
Abstract
Study Design
Retrospective study.
Objective
To investigate the impact of preoperative C2 slope (C2S) on change in sagittal vertical axis (SVA) and postoperative cervical sagittal imbalance (CSI) after laminoplasty (LP).
Methods
Consecutive patients who underwent LP between January 2015 and January 2022 with a minimum of 12-month follow-up were reviewed. The clinical variables and radiographic measurements were assessed. Patients were divided into improvement (ΔcSVA ≤ −10 mm), stable (−10 mm ≤ ΔcSVA <10 mm), and CSI groups (ΔcSVA≥10 mm). Correlation analysis was performed to explore the associations between ΔcSVA and preoperative factors, postoperative change and outcome variables. Multivariable logistics regression was conducted to determine the factors predicting CSI.
Results
Over the 186 enrolled patients, 23 developed CSI. The CSI group presented with significantly lower preoperative cSVA, greater cervical lordosis (CL) and C2S. At the final follow-up, the CSI group presented significantly higher increase in neck pain, C2S and C7S, and greater loss in CL and range of motion at flexion position. Correlation analysis revealed that ΔcSVA is correlated positively to preoperative CL and surgical segments and negatively to preoperative C2S and cSVA. Multivariable regression revealed that lower preoperative C2S (P = 0.026) was risk factor for postoperative CSI, with 8.9 as a potential cut-off value for C2S.
Conclusions
Lower preoperative C2S slope was risk factor for post-laminoplasty CSI. The cut-off value of C2S was 8.9. Laminoplasty should be carefully considered for patients with low C2S due to risk of postoperative CSI.
Background
Degenerative cervical myelopathy (DCM) is one of the most common reasons of disability in elderly patients. 1 Laminoplasty (LP) is a commonly used procedure for multilevel DCM (MDCM), which provides posterior decompression for spinal cord with satisfactory clinical outcomes.2-4 However, patients might experience postoperative increase in C2-7 cervical sagittal vertical axis (cSVA) and kyphosis change after laminoplasty, which has become an increasing concern.5-8
Abundant studies have associated the cervical sagittal imbalance (CSI) with postoperative neck pain, less ideal neurological function recovery and less favorable health related quality of life (HRQOL).9-13 Though the potential factors and mechanism for postoperative CSI after LP remain not fully understood, surgeons have reported different preoperative predictive factors for postoperative CSI, such as K-line tilt, paraspinal sarcopenia, preoperative ROM-F and T1 slope (T1S) and cervical lordosis (CL) mismatch (T1S minus CL, T1S-CL).14-18 However, the measurement of T1S-CL could be complicated as it needs collection and calculation of 2 parameters and sometimes impossible due to obstruction of shoulder.
Recently, C2 slope (C2S) has been highlighted as an important parameter for horizontal gaze, and an easily visible substitute for the T1S-CL. 19 As a one-step measurement, the C2S is equivalent to T1S-CL in mathematical form (T1S-CL = T1S-C7S + C2S ≈ C2S), while is easier to measure, and free from obstructions. Generally, the C2S has same relations with other cervical alignment parameters and pastient reported outcomes as T1S-CL does (positively to cSVA, and negatively to CL).19-21 However, few studies have evaluated the impact of C2S on CSI after laminoplasty. From where we stand, lower C2S might represent preoperative over-extension of C2, which might lead to higher potential of C2S decrease after surgery and thus higher increase of cSVA and CSI.
Therefore, we designed this retrospective study to explore the potential impacts of the preoperative factors, especially the C2S, on post-LP cSVA change and identify risk factors for post- LP CSI. In this study, CSI was defined as an increase in cSVA greater than 10 mm. 15 Our hypothesis is that C2S could be an effective predictor for post-LP CSI, and in patients with given comparable cSVA, the patients with lower C2S have a higher risk of post-LP CSI.
Methods
Patient Population
A total of 186 patients with MDCM who underwent laminoplasty between January 2015 and January 2022 were retrospectively included in this study. The study was approved by ethics committee of our hospital (IRB00006761-2016001). The requirement for informed consent was waived due to the retrospective nature of our study.
The inclusion criteria were as follows: (1) received LP for confirmed MDCM by clinical symptoms and radiological evidence (2) a minimum of 12-month follow-up. The exclusion criteria included: (1) preoperative CSI or cervical kyphosis, (2) previous history of spinal surgeries, cervical spine fracture or infection, (3) presence of cervical OPLL (4) previous history of congenital cervical deformity, ankylosing spondylitis or rheumatoid arthritis, and (5) patients whose C7 vertebral bodies could not be identified on lateral radiographs.
All patients underwent expansive open-door laminoplasty performed using the Hirabayashi method by 3 senior spine surgeons from single surgery unit of our orthopedic department. 2 The muscular attachments on C2 and/or C7 were routinely preserved as much as possible. All patients were allowed to get out of bed on the first day after surgery and wear a cervical collar for 2 weeks. Routine follow-ups were arranged for patients at 3 months, 6 months, 1 year, 3 years, and 5 years after surgery.
Clinical Evaluations
The demographic and comorbidity data were retrospectively collected from electronic medical records. The preoperative and postoperative neck pain was assessed by numerical rating scale (NRS). The preoperative and postoperative Japanese Orthopedic Association (JOA) score and JOA improvement and JOA recovery rate (JOARR) at the final follow-up was assessed.
Radiological Evaluations
The preoperative and postoperative cervical sagittal balance parameters were measured using neutral and flexion-extension radiographs preoperatively and at follow-up.
