
Abstract
Study Designs
Retrospective Database Analysis.
Objectives
Pre-operative glycemic control in diabetic patients undergoing lumbar fusion (LF) is essential for evaluating complication risk. However, current thresholds for preoperative HbA1c and same-day-glucose (SDG) are either non-specific or have low predictive power. This study uses HbA1c and SDG to provide data-driven risk stratification for 90-day major and wound complications in LF patients.
Methods
Using a national database, patients undergoing LF from 2013-2022 with a recorded preoperative HbA1c and SDG level were included for analysis. Multiple HbA1c and SDG strata were identified using stratum specific likelihood ratio analysis (SSLR). Each stratum was then propensity-score matched to the lowest strata and compared using risk ratios. Significance level was set at a P-value <0.05.
Results
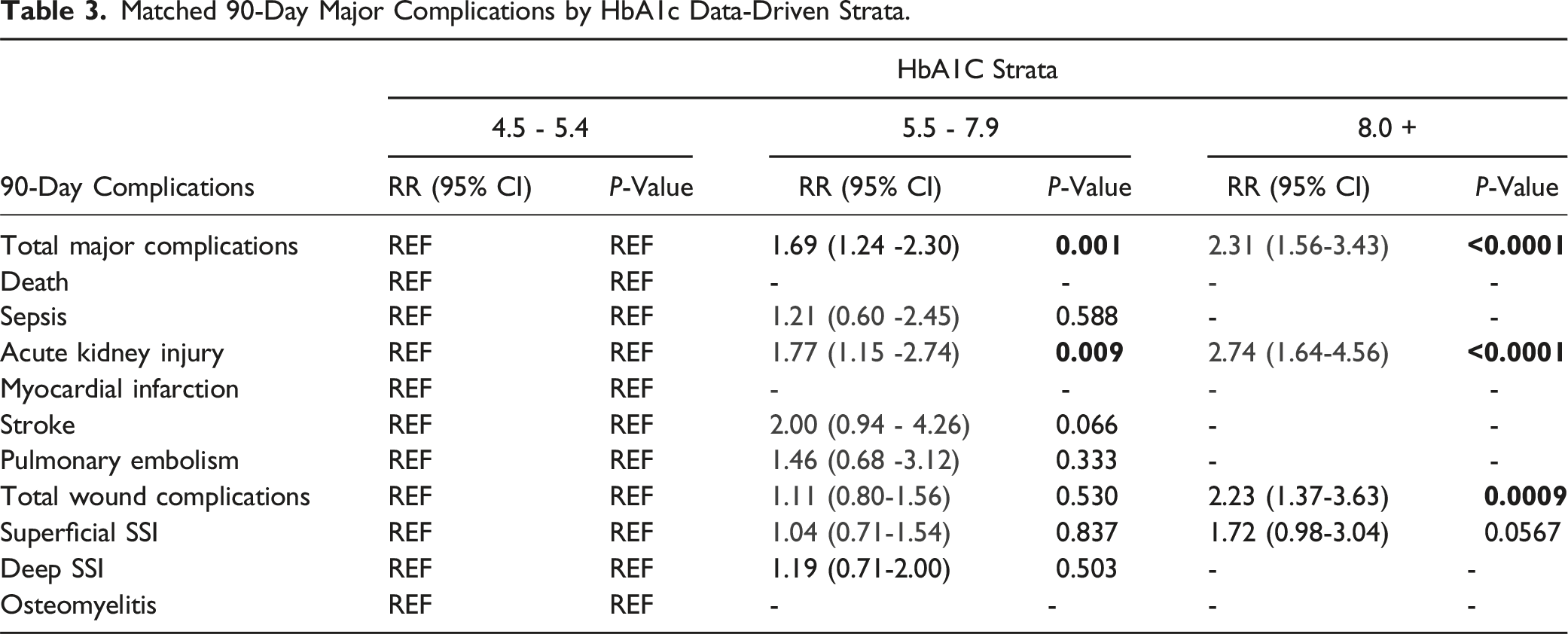
12,026 patients met inclusion criteria. For 90-day major complications, SSLR identified 3 predictive HbA1c (4.5-5.4, 5.5-7.9, and 8.0+) and SDG strata (60-159, 160-239, and 240+). Following propensity-matching, the 90-day major complication risk sequentially increased for HbA1c: 5.5-7.9 (1.69; P = 0.001; 95% CI 1.24-2.30), 8.0+(2.31; P < 0.001; 95% CI 1.56-3.43). Following propensity-matching, the SDG strata similarly demonstrated sequentially increasing 90-day major complication risk: 160-239 (1.34; P < 0.001; 95% CI 1.18-1.54), 240+ (1.64; P < 0.001; 95% CI 1.31-2.05). Matched analysis demonstrated a higher relative-risk of 90-day wound complications for the 8.0+ HbA1c strata (2.23; P = 0.001; 95% CI 1.37-3.63) compared to the HbA1c 4.5-5.4 strata. No other strata were identified that predicted differences in 90-day wound complications.
Conclusions
This study identified data-driven HbA1c and SDG strata that better risk-stratify 90-day major complications following LF. Instead of current single-value thresholds, these multiple strata may be utilized for better preoperative guidance.
Objectives
Diabetes mellitus (DM) is a well acknowledged risk factor for complications following lumbar spine surgery.1-3 These complications stem from poor glycemic control causing reduced immune function, poor vascularization, and overall decreased wound healing capacity.4-6 Previous studies have linked hyperglycemia to increased rates of perioperative infection, sepsis, septic shock, urinary tract infection, pneumonia, blood transfusion, in-hospital death, non-union, poor post-surgical pain improvement, longer hospital stays, and readmission for complications,7-10 as well as lower patient reported outcome measures in long-term follow-up.3,11-13 The current gold-standard marker for preoperative glycemic control is hemoglobin A1c (HbA1c), with some use of same day serum glucose (SDG) levels as a measure of perioperative glycemic management. Preoperative HbA1c levels provide insight into the average glycemic control a patient has attained over the previous 90 days, 14 while SDG measures give insight into current glycemic control.
