
Abstract
Study Design
This was a retrospective cohort radiographic study.
Objective
To determine the age- and gender-related normative values and correlation of cervical sagittal parameters in asymptomatic Chinese adults, and to explore the changes and compensating mechanisms across different age groups.
Methods
The asymptomatic subjects were divided into 6 groups according to age and then one-way analysis of variance was used to compare the multiple sets of cervical sagittal parameters among the different age groups. Independent t-tests were performed to compare the sagittal parameters among different gender and different cervical spine alignments. Relationships between each parameter were tested by Pearson’s correlation. Linear regression analysis based on T1 slope (T1S) and C2 slope (C2S) was used to provide an equation to predict normal cervical alignment.
Results
Mean values of each cervical sagittal parameter were presented based on age and gender. There were positive correlations between age and cervical lordosis (CL) (r = -.278, P < .001), T1S (r = .271, P < .001), cervical sagittal vertical axis (cSVA) (r = .218, P < .001), C2-C4 Cobb angle (r = -.283, P < .001), horacic inlet angle (TIA) (r = .443, P < .001), and neck tilt (NT) (r = .354, P < .001). Older groups (aged >50 years) had greater T1 Slope, C2S, and TIA. The C2-C4 Cobb angle maintained a steadily increasing trend and significantly increased in the older adult groups (P < .05), while the C5-C7 Cobb angle was relatively constant. Mean values of parameters were larger in males (P > .05). Linear regression analysis indicated a strong association between T1S and CL (R2 = .551, standard error 1.16°), T1S and C5-7 (R2 = .372; P < .001), and C2S and C2-4 (R2 = .309; P < .001).
Conclusions
Normative values of cervical sagittal parameters vary by age and sex. The CL, cSVA, and T1S, C2-4 Cobb angle changed with increasing age, and it can influence the recruitment of compensation mechanism. Normative CL of Chinese adults was predicted by the equation CL = T1S-14.7° ± 1.2°, which could serve as a reference when planning for cervical surgery.
Introduction
Generally, cervical sagittal alignment (CSA) and cervical sagittal balance (CSB) play a critical role in the maintenance of neutral head posture, horizontal gaze, and other physiological functions.1,2 Since cervical sagittal parameters are important indicators of cervical malalignment, these criteria are closely related to quality-of-life scores and were of high importance for assessment and evaluation of cervical alignment and surgical decisions.3,4 Indeed, imbalance of cervical spine alignment is known to cause neck pain and disability, which would negatively impact quality-of-life scores. Much also has been written on the relationship between the clinical and radiographic outcomes of cervical spinal surgery and the reconstruction of cervical sagittal balance and restoration of cervical alignment.5,6 For patients requiring cervical surgical treatment with implants and fusion, restoration of the normal sagittal balance and well alignment is important.7-9 Without suitable reference data of cervical sagittal parameters and the lack of ideal cervical lordosis (CL), predicted models make cervical malalignment procedures difficult and less accurate, leading to either residual malalignment or acquired iatrogenic deformity. Furthermore, surgeons may not have a clear target on cervical procedures and only aim to decompress and restore cervical lordosis and cSVA.
One of the pivotal goals for surgical treatment of cervical disorders is the personalized optimization of preoperative sagittal realignment strategy with reference to the normative values matched by age and gender of specific ethnic groups. 10 Previous studies have defined normative values of some cervical sagittal parameters of Western asymptomatic adults.11-13 It has been indicated that cSVA should be less than 40 mm, C2S should be less than 20°, and an ideal normative value of T1S-CL should be 17°; in contrast, a T1S-CL greater than 17° may imply a cervical kyphosis. 13
Prior studies indicated that spinal sagittal parameters of subjects with different ethnic backgrounds, age, gender, and races present differently. Consistent with this, a previous study of our research team found that the parameters of CSA and range of motion were affected by age, sex, and degeneration. 14 However, the normative values of parameters of the cervical sagittal spine of Chinese adults have not been reported in the literature. Thus, the main purpose of this study was to determine the age- and the sex-related normative values of cervical sagittal parameters in asymptomatic Chinese adults and to explore the changes and compensating mechanisms across different age groups.
