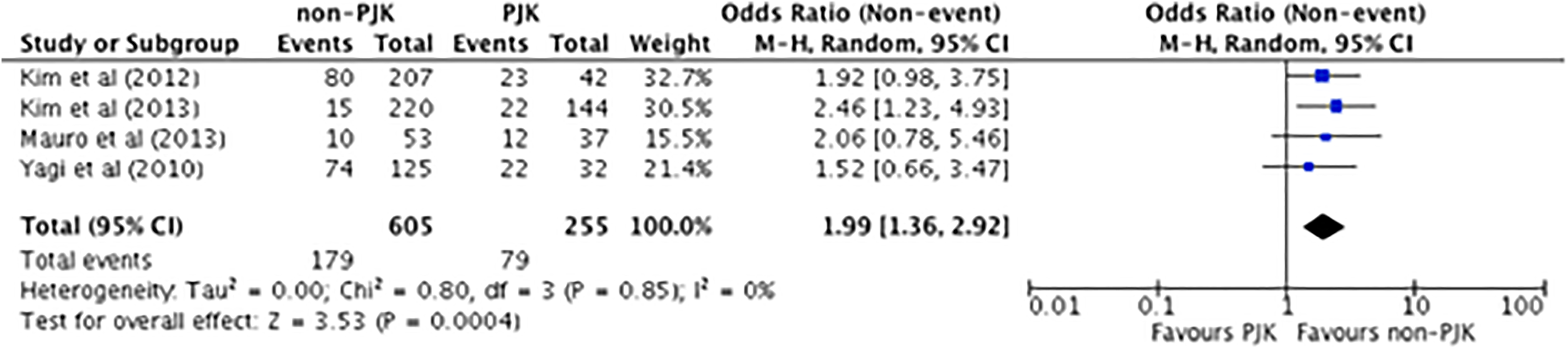
Odds ratio for osteopenia/osteoporosis.
Preoperative sagittal vertical axis (SVA) was significantly higher in the PJK group (n = 183) compared with the non-PJK group (n = 527) (WMD non-PJK vs PJK −17.52; 95% CI −32.06 to −2.98; I2 = 84%; P = .02) (Figure 4). Preoperative SVA was also significantly higher in the PJF group compared with the non-PJK group (WMD non-PJK vs PJF −35.5; 95% CI −58.97 to −12.03; P = .003). Postoperative SVA was significantly higher in PJK patients compared with non-PJK patients (WMD non-PJK vs PJK −7.79; 95% CI −13.54 to −2.04; I2 = 43%; P = .008) (Figure 5). The change in SVA was significantly greater in the PJK group compared with the non-PJK group (WMD non-PJK vs PJK −11.87; 95% CI −21.22 to −2.53; I2 = 70%; P = .01) (Figure 6). Similarly, the change in SVA was significantly greater in the PJF group compared with the non-PJK group (WMD non-PJK vs PJF −34.2; 95% CI −60.60 to −7.80; P = .01).
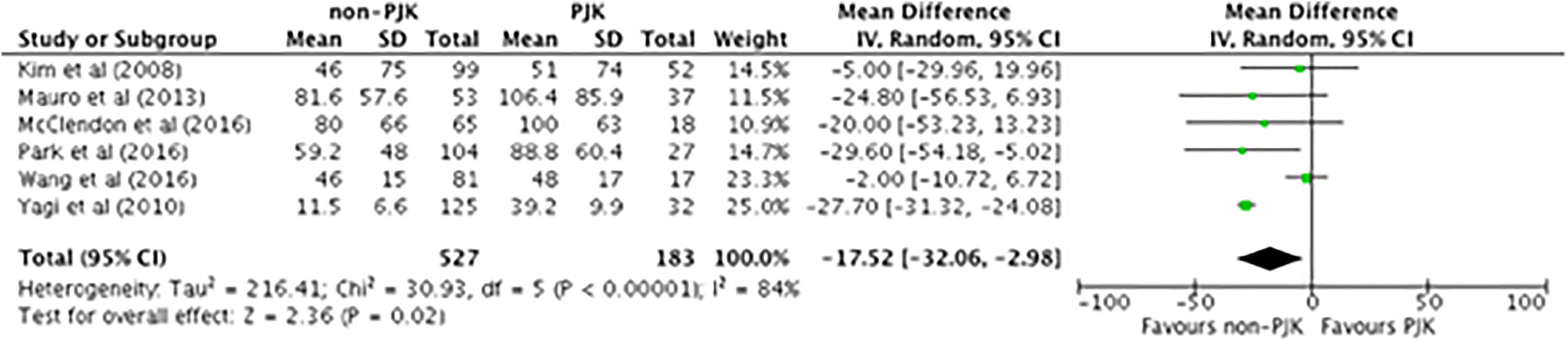
Weighted mean difference for preoperative sagittal vertical axis (SVA).