With evidence of increasing prevalence of patients with diabetes as lumbar fusion (LF) surgery candidates, 15 the importance of preoperative glycemic control evaluation measures cannot be understated. Although the consequences of poor glycemic management in the perioperative period are well defined, current established thresholds for preoperative HbA1c and blood glucose levels for LF are either non-specific or have low power in predicting complications. 16 Data-driven thresholds have been established for other orthopaedic surgeries, but not for LF. 17 Additionally, further risk stratification for 90-day major complications and 90-day wound complications following LF based on preoperative HbA1c and SDG levels has not been investigated.
Therefore, the objective of this study was to generate data-driven stratifications using stratum specific likelihood ratio (SSLR) analysis for preoperative HbA1c and SDG measures. We hypothesized that patients could be placed into 2 or more data driven strata, rather than a single threshold, that maximized the statistical significance of risk for 90-day major complications and 90-day wound complications based on both HbA1c and SDG levels.
Methods
Patients who underwent LF from 2013 to 2022 were identified in the TriNetX database (trinetx.com, 125 Cambridgepark Drive, Suite 500, Cambridge, MA 02140). The TriNetX database is a comprehensive resource that partners with data providers covering approximately 99% of U.S. health plans. This includes contributions from hospitals, primary care practices, and specialty treatment providers across a wide range of geographic regions, age groups, and socioeconomic levels. Data is aggregated directly from electronic medical record (EMR) systems on a continuous basis, ensuring it is both up-to-date and representative of a broad patient population. This systematic HCO-wide integration minimizes the risk of selection bias within an HCO and enhances the generalizability of the findings across multiple institutions and geographic regions. The Research Network sub-database was utilized which contains information of over 130 million patients from 70 HCOs in the United States. The database updates on a weekly basis, permitting access to the most up-to-date data. The first record from the first HCO in this sub-database was in 2005. Patients who underwent LF were identified using Current Procedural Technology (CPT) and International Classification of Disease (ICD-10) codes. The ICD-10 codes used were 22 533 (Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace [other than for decompression]; lumbar), 22 558 (Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace [other than for decompression]; lumbar), 22 612 (Arthrodesis, posterior or posterolateral technique, single interspace; lumbar [with lateral transverse technique, when performed]), and 22 630 (Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace [other than for decompression], single interspace, lumbar). Patients were included in the analysis if they were at least 18 years of age and had either a HbA1c level taken within 3 months before the procedure or a recorded SDG level on the day of surgery. Ninety-day major complications were defined as death, sepsis, acute kidney injury (AKI), myocardial infarction, stroke, or pulmonary embolism. 