
Abstract
Study Design:
Retrospective radiographic study.
Objectives:
T1 slope is an important parameter of sagittal spinal balance. However, the T1 superior endplate can be difficult to visualize on radiographs due to overlying anatomical structures. C7 slope has been proposed as a potential substitute for T1 slope when the T1 superior endplate is not well visualized. The objective of this study was 2-fold: (1) to assess the correlation between C7 and T1 slopes on upright cervical spine radiographs and (2) to evaluate the interrater reliability of C7 slope.
Methods:
Cervical spine radiographs taken between December 2017 and June 2018 at a single institution were reviewed. Two observers measured upper C7 slope, lower C7 slope, and T1 slope. The correlations between upper and lower C7 slope and T1 slope were evaluated, and linear regression analyses were performed. Interrater reliability of C7 slope was also assessed.
Results:
In this cohort of 152 patients, there was a strong correlation between upper C7 slope and T1 slope (r = 0.91, P < .001), as well as between lower C7 slope and T1 slope (r = 0.90, P < .001). T1 slope could be estimated from the linear regression equation, T1 slope = 0.87 × C7 slope + 7, with an overall model fit of R 2 = 0.8. There was strong interrater reliability for upper (intraclass correlation coefficient [ICC] = 0.95, P < .001) and lower C7 slope (ICC = 0.96, P < .001).
Conclusions:
Both the upper and lower C7 slope are strongly correlated with T1 slope and can be used as a substitute to estimate T1 slope when the superior endplate of T1 is not well visualized.
Introduction
Sagittal imbalance in the cervical spine is a major cause of fatigue, headache, neck pain, and disability. 1 -5 Parameters that characterize overall cervical sagittal balance include C2 to C7 lordosis and C2 to C7 sagittal vertical axis (SVA). However, these parameters do not fully characterize cervical sagittal balance and various new parameters have been proposed. Of these proposed parameters, T1 slope is one of the most important determinants of overall spinal sagittal balance. 6,7
A high T1 slope can be the result of thoracic hyperkyphosis or lumbopelvic sagittal malalignment, which can cause a compensatory anterior tilt of the cervical spine and a forward head posture. 8,9 A T1 slope greater than 40° has been associated with worse clinical outcomes in patients with adult spinal deformity. 10 In contrast, a T1 slope less than 25° has been associated with a higher degree of cervical disc degeneration and is a risk factor for cervical spondylosis. 11
While T1 slope has been demonstrated to be an important parameter of cervical sagittal balance, measurement of T1 slope can be difficult due to the anatomical positioning of the shoulders, especially in obese patients with thick thoracic trunks, which can obscure visualization of the T1 superior endplate on radiographs. As a result of this limitation, computed tomography (CT) and magnetic resonance imaging (MRI) have been utilized to measure T1 slope. 12 However, CT and MRI can be limited due to cost as well as accessibility. In addition, CT and MRI are performed in the supine position, which can change the biomechanics and alignment of the cervical spine. Cervical spine alignment parameters measured on supine MRI have been shown to differ significantly from those measured on upright radiographs. 13,14
To address these limitations, several authors have suggested using C7 slope as a proxy for T1 slope when the T1 superior endplate cannot be adequately visualized on radiographs. 15 -19 The purpose of this study was 2-fold. First, we aimed to assess the correlation between C7 slope and T1 slope on upright radiographs. Second, we evaluated the inter-rater reliability of measuring C7 slope.
Materials and Methods
Institutional review board approval was obtained for this study. Patients with lateral cervical spine radiographs taken between December 2017 and June 2018 at our institution were included in the study. When a patient had more than one lateral cervical spine radiograph within the study period, only the most recent radiograph was included for analysis. Patients with cervical instrumentation or unclear imaging were excluded. Patients with lateral cervical radiographs that did not have a clearly visible superior C7 endplate, inferior C7 endplate, and superior T1 endplate were excluded.
Lateral cervical radiographs were all taken in a standardized fashion at our institution with the patient sitting in a neutral weightbearing position. Two authors (IBY and RT) independently performed measurements on all included lateral cervical radiographs. Measured parameters included upper C7 slope, lower C7 slope, and T1 slope. Upper C7 slope was defined as the angle between the C7 superior endplate and a horizontal line. Lower C7 slope was defined as the angle between the C7 inferior endplate and a horizontal line. T1 slope was defined as the angle between the T1 superior endplate and a horizontal line. All radiographic measurements were performed using Centricity PACS (Picture Archiving and Communication System) system software (version 3.0, 8.0.1400.511).