The cervical curvature and range of motion (ROM) were evaluated according to the Cobb angle method. The measured parameters were as follows: C2−C7 lordosis Cobb angle (CL); C2−C7 lordosis Cobb angle on extension lateral radiography (CL-E); C2−C7 lordosis Cobb angle on flexion lateral radiography (CL-F); C7 slope (C7S), defined as the angle between the horizontal line and the upper endplate of C7; C2 slope (C2S), defined as the angle between the horizontal line and the lower endplate of C2; C2-7 sagittal vertical axis (cSVA), measured as the total distance from the plumb line of the center of the C2 vertebra to the posterosuperior corner of the C7 vertebra (Figure 1). Example of the radiological measurements. Measurements of cervical radiological parameters: a: C2-7 Cobb angle; b: C2 slope angle; c: C7 slope angle; d: C2-7 cSVA.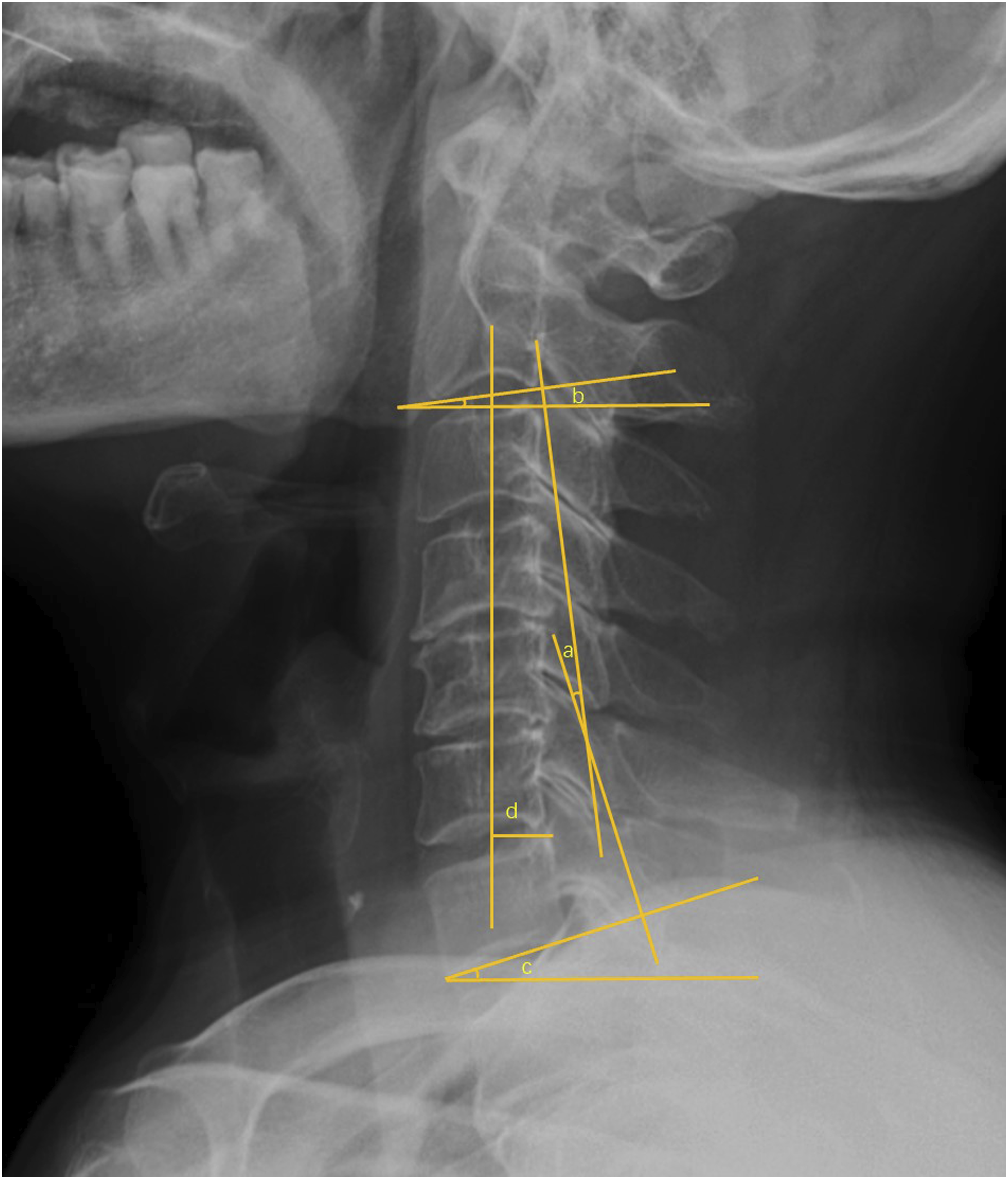
The cervical range of motion (ROM) was calculated as the CL-E minus CL-F. The extension and flexion capacity of cervical spine was assessed by the extension ROM (ROM-E) and flexion ROM (ROM-F), calculated by the CL-E minus CL and CL minus CL-F, respectively. ΔcSVA was calculated by the postoperative cSVA minus preoperative cSVA and patients were divided into improvement group (ΔcSVA ≤ −10 mm), stable group (−10 mm ≤ ΔcSVA <10 mm) and CSI group (ΔcSVA≥10 mm). 15
All measurements were conducted by 2 trained spine surgeons separately. The values were measured by both surgeons under supervision of a senior surgeon, and then the results were averaged.
Statistical Analysis
All the statistical analyses were performed using STATA (version 16.0; Stata Corp LLC, Texas, USA). Continuous variables are summarized as the mean ± standard deviation unless otherwise noted, and categorical variables are summarized as numbers and percentages. Intergroup differences were analyzed using the χ2 test, T tests and nonparametric tests. Spearman and Pearson correlation analysis were conducted on all potential factors and ΔcSVA to explore potential association between variables and confounding factors. A multivariable logistic regression analysis was conducted with all preoperative factors which showed significant correlation with ΔcSVA to control confounding bias. Odds ratios (ORs) and 95% confidential intervals (CIs) were calculated and a receiver operating characteristic (ROC) curve analysis was conducted and the cut-off value was determined.
Results
Patient Population and Baseline Characteristics
Among the 186 patients included, there were 123 males and 63 females, with a mean age of 54.5 ± 10.6 years old. The average preoperative JOA score of all patients was 12.9 ± 2.0. The mean surgery durations were 112.6 ± 37.0 mins, and the mean estimated blood loss was 166.7 ± 117.4 mL. The mean follow-up duration was 31.4 ± 7.8 (12 to 36) months.
The Preoperative Demographic, Clinical and Surgical Characteristics of Three Groups.