90-day wound complications included superficial surgical site infection (SSI), deep SSI, and osteomyelitis.
Distinct data-driven strata for HbA1c and SDG levels were established using stratum specific likelihood ratio (SSLR) analysis, a modified approach to analyzing Receiver Operating Characteristics (ROC) curves. SSLR analysis, which has been highly utilized in orthopaedic literature,17-21 has been shown to be more adaptive than using ROC curves. 22 In particular, SSLR analysis allows for the identification of data-driven strata that optimize differences in various complications by using likelihood ratios. The SSLR expansion on ROC curves provides a clinically meaningful statistical stratification of postoperative complication risk based on same-day glucose and HbA1c levels. SSLR analysis was performed using the initial 90-day major complication rates and 90-day wound complication rates for LF patients with HbA1c levels from 4.5-10+ and SDG levels from 60-240+. If SSLR was successful in identifying distinct strata that maximized the differences in probability of 90-day major complications or 90-day wound complications, the initial complication rates for these strata were then recorded for additional analysis.
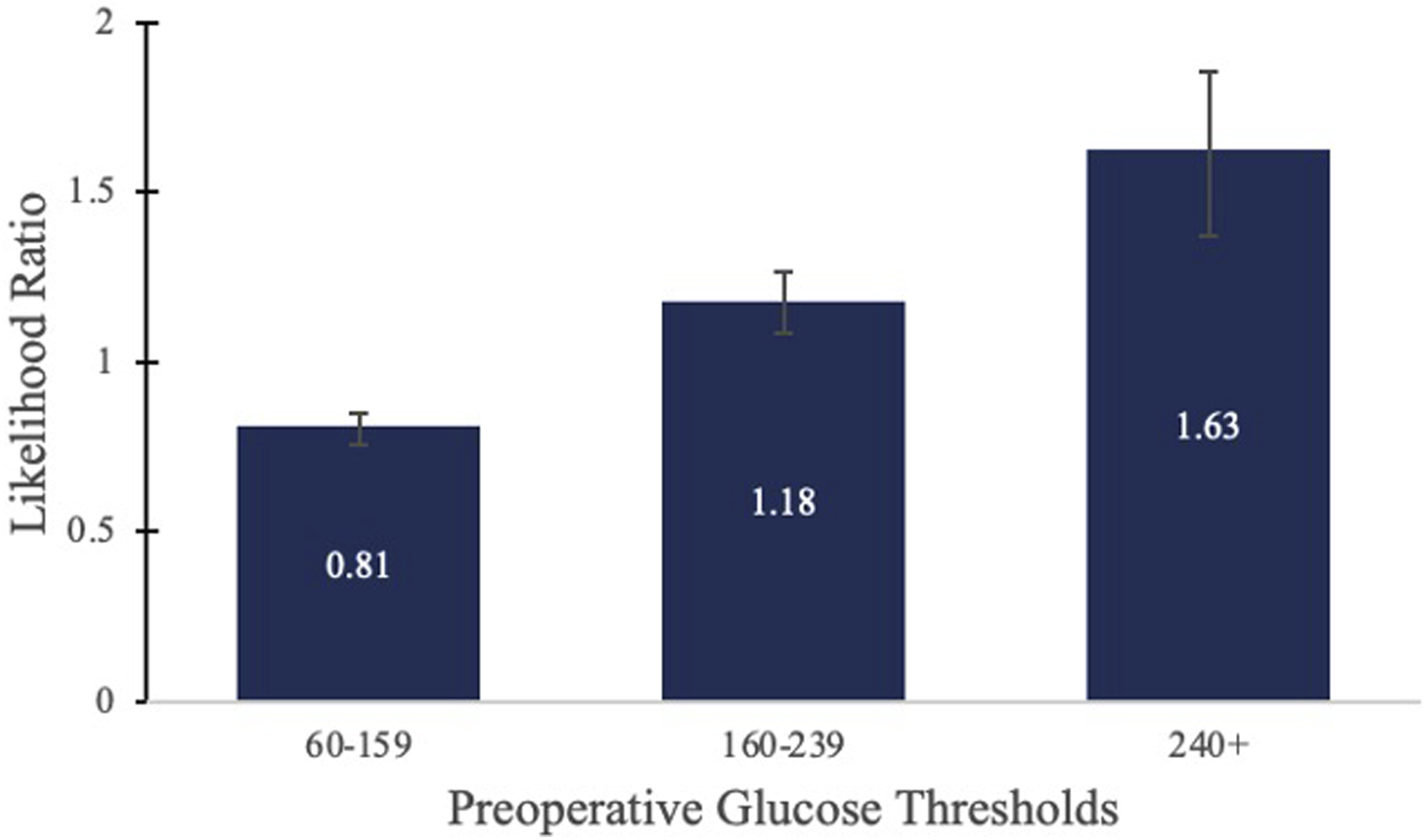
In further statistical analysis, the patients within the lowest strata for SDG and HbA1c values were determined to have the baseline risk profile for 90-day major complications and 90-day wound complications following LF surgery and were thereby used as the control cohorts. As opposed to single-value cut-offs previously reported in existing literature, using the lowest SSLR-generated strata as the baseline risk allowed us to compare risks between multiple cohorts that represent varying levels of glycemic control. To control for confounding variables, each stratum was propensity-score matched to the lowest strata based on age, sex, hypertension, heart failure, chronic obstructive pulmonary disease, and obesity. The risk ratio (RR) and 95% confidence interval (CI) for each stratum with respect to the lowest matched stratum was then observed. A significance level was set at a P-value threshold of <0.05. (Figures 1 and 2). Stratum specific likelihood ratio analysis for 90-day major complications after LF based on HbA1c Strata. Stratum specific likelihood ratio analysis for 90-day major complications after LF based on preoperative glucose strata.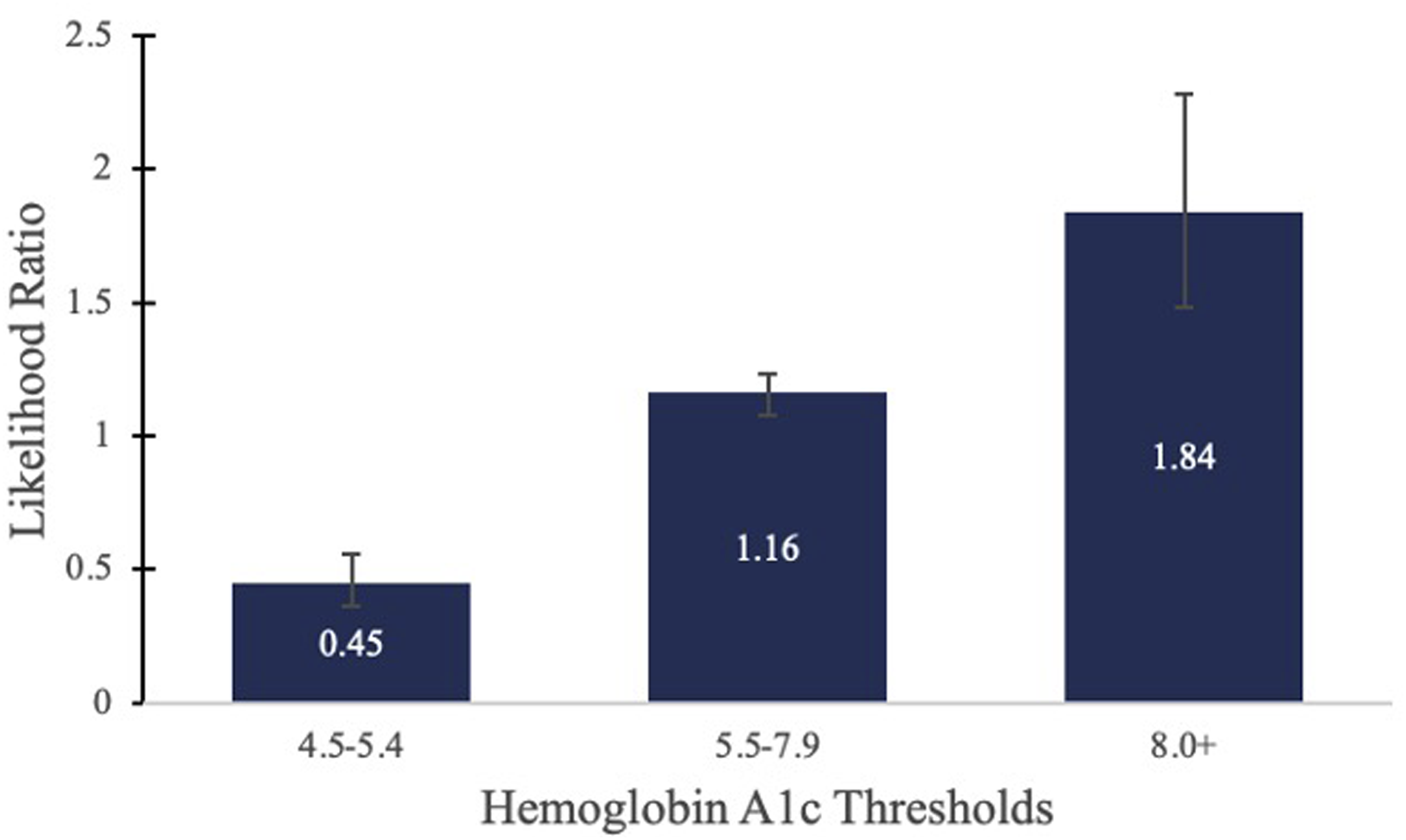
Results
Total Demographics.
