
Abstract
Study Design
Retrospective chart review.
Objectives
Transforaminal lumbar interbody fusion (TLIF) via open or minimally invasive (MI) techniques is commonly performed. Mobile applications for home-based therapy programs have grown in popularity. The purpose of this study was to (1) compare patient-reported outcome measures (PROMs) between postoperative patients who were the most and least compliant in using the mobile-based rehabilitation programs, (2) compare PROMs between open vs MI-TLIF cohorts, and (3) quantify overall compliance rates of home-based rehabilitation programs.
Methods
A retrospective chart review was performed. Patients were automatically enrolled in the rehabilitation program. Patient-Reported Outcomes Measurement Information System (PROMIS) and Oswestry Disability Index (ODI) scores were collected. Patients were separated into two study groups. Compliance rate was calculated as the difference between the number of active participants at the preoperative phase and final follow-up.
Results
220 patients were included. Average follow-up time was 23.2 months. No difference was found in the change in (∆) PROMIS scores (P = 0.261) or ∆ODI scores (P = 0.690) regardless of patient compliance. No difference was found in outcome scores between open vs MI-TLIF techniques stratified by download compliance (downloaded, DL+; did not download, DL-) and phone reminder compliance (set reminder, R+; did not set reminder, R-) postoperatively. Both cohorts demonstrated clinical improvement exceeding minimal clinically important difference at final follow-up. Overall patient compliance was 71% at final postoperative follow up.
Conclusion
Despite high long-term compliance and rising popularity, mobile applications for home-based postoperative rehabilitation programs have low clinical utility in patients undergoing TLIF.
Keywords
Introduction
Lumbar radiculopathy is a prevalent pathology, with reported incidence rates of 4.86 per 1000 person-years. 1 While conservative management resolves many cases, surgical intervention becomes essential for those who do not improve with non-surgical options. 2 Lumbar interbody fusion (LIF) is a well-established spinal procedure for the treatment of degenerative lumbar pathologies. 3 The transforaminal lumbar interbody fusion (TLIF) has been shown to be an effective LIF technique. 2 Currently, common approaches when performing TLIFs include the open or the minimally invasive (MI) approach. 3
Postoperatively, therapy and rehabilitation are commonly employed. Despite the increasing prevalence of lumbar fusion, there is limited data describing optimal protocols for rehabilitation efforts utilizing therapy.4-6 Additionally, the use of mobile applications (apps) for home-based therapy programs following orthopaedic procedures has been gaining popularity, without robust evidence demonstrating benefits of such programs when treating patients following TLIF. 7 Use of smartphone app-based remote rehabilitation has been employed for other orthopaedic procedures, including total knee and hip arthroplasty, demonstrating favorable results in such procedures.8,9 This may be a promising finding, specifically for medically underserved populations such as those in rural areas with a distinct lack of physical therapists, as this may provide extended access to postoperative therapy. 10 Additionally, the use of a mobile app rehabilitation program could help lower costs related to physical therapy when treating lower back pain, which is associated with increased costs per patient. 11 However, there is limited data describing the utility and compliance with such self-directed programs and its effects on patient-reported outcome measures (PROMs) following TLIF. Investigating the effects of an app-based physical therapy on PROMs could offer valuable insights to guide physicians in optimizing patient outcomes.
The purpose of this study was to (1) compare PROMs between patients who were the most compliant in utilizing the at-home therapy app and those who were the least compliant in utilizing the at-home therapy app following transforaminal lumbar fusion, (2) compare patient propensity to utilize the at-home therapy application between open TLIF and MI-TLIF patient populations, and (3) quantify the overall compliance with home-based rehabilitation programs.