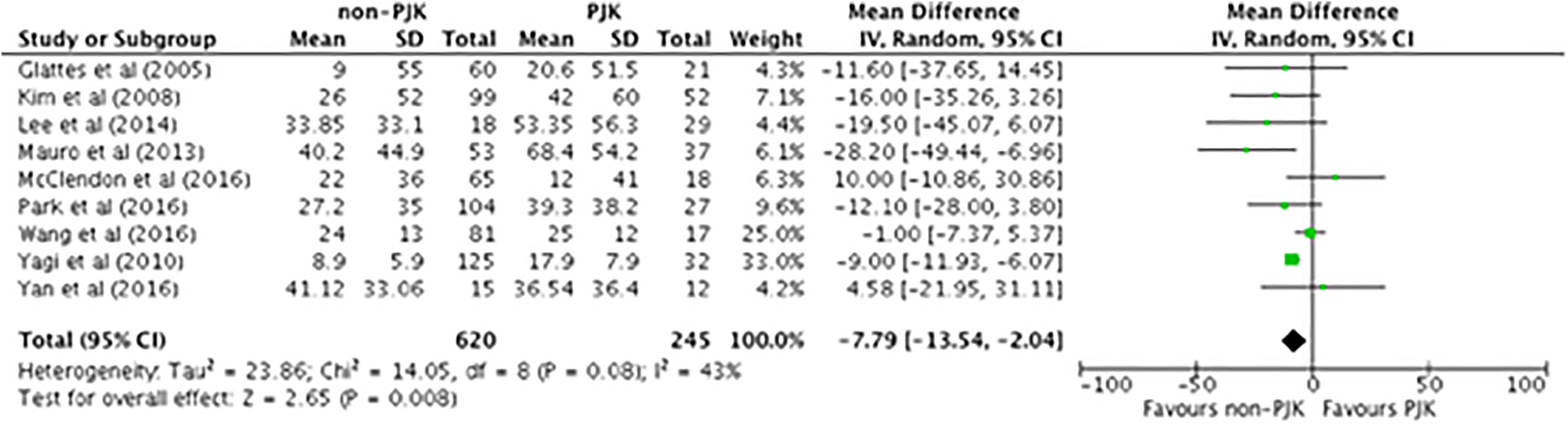
Weighted mean difference for sagittal vertical axis (SVA).
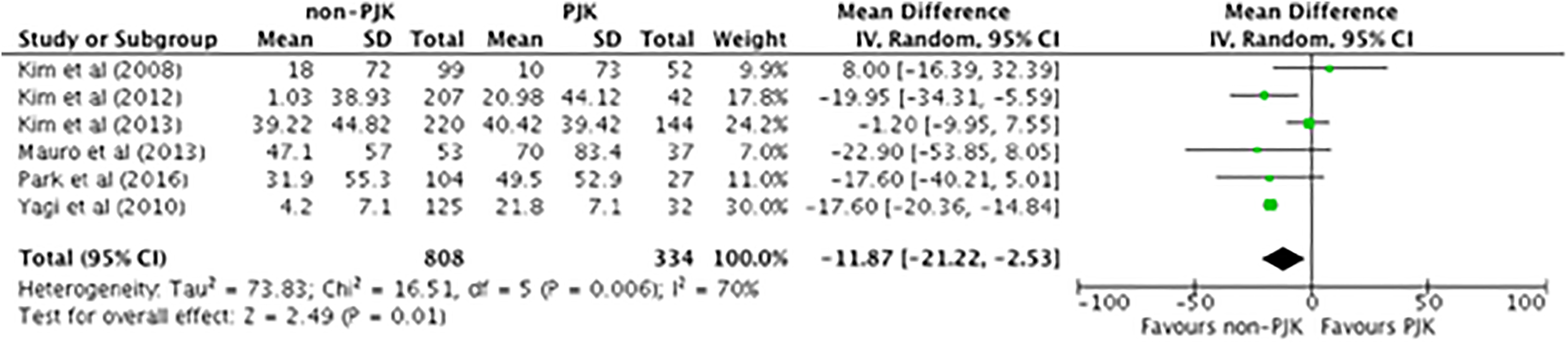
Weighted mean difference for change in sagittal vertical axis (SVA).