SSLR analysis identified 3 data-driven HbA1c strata (4.5-5.4, 5.5-7.9, and 8.0+) and 3 data-driven SDG strata (60-159, 160-239, and 240+) that predicted 90-day major complications. The patients with HbA1c values between 4.5 and 5.4 and SDG values between 60-159 were determined to have the baseline risk profile and therefore were used as controls for further statistical analysis. Prior to propensity matching, HbA1c patient cohorts contained the following patient counts: 4.5-5.4 (n = 1437), 5.5-7.9 (n = 3091), and 8.0+ (n = 507).
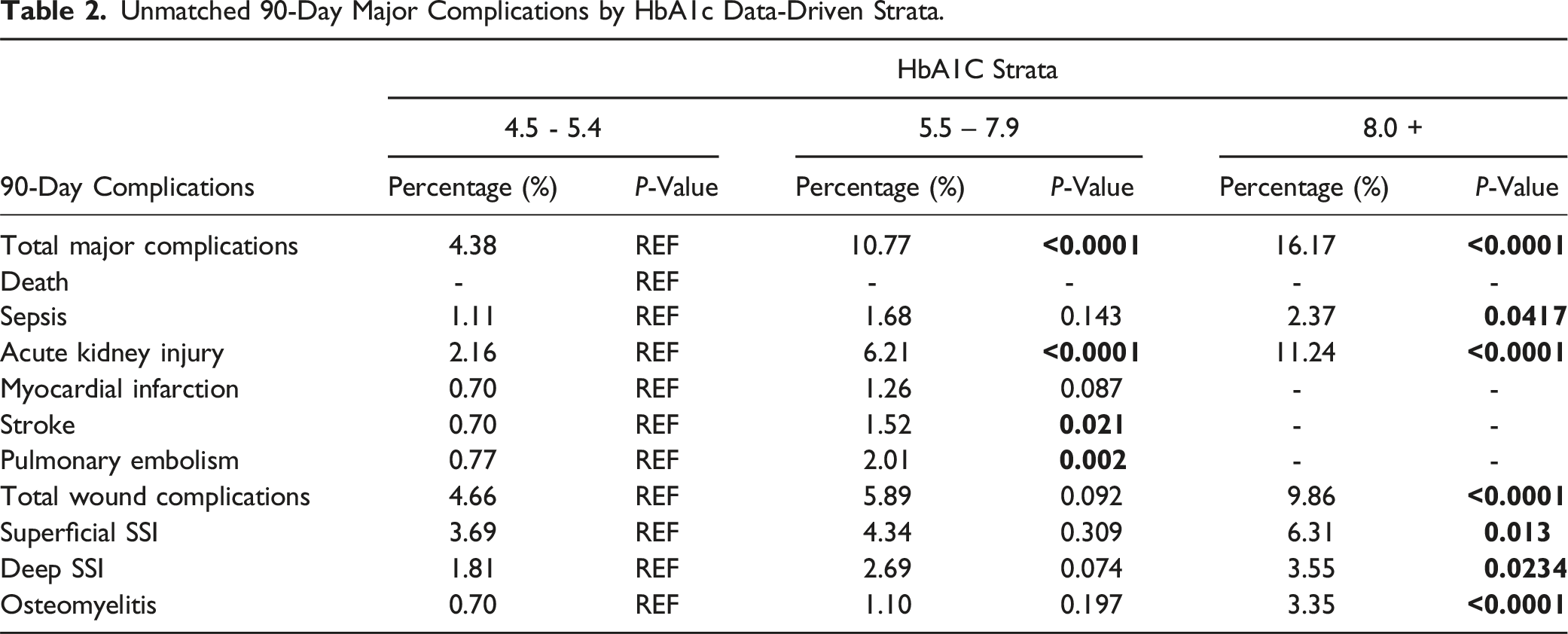
Unmatched 90-Day Major Complications by HbA1c Data-Driven Strata.
Matched 90-Day Major Complications by HbA1c Data-Driven Strata.