The Pearson correlation coefficient was used to evaluate the strength of association between upper C7 slope and T1 slope, as well as between lower C7 slope and T1 slope. Simple linear regression analyses were performed to generate linear regression equations to predict T1 slope from either upper or lower C7 slope, respectively. We also assessed the interrater reliability of measurements of upper C7 slope, lower C7 slope, and T1 slope using the intraclass correlation coefficient (ICC) and a paired-sample t test. Statistical significance was set at the level of .05. The average measurement between the 2 authors (IBY and RT) was used for each parameter of interest in the statistical analysis. All statistical analyses were performed using SAS System version 9.4 (SAS Institute Inc, Cary, NC, USA).
Results
A total of 650 cervical spine radiographs taken between December 2017 and June 2018 at our institution were reviewed. The superior endplate of C7, inferior endplate of C7, and superior endplate of T1 were visible in 72.9%, 50.2%, and 31.2% of the 650 radiographs, respectively. Cervical instrumentation was present in 22.1% of radiographs and excluded. After applying our selection criteria, 152 patients were included in this study. The average age was 48.1 years, with 70.4% females and 29.6% males.
The average upper C7 slope, lower C7 slope, and T1 slope was 23.5° ± 9.1°, 22.9° ± 9.0°, and 27.5° ± 8.7°, respectively. There was a strong correlation between upper C7 slope and T1 slope (r = 0.91, P < .001), as well as between lower C7 slope and T1 slope (r = 0.90, P < .001). Linear regression modeling of the correlation between upper C7 slope and T1 slope yielded the following equation with an overall model fit of R 2 = 0.82 (Figure 1):
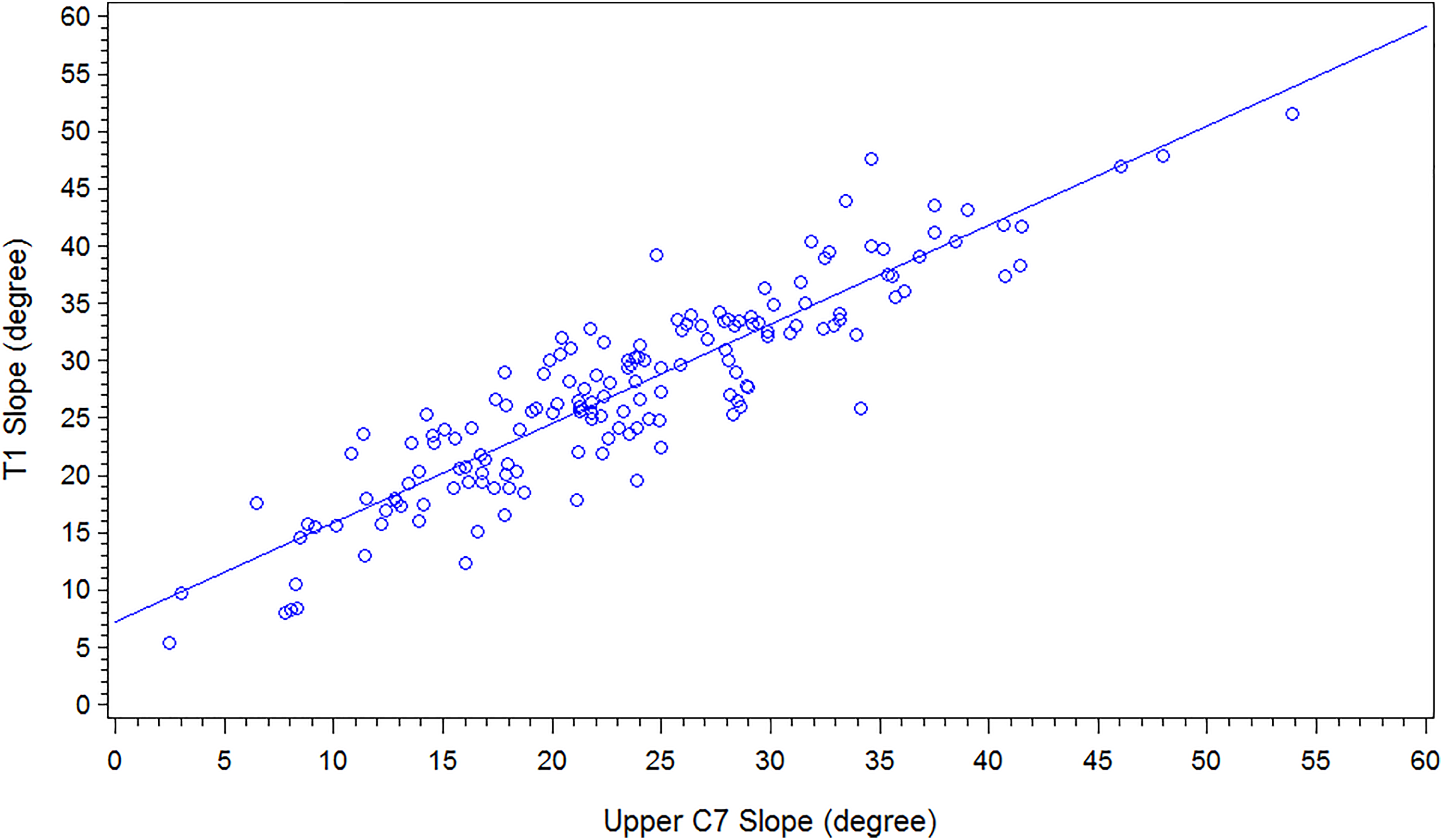