There was no significant difference in preoperative thoracic kyphosis (TK) between non-PJK and PJK patients (WMD −1.62; 95% CI −4.66 to 1.43; I2 = 64%; P = .30), and also no difference between non-PJK and PJF patients (WMD −2.66; 95% CI −17.63 to 12.30; I2 = 89%; P = .73). There was no significant difference in postoperative TK between non-PJK and PJK patients (WMD −3.25; 95% CI −7.01 to 0.50; I2 = 82%; P = .09), and also no significant difference between non-PJK and PJF patients (WMD −2.38; 95% CI −12.53 to 7.76; I2 = 74%; P = .65).
Preoperative lumbar lordosis (LL) was significantly lower in PJK patients compared with non-PJK patients (WMD non-PJK vs PJK 1.67; 95% CI 0.59 to 2.74; I2 = 0%; P = .002) (Figure 7). No difference in preoperative LL was found between non-PJK and PJF patients (WMD −1.71; 95% CI −17.07 to 13.64; I2 = 92%; P = .83). There was no significant difference in postoperative LL between non-PJK and PJK patients (WMD −0.41; 95% CI −3.56 to 2.74; I2 = 70%; P = .80), and also no significant difference between non-PJK and PJF patients (WMD 6.19; 95% CI −17.75 to 5.37; I2 = 87%; P = .29). Change in LL was significantly greater in the PJK group compared to the non-PJK group (WMD non-PJK vs PJK −5.61; 95% CI −10.07 to −1.15, I2 = 50%; P = .01) (Figure 8). There was a no significant difference in change in LL between the non-PJK and PJF groups (WMD −7.10; 95% CI −14.49 to 0.29; P = .06).
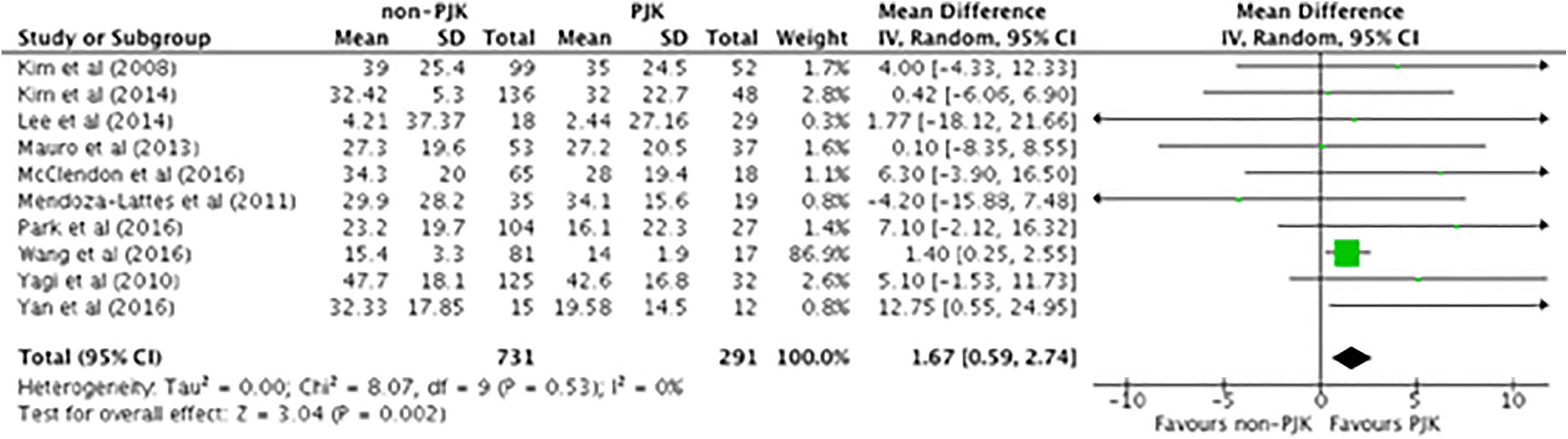
Weighted mean difference for preoperative lumbar lordosis (LL).