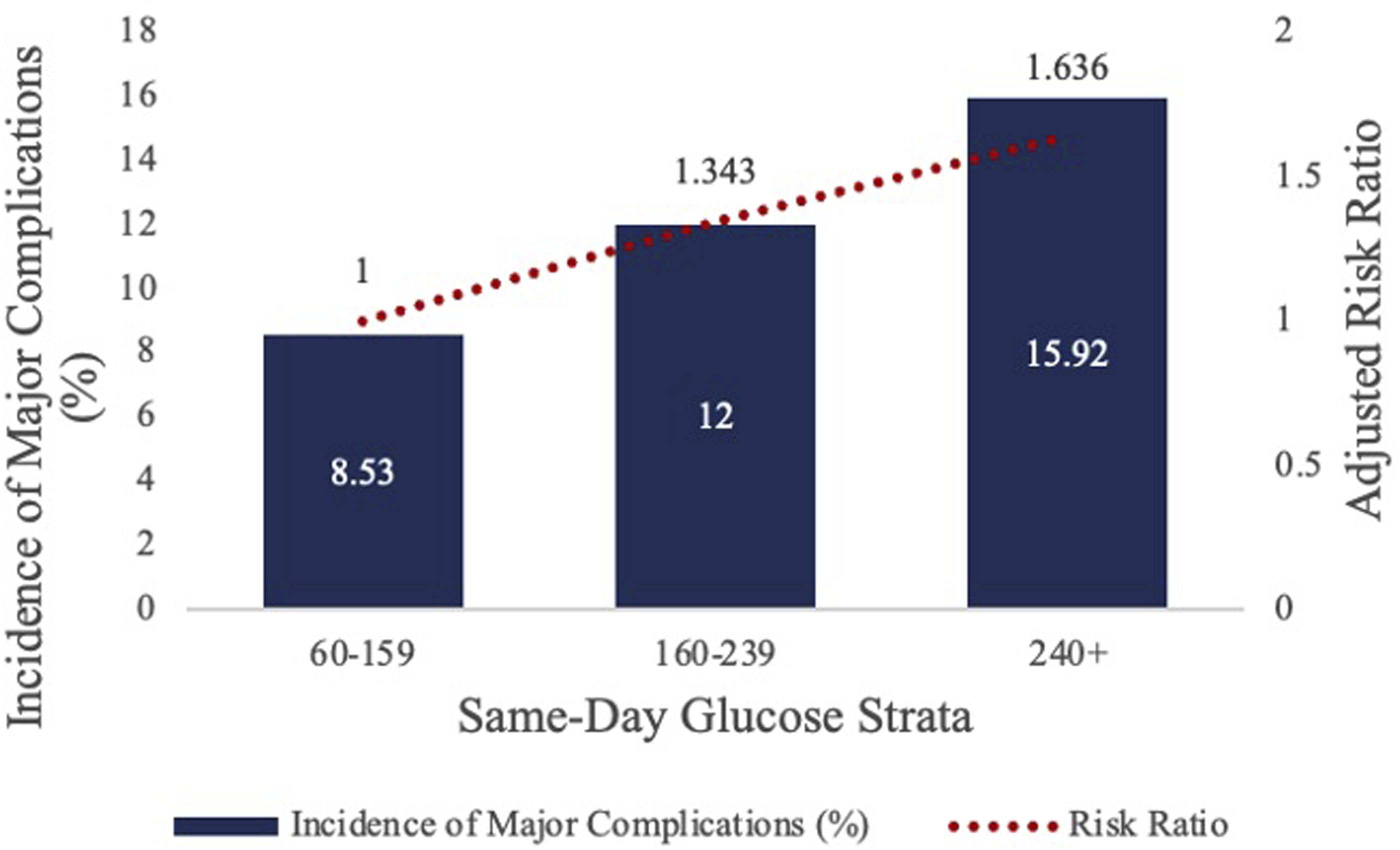
SSLR analysis identified 3 data-driven SDG strata (60-159, 160-239, and 240+) that predicted 90-day major complications. The patients with SDG values between 60-159 were determined to have the baseline risk profile and therefore were used as controls for further statistical analysis. Prior to propensity matching, unmatched SDG patient cohorts had the following patient counts: 60-159 (n = 7035), 160-239 (n = 3785), and 240+ (n = 1099).
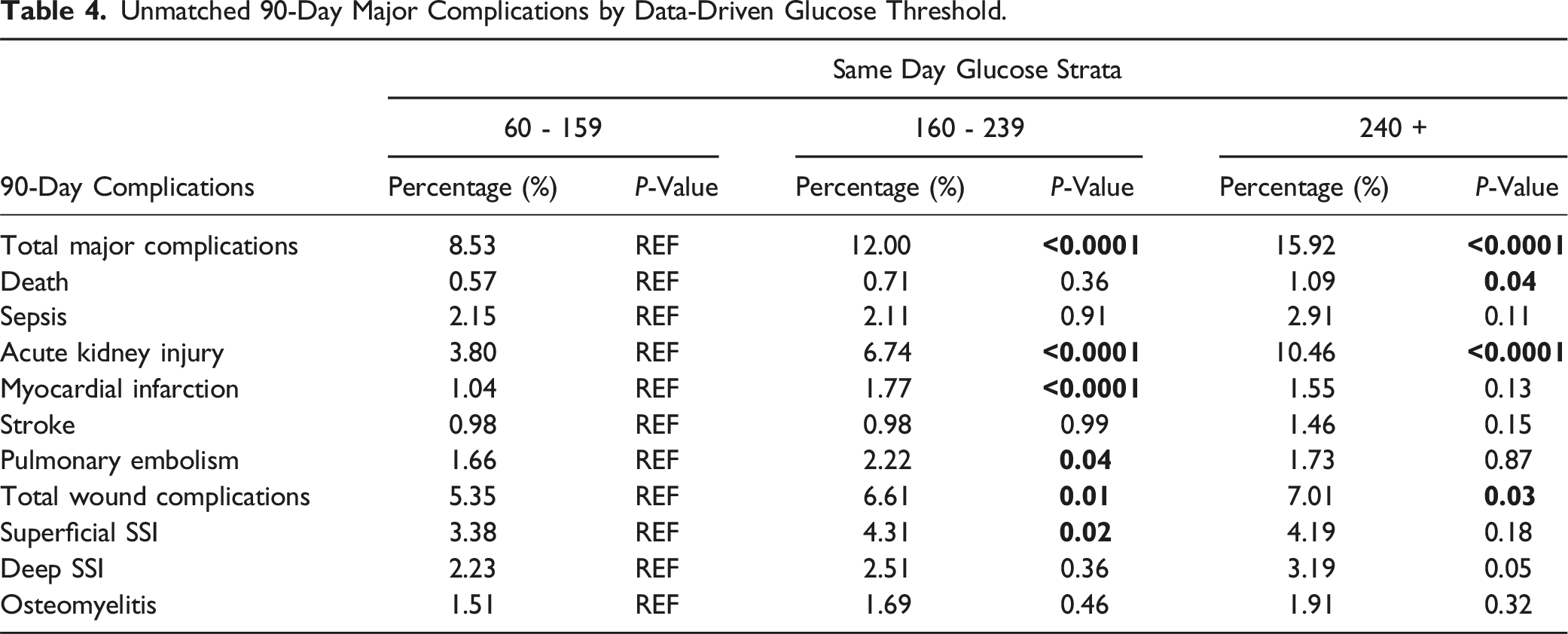
Unmatched 90-Day Major Complications by Data-Driven Glucose Threshold.
Matched 90-Day Major Complications by Data-Driven Glucose Threshold.