Correlation between upper C7 slope and T1 slope with a linear regression equation of “T1 slope” = 0.87 × “upper C7 slope” + 7.21 (R 2 = 0.82).

Similarly, linear regression modeling of the correlation between lower C7 slope and T1 slope yielded the following equation with an overall model fit of R 2 = 0.81 (Figure 2):
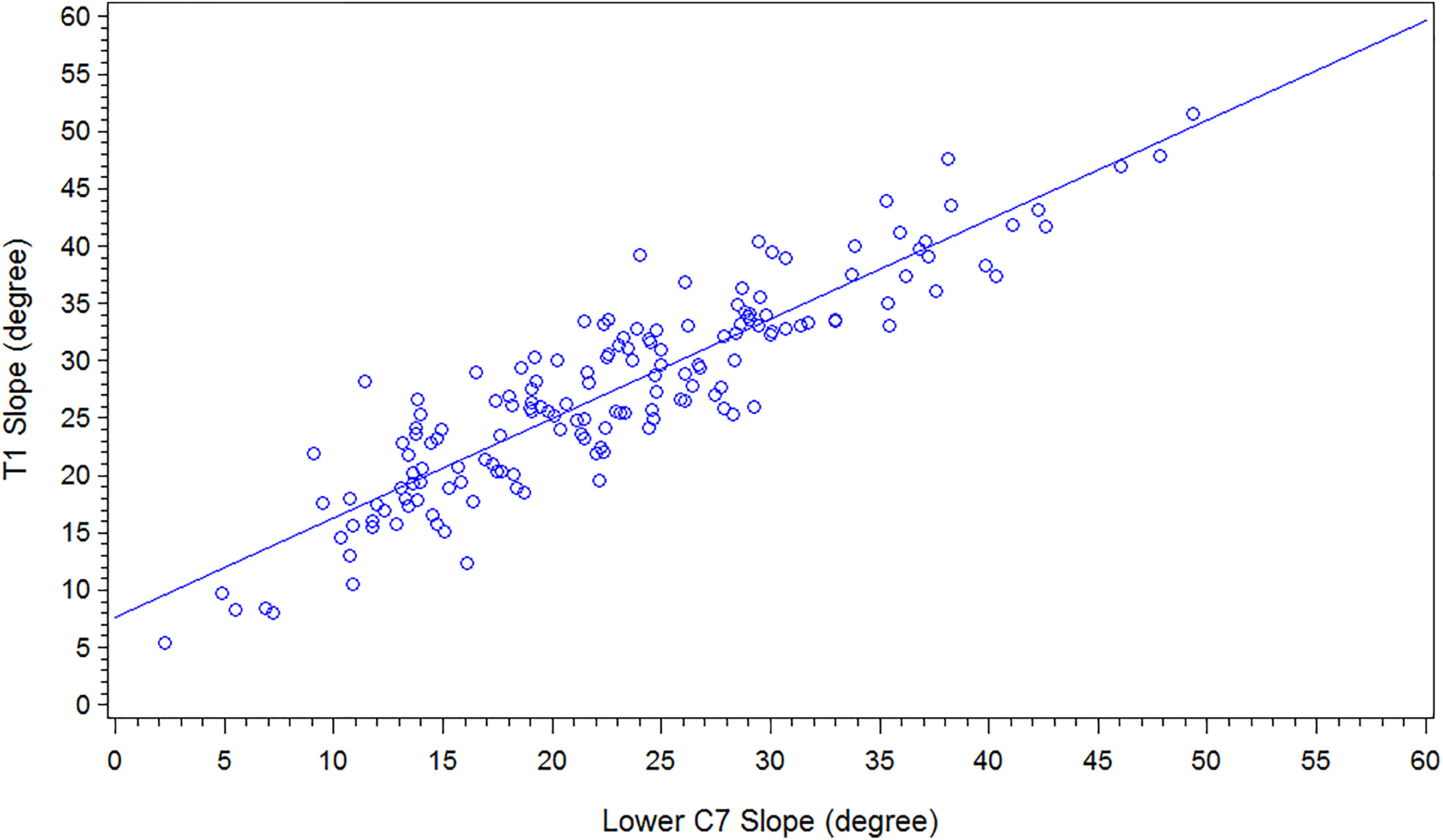
Correlation between lower C7 slope and T1 slope with a linear regression equation of “T1 slope” = 0.87 × “lower C7 slope” + 7.60 (R 2 = 0.81).

There was strong interrater reliability for upper C7 slope (ICC = 0.95, P < .001), lower C7 slope (ICC = 0.96, P < .001), and T1 slope (ICC = 0.89, P < .001).
Discussion
T1 slope is an important parameter for spinal sagittal balance. Unfortunately, the superior endplate of T1 is not always easily visualized on radiographs due to anatomical interferences from the shoulders and thoracic trunk. Therefore, in this study, we examined the correlation between C7 slope and T1 slope on standard lateral radiographs. Both upper C7 slope and lower C7 slope were found to be strongly correlated with T1 slope, suggesting that either parameter can be used as a proxy for T1 slope when the superior endplate of T1 is not adequately visualized.
Many factors influence overall sagittal balance of the spine, and the position of the occiput in relation to the sacrum is important. Cervical sagittal balance is affected by thoracic as well as global alignment. T1 slope has emerged as a parameter that may be useful in evaluating cervical sagittal balance. While standard lateral cervical spine radiographs can be used to measure T1 slope, anatomical interferences from the shoulders and thoracic trunk can hinder visibility of the T1 superior endplate, especially in obese patients. Attempts to modify shoulder or arm positioning in order to allow for better