
Abstract
Study Design
Retrospective cohort study.
Objective
To investigate the independent predictive factors for moderate-severe pulmonary impairment (MSPI) among adolescent idiopathic scoliosis (AIS) patients.
Methods
The preoperative pulmonary function tests (PFTs) of 102 AIS patients (major Cobb angle ≥45°) operated between 2015 and 2020 were retrospectively reviewed. Patients were divided into 2 groups based on the predicted forced vital capacity (FVC) and forced expiratory volume in one second (FEV 1 ), respectively. Group 1 had normal/ mild pulmonary impairment (FVC or FEV 1 >65% predicted) whereas Group 2 had MSPI (FVC or FEV 1 ≤65% predicted). Multivariate logistic regression analysis was performed to determine the predictive factors for MSPI.
Results
41.2% (N = 42) and 52.0% (N = 53) of the total patients were categorised into Group 2 (MSPI) based on predicted FVC and FEV1, respectively. In general, Group 2 had more patients with a major main thoracic (MT) curve, larger MT curve with lower MT flexibility, a larger MT apical vertebra translation (MT-AVT), and a smaller thoracolumbar-lumbar (TL/L) AVT than Group 1 (P < .05). When analyzing the MT Cobb angle for every 10° increment, patients with MT Cobb angle ≥70° had MSPI (N = 31.4%). Body mass index (BMI) (FVC: aOR .8; FEV1: aOR .9) and MT Cobb angle (for every 10° increment, FVC: aOR 1.7; FEV1: aOR 1.8) were the significant independent predictive factors for MSPI.
Conclusion
MSPI was evident in patients with MT Cobb angle ≥70°, with MT Cobb angle and BMI being the significant independent predictive factors.
Introduction
Scoliosis is a three-dimensional (3D) deformity of the spine, and thoracic/rib cage deformity is one of the main components involved.1,2 The impact of scoliosis on thoracic deformity was thought to be complex. Notably, scoliosis impedes ribs movement thus compromising the respiratory muscles and displacing the organs in the thoracic cavity. Eventually, this reduces the chest wall compliance directly and the lung compliance indirectly. 3
Studies had been relating the spine deformity in adolescent idiopathic scoliosis (AIS) patients with its adverse effects on pulmonary functions. 4 Machino et al 5 concluded that AIS patients with restrictive lung disorder (RLD) had significantly smaller rib-cage volume than patients without RLD (3.94 L vs. 4.49 L, respectively). Several authors also demonstrated that pulmonary impairment was present among AIS patients with larger main thoracic (MT) Cobb angle, greater apical vertebral rotation angle, or hypokyphosis.4,6,7 Moderate to severe pulmonary impairment had been reported as clinically relevant pulmonary impairment.8-11 Yaszay et al 7 reviewed preoperative pulmonary function tests (PFTs) and 3D reconstructed imaging of 163 AIS patients, and deduced that patients with moderate to severe pulmonary impairment (≤65% predicted PFTs values) had 3D coronal Cobb >80°, thoracic lordosis >20°, and absolute apical rotation >25°. Nevertheless, majority of the earlier studies did not include clinical factors ie, age, gender, or body mass index (BMI), in their analysis of predictive factors for pulmonary impairment.
Despite extensive literature review, only scarce data reported on both clinical and radiological predictive factors for poor pulmonary function among AIS patients were found. To date, controversies on the negative impact of scoliosis on pulmonary function still persist. 4 Therefore, the purpose of this study was to investigate the clinical and radiological predictive factors for moderate-severe pulmonary impairment (MSPI) among AIS patients. The reported data would benefit surgeons in risk counselling, preoperative planning, and preoperative optimization to avoid detrimental respiratory complications.
Methodology
This was a retrospective study conducted in a single academic institution involving AIS patients who underwent posterior spinal fusion (PSF) between the years 2015 and 2020. This research was approved by our institution ethical board (MREC ID NO.: 2020108-9138). AIS patients who were of Asian ethnicity, aged between 10 and 18 years old, with a major Cobb angle of ≥45°, and inclusive of all Lenke curve types were recruited. Patients who had non-idiopathic scoliosis, anterior surgery, revision surgery, or patients with pre-existing cardiopulmonary diseases were excluded.