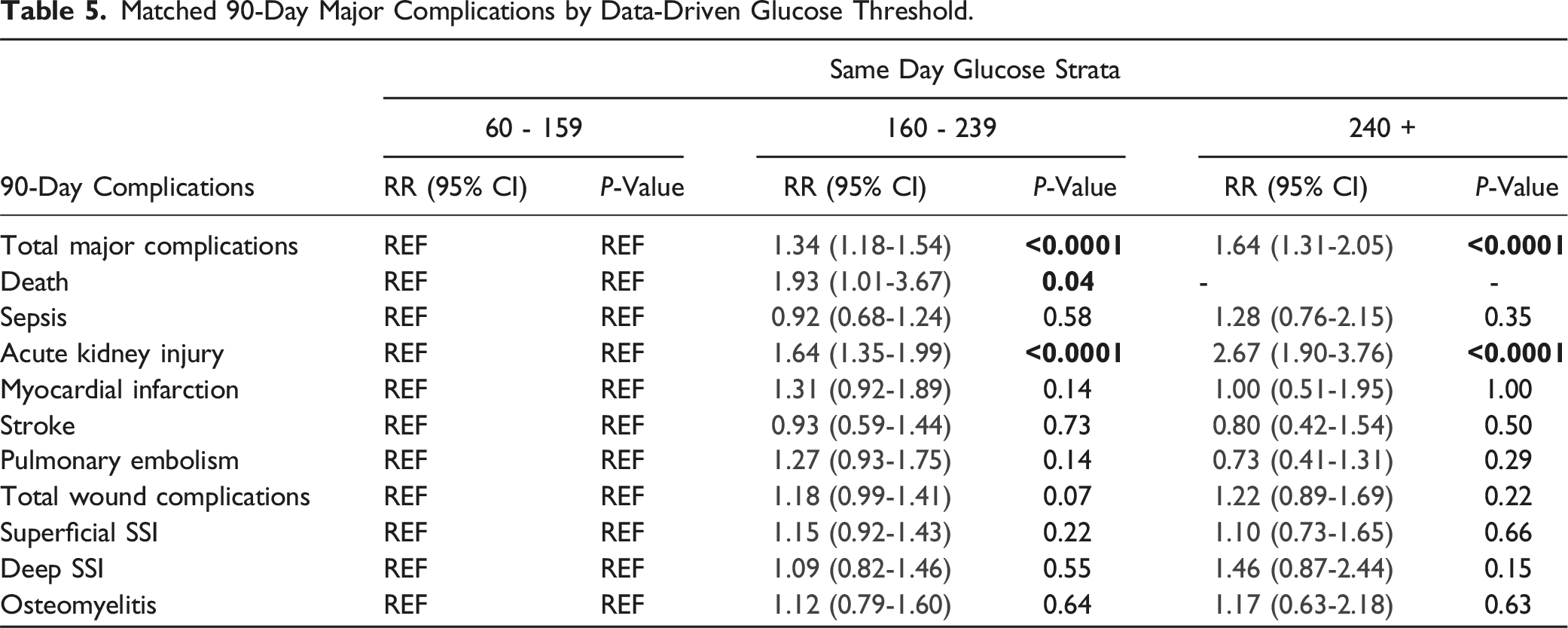
Additionally, SDG and HbA1c were statistically significant predictors of acute kidney injury (AKI) when the data-driven strata were compared. When propensity-matched to the lowest strata (60-159), the risk of 90-day AKI sequentially increased as the SDG strata increased: 160-239 (1.64; P < 0.001; 95% CI 1.35,1.99), 240+ (2.67; P < 0.001; 95% CI 1.90, 3.76). Similarly, for HbA1c, when propensity-matched to the lowest strata (4.5-5.4), the risk of 90-day AKI sequentially increased as the SDG strata increased: 5.5-7.9 (1.77; P = 0.009; 95% CI 1.15, 2.74), 8.0+ (2.74; P < 0.001; 95% CI 1.64, 4.56) (Tables 3 and 5).
SSLR was unsuccessful in identifying any HbA1c or SDG strata using the initial 90-day wound complication rates that predicted significant differences in 90-day complication rates. Therefore, no unmatched or matched analysis was able to be performed using 90-day wound complication rate generated strata (Figures 3 and 4). Data-Driven HbA1C Strata on the Incidence and Relative Risk of 90-day Major Complications. Figure 3 depicts the results of the stratum specific likelihood ratio analysis on HbA1c and 90-day major complications following LF. The bar graph represents the incidence of 90-day major complications for each identified HbA1c strata while the overlaid line graph represents the relative risk of 90-day major complications for each HbA1c strata. Data-Driven Same-Day Glucose Strata on the Incidence and Relative Risk of 90-day Major Complications. Figure 4 depicts the results of the stratum specific likelihood ratio analysis on same-day glucose and 90-day major complications following LF. The bar graph represents the incidence of 90-day major complications for the 3 identified same-day glucose strata while the overlaid line graph represents the relative risk of 90-day major complications.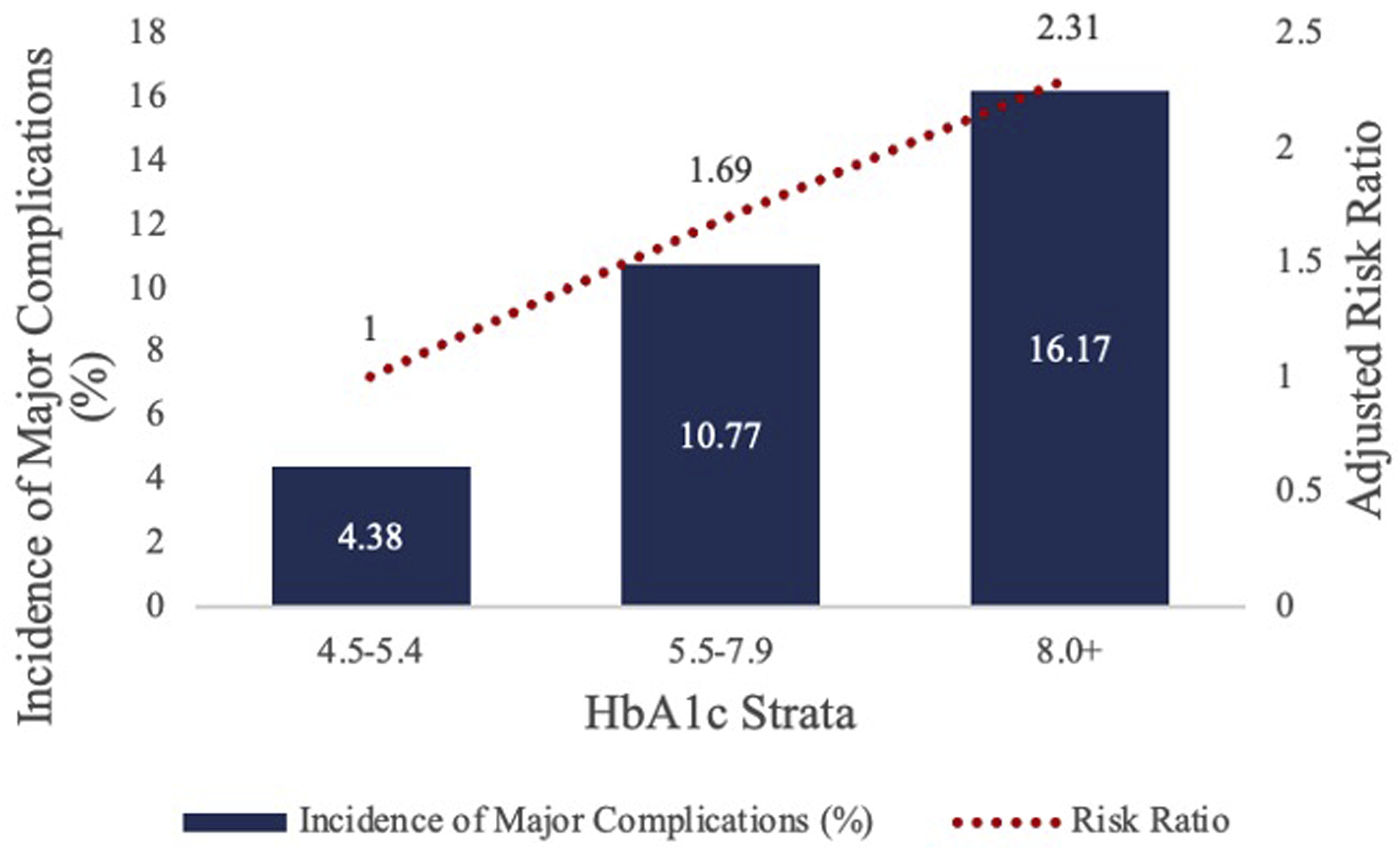
Conclusions
The purpose of this study is to generate data-driven preoperative HbA1c and SDG stratifications using SSLR analysis. Our study identified 3 HbA1c strata (4.5-5.4, 5.5-7.9, and 8.0+) and 3 SDG strata (60-159, 160-239, and 240+) that maximized the differences in the likelihood of 90-major complications following LF. This finding supports our hypothesis and suggests that a single cut-off value for both HbA1c and SDG as identified in prior literature may not be the most accurate way to assess risk for postoperative 90-day major complications. This has previously been successfully performed in total hip arthroplasty but the study determined different strata. 17 This emphasizes the importance of creating specific strata for procedures, as different surgeries have different risks, thus affecting the strata.