visualization of the T1 superior endplate may not be successful without violating the standardized positioning used for spinal radiographs. In this study, the superior endplate of T1 was only visualized in 31% of weightbearing sitting radiographs. However, this was actually a higher visualization rate than previously reported. Park et al 20 reported an 11% visualization rate of the T1 superior endplate in their series of cervical spine radiographs in 200 patients. The reduced visibility of the T1 superior endplate on standard radiographs is problematic as it precludes the use of T1 slope as a parameter in the assessment of spinal sagittal balance.
Given the proximity of C7 to T1, several studies have suggested the use of C7 slope as a potential substitute for T1 slope in the assessment of cervical sagittal balance. 17 -19 The more cephalad anatomical location of C7 makes it less susceptible to being obscured by the shoulders or thoracic trunk on lateral radiographs when patients are positioned in the standardized upright manner for radiographs. In this study, the endplates of C7 were indeed more easily visualized than the superior endplate of T1. The superior and inferior endplates of C7 were visible in 73% and 50% of radiographs, respectively, compared with only 31% for the superior endplate of T1.
We found a strong correlation between both upper and lower C7 slope with T1 slope in this study. In addition, there was good interrater reliability in measurements of upper and lower C7 slope, as well as T1 slope. These findings suggest that upper or lower C7 slope can be used as a proxy measurement for T1 slope when the superior endplate of T1 is not well visualized. The linear regression equation, “T1 slope” = 0.87 × “C7 slope” + 7, can be used to approximate T1 slope based on upper or lower C7 slope.