Pulmonary Function Tests (PFTs)
Preoperative PFTs were performed in 107 AIS patients. We excluded 5 patients with incomplete PFTs data. Plethysmography and PFTs were used to measure total lung capacity (TLC), forced vital capacity (FVC), and forced expiratory volume in one second (FEV1). Each test was repeated 3 times and the single best effort was recorded. Age, gender, and height-matched standards published by the American Thoracic Society were used to generate a percentage of the predicted values for each pulmonary parameter (predicted FVC or predicted FEV 1 ). In this study, pulmonary function was identified as normal when FVC or FEV 1 were >80% of the predicted values. Mild pulmonary impairment was defined as FVC or FEV 1 ≤80% but >65% predicted, whereas moderate pulmonary impairment was FVC or FEV 1 ≤65% but ≥50% predicted. Severe pulmonary impairment was defined as FVC or FEV 1 <50% predicted.8-12
The definitions of PFTs parameters are as follows
6
: 1. Forced vital capacity (FVC): maximum volume of air expelled as rapidly and completely as possible by a maximum effort after a maximum inspiration. 2. Forced expiratory volume in one second (FEV1): The amount of air expired in one second during a rapid and maximal expiration from full inspiration. 3. Total lung capacity (TLC): summation of FVC and reserved volume (RV).
Data Collection
Clinical data collected were age, gender, menarche age, and BMI. Lenke curve types, Risser sign, MT and thoracolumbar/lumbar (TL/L) Cobb angle, side bending (SB) Cobb angle, flexibility, thoracic kyphosis (TK), location of apical vertebra, number of vertebrae involved, coronal deformity angular ratio (C-DAR), MT apical vertebra translation (MT-AVT), and TL/L apical vertebra translation (TL/L-AVT) were documented.
