
Abstract
Study Design:
Retrospective single-center study.
Objectives:
K-line is a decision-making tool to determine the appropriate surgical procedures for patients with cervical ossification of the posterior longitudinal ligament (C-OPLL). Laminoplasty (LAMP) is one of the standard surgical procedures indicated on the basis of K-line measurements (+: OPLL does not cross the K-line). We investigated the impact of K-line tilt, a radiographic parameter of cervical sagittal balance measured using the K-line, on surgical outcomes after LAMP.
Methods:
The study included 62 consecutive patients with K-line (+) C-OPLL who underwent LAMP. The following preoperative and postoperative radiographic measurements were evaluated: (1) the K-line, (2) K-line tilt (an angle between the K-line and vertical line), (3) center of gravity of the head –C7 sagittal vertical axis, (4) C2–C7 lordotic angle, (5) C7 slope, and (6) C2–C7 range of motion. Clinical results were evaluated using the Japanese Orthopedic Association scoring system for cervical myelopathy (C-JOA score).
Results:
All the patients had non-kyphotic cervical alignment (CL ≥ 0°) preoperatively; however, kyphotic deformity (CL < 0°) was observed in 6 patients (9.7%) postoperatively. The recovery rate of the C-JOA scores was poor in the kyphotic deformity (+) group (7.8%) than in the kyphotic deformity (−) group (47.5%). The K-line tilt was identified to be a preoperative risk factor in the multivariate analysis, and the cutoff K-line tilt for predicting the postoperative kyphotic deformity was 20°.
Conclusions:
LAMP is not suitable for K-line (+) C-OPLL patients with K-line tilts >20°.
Keywords
Introduction
Cervical laminoplasty (LAMP) is one of the standard surgical procedure in patients with cervical myelopathy caused by ossification of the posterior longitudinal ligament (C-OPLL).1-3 However, LAMP is well known to be unsuitable for patients with massive ossification of the posterior longitudinal ligament (OPLL) lesions or preoperative cervical kyphotic alignments.4-6 In addition, one of the important complications after LAMP is postoperative kyphotic deformity, which prevents posterior spinal cord shift and leads to postoperative anterior compression of the spinal cord.7,8
The K-line, which connects the midpoints of the spinal canal at C2 and C7 on neutral lateral radiography, is a simple and effective indicator for predicting incomplete indirect decompression in patients with OPLL. The K-line can evaluate the OPLL size and cervical alignment in 1 parameter. 9 Neurological recovery after LAMP is reported to be poor if the OPLL crosses the K-line (K-line (−)). We can estimate neural decompression immediately after surgery using the K-line, but the K-line cannot predict the postoperative kyphotic change after LAMP.
Previously, we reported that preoperative cervical sagittal imbalance is a predictive factor of postoperative kyphotic deformity and poor neurological recovery after LAMP.10,11 To establish a more useful and appropriate predictor of clinical outcomes in addition to the conventional K-line, we focused on K-line tilt,12-14 which can be used to evaluate cervical sagittal balance using the K-line. In this study, we investigated the effect of K-line tilt on the radiological and clinical outcomes after LAMP in patients with C-OPLL.
Materials and Methods
Ethics and Patient Consent
The study was conducted with the approval of our institutional review board (approval No. 2921, ethics committee of the Saiseikai Kawaguchi General Hospital). All the patients provided written informed consent to participate in this study.
Materials
A total of 69 consecutive patients who underwent LAMP for K-line (+) C-OPLL at our hospital between 2008 and 2016 were enrolled in this study. Patients with myelopathy caused by cervical disc herniation or spondylosis, K-line (−) C-OPLL, and a history of previous cervical surgery or spinal cord injury and those who could not maintain an upright position without assistance were excluded.
Operative Procedure
Double-door LAMP was performed as described by Miyazaki and Kirita. 15 The paravertebral muscles were detached from the spinous processes on both sides, and the processes at C3–C6 were removed. The laminae at C3–C6 were split at the midline, and bilateral gutters were made using a high-speed air-burr drill (Figure 1A). The bilateral laminae were kept open by anchor sutures to the capsule of the facet joint (Figure 1B). In the patients who had spinal cord compression at the C2/C3 level, the inferior part of the C2 lamina was fenestrated. In the patients who had spinal cord compression at the C6/C7 level, the upper part of the C7 lamina was fenestrated. When segments C2–C7 were operated on, fenestration of the inferior part of the C2 lamina, upper part of the C7 lamina, and C3–C6 laminoplasty were performed. All the patients had preserved C2 and C7 spinous processes and paravertebral muscle, which touched these spinous processes.