Materials and Methods
This study was approved by the institutional review boards of Peking University People’s Hospital and was a retrospective cross-sectional study of healthy physical examination individuals who had cervical spine X-rays film taken at our hospital between January 2016 and January 2020. Asymptomatic adults aged 20-90 years with no neck or back pain were included. Standard neutral lateral cervical spine radiographs were taken in a neutral weight-bearing position. 14 Subjects were excluded if they met any of the following criteria: (1) congenital or secondary cervical fusion; (2) spinal deformity; (3) the T1 superior endplate was not clearly visible on X-rays; (4) a history of spinal surgery or spinal trauma, deformity, tumor; or (5) other spinal diseases, such as ankylosing spondylitis. 15
Patient demographics collected included age and sex. Radiographic parameters measured included: C2 slope (C2S), C1-C2 Cobb angle, C2-C7 Cobb angle (CL), C2-C4 Cobb angle, C5-C7 Cobb angle, cervical sagittal vertical axis (cSVA), T1 slope (T1S), thoracic inlet angle (TIA), neck tilt (NT), and T1S minus CL (T1S-CL) (Figure 1). These parameters were measured twice by 2 authors independently using a picture archiving and communication system (PACS) and the average score was used in analyses. The intraclass correlation coefficient (ICC) was calculated to evaluate intra- and inter-observer variability. For all of the Cobb parameters, we set the lordosis angle as negative values and kyphosis angle as positive values. Cervcial sagittal radiograph with representative measurements. (CL: cervical lordosis (C2-C7 Cobb angle), C2S: C2 Slope, cSVA: cervical sagittal vertical axis, T1S: T1 slope, TIA:thoracic inlet angle).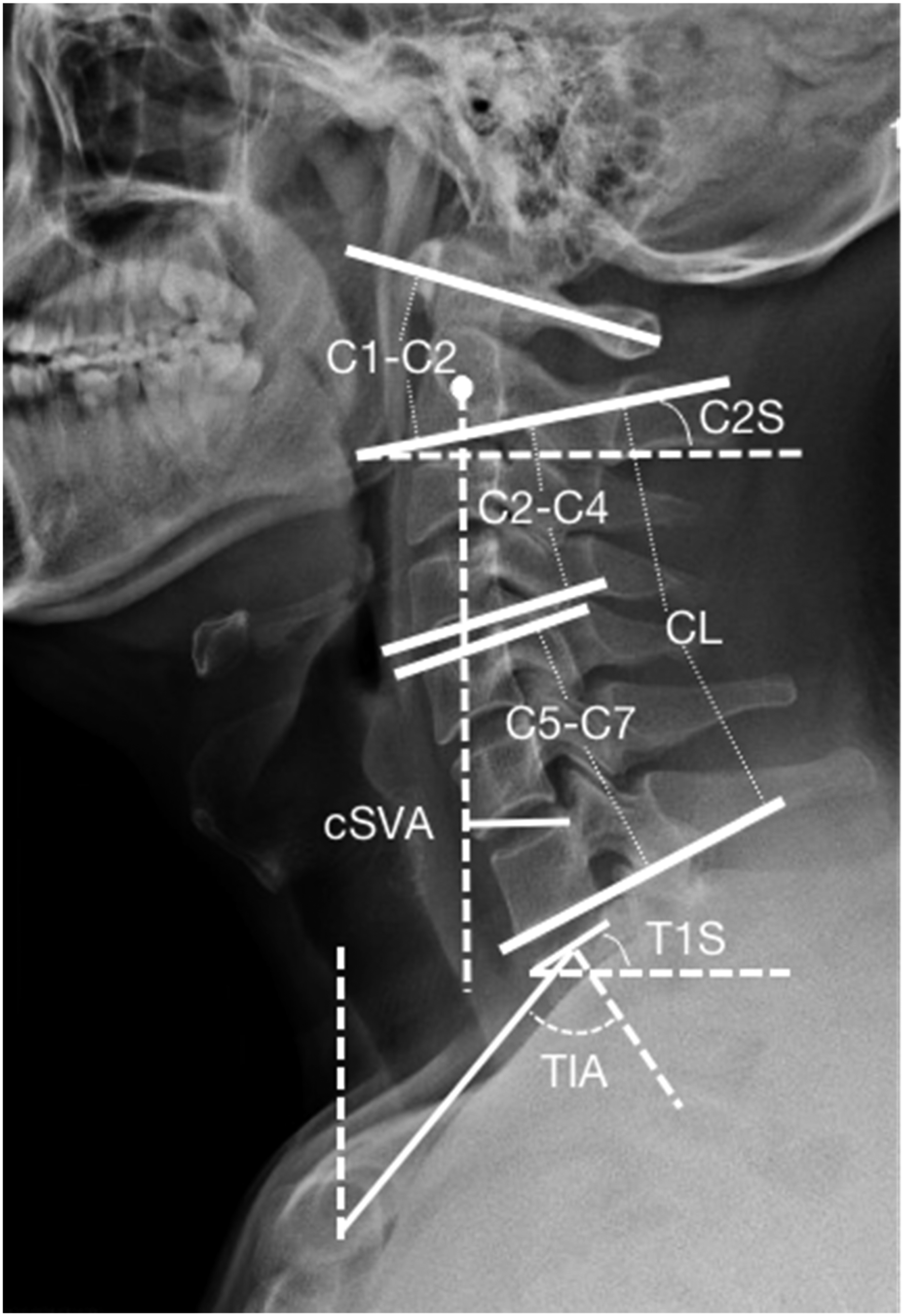
The subjects were divided into 6 different age groups (Group I: 20-29 years, Group II: 30-39 years, Group III: 40-49 years, Group IV: 50-59 years, Group V: 60-69 years, Group VI: >70 years) for analysis and to determine the trend in cervical sagittal alignment with increasing age. In addition, subjects were subdivided into males and females. All of the subjects were also subdivided into the lordosis group (CL <0°) or the kyphosis group (CL >0°).