Below are the definitions of the radiological parameters: 1. Side bending (SB) flexibility: 2. Coronal deformity angular ratio (C-DAR): unitless number used to evaluate the severity of the coronal deformity. 3. Main thoracic apical vertebra translation (MT-AVT): the horizontal distance from the midpoint of the MT curve apical vertebra (or intervertebral disc) to C7 plumb line. 4. Thoracolumbar-lumbar apical vertebra translation (TL/L-AVT): the horizontal distance from the midpoint of the TL/L curve apical vertebra (or intervertebral disc) to central sacral vertical line (CSVL). 5. Thoracic kyphosis (TK): Cobb angle between the superior end plate of T5 vertebra and the inferior end plate of T12 vertebra, measured in the sagittal plane.


Statistical Analysis
Data analysis was performed using the SPSS version 26.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA). Descriptive data analysis was conducted for all clinical, radiological, and PFTs data. Independent samples t-test and chi-square test were performed for continuous variables and categorical variables, respectively. For statistical analysis, all patients in this cohort were classified into 2 groups based on the predicted FVC or FEV1, respectively. Group 1 patients had normal/ mild pulmonary impairment (FVC or FEV 1 >65% predicted) whereas Group 2 patients had moderate-severe pulmonary impairment (MSPI) (FVC or FEV 1 ≤65% predicted).