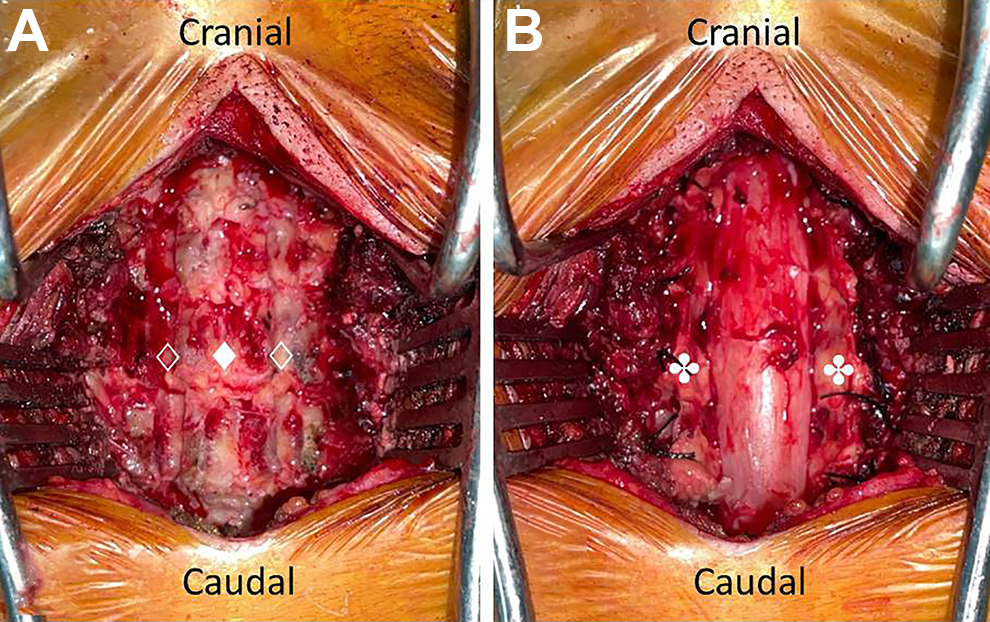
Double-door laminoplasty. The laminae are split at the midline (♦), and bilateral gutters (⟡) are made using a high-speed air-burr drill (A). The bilateral laminae were kept open by anchor sutures to the capsule of the facet joint (✤) (B).
Outcome Measures
The K-line tilt was defined as an angle between the K-line, which connects the midpoints of the spinal canal at C2 and C7, and a vertical line (Figure 2).12-14 Cervical lateral radiography images were evaluated preoperatively and at the final follow-up visit. Radiographic measurements included the following: (1) K-line, (2) K-line tilt, (3) center of gravity of the head (CGH) –C7 sagittal vertical axis (SVA), 16 (4) C2–C7 lordotic angle (CL), and (5) C7 slope in the neutral position while standing in the relaxed head position with forward gaze, and (6) C2–C7 range of motion (ROM) in the flexion and extension positions. The radiographic tube was centered on C4, and the radiographic film cassette was 150 cm from the tube. The clinical results were evaluated using the Japanese Orthopedic Association scoring system for cervical myelopathy (C-JOA score) and the recovery rate of the C-JOA score, which is calculated using Hirabayashi’s method. 17
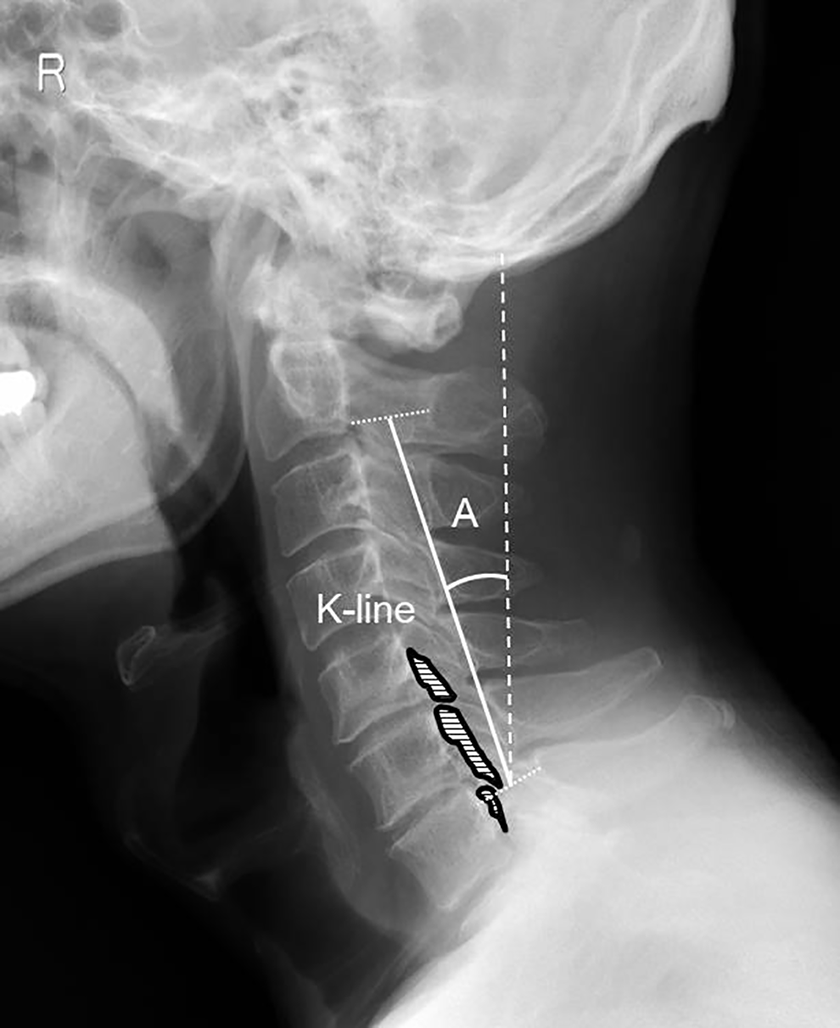
K-line tilt (A). This is an angle between the K-line, which connects the midpoints of the spinal canal at C2 and C7, and the vertical line.