Statistical Analysis
Data were expressed as mean values ± SD. Statistical analyses were performed using SPSS version 21 (SPSS, Chicago, IL). The one-way analysis of variance (ANOVA) statistical method was used to compare the multiple sets of cervical sagittal parameters among different age groups. The association between each parameter was assessed by the Pearson’s correlation and a linear regression analysis. Differences in the parameters between subgroups were examined with the Student’s t-test. Statistical significance was set at P < .05.
Results
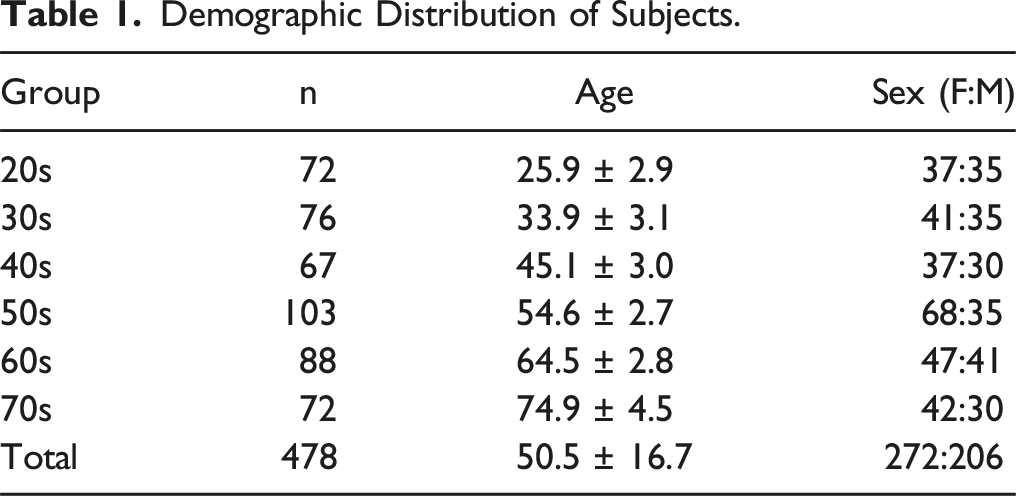
Demographic Distribution of Subjects.
Cervical Sagittal Parameters
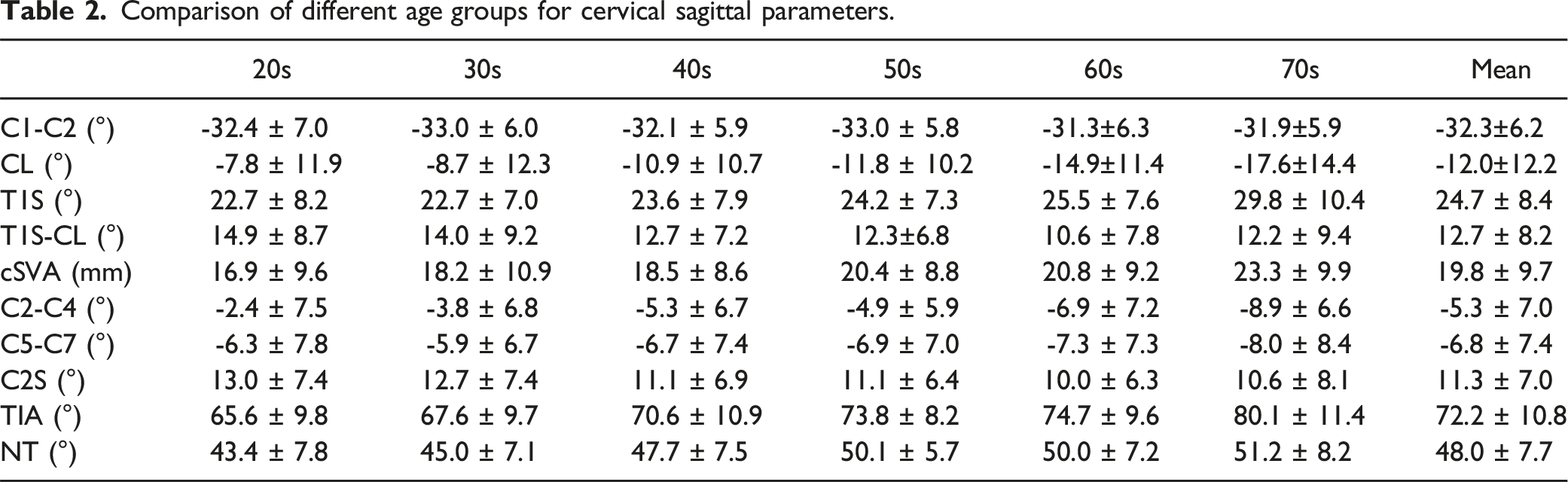
Comparison of different age groups for cervical sagittal parameters.