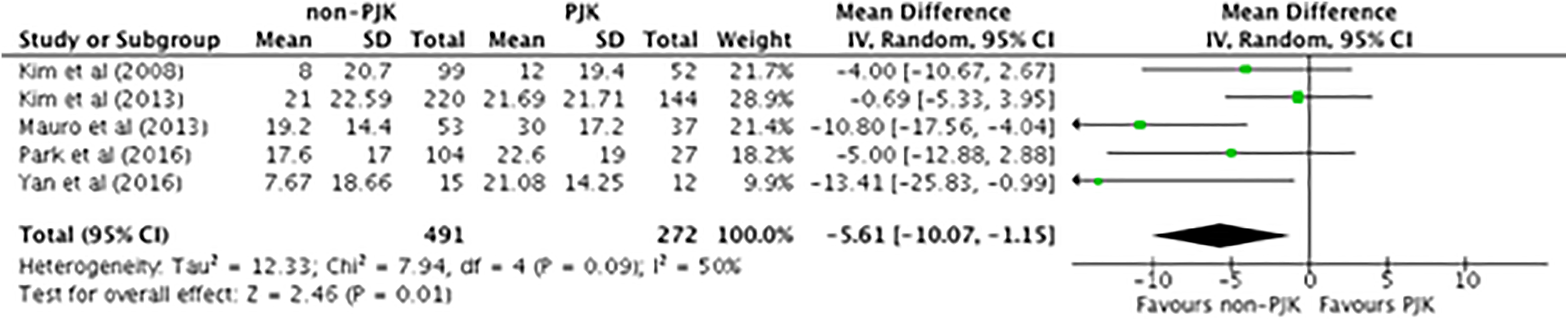
Weighted mean difference for change in lumbar lordosis (LL).
There was no significant difference in preoperative pelvic incidence (PI) between non-PJK and PJK patients (WMD −1.22; 95% CI −3.08 to 0.64; I2 = 0%; P = .20). Preoperative PI was significantly higher in the PJF group compared with the non-PJK group (WMD non-PJK vs PJF −5.50; 95% CI −10.12 to −0.88; P = .02).
No significant difference in the number of levels fused was found between non-PJK and PJK patients (WMD −0.07; 95% CI −0.67 to 0.53; I2 = 0%; P = .82). However, the PJF group had a significantly higher number of levels fused than the non-PJK group (WMD non-PJK vs PJF −2.43; 95% CI −3.07 to −1.79; P < .001).
There was no significant difference in the proportion of patients undergoing a combined anterior-posterior approach between the non-PJK and PJK groups (44.96% vs 56.86%; OR 1.18; 95% CI 0.76 to 1.83; I2 = 40%; P = .45).
No significant difference in the use of hook instrumentation at the UIV was found between non-PJK and PJK patients (35.3% vs 29.2%; OR 0.75; 95% CI 0.46 to 1.21; I2 = 35%; P = .24). There was also no difference between non-PJK and PJF patients (P = .14).
Use of pedicle screw instrumentation at the UIV was significantly higher in PJK patients than non-PJK patients (57.6% vs 40%; OR 1.67; 95% CI 1.08 to 2.59; I2 = 48%; P = .02) (Figure 9). In contrast, there was no significant difference between the non-PJK and PJF groups (64.7% vs 86.4%; OR 3.45; 95% CI 0.97 to 12.27; P = .06).