Univariate logistic regression analysis followed by multivariate logistic regression analysis was performed to identify the independent predictive factors for MSPI (FVC or FEV 1 ≤65% predicted). Factors with P < .25 identified in the univariate logistic regression analysis were subsequently included in the multivariate logistic regression analysis. Independent predictive factors were determined by P < .05. Receiver-Operating-Characteristics (ROC) curve was drawn to predict MSPI for various MT Cobb angles. Youden Index was calculated for various points on ROC curve, whereby the optimal cut-off value was defined as the point with the highest Youden Index.13,14
Results
Preoperative Clinical and Radiological Data of 102 AIS Patients in Relation to the Predicted FVC (%).
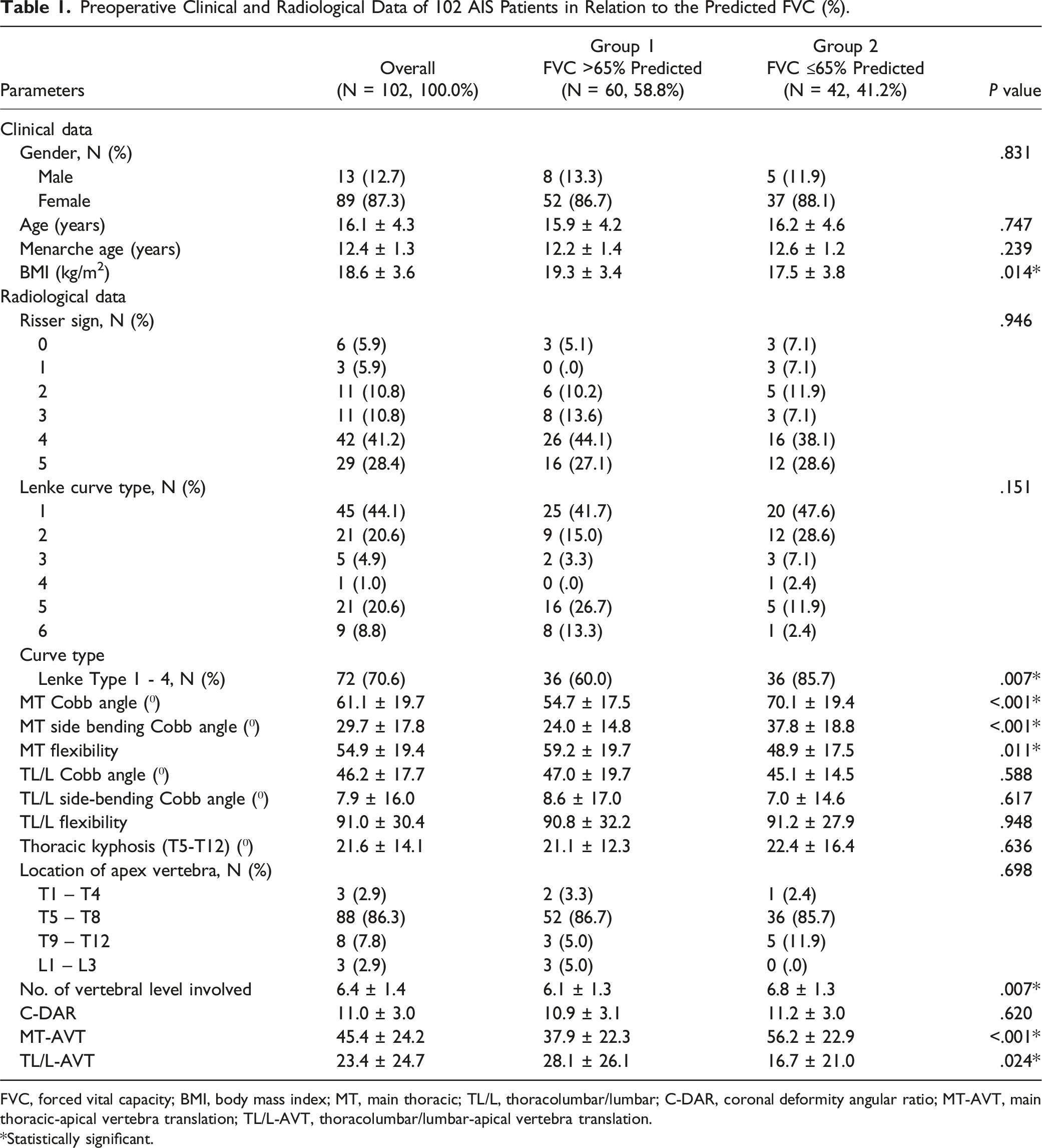
FVC, forced vital capacity; BMI, body mass index; MT, main thoracic; TL/L, thoracolumbar/lumbar; C-DAR, coronal deformity angular ratio; MT-AVT, main thoracic-apical vertebra translation; TL/L-AVT, thoracolumbar/lumbar-apical vertebra translation.
*Statistically significant.
Preoperative Clinical and Radiological Data of 102 AIS Patients in Relation to the Predicted FEV1 (%).
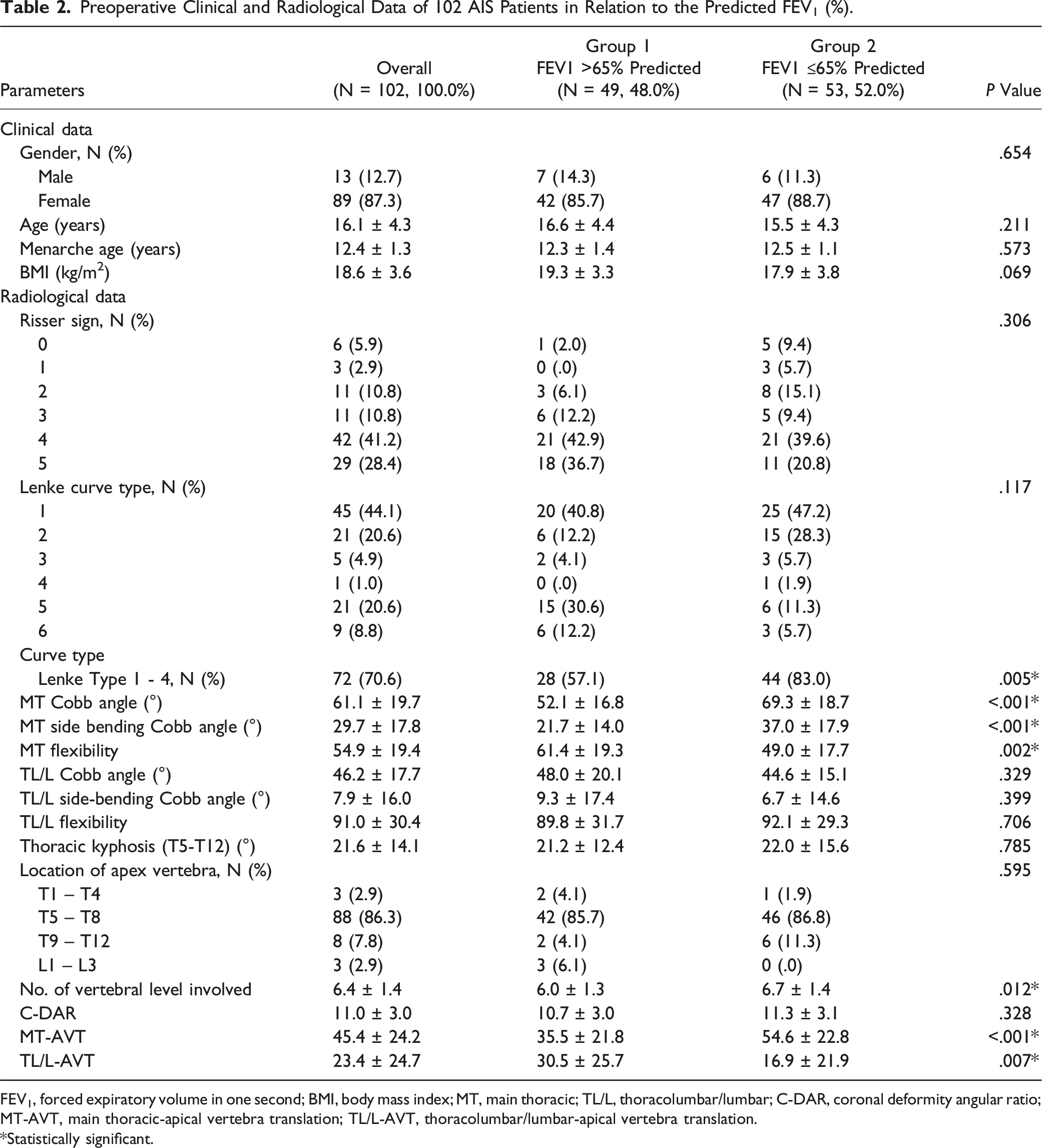
FEV1, forced expiratory volume in one second; BMI, body mass index; MT, main thoracic; TL/L, thoracolumbar/lumbar; C-DAR, coronal deformity angular ratio; MT-AVT, main thoracic-apical vertebra translation; TL/L-AVT, thoracolumbar/lumbar-apical vertebra translation.
*Statistically significant.
PFTs
Pulmonary Function Tests (PFTs) Stratified by the Magnitude of Main Thoracic (MT) Curves.
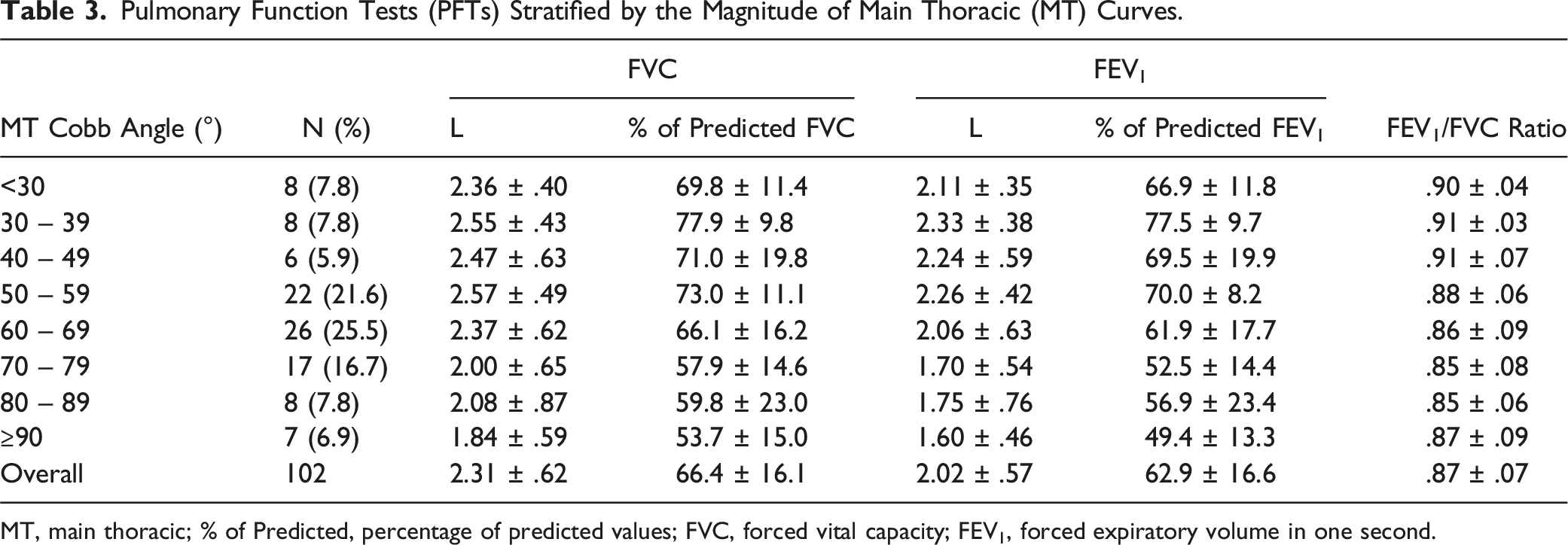
MT, main thoracic; % of Predicted, percentage of predicted values; FVC, forced vital capacity; FEV1, forced expiratory volume in one second.