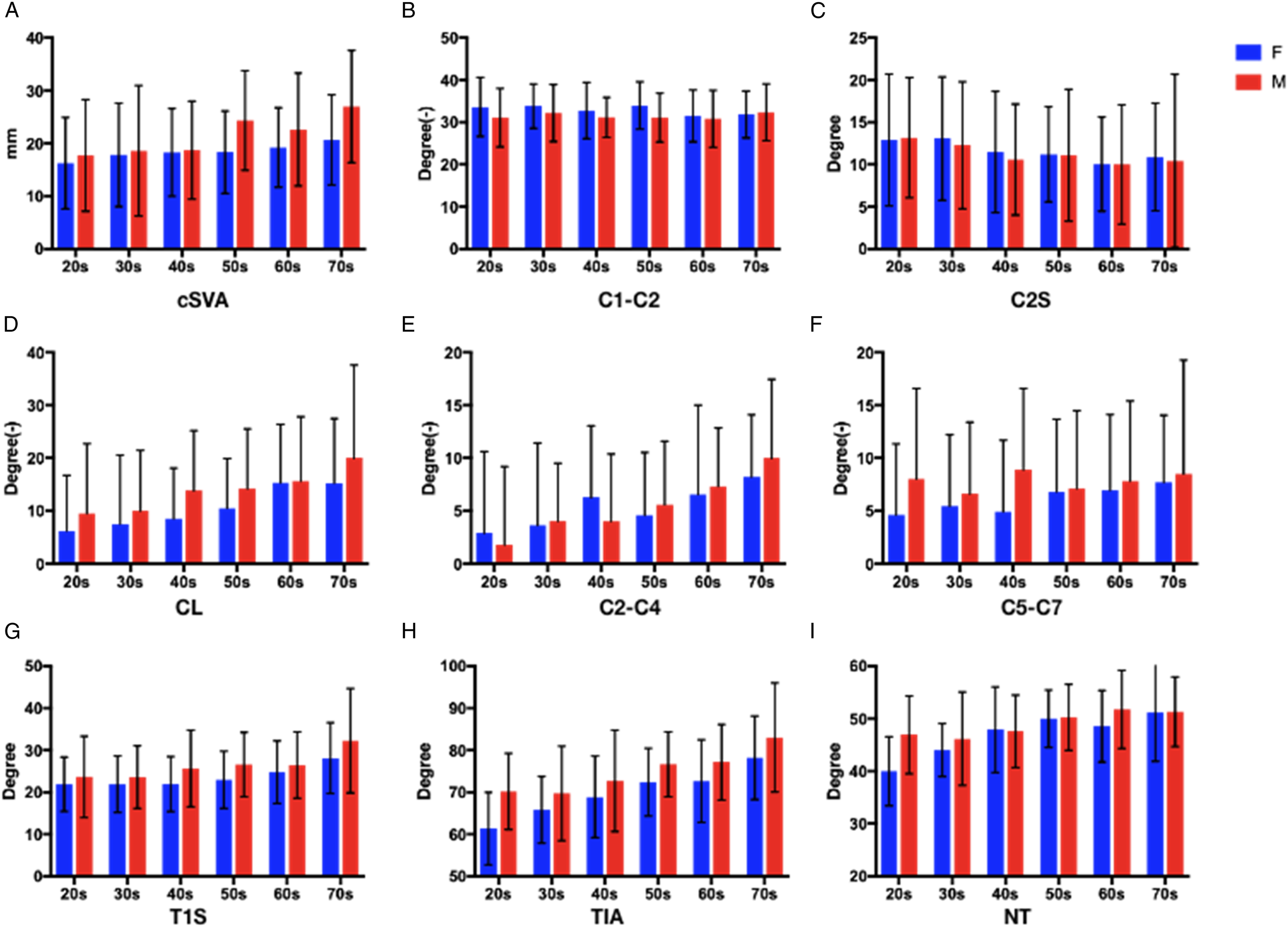
Changes in cervcial sagittal alignment parameters with age in male (M) and female (F).
Comparison of Young and Older Adult Groups.