Methods
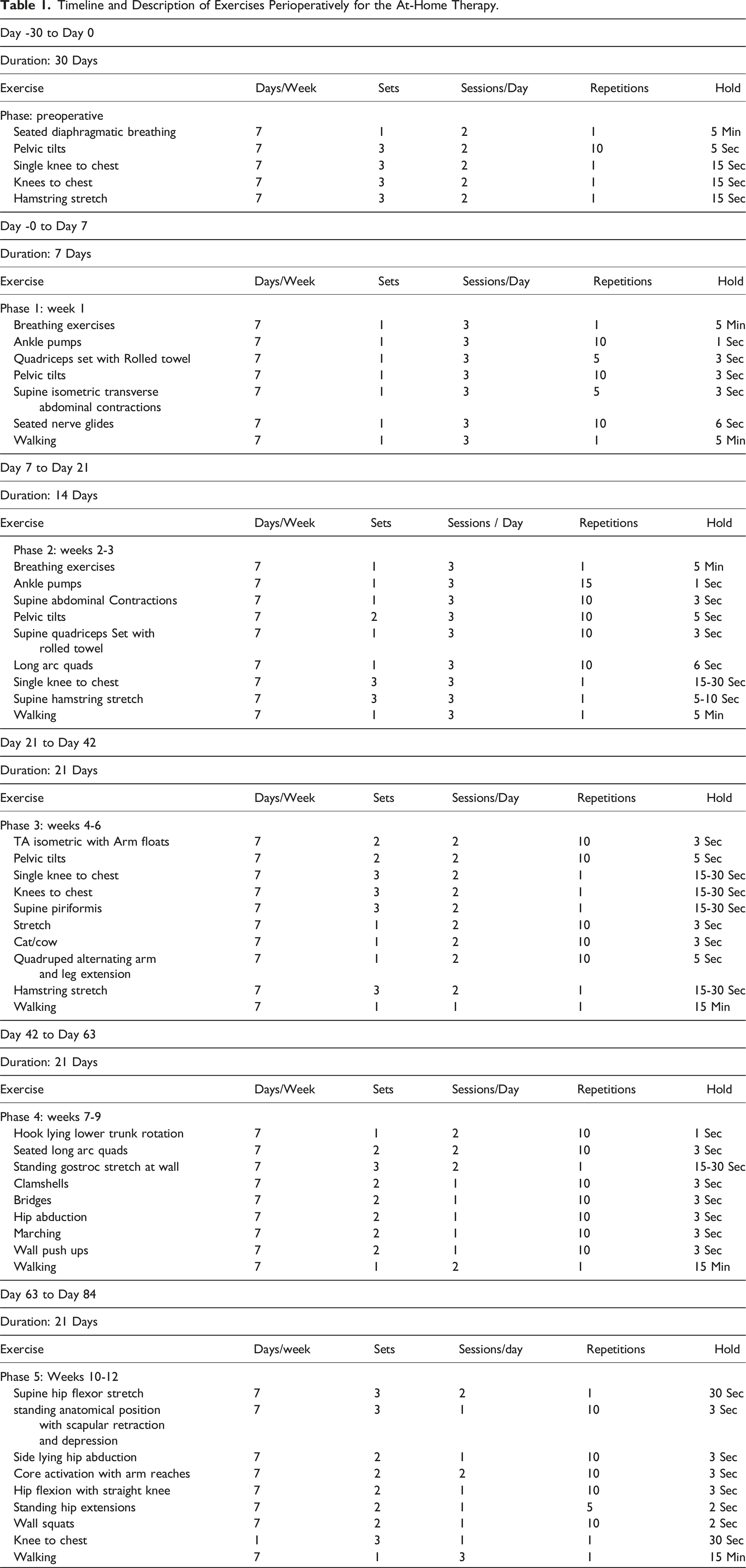
Description of at-Home Therapy Application
Timeline and Description of Exercises Perioperatively for the At-Home Therapy.
This was a retrospective cohort study performed at a large rural healthcare system including a continuous series of surgical patients. Patient consent was not directly obtained, rather, response to voluntary outcome measures implied consent for research inclusion. This study was exempt from review by the institutional review board. Patients who underwent one- or two-level TLIF or MI-TLIF between November 2019 and April 2023 with a preoperative diagnosis of spondylolisthesis, lumbar spinal stenosis, severe degenerative disc disease, facet arthropathy, or pars defect were included in the review. Exclusion criteria included patients with greater than two-level fusions, previous lumbar instrumentation or fusion, lumbar spine trauma or spinal tumors.
Postoperatively, all patients underwent routine standard of care follow-up. In addition, all patients received an email invitation to enroll in the digital home-based therapy program. Patients who accepted the invitation by downloading the application were considered download compliant (DL+) and those who enabled push-notification reminders were considered reminder compliant (R+). In addition to at-home therapy instructions, patients received in-app survey requests throughout the post-operative period to complete PROM collection. Completion of in-app surveys served as a surrogate for at-home compliance with the physical therapy protocol.