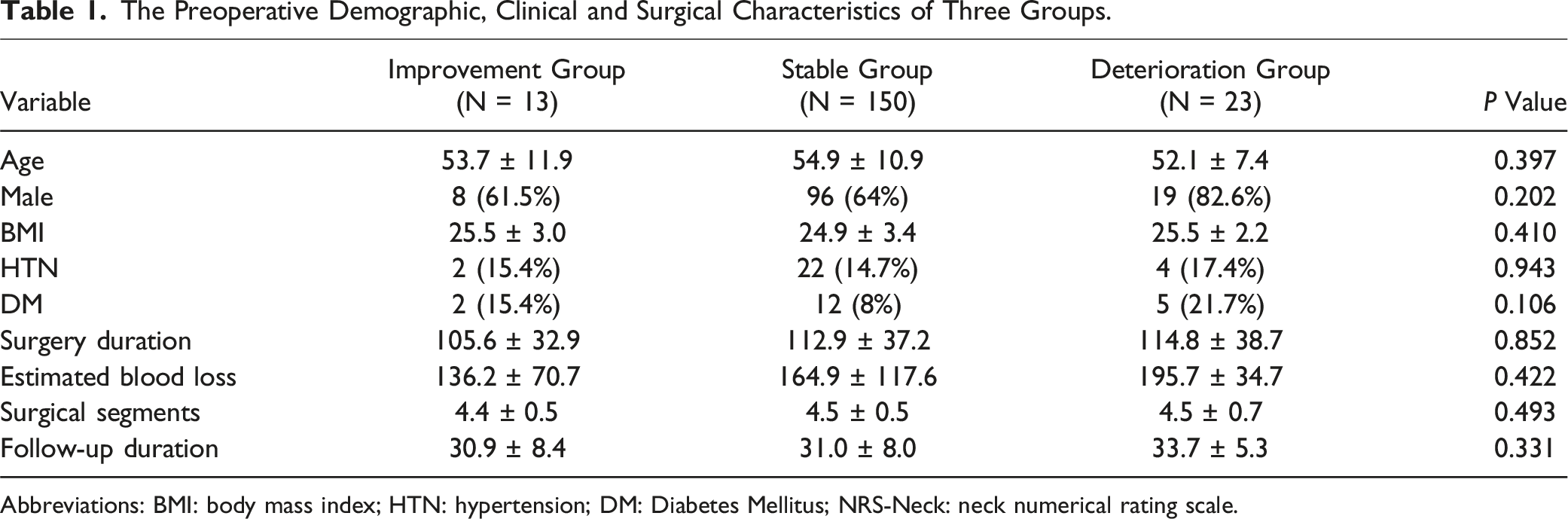
Abbreviations: BMI: body mass index; HTN: hypertension; DM: Diabetes Mellitus; NRS-Neck: neck numerical rating scale.
The Preoperative Cervical Sagittal Balance Parameter of Three Groups.
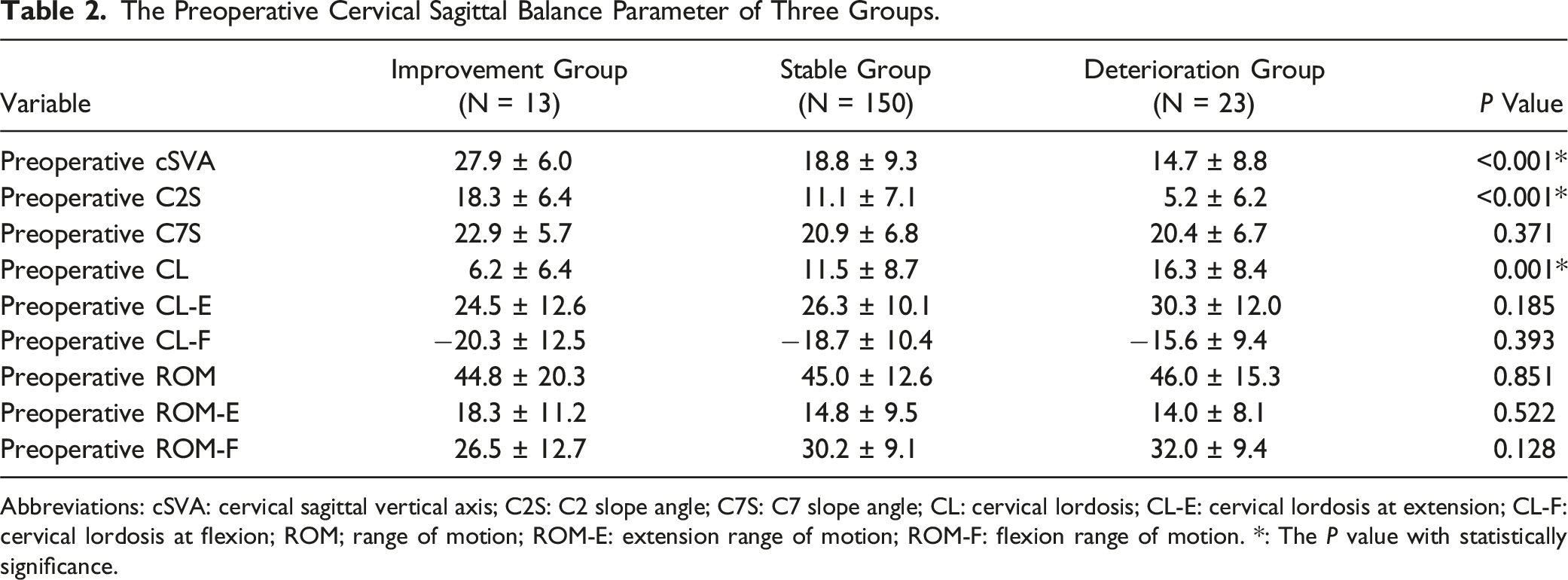
Abbreviations: cSVA: cervical sagittal vertical axis; C2S: C2 slope angle; C7S: C7 slope angle; CL: cervical lordosis; CL-E: cervical lordosis at extension; CL-F: cervical lordosis at flexion; ROM; range of motion; ROM-E: extension range of motion; ROM-F: flexion range of motion. *: The P value with statistically significance.
Patient Reported Outcomes of Three Groups
The Patient Reported Outcomes of Three Groups.