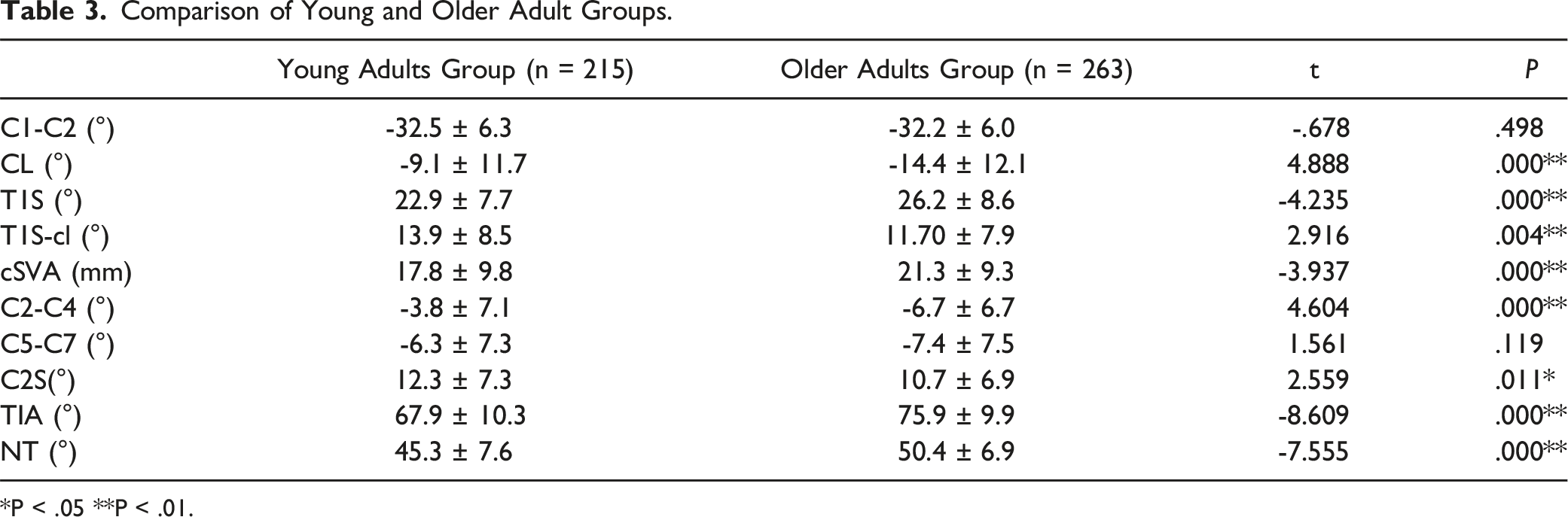
*P < .05 **P < .01.
Comparison of Lordosis and Kyphosis Groups.
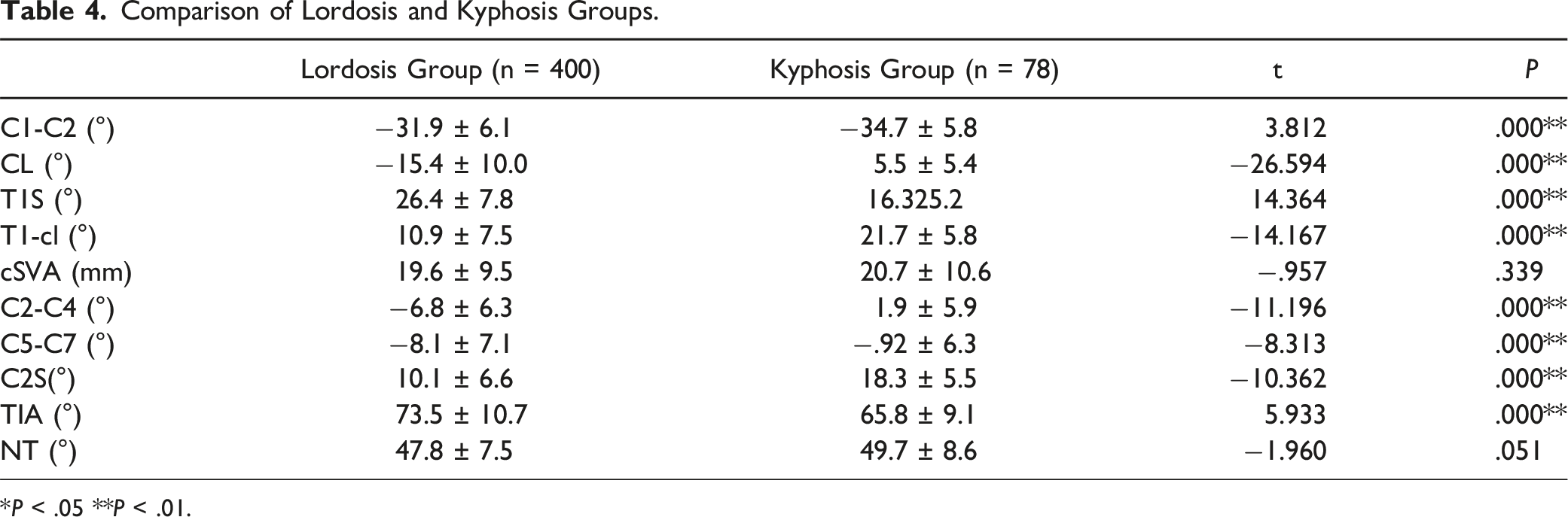
*P < .05 **P < .01.