Patients were separated into two study groups for comparison based on application compliance and surgical technique. Patient-Reported Outcomes Measurement Information System (PROMIS) and Oswestry Disability Index (ODI) were collected pre-operatively and at 6 weeks, 3 months, 6 months, and 12 months postoperatively. PROMIS is a validated ten question survey which measures subjective physical, mental, and social domains of health. 12 PROMIS Physical, Mental, and Overall scores were recorded, as well as a change in (Δ) PROMIS overall scores from preoperative to final follow-up. ODI is a validated subjective assessment of disability or function in activities of daily living. 13 ΔODI was also evaluated at final follow-up. Surgical technique was determined by reviewing the operative note of each patient.
Patient compliance was calculated as the percentage of respondents to the ODI and PROMIS questionnaires at each time point. Percent difference for compliance was calculated as the difference in PROMs at each time point compared to preoperatively.
Statistical analysis included group average and standard deviation calculations, student t-test, and ANOVA analyses between groups where applicable. All statistical analysis was performed using SPSS. 14 Statistical significance was determined as P-value less than or equal to 0.05.
Results
Patient Demographic and Mobile App Data by Surgical Technique.
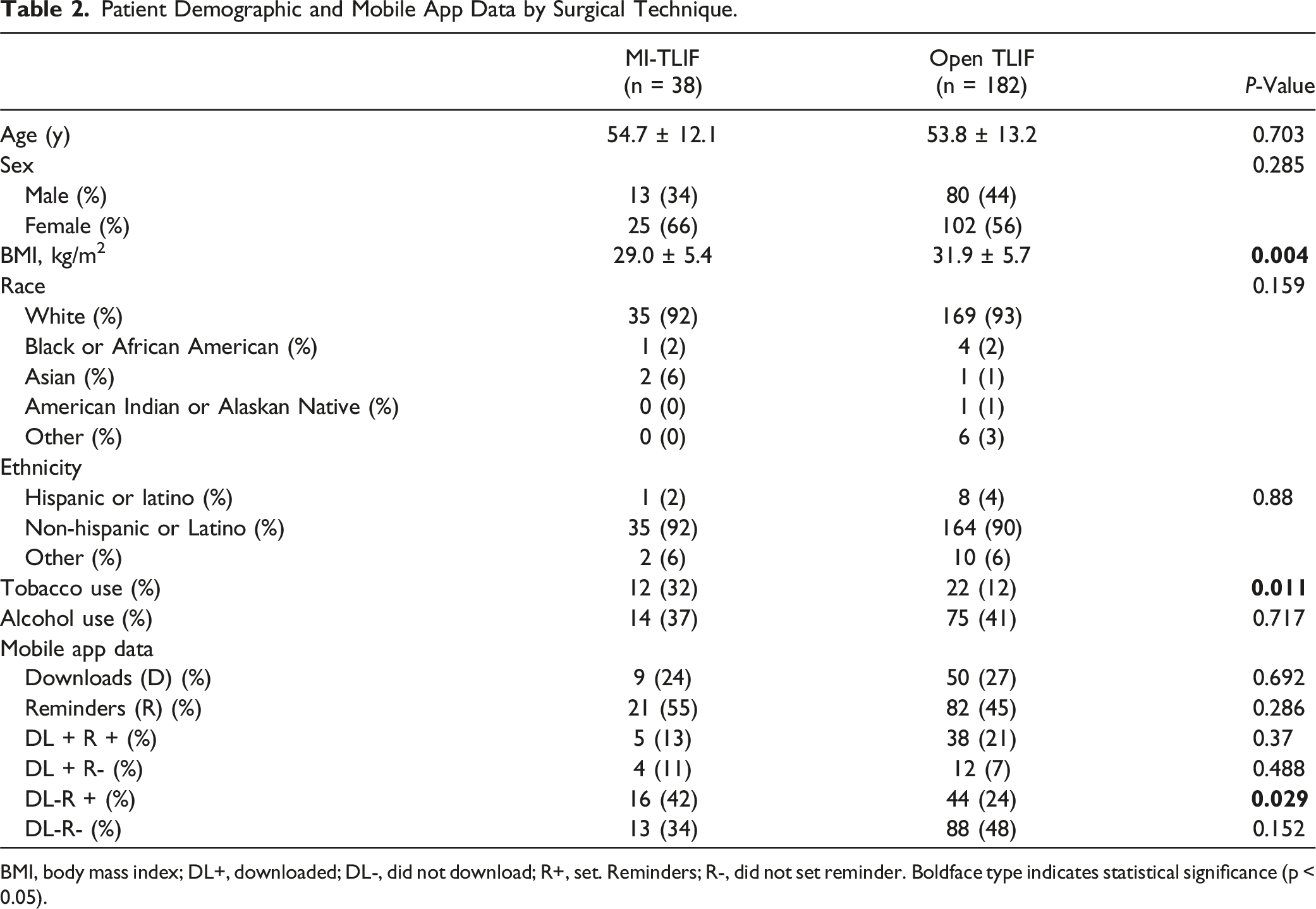
BMI, body mass index; DL+, downloaded; DL-, did not download; R+, set. Reminders; R-, did not set reminder. Boldface type indicates statistical significance (p < 0.05).