Statistical Analyses
Statistical analyses were performed using SPSS version 24 for Windows (SPSS Institute, Chicago, IL). Univariate statistical analyses were performed using the Mann-Whitney U test or χ2 test. The Pearson correlation coefficient was used to investigate correlation analyses. Risk factor analysis was performed using multivariate logistic regression with a forward stepwise procedure (P < 0.1 for entry). The sensitivity, specificity, and receiver-operating characteristic curve were measured to evaluate the valuable indexes for predicting postoperative kyphotic deformity. A statistically significant difference was set at a P-value <0.05.
Results
Patient Demographics
Of the 69 patients, 62 (89.6%, 44 men and 18 women) completed the 1-year follow-up, and complete data was obtained. Data of the 62 patients was analyzed. The mean follow-up period was 4.5 years. The patients’ demographic data is shown in Table 1. The OPLL was classified as a continuous type in 8 patients, segmental type in 27 patients, and mixed type in 27 patients. The mean canal narrowing ratio of OPLL (CNR) was 35.9%, and the mean preoperative C-JOA score was 10.7 points. The operative segments were C2–C6 in 4 patients, C2–C7 in 12 patients, C3–C6 in 9 patients, and C3–C7 in 37 patients.
Demographic Data of Patients.
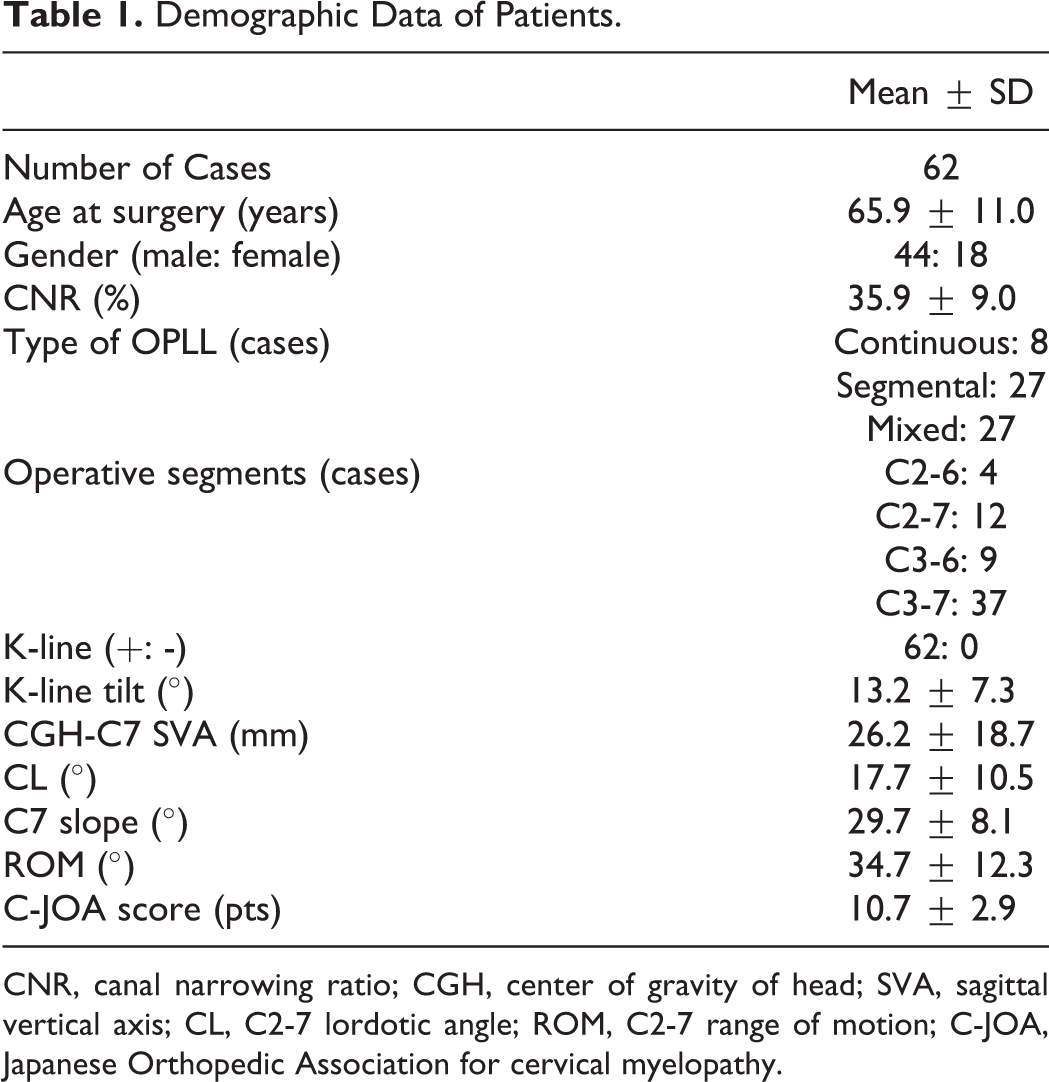
CNR, canal narrowing ratio; CGH, center of gravity of head; SVA, sagittal vertical axis; CL, C2-7 lordotic angle; ROM, C2-7 range of motion; C-JOA, Japanese Orthopedic Association for cervical myelopathy.
Kyphotic Deformity after LAMP
Before operation, all the 62 patients had a non-kyphotic cervical alignment (CL ≥0°); however, a postoperative kyphotic deformity (CL < 0°) was observed in 6 patients (9.7%), and 4 (6.5%) of these patients had changed from K-line (+) to K-line (−) at the final follow-up. We compared the preoperative factors between the kyphotic deformity (+) group (6 cases) and the kyphotic deformity (−) group (56 cases; Table 2). The age, sex, CNR, type of OPLL, number of operative segments, preoperative CL, C7 slope, and ROM were similar between the 2 groups; however, the preoperative K-line tilt, CGH-C7 SVA, and C7 slope were significantly larger in the kyphotic deformity (+) group than in the kyphotic deformity (−) group (P = 0.000, P = 0.000, and P = 0.045, respectively). Although the preoperative C-JOA