Correlation Analysis and Linear Regression Analysis
Person Correlation Between Parameters.
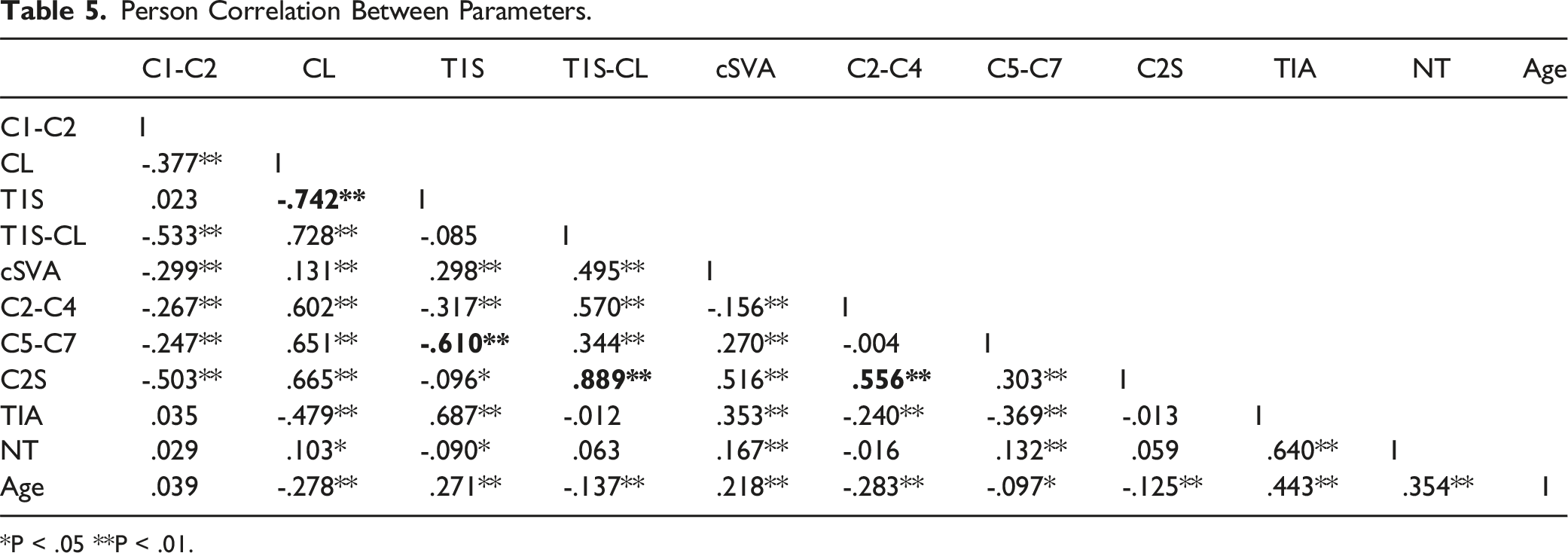
*P < .05 **P < .01.
The linear regression analysis of CL and T1 Slope, C2S and C2-C4, and T1 Slope and C5-C7 are shown in Figure 3. The results of the linear regression analysis indicated a very strong association between T1 Slope and CL (R2 = .551, standard error 1.16°) and led to the equation CL = -1.081 *T1Slope +14.7. Beta coefficients from the regression analysis indicated that a nearly 1:1 relationship exists between T1 Slope and CL (beta = -1.081). For purposes of clinical applicability, we simplified this equation as CL = T1S - 14.7° ± 1.2°. Linear regression analysis also demonstrated the strong association between T1 Slope and C5-C7 (R2 = .372; P < .001) and C2S and C2-C4 (R2 = .309; P < .001). Linear regression analysis model of the parameters. A:T1 Slope vs CL (R2 = .551, P < .001); B: C2-C4 vs C2 Slope (R2 = .309,P < .001); C: C5-C7 vs T1 Slope (R2 = .372; P < .001).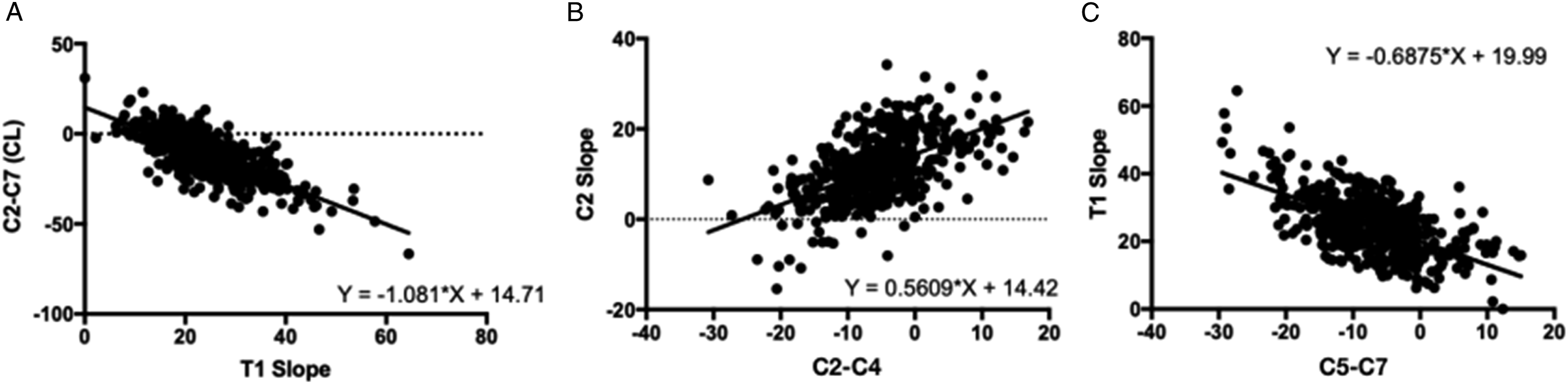
Discussion
The well-known theory of the “cone of economy” establishes that the cervical sagittal balance (CSB) is important for the maintenance of horizontal gaze and support of the neutral head posture.1,15 Alterations in CSB that occur with increasing age have been reported and described in previous studies; this could be used to predict cervical spine pathologies and optimize alignment for surgical planning.12,16,17 However, there are currently few studies reporting the normative values of age- and sex-related cervical sagittal parameters based on large Chinese samples. In this study, we performed a comprehensive analysis of cervical sagittal alignment with equal age and gender distribution in a large number of asymptomatic Chinese patients. In addition, normative reference data of cervical sagittal parameters for healthy adults were constructed for each gender and age group.
Using standard cervical radiographs, we demonstrated that changes in several cervical sagittal parameters were significantly associated with advancing age. Similar to previous studies, age was positively correlated with the C2-C7 Cobb angle and T1S.18,19 Older subjects tended to have greater TIA, NT, and cSVA. In fact, the accumulation of spinal degeneration with age affect the overall spine sagittal alignment.14,15,22 To be specific, decreased lumbar lordosis, increased thoracic kyphosis, and pelvic retroversion has been associated with age. 15 Furthermore, alterations in the thoracic spinal region due to age can also occur independently from the lumbar spine. The change of thoracic kyphosis is a complex compensatory