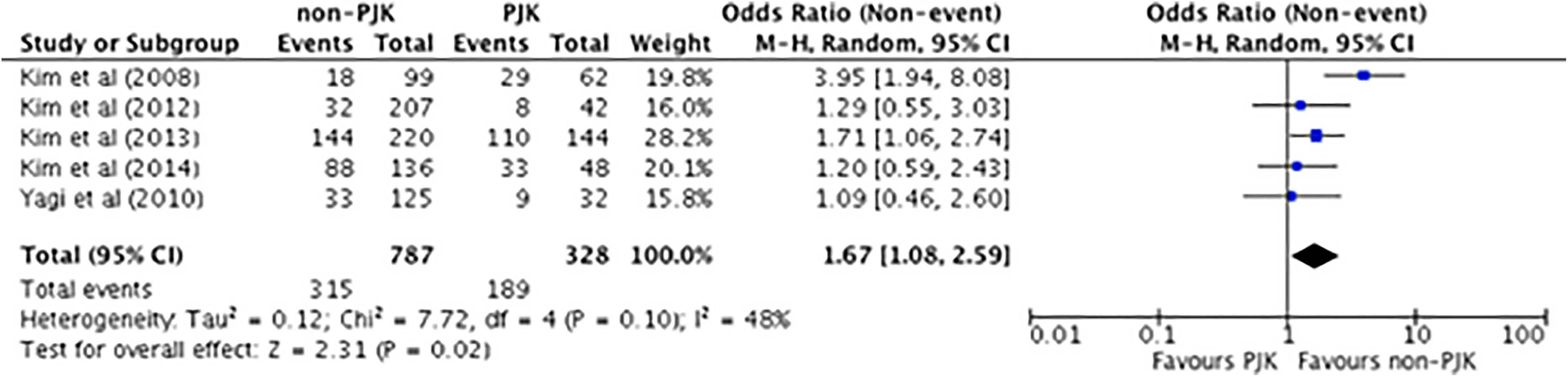
Odds ratio for the use of pedicle screw instrumentation at the upper instrumented vertebra (UIV).
The proportion of patients undergoing fusion to the sacrum/pelvis/iliac region was significantly higher in the PJK group compared with the non-PJK group (71.2% vs 53.6%; OR 2.14; 95% CI 1.58 to 2.91; I2 = 7%; P < .001) (Figure 10). Similarly, the proportion of patients undergoing fusion to the sacrum/pelvis/iliac region was significantly higher in the PJF group compared with the non-PJK group (OR 2.34; 95% CI 1.07-5.13; P = .03).
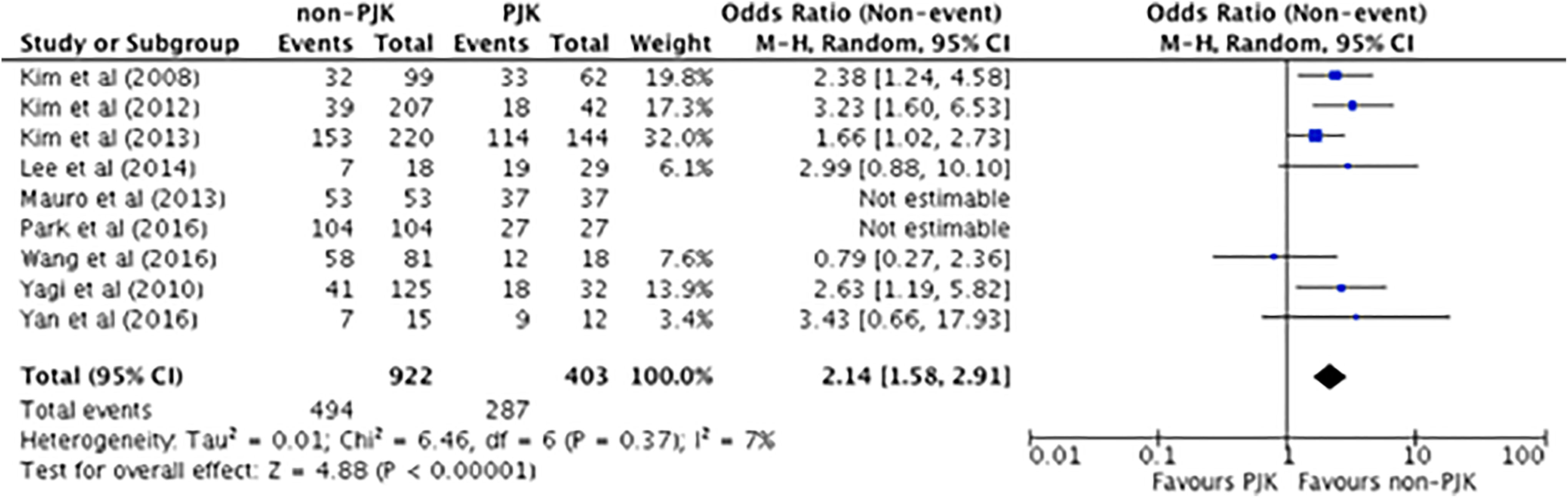
Odds ratio for fusion to the sacrum/pelvis/ilium.