When compared to the HbA1c 4.5-5.4 cohort, the HbA1c 5.5-7.9 cohort had a statistically significant increase in risk for 90-day major complications. A study by Guzman et al. 15 found that uncontrolled DM was a significant independent predictor of in-patient mortality following lumbar spine surgery, and also increased risk of postoperative respiratory, cardiac, thrombotic, genitourinary, infectious, and hemorrhagic complications. However, these findings were correlated to ICD-9 coding for diabetic glycemic control, giving a less quantitative measurement than HbA1c, as used in our study. A study by Lim et al, 12 used HbA1c as an indicator for glycemic control in the perioperative period of lumbar spine surgery in 4778 patients. The study used an HbA1c cut-off of 8.0, based on prior literature unspecific to lumbar spine surgery, as the measure of glycemic control, with measurements above 8.0 indicating poor control.23-25 Lim et al. 12 found that patients with an HbA1c greater than 8.0 had an increased risk for major complications following lumbar spine surgery compared to patients with HbA1c values less than 8.0, similar to the findings of our study. However, we expand the existing literature by identifying statistically significant differences in 90-day major complication risks for 3 data-driven strata for HbA1c values specific to LF surgery. No prior studies have documented the comparatively increased risk in patients with HbA1c levels in the range of 5.5-7.9 vs the lowest strata of 4.5-5.4. The identification of 3 significant strata indicates that a single threshold for HbA1c may not be a reliable predictor of 90-day major complications following LF surgery.
Our study suggests that SDG levels can be used to stratify patient risk for 90-day major complications following LF procedures, as patients with SDG above 240 had the highest risk, and patients with SDG between 160 and 239 still had an increased risk when compared to those below 159. Current literature has established that poor glycemic control increases risk for postoperative complications, however, it is limited by lack of specificity to LF surgery, little exploration of post-operative complications beyond SSI, and the absence of quantitative stratification based on SDG values. A study by Zhuang et al., 26 found that poor glycemic control was associated with increased risk of pneumonia, urinary tract infection, AKI, pulmonary embolism, and need for a blood transfusion following LF. However, their study used ICD-9 coding, providing no quantitative information for stratifying risk based on SDG values. Further review of prior literature yields that preoperative hyperglycemia outside of the realm of spinal surgery increases the risk for pulmonary embolism, 27 morbidity, 28 mortality, 29 pneumonia, 30 renal failure, 30 and SSIs.3,31 The American Diabetes Association recommends perioperative blood glucose levels between 100 and 180 in the perioperative period for all surgeries to decrease risk for mortality and post-operative complications. 32 One important aspect of perioperative glycemic measurements to note is that unnecessarily low SDG values put diabetic patients at risk for a hypoglycemic episode during operations due to prolonged fasting.32-34 Therefore, due to the risks of both high and low levels of serum glucose, careful management of peri-operative serum glucose levels is of great importance.