process with multiple factors that include interactions between degenerative changes of the disc and facet, altered biomechanics of the spine, muscular fat infiltration and weakness, vertebral osteoporosis, and microfractures.23-28 And T1 vertebral body was fixed in a bony circle of the thoracic inlet due to anatomical reasons, and the declination of T1 was changed along with the thoracic spine curvature. In the sagittal plane, the increased T1S and TIA were mainly determined by the progress of T1 declination. Yokoyama et al 11 suggested that increases in cervical lordosis and T1 slope occurred along with age-related changes of thoracic kyphosis. Similarly, Kuang-Ting et al 20 demonstrated that increased thoracic kyphosis results in an increased T1 slope. However, there are also conflicting results: Yiwei Chen et al 18 showed that some parameters, such as TIA, T1S, and NT, have a turning point at the middle age of subjects, although the data generally show an age-related increased trend. Park et al 21 found a decrease in T1 slope in older subjects compared to younger subjects. They speculated that T1 declination changes to a more horizontal direction with age in order to reestablish horizontal gaze. Indeed, bias may also exist in the results of prior studies due to the limited sample size.
Evidence from previous studies suggests that T1S is a key modifier that affects the entire cervical alignment.29,30 Concerning the cervical spine, cervical lordosis and cSVA are increased as a compensatory cascade of cervicothoracic regions, which offsets the increased thoracic kyphosis and maintains a neutral head position. 27 Hwee et al 30 indicated the T1S <20° is predictive of C4-C7 kyphosis. Our results revealed that the middle cervical (C2-C4) Cobb angle significantly increased with age, while the lower cervical (C5-C7) Cobb angle increased with a slight tendency to level off. One possible explanation for these findings is that the lower cervical spine mainly corresponds to the T1S, while the upper and middle cervical spine adjusted the cranial angle to maintain horizontal gaze, which is consistent with past studies. Interestingly, previous studies indicated that C5-C7 segments had more advantageous effects on cranial sagittal alignment than middle or upper cervical lordosis. however, age-related disc degeneration, ligament weakness, and osteoporosis at C4-C7segment may decrease the compensatory mobility of the lower cervical spine. An increase of middle cervical lordosis may be a secondary inherent self-adaptive compensation for the change of the lower and upper cervical spine because the middle and lower cervical spine may play different roles in CBS.