Difference in PROMIS or ODI Scores in MI- vs Open TLIF.
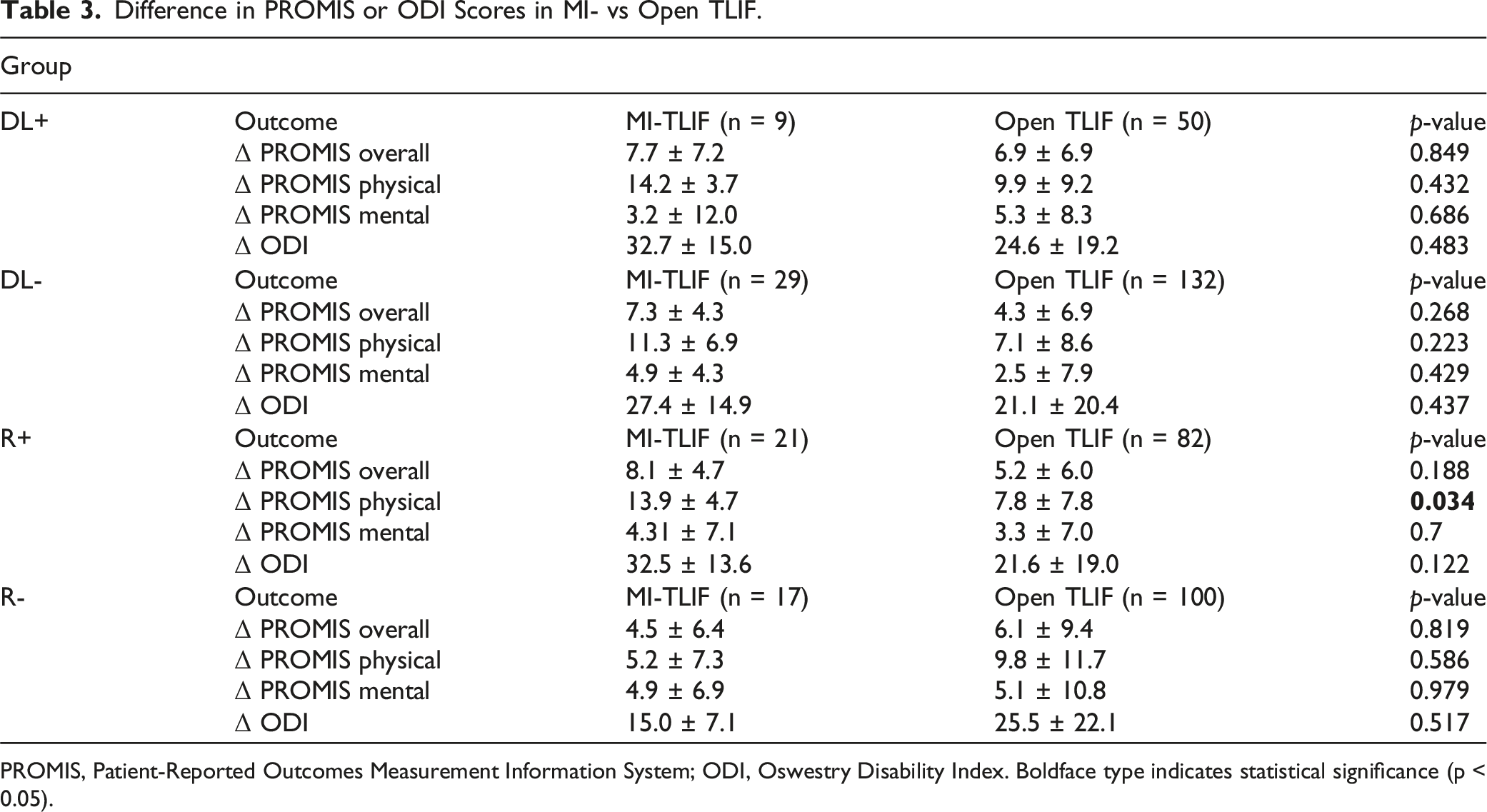
PROMIS, Patient-Reported Outcomes Measurement Information System; ODI, Oswestry Disability Index. Boldface type indicates statistical significance (p < 0.05).