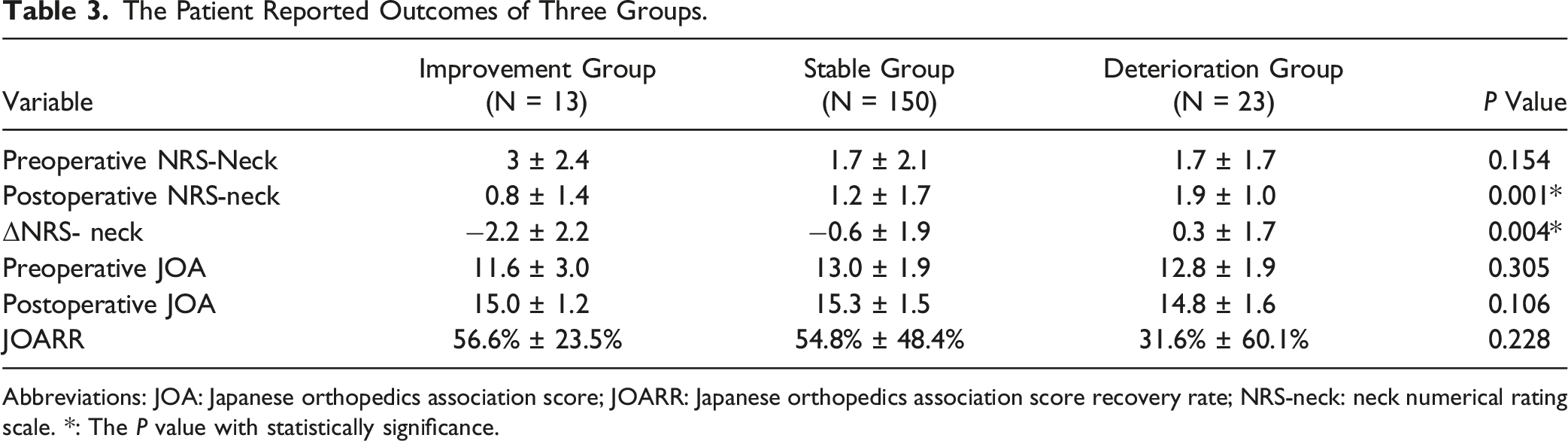
Abbreviations: JOA: Japanese orthopedics association score; JOARR: Japanese orthopedics association score recovery rate; NRS-neck: neck numerical rating scale. *: The P value with statistically significance.
However, the CSI group presented significantly higher postoperative NRS-neck than the other groups. Furthermore, the CSI group presented significantly increased neck pain (ΔNRS- neck:0.3 ± 1.7), while the other 2 groups presented with alleviated neck pain (improvement group ΔNRS- neck: −2.2 ± 2.2, stable group ΔNRS- neck: −0.6 ± 1.9) postoperatively (P = 0.004).
Cervical Balance Parameter Outcomes of Three Groups
The Postoperative Change in Cervical Balance Parameters of Three Groups.
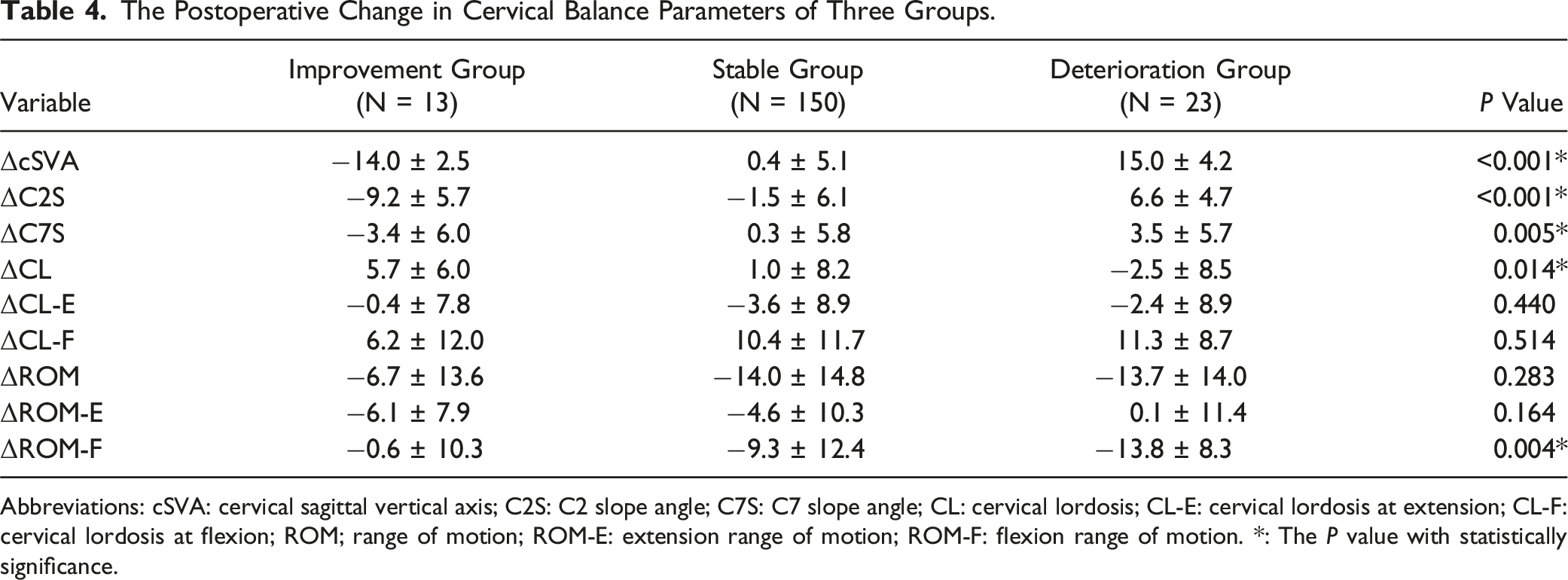
Abbreviations: cSVA: cervical sagittal vertical axis; C2S: C2 slope angle; C7S: C7 slope angle; CL: cervical lordosis; CL-E: cervical lordosis at extension; CL-F: cervical lordosis at flexion; ROM; range of motion; ROM-E: extension range of motion; ROM-F: flexion range of motion. *: The P value with statistically significance.
Correlation Analysis
Relationship Between ΔcSVA and Change of Other Sagittal Balance Parameters and Patient Reported Outcomes
Correlations Between ΔcSVA, Postoperative Change in Other Cervical Balance Parameters and Patient Reported Outcomes.