The T1S-CL could be a key parameter for understanding CSB.13,28,31 Matching of the T1S and CL is an important factor that determines the clinical outcomes of cervical surgery. Staub BN et al 31 reported that the ideal CL of Westerners could be predicted by the formula CL = T1S - 16.5° ± 2° and indicated that T1S <16.5° may imply a kyphotic cervical alignment. The mean T1S and CL observed in this study agree with the values reported in previous studies of Asian groups, but these values are smaller than those in studies of Western populations.11,18 Previous studies demonstrated that the spinal and pelvic sagittal parameters of healthy Chinese subjects were smaller than that of Western populations. 32 These spinal and pelvic morphologies and orientation differences could have triggered the cascade of compensation mechanisms in cervical spine. Thus, we determined the value of T1S-CL based on the data from the Chinese asymptomatic population, and we report the formula CL = T1S - 14.7° ± 1.2°. This distinction is of importance to identify an operative indication and establish the goal of correction.
In addition, as a novel alignment parameter, C2S is important in describing cervical deformity. 33 Themistocles et al reported that C2S is correlated with health-related quality of life and indicated that outcome measures seemed to diminish as C2S crossed a 17-20° threshold. And C2S is a mathematical approximation of T1S- CL in normal sagittal alignment subjects. 33 This paper reports the C2S value of Chinese individuals as 11.3° ± 7.0°, which is lower than past studies. This may be associated with the less values of CL. While we did observe greater C2S in the older group, this difference was not clinically significant (only 1-2° difference) among young and older adults. It can be considered that the parameter was relatively stable and approximation in the different age groups. The same phenomenon was observed in the C1-C2 Cobb angle. Liu Hu et al 34 indicated that upper cervical alignment was relatively stable or slowly changed in asymptomatic adults. Ray Tang et al 12 demonstrated that the stability of upper cervical sagittal alignment is an important factor in maintaining neutral head posture. Moreover, this stability is related to the complex anatomy of the atlantoaxial joint, which has no intervertebral disc between C1-C2, and thus undertakes the function of axial rotation rather than flexion and extension.35,36
Few reports on gender-related differences among CSB parameters have been published, despite there are relevant differences among sagittal spinal and spinopelvic parameters. In a previous study from our center, Baoge et al 14 conducted a small sample, cohort study, and demonstrated that cervical alignment parameters in female subjects was lower than that in male subjects. A Taiwanese cohort study indicated that asymptomatic male subjects had higher values of T1S in spinal sagittal alignment compared with that of females. 20 The present study found the existence of a gender difference in sagittal parameters of the subaxial cervical spine across the different age groups based on a large, population-based cohort. Females’ cervical sagittal parameters are somewhat smaller than the corresponding parameters of males. We speculate that this phenomenon might result from differences in physiological structure, body size, and degree of spinal degeneration, which might been indirectly strengthened by the kinematics study by Greaves et al. Here, they showed cervical spine kinematics in females have a more anterior helical axis of motion in flexion-extension compared to males. 37 In another analysis on histological osteoarthritic changes in cervical spine facet joints, 38 it domenstrated the osteocartilaginous junction and the subchondral bone were affected males more severely, which would resulted to the larger thoracic kyphosis and cervical lordosis, but further analysis needed to be performed.
Age- and sex-related changes in cervical sagittal alignment should be taken into consideration in the preoperative evaluation of patients with various cervical spine disorders. Nonetheless, there were some limitations in this study. First, the whole spinal X-ray was not taken and the sagittal parameters of thoracic, lumbar, and spinopelvic segments were not measured. Associating the CSB with full spinal sagittal alignment may clarify the changes of cervical sagittal alignment more comprehensively. Second, some subjects were excluded because of the obscured superior T1 endplate on X-ray, which may introduce selection bias in the results. To improve the objectivity and accuracy of the results, further subgroup analysis based on different ethnic groups, occupations, lifestyles, and BMI should be investigated in the future.
Conclusion
In this radiographic study, we found that the cervical sagittal parameters differed by age and gender in asymptomatic Chinese adults. In addition to the CL, cSVA, and T1S, the C2-4 Cobb angle of older subjects was significantly higher, suggesting age can influence the compensatory mechanisms that involve the middle cervical spine. Normative CL of Chinese adults could be predicted by the equation CL = T1S - 14.7° ± 1.2°, which suggests the threshold of cervical deformity and provides a clear surgical target for correction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Beijing Natural Science Foundation [grant number: 7232182]; Research and Development Fund of Peking University People’s Hospital [grant number: RDY2021-12]; Research and Development Fund of Peking University People’s Hospital [grant number: RDL2022-52].
Ethical Approval
We have acquired approval by local ethics committee.
Informed Consent
All authors have signed patient consent forms.
IRB Statement
This study was approved by the institutional review boards of Peking University People’s Hospital (2018PHC076).