Logistic Regression Analysis
Multivariate Logistic Regression Analysis Performed to Determine the Independent Predictive Factors for Moderate-Severe Pulmonary Impairment (MSPI) (FVC or FEV 1 ≤65% predicted).
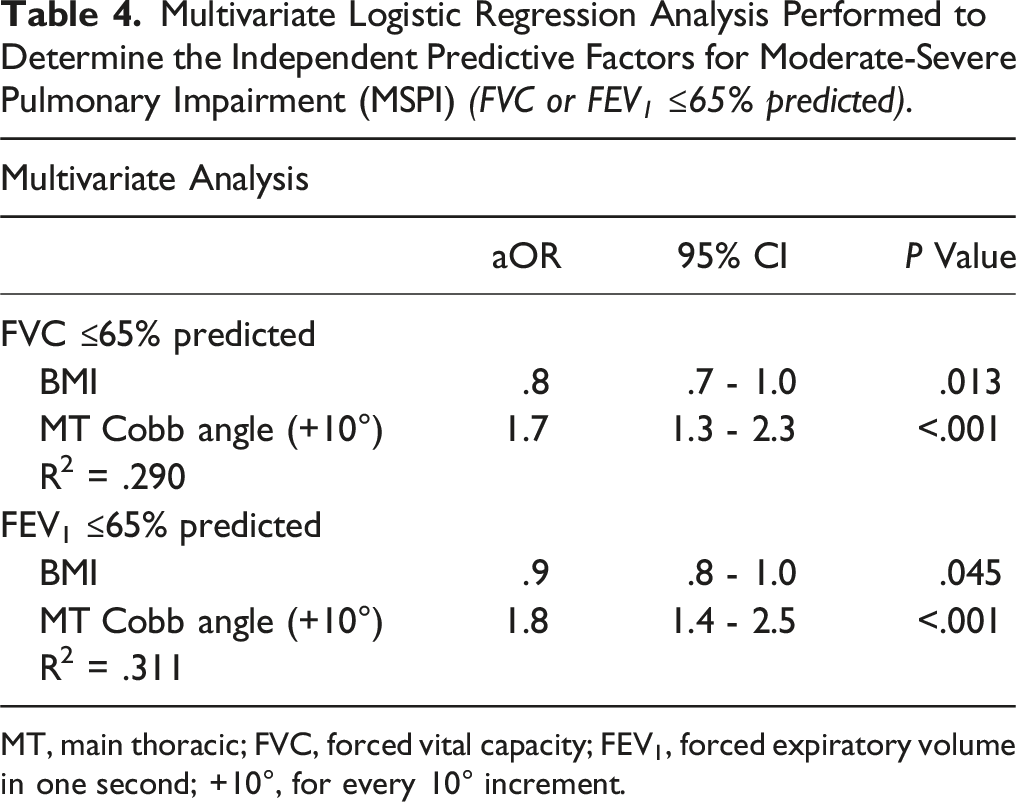
MT, main thoracic; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; +10°, for every 10° increment.