scores were similar between the 2 groups, the postoperative C-JOA scores in the kyphotic deformity (+) group were inferior to those of the kyphotic deformity (−) group (P = 0.037). The recovery rate of the C-JOA score was inferior in the kyphotic deformity (+) (7.8%) group as compared with the kyphotic deformity (−) group (47.5%; P = 0.026).
Preoperative Factors and Clinical Outcomes in the Kyphotic Deformity (+) and the (-) Groups.
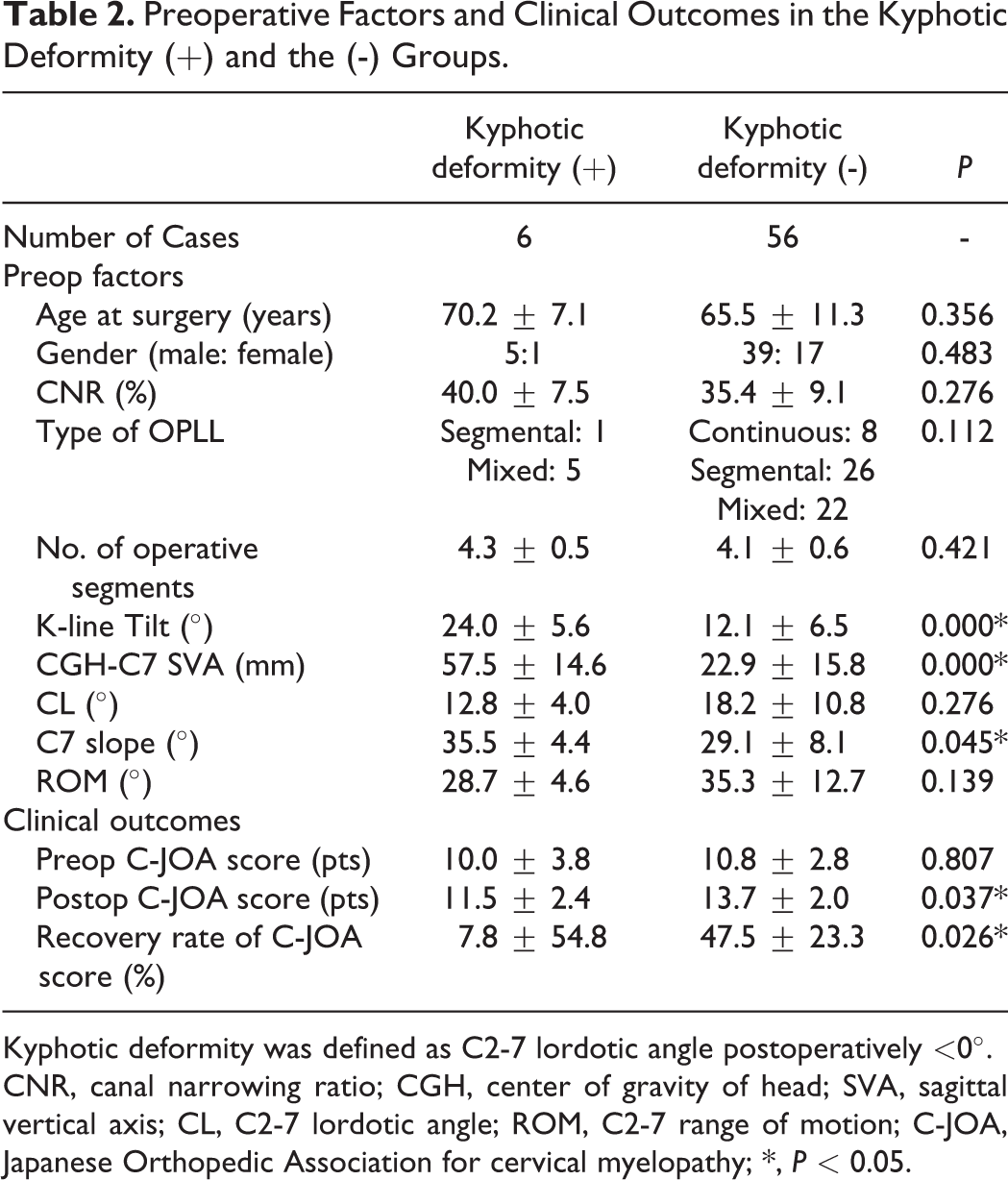
Kyphotic deformity was defined as C2-7 lordotic angle postoperatively <0°.
CNR, canal narrowing ratio; CGH, center of gravity of head; SVA, sagittal vertical axis; CL, C2-7 lordotic angle; ROM, C2-7 range of motion; C-JOA, Japanese Orthopedic Association for cervical myelopathy; *, P < 0.05.
Correlation between K-line Tilt and CGH-C7 SVA
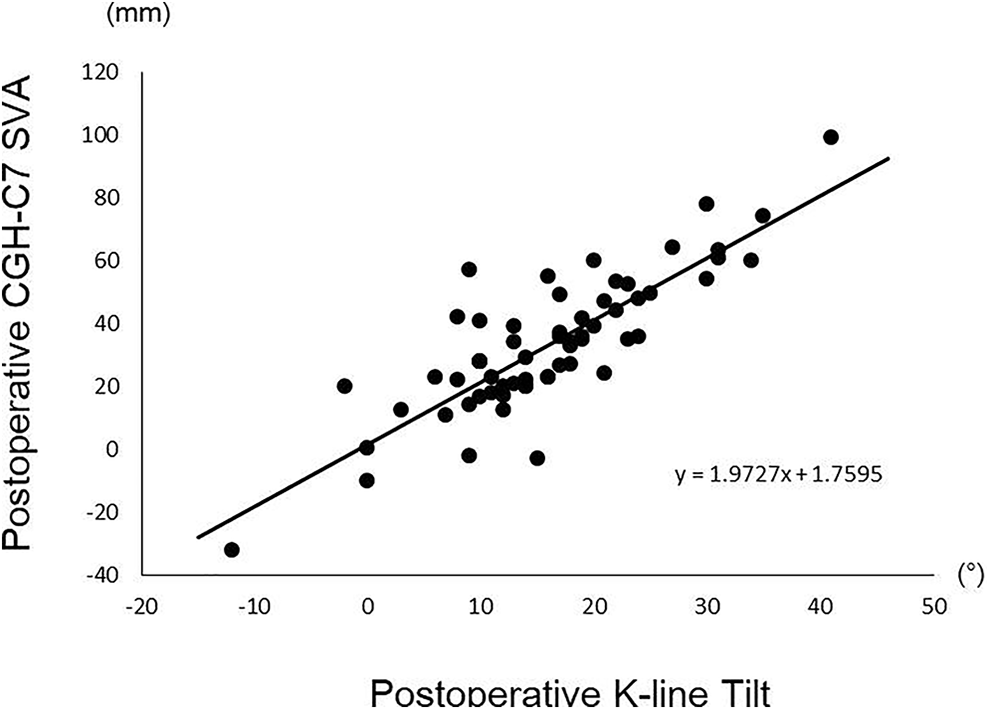
To investigate whether the K-line tilt is used as cervical sagittal balance instead of the CGH-C7 SVA, we analyzed correlations between the K-line tilt and the CGH-C7 SVA (Table 3). The K-line tilt strongly correlated with the CGH-C7 SVA preoperatively (R = 0.851, P = 0.000; Figure 3) and postoperatively (R = 0.837, P = 0.000; Figure 4).