Publication Bias
The number of studies included in the analysis was relatively small, so it was difficult to correlate the funnel plot. Publication bias was not assessed because of the limited number of every factor (\10) of studies included in each analysis.
Discussion
PJK has a multifactorial etiology. Many surgical and patient-related risk factors that have been proposed in the literature remain controversial, and the relative importance of these risk factors has not been fully delineated. 5 -7,12 We performed a meta-analysis to evaluate the risk factors associated with PJK and PJF. The pooled results from this meta-analysis found that (1) PJK and PJF patients were older, (2) PJK patients had a higher prevalence of osteopenia/osteoporosis, (3) PJK and PJF patients had a higher preoperative SVA, (4) PJK patients had a higher postoperative SVA, (5) PJK and PJF patients had a greater correction of SVA, (6) PJK patients had a lower preoperative LL, (7) PJK and PJF patients had a greater correction of LL, (8) PJF patients had a higher preoperative PI, (9) PJF patients had a higher number of levels fused, (10) PJK patients had a higher prevalence of pedicle screw instrumentation at the UIV, and (11) PJK and PJF patients had a higher prevalence of fusion to the sacrum/pelvis/iliac region.
Patients who developed PJK or PJF were 3.74 and 3.80 years older than patients who did not develop PJK, respectively. Four studies identified age as a risk factor for PJK and one study identified age as a risk factor for PJF. 3,5,8,9 This association of age with PJK and PJF may be partially explained by age-dependent disc changes, facet joint degeneration, and less developed paraspinal musculature in older patients. 8 In addition to age, patients with osteoporosis/osteopenia had 2 times higher odds of developing PJK. This is consistent with prior studies that have demonstrated a similar relationship between low bone mineral density and a higher incidence of PJK. 7
Our results demonstrated that the PJK and PJF group had a higher preoperative SVA compared to the non-PJK group, suggesting that these patients had worse radiographic sagittal malalignment that may have predisposed them to the development of proximal junctional disease. The degree of sagittal correction as represented by the change in SVA was significantly greater in the PJK and PJF cohorts. PJK patients had 7.79 mm greater postoperative SVA than non-PJK patients. Our findings are consistent with prior studies that have demonstrated that PJF is associated with greater preoperative SVA and greater SVA correction. 17
PI is another key pelvic parameter that is a functional determinant of sagittal spinal alignment. 18 Increasing SVA has been strongly correlated with an increase in the PI-LL mismatch, which has been associated with adverse patient-reported outcomes. 19,20 In this meta-analysis, we found that preoperative PI was significantly greater in PJF patients, but no difference was seen between the PJK and non-PJK patients. In contrast, preoperative LL was significantly lower in patients who developed PJK, and both patients who developed PJK or PJF had greater correction of LL. Preoperative loss of LL may indicate positive sagittal malalignment, which influences other parameters, such as preoperative SVA. 11 This is consistent with our finding that preoperative SVA was higher in PJK patients. Given that the PJK group had lower preoperative LL with no difference in preoperative PI compared to the non-PJK group, these parameters suggest PI-LL mismatch and sagittal imbalance. The PJK group had a greater correction in LL than the non-PJK group. Unfortunately, our dataset was limited and did not allow us to examine postoperative PI or the correction in PI. Thus, we were unable to determine the role of PI-LL mismatch in the development of PJK and PJF. This is certainly a limitation of this study.