There were no significant differences between ΔPROMIS overall for the DL + group (P = 0.849) or DL-group (P = 0.268), ΔPROMIS physical for the DL + group (P = 0.432) or DL-group (P = 0.223), and ΔPROMIS mental for the DL + group (P = 0.686) or DL-group (P = 0.429). There were no significant differences between ΔODI scores for the DL + group (P = 0.483), DL-group (P = 0.437), R+ group (P = 0.122), or R-group (P = 0.517) in the remaining subgroups.
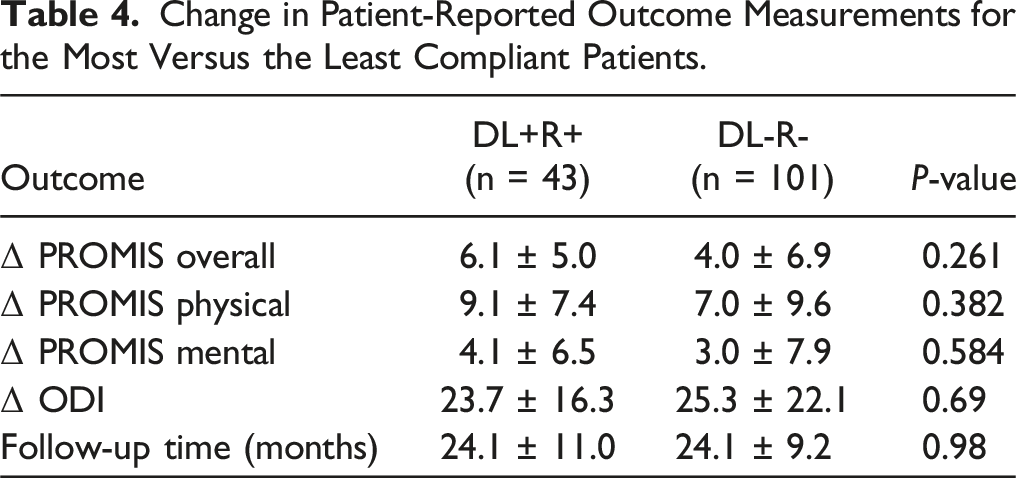
Change in Patient-Reported Outcome Measurements for the Most Versus the Least Compliant Patients.
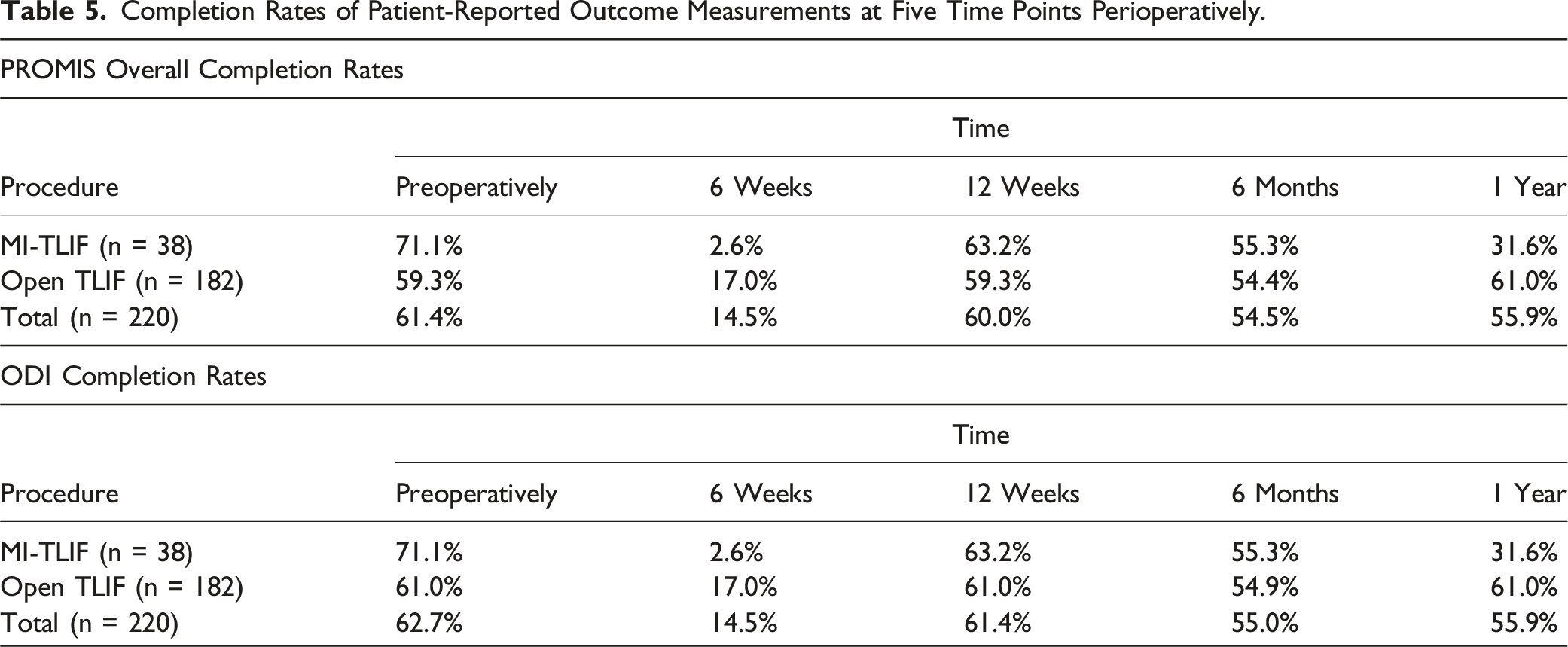
Completion Rates of Patient-Reported Outcome Measurements at Five Time Points Perioperatively.
Discussion
The use of technology in medicine is rapidly adapting and evolving. To optimize postoperative outcomes, it is vital for patients to undergo quality rehabilitation. This study aimed to determine the benefits of a mobile-based rehabilitation program on perioperative PROMs for the most vs least compliant patients and in patients undergoing open vs MI-TLIF Figure 1. Cohorts were divided into groups defined as DL + R+, DL + R-, DL-R+, or DL-R-. These divisions allowed for comparison between the most and the least compliant patients, as well as comparison of patients who were partially compliant. The divisions also offered subgroup analyses based upon compliance and surgical technique, providing information regarding the likelihood of patients undergoing open vs MI-TLIF to be compliant with a home-based rehabilitation program perioperatively. Flow chart describing an overview of the order and process of the study.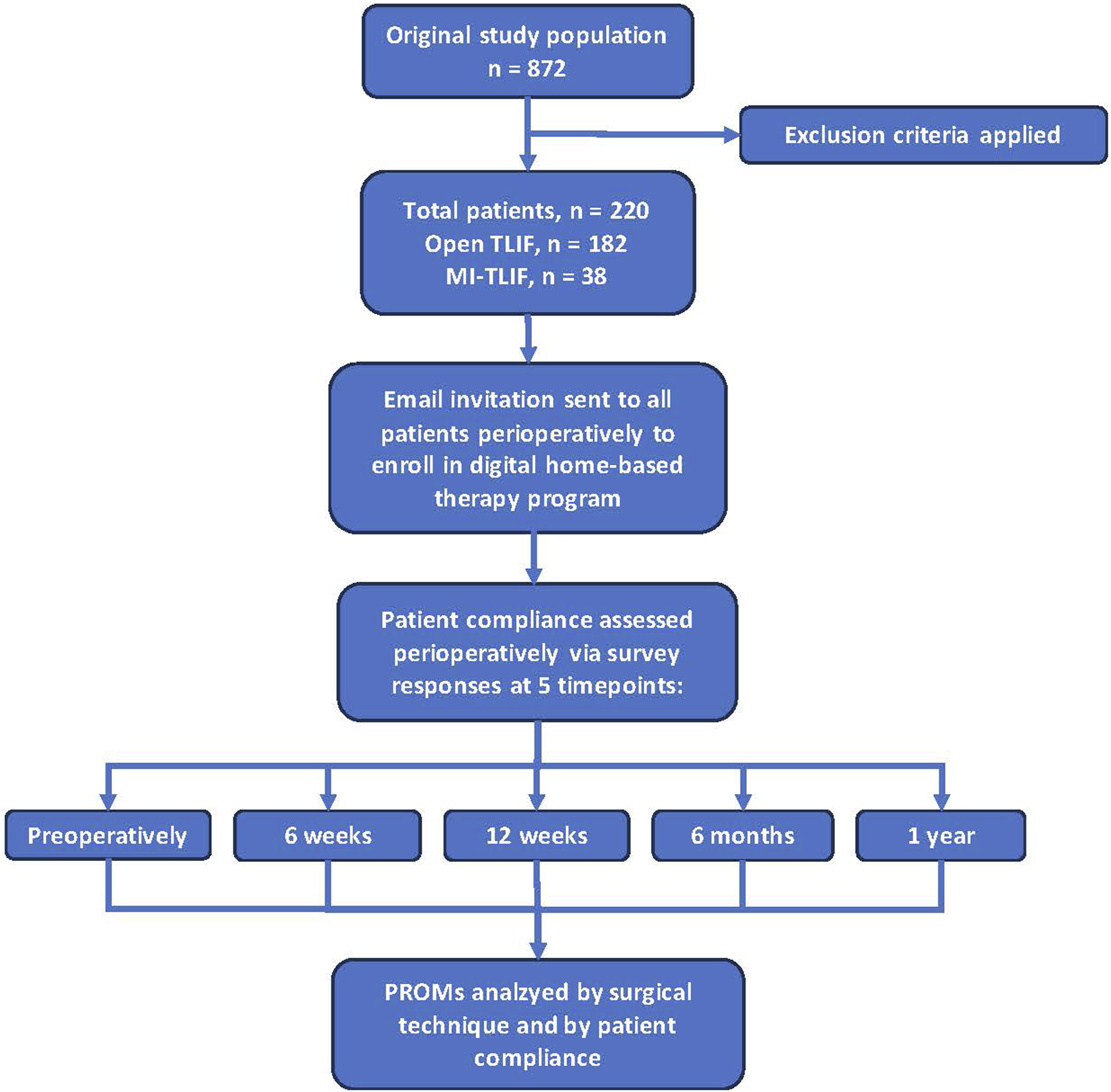