Correlations Between K-Line Tilt and CGH-C7 SVA.
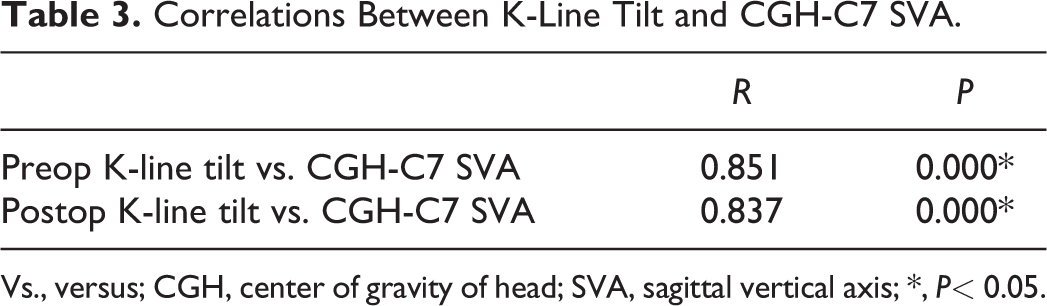
Vs., versus; CGH, center of gravity of head; SVA, sagittal vertical axis; *, P< 0.05.
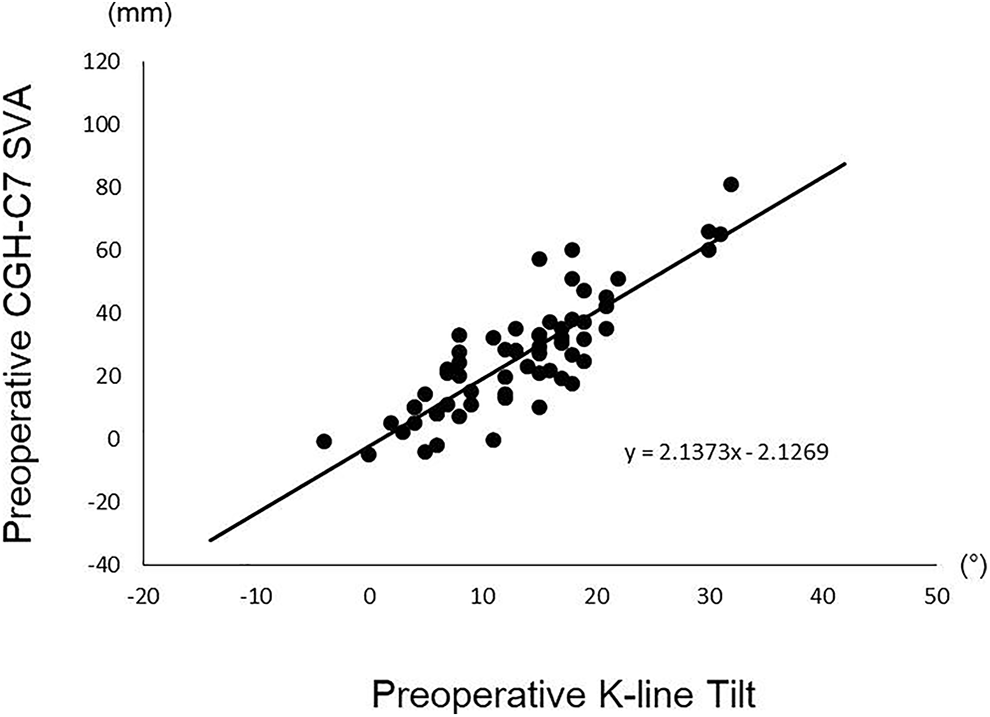
Correlation between preoperative K-line tilt and CGH-C7 SVA.
Correlation between preoperative K-line tilt and CGH-C7 SVA.
Preoperative Risk Factors of Postoperative Kyphotic Deformity
By forward stepwise logistic regression analysis using the K-line tilt as an indicator of cervical sagittal balance instead of the CGH-C7 SVA, the preoperative K-line tilt (odds ratio, 1.320; 95% confidence interval, 1.110–1.584, P = 0.003) was a crucial preoperative risk factor of the occurrence of postoperative kyphotic deformity after LAMP (Table 4). Moreover, the receiver-operating characteristic curve analysis yielded an area under the curve of 0.951 (95% confidence interval, 0.892–1.000; P = 0.001), and a cutoff K-line tilt of 20° was associated with 83.3% sensitivity and 94.6% specificity for predicting postoperative kyphotic deformity. The probability in each patient was calculated using the following equation: P = exp Z/(1 − exp Z) (Z = −7.179 + 0.278X: X = preoperative K-line tilt (°)).
Preoperative Risk Factors of the Kyphotic Deformity.