ROC Curve Analysis
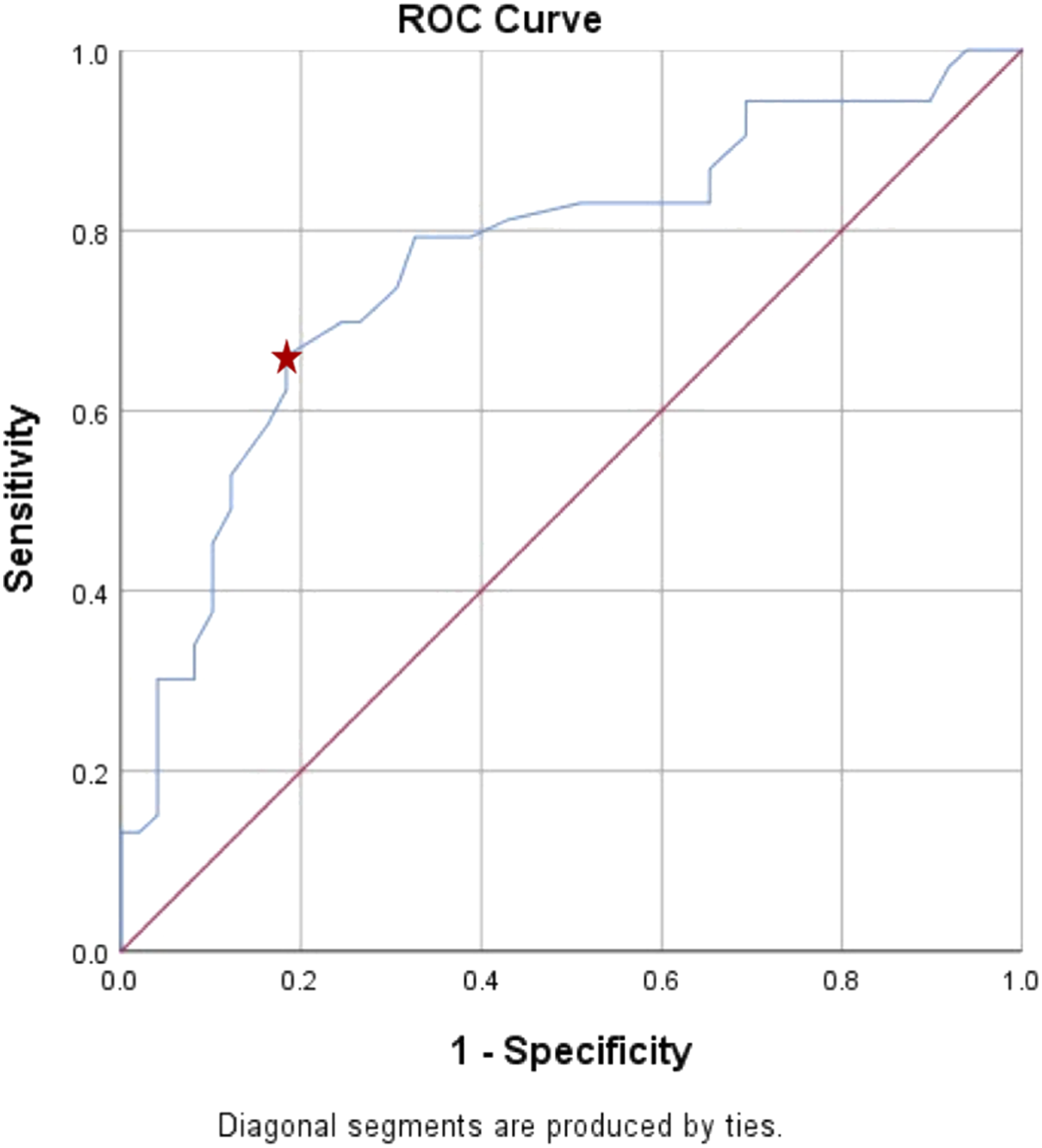
Upon establishing that MT Cobb angle was a statistically significant independent predictor for MSPI, we proceeded to analyse the data using ROC curve analysis. Using the predicted FVC, we identified that a MT Cobb angle of 64.5° had the highest Youden Index (.481) with area under the curve (AUC) of .751 in predicting MSPI (FVC ≤65% predicted) (P < .001). This cut-off value of 64.5° for MT Cobb angle had a sensitivity of 71.4% and specificity of 76.7% (Figure 1). Similarly, ROC curve analysis using the predicted FEV1 illustrated that a MT Cobb angle of 64.5° had the highest Youden Index (.476) with AUC of .767 (P < .001). It has a lower sensitivity of 66.0% but a relatively higher specificity of 81.6% in predicting MSPI (Figure 2). Receiver-operating-characteristic (ROC) curve for the MT Cobb angle cut-off value of 64.5° in predicting moderate-severe pulmonary impairment (MSPI) (FVC ≤65% predicted) in a single curve. Star indicated 71.4% sensitivity, 76.7% specificity, youden index of .481, and AUR of .751. Receiver-operating-characteristic (ROC) curve for the MT Cobb angle cut-off value of 64.5° in predicting moderate-severe pulmonary impairment (MSPI) (FEV
1
≤65% predicted) in a single curve. Star indicated 66.0% sensitivity, 81.6% specificity, youden index of .476, and AUR of .767.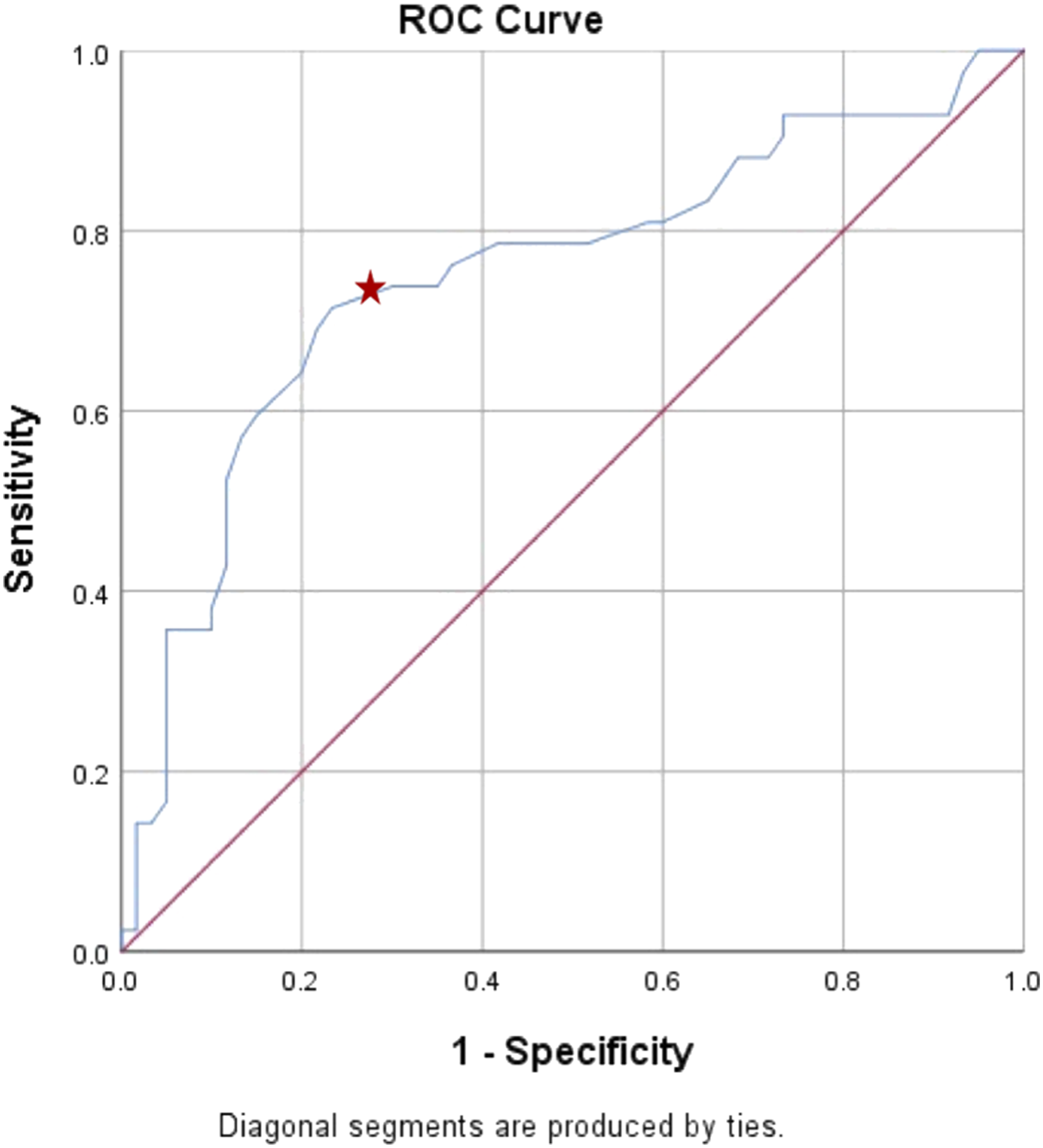
Discussion
Clinical studies had explored the connection between spinal deformities and pulmonary function, particularly in examining the link between AIS and pulmonary impairment.4,8,16,17 Clarification on the widely held presumption that only severe scoliosis is associated with pulmonary impairment remains inconclusive, despite numerous prior studies. In