Our findings showed no differences between perioperative PROMs for open vs MI-TLIF and for the most vs the least compliant patients. Between the most compliant patients (DL + R+) and the least compliant patients (DL-R-), we found no significant differences in Δ PROMIS Overall, Δ PROMIS Physical, Δ PROMIS Mental, or Δ ODI scores perioperatively (Table 4). Therefore, an app-based perioperative rehabilitation program following spinal fusion may lack utility. Of note, our data describes a higher patient engagement postoperatively compared to previous studies. One study examining patient engagement with a digital app following total knee and hip arthroplasty found that by 12 weeks postoperatively, patient engagement with the app was 30%. 15 The present study resulted in about 60% patient engagement at 12 weeks postoperatively (Table 5). Because adherence to an app-based rehabilitation program can be a significant barrier to proper postoperative recovery, patient compliance is vital. 16
Our study demonstrated that current smokers were significantly more likely to undergo MI-TLIF vs open TLIF (Table 2). While the present study did not compare PROMs for smoking patients vs non-smoking patients, the negative perioperative effects of smoking on orthopaedic procedures, such as wound dehiscence and pseudarthrosis, should be noted. 17 Because of the smaller operative wounds and quicker postoperative recovery, smokers may benefit from undergoing MI-TLIF, and as a result, may be more likely to report improved PROMs. 18 There may also have been a negative selection criteria for surgeons when opting to perform open vs MI-TLIF for the perioperative risk factors discussed. Therefore, the influence of smoking, surgical technique, and patient compliance to app-based rehabilitation should be examined.
It has been suggested that encouraging patients to become self-motivated and educated in their healthcare, such as with app-based rehabilitation programs, may decrease excessive emergency visits and lower costs.15,19,20 Alexander et al determined that the use of a smartphone-based care platform following primary knee arthroplasty resulted in significantly less visits to the emergency department. 21 With the increasing costs of ED visits, implementing such apps appears attractive. 22 App-based rehabilitation programs have been demonstrated to be a cost-saving intervention compared to traditional institutional-based rehabilitation programs in other medical specialties.23,24
While the app-based program could provide cost reductions, the present study determined that PROMs are not significantly improved with the use of a remote rehabilitation platform for TLIF patients in the perioperative period. Additionally, prior studies have demonstrated no significant differences of perioperative PROMs between open vs MI-TLIF surgical techniques, which is consistent with the findings presented here.18,25-27 Our findings indicate that surgical technique does not influence the PROMS for the most and the least compliant patients participating in the home-based therapy.