When propensity matched, our analysis showed the 3 data-driven strata were not significantly different in 90-day wound complications using HbA1c or SDG cutoffs. We did find statistical significance when comparing patients with HbA1c levels of 4.5-5.4 vs 8.0+ . However, the lack of significance between the 4.5-5.4 and 5.5-7.9 groups when propensity matched prevents us from determining that HbA1c can be used to risk stratify patients into more than 2 distinct categories for 90-day wound complications following LF surgery. For SDG, when compared to the lowest strata of 60-159, levels of 160-239 or 240+ did not have a significantly increased risk for superficial SSI, deep SSI, or osteomyelitis within 90 days of LF surgery. Hikata et al, 10 found that perioperative hyperglycemia, defined as serum glucose >125 pre-operatively or >200 post-operatively, did not increase risk for SSI following thoracic or lumbar spinal surgery but that a HbA1c > 7 did have a significantly increased risk for SSI. Notably, their study population included a total of 39 patients with DM, while our study utilized a total of 12,026 patients, which could have potentially accounted for our differing HbA1c cutoff values of 7 vs 8 and conclusions concerning perioperative hyperglycemia. Alternatively, a study by Lim et al., 12 found no significant increase in risk for SSIs when comparing patients undergoing lumbar spine surgery based on a HbA1c cutoff value of 8.0, agreeing with our conclusions. However, many studies do declare a positive association between HbA1c values and risk for SSI. One such study, by Cancienne et al., 35 found that a preoperative HbA1c level of 7.5+ increased a patient’s risk for deep SSI following single-level lumbar decompression. However, our study used a stricter definition of wound complications and a shorter postoperative period of 90-days while Cancienne included all SSI’s and inflammation occurring within 1 year. Concerning SDG as a predictor of SSI, the findings of our study and those of Hikata et al, contradict prior literature and the consensus of increased risk for SSI in patients with perioperative hyperglycemia. One such study, by Upadhyaya et al. 36 found that in 3664 patients, serum glucose values >140 following spinal fusion surgery were associated with a more than 2-fold increase in risk for revision surgery due to infection. Potential reasons for the differing results include their broader definition of a SSI, and that the mean time to infection for their patient cohort was 147 days, while our study only included SSIs occurring within 90-days of LF surgery. Therefore, their study provides information on longer-term risk for SSI, while we provide data on the development of SSI more closely following LF surgery. Additional studies have found higher rates of SSI’s in diabetic patients following orthopedic surgery, however, these studies either did not analyze SDG values or are non-specific to LF surgery.2,15,26,37-39
An additional finding of our study was that elevated HbA1c and SDG values were statistically significant predictors of 90-day AKI following LF. After propensity matching, both HbA1c and SDG displayed increasing risk for AKI when comparing all 3 cohorts for each measurement. This finding is supported by Zhuang et al as they 26 similarly concluded that patients with uncontrolled DM had an increased risk for AKI following LF when compared to patients with well controlled diabetes. However, Zhuang et al utilized ICD-9 codes rather than quantitative values of glycemic measurement. Therefore, our study allows for more optimized and accurate perioperative risk assessment by providing specific HbA1c and SDG values for risk stratification.
Limitations of our study are largely related to the nature of large database analyses. We used the TriNetX database which provided us the ability to include 12,026 patients undergoing LF surgery that had documented HbA1c values within 3 months of the operation or a SDG the day of the operation. The use of numerical values (ie, a continuous variable) allowed us to avoid potential variations in classifying glycemic management between clinical sites as this is a limitation of previous studies that used ICD codes for their analysis. Additionally, we were able to use these values to identify data-driven strata that maximized differences in risk for 90-day major complications and 90-day wound complications. However, the nature of large database queries limited our ability to discern the reliability of certain data points such as the SDG levels, including the timing of when the SDG labs were drawn. As such, 1 major limitation of our study is the grouping of pre-operative and post-operative measurements of serum glucose values. As previous studies24,33,40,41 have shown, pre-operative and postoperative serum glucose measurements have different threshold values for predicting complications. This may have contributed to our study’s finding of no statistical significance between SDG strata and risk of SSI, as prior literature supports a positive association between the 2 variables. An additional aspect of the database analysis that limits our study is that patients with extremely high HbA1c or SDG values may have been discouraged from LF surgery. This possibility could limit our data set to a smaller cohort of patients with poor glycemic control, thereby causing an underestimation of the association between high SDG and HbA1c values and 90-day postoperative major and wound complications. Database analysis makes our findings highly generalizable as a large number of patients were included in each cohort across a number of clinical sites. Future studies should continue to refine the SDG and HbA1c thresholds, identified in this paper, for risk stratification of major complications and wound complications following LF surgery. Additional avenues for future investigation include additional SSLR analyses using immediate preoperative HbA1c values, propensity-matching for smoking, and exploring the relationships of immediate preoperative, intraoperative, and postoperative glucose levels with post-operative complications.
Conclusion
Using a national database, we were able to identify 3 data-driven strata for HbA1c (4.5-5.4, 5.5-7.9, and 8.0+) and SDG (60-159, 160-239, 240+)) that maximized the difference in risks for 90-day major complications but not 90-day wound complications in LF patients. The multiple strata identified for HbA1c and SDG levels demonstrate that single cut-off values as identified in prior literature may not be ideal for preoperative management of patients with poor glycemic control. Rather, risk stratification incorporating our multiple HbA1c and SDG strata with other parameters may be a better approach to preoperative risk stratification and counseling for 90-day major complications following LF in patients with poor glycemic control. Future studies can incorporate these LF-specific strata into risk calculators to predict the risk of 90-day major complications.
Footnotes
Author Contributions
Chloe Farnham: Wrote and revised the manuscript; prepared the manuscript for submission. Ivan Liu: Conceived and designed the study; conducted the data analysis and interpretation; contributed to the manuscript drafting and revision. Amil Agarwal: Assisted with the study design; contributed to the interpretation of results; contributed to the manuscript drafting and revision. Philip Parel: Contributed to the design of the study; assisted with manuscript drafting and revision. Theodore Quan: Contributed to the design of the study; assisted with manuscript drafting and revision. Wesley Durand: Contributed to the design of the study; assisted with manuscript drafting and revision. Amit Jain: Contributed to the design of the study; provided clinical insights and expertise; provided oversight and critical review of the manuscript. All authors made significant contributions to this work and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.