the study of the natural history of scoliosis, Weinstein et al 18 reported that having a Cobb angle of ≥50° at skeletal maturity was a significant predictor for reduced pulmonary function. Early study by Szeinberg et al 19 reported that pulmonary impairment was even found among idiopathic scoliosis patients with Cobb angle <60°. A large series study involving fifteen centers by Johnston et al 8 later reported that clinically relevant pulmonary impairment was present among AIS patients with mean MT curves of more than 70°. The authors concluded that PFTs correlated with the severity of MT curve, sagittal plane hypokyphosis (T5-T12 < 10°), and to a lesser extent in proximal thoracic (PT) curve (PT Cobb angle >30°). 8
Likewise, our study revealed that moderate pulmonary impairment (FVC or FEV 1 ≤65% but ≥50% predicted) was present among AIS patients with MT Cobb angle of ≥70° and severe pulmonary impairment (FVC or FEV 1 <50% predicted) could be observed notably among patients with severe scoliosis (MT Cobb angle ≥90°). In the recent systematic review and meta-analysis by Kan et al, 4 the team concluded that larger PT and MT Cobb angles, hypokyphosis, greater lumbar lordotic angles, longer thoracic curve, larger rib hump, increased apical vertebral rotation angles, and smaller rib cages, were the variables associated with poorer pulmonary functions. In a long term follow-up study of more than 27 years after surgery, 27.7% of the AIS patients in the study had restrictive pulmonary function whereby large rib humps and large vertebral rotation were the significant factors identified for poor predicted FVC. 20 Nevertheless, in our study cohort, the only significant radiological predictive factor identified for MSPI was the MT Cobb angle.