Therefore, an app-based rehabilitation does not appear to be effective at improving PROMs in TLIF patients. Notably, the present study only examined subjective outcomes while previous research has demonstrated improved objective metrics for patients participating in postoperative therapy, such as walking distance, lumbar muscle strength, trunk extension, and lateral flexion.28-30 Examination of objective measurements for this home-based rehabilitation program should therefore be explored.
Importantly, there is no consensus amongst spine surgeons or physical therapists concerning the utility of rehabilitation protocols following spinal fusion and current literature remains conflicting. 4 For instance, a randomized controlled trial from 2013 examining the timing of rehabilitation following lumbar spinal fusion either 6 or 12 weeks postoperatively demonstrated no significant difference in functional outcomes such as walking distance and fitness. 31 However, a 2017 systematic review determined some superiority of initiating rehabilitation at 12 weeks postoperatively vs an earlier 6 week start. 4 Still other studies have determined that early initiation (as early as 3 weeks postoperatively) can provide benefits following lumbar spinal fusion.28,32 A systematic review from 2016 determined self-reported improvements up to 12 months postoperatively for patients who participated in rehabilitation following lumbar spinal fusion. 33 Lack of high level prior evidence supporting postoperative therapy, timing of therapy, and long-term outcomes following therapy precludes the formation of reliable clinical practice guidelines.5,34
In addition, it is important to highlight the potential use of an app-based therapy in other contexts, such as in the setting of rural communities and for pre-habilitation. Use of remote rehabilitation programs have demonstrated a possible correlation between cost-saving and access to care through reducing barriers related to time and distance to rehabilitation. 35 As identifying healthcare inequity continues to be heavily examined, use of a remote-based therapy should be further investigated. Studies have also found that preoperative physiotherapy increases physical activity level in patients with degenerative lumbar spine disorders postoperatively.36,37 While there is no definitive pre-habilitation program to improve all outcome measures, there seems to be no negative effects of such efforts. 38 Therefore, utilization of this home-based program for pre-habilitation could be advantageous.
In large healthcare systems, the cost for enrollment per patient into the home-based rehabilitation app is approximately $200 USD. This provides access to all features of the app, including the exercise instructions, pain management, physical limitations, time-specific survey responses, and messaging capabilities with the patients’ care teams. When compared to the average cost for an in-person physical therapy program of $1000 USD, the home-based app could offer significant healthcare savings per patient, particularly at large healthcare systems where annual patient enrollment in the app may surpass 5000 patients. Given the low utility of the app based on our study’s findings, discontinuing its use within the healthcare system may significantly reduce costs associated with the app alone. However, removal of the app would likely also decrease ease of recording outcome measurements and may potentially increase net costs if in-person physical therapy use is then increased. More research and cost analyses are needed to determine the cost effectiveness of the home-based app therapy.
This study has several limitations; first, the metric for compliance to the physical therapy protocol is an indirect measurement. Although survey completion was only possible through the application interface, patients may have completed surveys without following the remaining daily therapy instructions. Additionally, specific patient support was not factored into the present study, such as competency of discharge information for caregivers within the home, which can significantly impact recovery for patients. 39 This study also had a disproportionate amount of open TLIF compared to MI-TLIF (182 vs 38, respectively) procedures, although MI-TLIF remains a less commonly performed procedure nationally. Future studies should incorporate a larger cohort of MI-TLIF. While several limitations exist, efforts to increase generalizability of the present study included multiple surgeons performing spinal fusions, blinded data collected and review, as well as including a continuous patient series.
In conclusion, long-term compliance to the home-based rehabilitation program was high. However, similar improvements in PROMs were found between patients regardless of therapy compliance. This suggests low utility of the home-based program following transforaminal lumbar interbody fusion amongst patients undergoing open and MI-TLIF. While remote health applications are rising in popularity, health systems should continue to evaluate the utility of providing such platforms to patients, particularly in the setting of rising healthcare costs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.