Our findings are consistent with prior studies. Tamai et al 16 found a similarly strong correlation between upper C7 slope and T1 slope with an R 2 of 0.82, as well between lower C7 slope and T1 slope with an R 2 of 0.84. However, it is important to note that their measurements were made using sitting weightbearing kinematic MRI images, rather than standard radiographs. Other studies have demonstrated a correlation between T1 slope and other cervical sagittal balance parameters as well, including C2-C7 SVA and C2-C7 Cobb angle using kinematic MRI and CT imaging. 20,21 However, these imaging modalities have limitations. CT imaging is obtained in the supine position, which can affect the biomechanics and alignment of the cervical spine. CT imaging also involves significantly higher radiation exposure compared to standard radiographs. 13,14 While kinematic MRI avoids both of these issues, it is not as readily available as standard supine MRI. In addition, CT and MRI are both advanced imaging modalities that incur significantly higher costs than plain radiographs. Therefore, the ability to assess C7 slope on radiographs as a substitute for T1 slope provides an easily accessible and cost-effective method for characterizing cervical sagittal balance.
T1 slope is an important parameter in assessing cervical sagittal balance. The cervicothoracic junction is a transitional region between the mobile, lordotic cervical spine and the rigid, kyphotic thoracic spine, which predisposes this region to potential instability. Knott et al 22 examined the utility of T1 slope in predicting overall sagittal balance of the spine in a retrospective analysis of radiographs. Their results demonstrated that a T1 slope >25° was associated with at least 10 cm of positive sagittal imbalance, whereas a T1 slope <13° was usually associated with negative sagittal balance. 22 Furthermore, T1 slope was found to be the parameter that was most strongly correlated with the SVA of the cervical spine from C2 to C7. 22 Another radiographic study by Diebo et al 23 demonstrated that T1 slope and cervical SVA significantly increased with increasing thoracolumbar SVA measured from C7 to S1. Higher T1 slope resulting from increased thoracic kyphosis led to greater cervical lordosis as a compensatory mechanism in order to maintain horizontal gaze. 23 In contrast, low T1 slope has been associated with a higher degree of degeneration in the cervical spine, and may be a potential risk factor for cervical spondylosis. 11
The relationship between T1 slope and surgical outcomes has also been studied in recent literature. T1 slope ≥40° has been associated with lower health-related quality-of-life measures in patients older than 50 years. 24 In contrast, Jeon et al 25 found no correlation between T1 slope and postoperative Neck Disability Index or visual analogue scale scores following anterior cervical discectomy and fusion (ACDF) involving 3 or more levels for cervical stenosis. High T1 slope has also been associated with negative radiographic outcomes following spinal surgery. Kim et al 26 found more kyphotic alignment changes following cervical laminoplasty for cervical myelopathy in patients with high T1 slope. 26 Oe et al 10 determined that T1 slope ≥40° was a risk factor for worsened cervical SVA at 2 years following adult spinal deformity surgery. T1 slope has therefore been shown to be an important parameter in cervical sagittal balance.
This study has several limitations. This was a purely radiographic study and we did not assess the correlation between C7 or T1 slope and clinical measures. In addition, we did not differentiate between patients with cervical spine disorders and those without. Future studies should examine the relationship between C7 or T1 slope and clinical outcomes in patients with and without cervical spine disorders in order to further elucidate the role of C7 or T1 slope in cervical sagittal balance. We also did not include patients who had undergone cervical instrumentation—that is, we excluded a certain proportion of patients who had undergone prior cervical spine surgery. It would be of interest in future studies to examine the visibility of C7 or T1 slope on radiographs in patients with cervical instrumentation, as this may limit the utility of C7 or T1 slope in assessing postoperative cervical sagittal balance.
Conclusions
T1 slope is an important parameter in the assessment of both cervical and global spinal sagittal balance. Unfortunately, the superior endplate of T1 is sometimes obscured on standard lateral radiographs due to the overlying anatomical structures, including the shoulders and thoracic trunk. While advanced imaging such as CT or MRI can provide clear visualization of the superior endplate of T1, these advanced imaging techniques are most commonly performed in the supine position and also incur significant costs. In this retrospective study of 152 patients, we found that both the upper and lower C7 slope are strongly correlated with T1 slope. We found that the regression equation, “T1 slope” = 0.87 × “C7 slope” + 7, can be used to predict T1 slope from either the measured upper or lower C7 slope on a standard radiograph. Furthermore, there was good interrater reliability for upper C7 slope, lower C7 slope, and T1 slope. Therefore, when the superior endplate of T1 is not visualized on standard radiographs, the upper or lower C7 slope can be used as a proxy measurement in the assessment of sagittal balance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.