Both over- and undercorrection of SVA and PI-LL mismatch have been proposed as potential risk factors leading to the development of PJK. Yan et al 13 have suggested that in patients who undergo extensive corrective surgery with sagittal overcorrection, postoperative alignment might not be sustainable, as the body tends to balance itself. For instance, they proposed that patients with an overcorrected sagittal profile would unconsciously generate compensatory mechanisms to realign and correct sagittal balance, commonly via the unfused segments and pelvic compensation. 13 Additionally, in patients who undergo aggressive correction, the development of PJK may be influenced by surgical technique. Mauro et al 10 predicted that when rod cantilever techniques with multiple Smith-Peterson osteotomies were used, this could lead to significant stresses at the proximal adjacent disc and vertebrae, which may lead to PJK.
On the other hand, undercorrection of sagittal imbalance can result in persistent or worsening PI-LL mismatch and a positive postoperative global sagittal alignment that may induce positive SVA. Positive SVA may lead to an increase in the mechanical stress at the proximal and distal junction of instrumentation that may result in PJK. 25 Undercorrection of sagittal plane deformity should be avoided, as it leads to disability and poor health-related quality of life measures. 17
Recent studies have suggested that clinical outcomes might benefit from sagittal imbalance corrections that are tailored to individual patient factors such as age. For instance, some studies have demonstrated that SVA increases with age. 21,22,23 Thus, Lafage et al 24 have suggested that it may be acceptable in older patients to have a modest increase in anterior shift and pelvic retroversion. Further research is needed to better delineate the target parameter values and examine the outcomes of age-adjusted realignment targets.
Distal fusion to the sacrum or pelvis was associated with a significantly higher prevalence of PJK. A more rigid construct achieved by anchoring a long fusion segment to the pelvis might lead to a higher prevalence of PJK. 8 Long instrumented fusions to the sacrum leave the proximal unfused levels to adjusted to any further compensation. 25 Smith et al 3 demonstrated a significant relationship between fusion to the sacropelvic region and PJF. Eliminating motion at the caudal end of the construct places added stress at the cephalad end, leading to kyphosis and/or failure. Performing a fusion to the sacrum requires careful consideration. Yagi et al 25 suggested that although a long fusion to the sacrum was associated with PJK, it was beneficial for adult scoliosis patients because it mitigated accelerated degeneration of the L5-S1 disc and subsequent sagittal decompensation. Kim et al 8 found that a higher number of levels fused was significantly greater in the PJF cohort than the non-PJK cohort. Longer fusions that reach the upper thoracic vertebrae and higher number of levels fused (suggesting a greater implant density) may contribute to development of PJF. 11
Use of pedicle screw instrumentation at the UIV was a risk factor for PJK. Use of pedicle screws may lead to soft tissue damage (eg, the ligamentous structures and capsule of the supra-adjacent facet) that can influence proximal junctional strength and stability. Soft tissue damage can be further compounded by an increasing number of levels that are dissected and exposed. Pedicle screws at the UIV create a more rigid construct compared to other instrumentation methods such as transverse process hooks. This may contribute to increased stress on the proximal junction by transmitting force through the UIV to the proximal junction. Preserving soft tissue during dissection increases proximal soft tissue integrity and may contribute to preventing the development of PJK. 26
There were several limitations in this study. The heterogeneity of the studies remains with regard to patient demographics and severity of disease is a concern in any meta-analysis. The studies reporting PJF were few and further research is needed with regard to this disease entity. There may be other factors (ie, selection of UIV, mismatch between rod-contouring, postoperative proximal spinal curve) that may be contributing risk factors but were not analyzed in this study. Many of these factors are likely not independently associated with PJK, and it is possible that there are confounding variables.
Conclusion
The risk factors for PJK were age, osteoporosis/osteopenia, high preoperative SVA, high postoperative SVA, and low preoperative LL, use of pedicle screws at UIV, SVA change/correction, LL change/correction, and fusion to sacrum/pelvis/iliac region. The risk factors of PJF include age, high preoperative SVA, SVA change/correction, fusion to sacrum/pelvis/iliac region, high preoperative PI, and greater number of levels fused. However, smoking, BMI, preoperative TK, anterior-posterior combined surgical approach, usage of hook at UIV, postoperative LL, and postoperative thoracic kyphosis were not associated with PJK or PJF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.