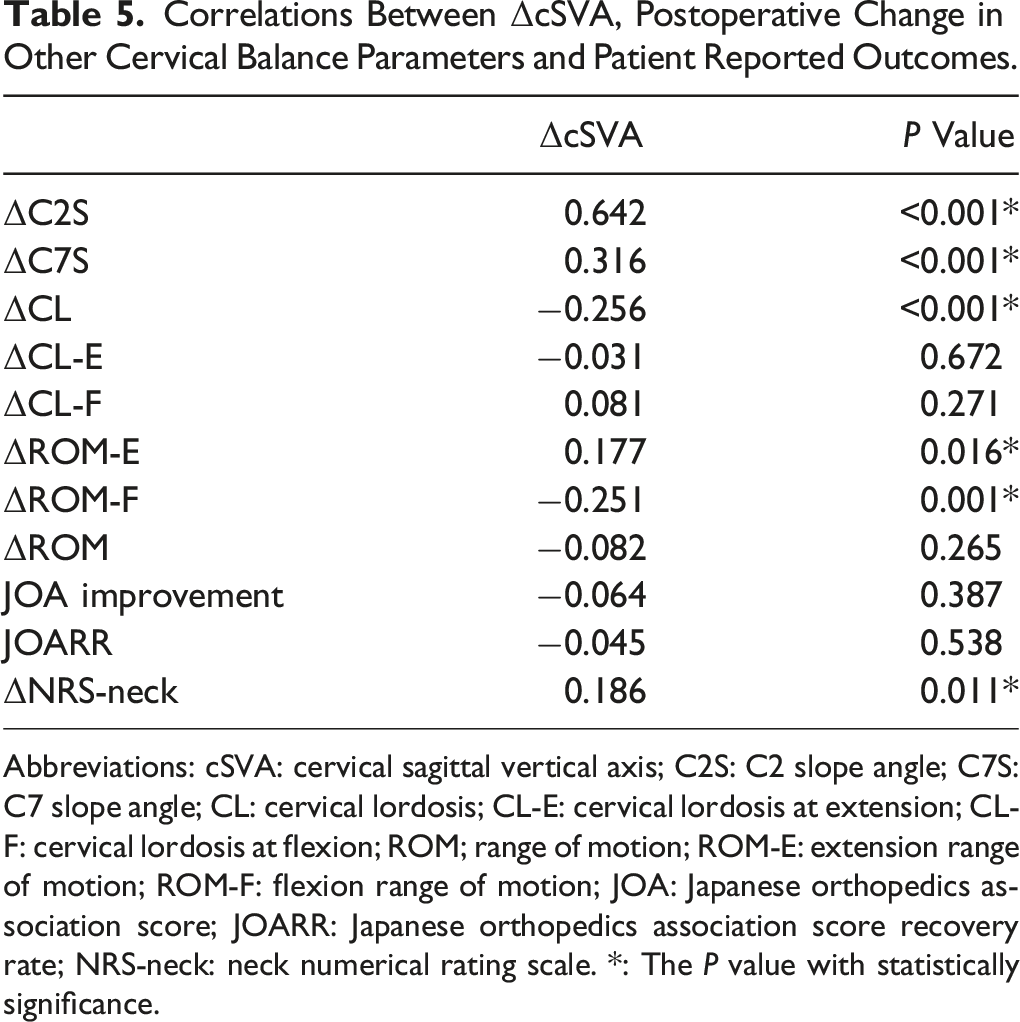
Abbreviations: cSVA: cervical sagittal vertical axis; C2S: C2 slope angle; C7S: C7 slope angle; CL: cervical lordosis; CL-E: cervical lordosis at extension; CL-F: cervical lordosis at flexion; ROM; range of motion; ROM-E: extension range of motion; ROM-F: flexion range of motion; JOA: Japanese orthopedics association score; JOARR: Japanese orthopedics association score recovery rate; NRS-neck: neck numerical rating scale. *: The P value with statistically significance.
Relationship Between ΔcSVA, ΔC2S and Preoperative Factors
Correlations Analysis Between ΔcSVA, ΔC2S and Preoperative Factors.
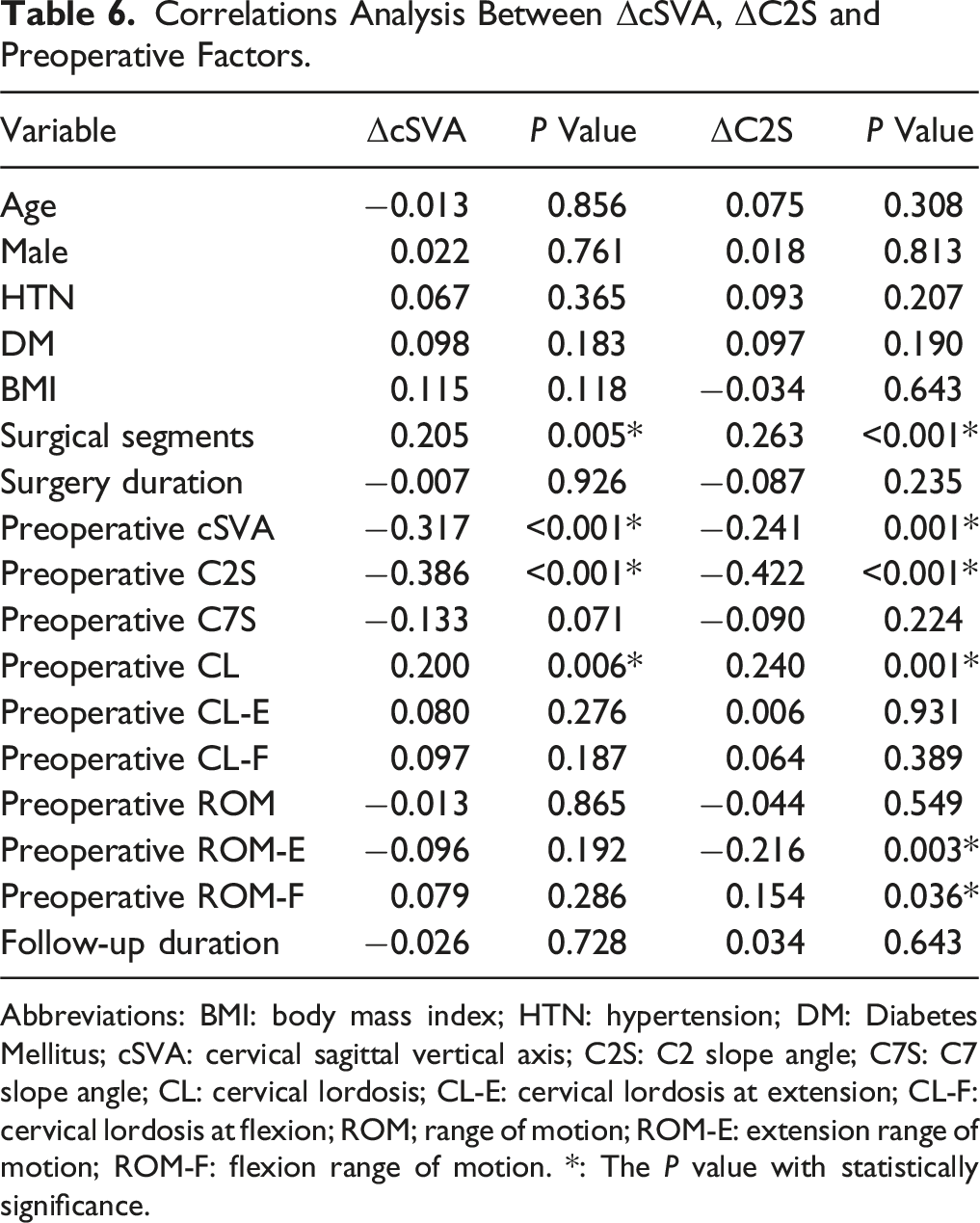
Abbreviations: BMI: body mass index; HTN: hypertension; DM: Diabetes Mellitus; cSVA: cervical sagittal vertical axis; C2S: C2 slope angle; C7S: C7 slope angle; CL: cervical lordosis; CL-E: cervical lordosis at extension; CL-F: cervical lordosis at flexion; ROM; range of motion; ROM-E: extension range of motion; ROM-F: flexion range of motion. *: The P value with statistically significance.
Multivariable Logistics Regression Analysis
Multivariable Logistics Regression Analysis for Predicting Postoperative CSI.
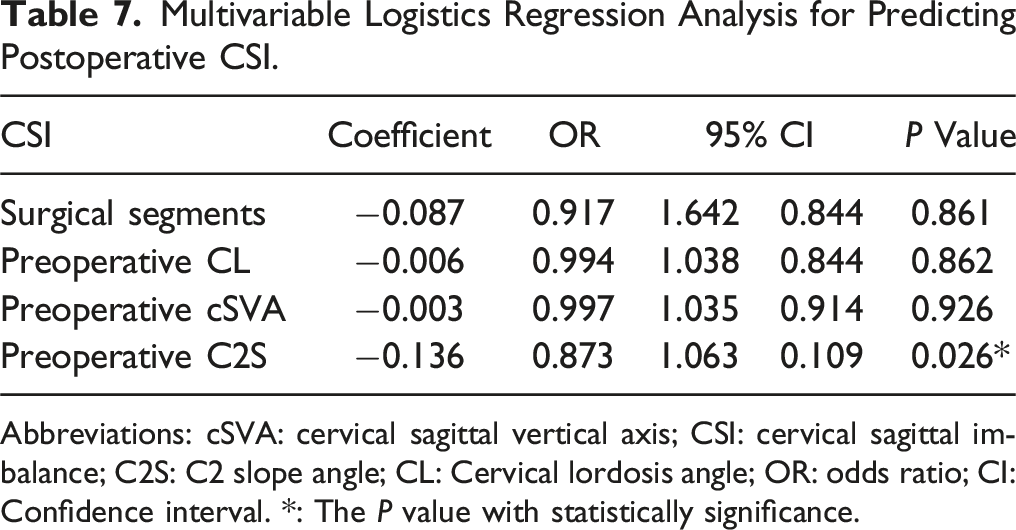
Abbreviations: cSVA: cervical sagittal vertical axis; CSI: cervical sagittal imbalance; C2S: C2 slope angle; CL: Cervical lordosis angle; OR: odds ratio; CI: Confidence interval. *: The P value with statistically significance.
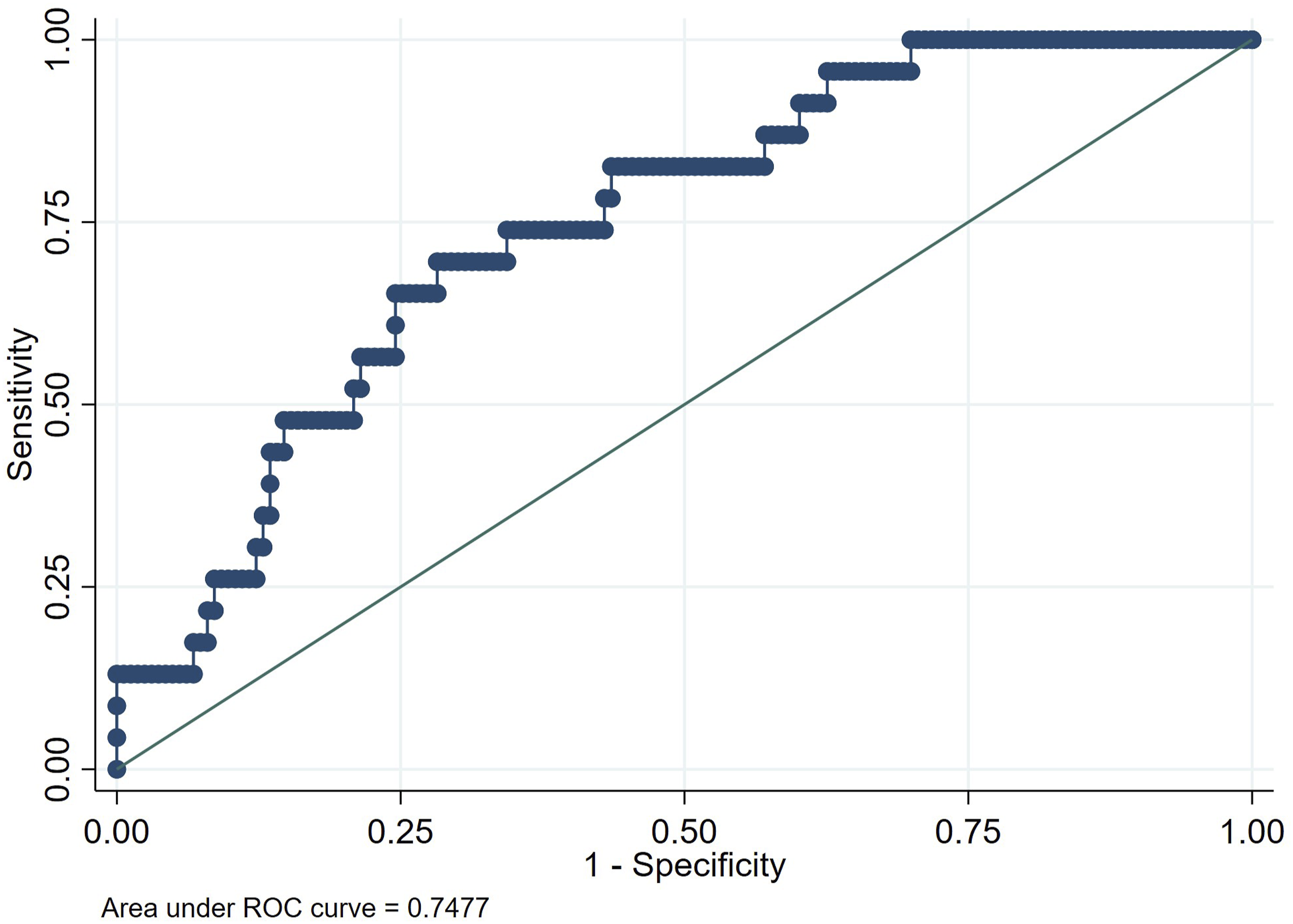
The receiver operating characteristic curve analysis of the mutivariable logistics regression model.
Discussion
In this study, we sought to explore the impact of preoperative C2S on ΔcSVA, and to identify potential risk factors of CSI after laminoplasty. Our results firstly demonstrated that after adjustment of the confounders, C2S was negatively associated with ΔcSVA, and lower C2S might be risk factor for postoperative CSI. We advocated surgeons paying more attention to the preoperative C2S when planning laminoplasty. Meanwhile, for patients with preoperative high cSVA and low C2S, posterior fusion procedure or other alternatives might also be considered.