Newton et al 11 reported that AIS patients with hypokyphosis (≤10°) were more likely to have MSPI. Dreimann et al 12 concluded that both spectrums of thoracic kyphosis with combination of thoracic curve magnitude have significant impact on predicted FVC. Patients with lordoscoliosis as well as kyphoscoliosis have an increased risk for reduced predicted FVC. Meanwhile, in our current study, the mean thoracic kyphosis (T5-T12) for Group 2 patients (MSPI) were 22.4 ± 16.4° and 22.0 ± 15.6° for the predicted FVC and predicted FEV1, respectively. However, no statistical significance was identified when they were compared to Group 1 patients. Our data analysis also revealed that Group 2 patients (MSPI) had a significantly more severe MT curve with lower MT flexibility, larger MT-AVT, and smaller TL/L-AVT. Similarly, Wang et al 6 conducted a correlation analysis between PFTs and radiological parameters of the main right thoracic curve in AIS patients and deduced that the predicted FVC had significant negative correlations with MT Cobb angle, MT curve-rib hump, MT curve apical vertebral body-to-rib ratio (MT-AVB-R), and MT-AVT.
By analysing the clinical parameters, we identified that BMI was the other significant independent predictive factor for MSPI (FVC: aOR .8; FEV1: aOR .9) (P < .05). Besides denoting nutritional status, BMI was also reported in prior research findings to have a correlation with poor pulmonary function.21-23 In a prospective study by Xu et al, 23 a positive correlation was found between BMI and pulmonary function whereby low BMI (BMI <17.7 kg/m2) was significantly associated with pulmonary impairment. Our logistic regression analysis affirmed the results reported in the aforementioned studies regarding the relationship between BMI and pulmonary impairment. Based on the predicted FVC, Group 2 patients (MSPI) in our study had significantly lower BMI of 17.5 ± 3.8 kg/m2 (P = .014).
It was proven that ethnicity difference does have a role in affecting patients’ pulmonary function. Generally, smaller reduction (∼11%) in FVC and FEV1 were observed in Southeast Asian patients as compared to patients of Caucasian ethnicity. 24 Therefore, the results in our study would be relatively more pertinent to an Asian population. The variability of accuracy in pulmonary function testing could be one of the main limitations of this study.11,25 There were theoretical concerns regarding the usage of normative data based on height and gender to derive predicted values for PFTs in the evaluation of a condition affecting the height of the test subjects, for instance, AIS population in this study. 25 The results of the current PFTs in this study were not corrected for the height difference due to scoliosis. This could potentially lead to the underestimation of the reduced pulmonary function. Nevertheless, the authors made an attempt to reduce the impact of other confounding variables by excluding patients with known cardio-pulmonary diseases. Despite PFT being an objective measure of pulmonary function, another notable drawback in this study was the lack of patient reported outcome measurements (PROMs) to reflect the clinical relevance in terms of respiratory symptoms. Future studies could incorporate PROMs into the analysis.
This study will be crucial for deformity surgeons to be vigilant in identifying patients at high risk for MPSI (especially those do not comply with PFT) before proceeding with surgical procedures that could further compromise the pulmonary function, such as thoracotomy, thoracoplasty, and rib resections with 3-column osteotomies. We also found that larger MT curves were associated with moderate to severe pulmonary impairment with a 1.7 to 1.8 times increased likelihood of having MSPI for every 10° increment in Cobb angle. Therefore, corrective surgeries should be performed as early as possible among AIS patients with worsening thoracic curvatures to prevent deterioration in pulmonary function.
Conclusion
MSPI was evident in AIS patients with a MT Cobb angle of ≥70°. MT Cobb angle and BMI were significant independent predictive factors for MSPI in AIS patients with a major Cobb angle of ≥45°. The ROC curve analysis demonstrated that a MT Cobb angle of 64.5° is the cut-off value for predicting MSPI in AIS patients, with a sensitivity of 71.4% and specificity of 76.7% for predicted FVC, and sensitivity of 66.0% and specificity of 81.6% for predicted FEV1.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.