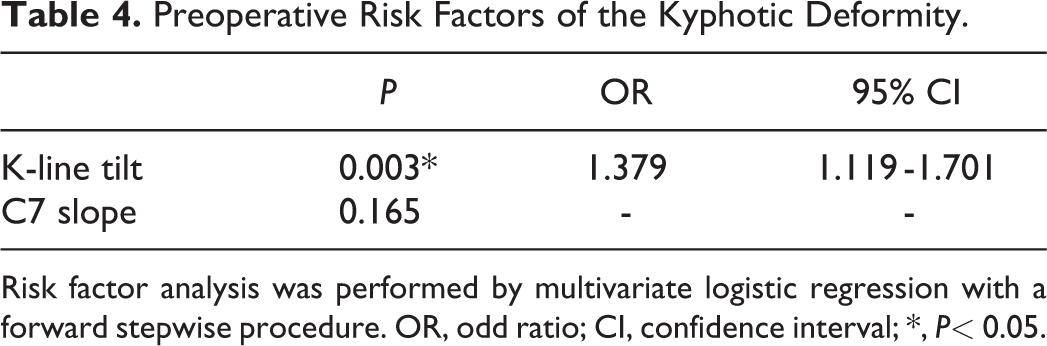
Risk factor analysis was performed by multivariate logistic regression with a forward stepwise procedure. OR, odd ratio; CI, confidence interval; *, P< 0.05.
Case Presentation
A 70-year-old man (Figure 5) had a combined type of OPLL (CNR, 46%) and lordotic cervical alignment (CL, 11°). The patient was K-line (+) but had a large K-line tilt of 30°. The preoperative C-JOA score was 14.5. After LAMP, the spinal cord was decompressed, and the neurological symptom temporarily recovered. However, myelopathy worsened at 10 months postoperatively. The radiological images at the 3-year follow-up period showed kyphotic deformity (CL, −11°) and K-line (+) changed to K-line (−). The C-JOA score decreased to 12.0 at the 3-year follow-up period.
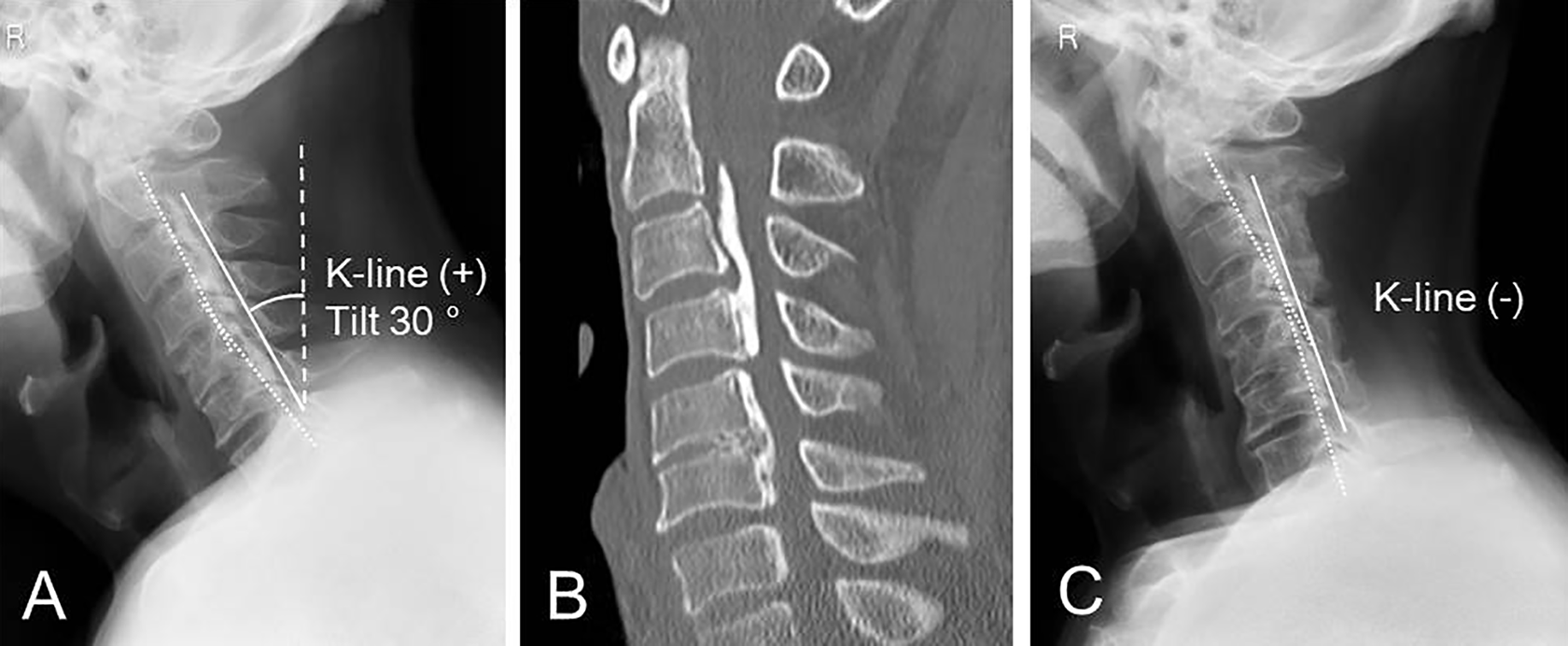
Preoperative radiography (A) and computed tomography images (B) of a 70-year-old male patient. He had a combined type of OPLL and cervical lordotic alignment (K-line (+)) with cervical sagittal imbalance (K-line tilt: 30°). The radiography image (C) at 3-year follow-up after LAMP showed a postoperative kyphotic deformity and change in the K-line (−).