Cervical sagittal balance is important in maintaining head posture and horizontal gaze. 22 Postoperative CSI usually leads to more excessive work of the posterior paraspinal muscles and might result in post-LP axial pain. 23 Literature has also reported postoperative CSI is often accompanied by loss in CL, which could impact cord posterior drifting and lead to poor neurological recovery.24-28 In this study, we found the CSI patients present significantly more severe neck pain than non-CSI patients. Meanwhile, correlation analysis revealed that ΔcSVA was associated with higher postoperative neck pain and less neck pain alleviation (Table 5). These results were consistent with existing literature. However, though the non-CSI group have a trend of higher JOARR, no significant intergroup difference was found. Another interesting finding was that cSVA increase might lead to decreased flexion capacity and increased extension capacity.
Previous studies have explored the relationship between cSVA and other sagittal balance parameters, however, the potential risk factors for postoperative CSI after LP remain not fully understood. In general, the cSVA was positively correlated to T1S, C7S, C2S and negatively correlated to CL.29,30 Furthermore, Rao et al 17 have reported patients with preoperative T1S and CL mismatch could have higher postoperative cSVA. However, importantly, Abe et al 18 have reported the ΔcSVA was negatively correlated with preoperative T1S-CL, but in which study no appropriate adjustment of confounders, especially the preoperative cSVA, was conducted. Meanwhile, several studies have reported the strong correlations between C2S, a substitute of T1S-CL, and other sagittal parameters and patient reported outcomes in anterior cervical discectomy and fusion, posterior decompression and fusion surgery and cervical deformity surgeries.19-21,31 However, few studies have investigated the impact of C2S on ΔcSVA after laminoplasty.
In our study, correlation analysis was conducted to explore the relation of parameters and ΔcSVA, and screen for potential risk factors of CSI. The results showed that ΔcSVA is significantly positively correlated to surgical segments (r = 0.205, P = 0.005) and preoperative CL (r = 0.200, P = 0.006), and negatively correlated with preoperative cSVA (r = −0.317, P < 0.001) and preoperative C2S (r = −0.386, P < 0.001) (Table 6). This result was consistent with Abe’s study (preoperative T1S-CL: r = − 0.28, P = 0.004) and Liu’s study (preoperative cSVA: r = −0.251, P < 0.05).14,15 Interestingly, recent study has reported higher flexion capacity (ROM-F) as possible risk factor for postoperative CSI after LP, however, this correlation was not observed in our study. 15