Discussion
LAMP is a standard surgical procedure for OPLL and provides a good surgical result in the long term.1-3 Various authors reported that neurological recovery after LAMP was poor in cases with massive OPLL or preoperative kyphotic cervical alignment as compared with those with anterior decompression with fusion (ADF) or posterior decompression with fusion (PDF).4-6,18 Therefore, proper assessments of cervical spine alignment and OPLL size preoperatively are important when selecting the surgical procedures. The K-line proposed by Fujiyoshi et al. is a good clinical tool in determining the surgical procedure for patients with C-OPLL, and ADF or PDF is recommended for patients with K-line (−).9,18 The K-line is an extremely simple and visual indicator, which allows the evaluation of OPLL size and cervical spine alignment with a single parameter. We also used this parameter for choosing surgical procedures and performed LAMP only for K-line (+) cases.
Postoperative kyphotic deformity is one of the most important complications of LAMP, resulting in the failure of indirect decompression via posterior spinal shift, with a reported frequency of 6%–35%.2,7,8 The K-line can predict the effectiveness of neural decompression after LAMP but cannot predict postoperative kyphotic deformity. Indeed, postoperative kyphotic deformity developed in 9.7% of our patients, and importantly, their neurological recovery was poor. Clinical outcomes after LAMP have been reported to be poor when kyphosis develops postoperatively.8,19,20 Our study also highlights the importance of alignment change after LAMP by showing that postoperative kyphosis caused increased anterior spinal cord compression by OPLL and subsequently caused poor neurological recovery.
We previously reported that preoperative cervical sagittal imbalance based on large cervical SVA was a risk factor of kyphotic deformity after LAMP. 10 In fact, LAMP has been reported to have worse surgical outcomes than ADF and PDF in patients with high cervical SVA.11,21 In a state of cervical sagittal imbalance, patients have a large cervical lordosis due to compensatory mechanisms for forward gaze, which increases the strain on the cervical extensor muscles.22,23 In these conditions, invasion in the posterior extension mechanism of LAMP is speculated to cause a postoperative kyphotic deformity. Kim et al. proposed a similar mechanism of kyphotic deformity after LAMP. They reported that high T1 slope is a risk factor of postoperative kyphotic deformity because of increased strain on the extensor muscles. 24 K-line tilt is a new cervical sagittal plane balance parameter that has received much attention. Other researchers also reported that K-line tilt correlates with the C2-7 SVA and is an alternative to the classic cervical SVA.13,14 In fact, in our study, K-line tilt strongly correlated with the CGH-C7 SVA, and large K-line tilt (>20°) was found to be a risk factor of postoperative kyphotic deformity.
Both cervical SVA and K-line tilt can be used to evaluate cervical sagittal balance. However, K-line tilt is considered a simpler and more useful parameter to visually recognize sagittal balance. Simultaneously, it can also be used for the original purpose (judging as (+) or (−)) of selecting surgical procedures for patients with C-OPLL. In addition, K-line tilt is not affected by the magnification of the radiographic image because it is an angular parameter, but SVA is affected by it because it is a length parameter. From the results of our study, ADF or PDF should be considered rather than LAMP not only for patients with K-line (−) but also for those with K-line (+) with K-line tilts >20°.
This study has the following limitations: 1) this was a retrospective study; 2) the number of patients included was relatively small; 3) thoracolumbar or spinopelvic parameters were not assessed; and 4) patient-reported outcome was not evaluated. Further studies that include whole-spine parameters with larger samples sizes would be needed in the future. Nonetheless, to our knowledge, this is the first study to demonstrate the effectiveness of using K-line tilt to predict radiological and clinical outcomes after LAMP. The results of this study could help surgeons make a more appropriate choice of surgical procedures for patients with C-OPLL.
Conclusion
A K-line tilt >20° is a predictor of kyphotic deformity after LAMP for patients with K-line (+) C-OPLL, and LAMP is not suitable for these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Japanese Health Labour Sciences Research Grant (grant No. 040).