As C2S was significantly correlated to cSVA, multivariate logistic regression was conducted to control the confounding bias (Table 7). The regression results showed that lower preoperative C2S is significant singular risk factor for postoperative CSI, which means that for patients with given preoperative cSVA, the patients with lower preoperative C2S might have higher risk of CSI than those with higher C2S. This result has not been reported before, while we supposed it is reasonable, as Abe et al have proposed T1S-CL could be negatively associated with cSVA increase. 14
We speculated the possible mechanism of this association might be as follows: C2S might represent the preoperative over-extension of C2. For patients with similar preoperative cSVA preoperatively, the patients with lower preoperative C2S rely on an higher over-extension of C2 to maintain cervical balance. After the surgery, this over-extension was disrupted along with the intraoperative damage on posterior muscles, and the C2S increased along with the force of head weight, then the cSVA increased accordingly. On contrast, the patients with higher preoperative C2S did not rely much on this over-extension capacity preoperatively to maintain horizontal gaze, thus the posterior damage might have less impact on the C2S, and then the C2S and cSVA tend to be maintained (Figure 3). A potential proof of this mechanism was that the ΔC2S was significantly negatively correlated with preoperative ROM-E, which means patients without over-extension might have less C2S increase postoperatively. Illustration of 2 cases with similar preoperative cSVA and distinct preoperative C2S and the possible mechanisms. A and C represent 2 patients with similar preoperative cSVA and distinct C2S. B and D represent the postoperative cervical alignment of 2 patients. A: A 60 year-old male, the preoperative cSVA is 8.76 mm and the preoperative C2S is :12.9°. C: A 52 year-old male, the preoperative cSVA is 2.88 mm and the preoperative C2S is 6.7°. B: After surgery, the C2S in patient C increased to 23.1° and the cSVA of patient C increased to 25.6 mm. D: On the contrast, the C2S of patient A maintained at 8.3 °and the cSVA decreased to 5.23 mm.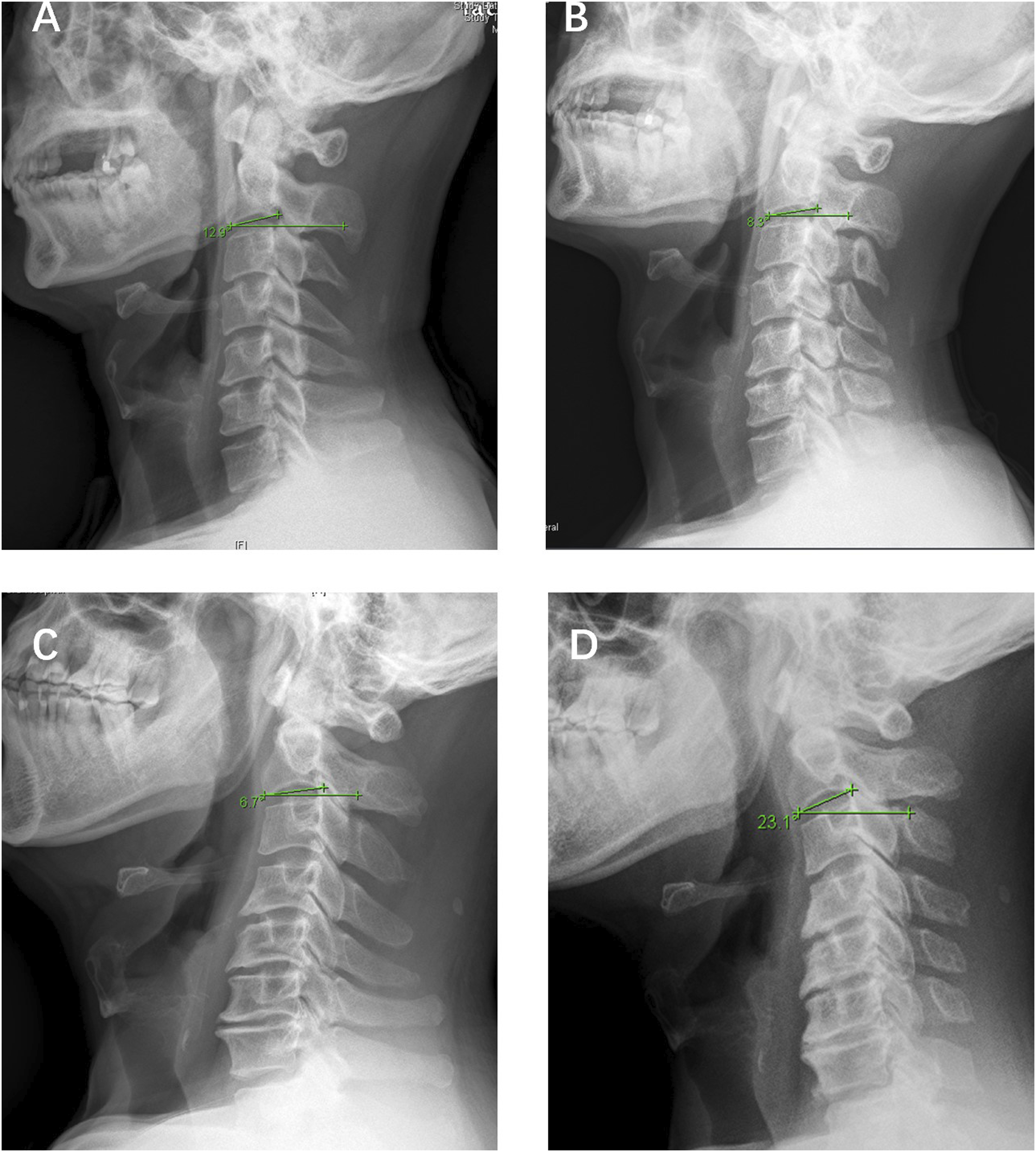
Though some previous studies have suggested the association between T1S-CL and ΔcSVA and investigated C2S, limited studies have focused on the impact of C2S on postoperative CSI after laminoplasty. This study firstly reported that the C2S was negatively associated with cSVA increase after laminoplasty, and could serve as risk factor for post-LP CSI prediction. From where we stand, the C2 slope is an easier measurement compared to T1S-CL, and would not be unmeasurable due to obstruction of T1 vertebra. We suggested 8.9 as a cut-off value of C2S based on ROC analysis (Figure 2). We advocate the evaluation of C2S in the assessment of risk of post-LP CSI before surgery. For patients with C2S lower than 8.9, especially with preoperative boundary high cSVA (30∼40 mm), LP should be carefully considered. Further studies are needed to explore the impact and mechanism of C2S on CSI after laminoplasty.
There were several limitations to be acknowledged in this study. First, this study is a retrospective cohort study without randomized and prospective design, which introduced unavoidable bias. Secondly, though the area under the curve is relatively large, the CSI sample was relatively small and external validation was lacked, which might lead to limitations of its prediction efficacy and limit the generalizability of our prediction model. Thirdly, there could be measurement bias. Further validation of our results would further clarify the impact of C2S on CSI. We are also planning further studies with assessment of C2 slope extension capacity (C2S at extension minus at C2S at neutral position) and global alignment including thoracic kyphosis and lumbar lordosis, to study the specific role of C2S in CSI after laminoplasty and potential mechanisms.
Conclusions
Patients with CSI have lower pain alleviation than those without. Despite developing imbalance, achieving decompression provides meaningful JOA improvement as well. Lower preoperative C2S slope might represent an over-extension state of C2, and could be a risk factor for CSI after laminoplasty. The cut-off value of C2S was 8.9. Laminoplasty should be carefully considered for patients with low C2S and boundary cSVA due to risk of postoperative CSI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.