
Abstract
Study Design
Retrospective bicentric Cohort Study.
Objective
Posterior (PLIF) and transforaminal lumbar interbody fusion (TLIF) have been clinically proven for the surgical treatment of degenerative spinal disorders. Despite many retrospective studies, the superiority of either technique has not been proven to date. In the literature, the complication rate of the conventional PLIF technique is reported to be significantly higher, but with inconsistent complication recording. In this retrospective bicentric study, a less invasive PLIF technique was compared with the conventional TLIF technique and complications were recorded using the validated SAVES V2 classification system.
Methods
1142 patients underwent PLIF (702) or TLIF (n = 440) up to 3 levels in two specialized centers. Epidemiological data, intra- and postoperative complications during hospitalization and after discharge were analyzed according to SAVES V2.
Results
The overall complication rate was 13.74%. TLIF-patients had slightly significant more complications than PLIF-patients (TLIF = 16.6%/PLIF = 11.9%, P = .0338). Accordingly, complications during revision surgeries were more frequent in the first cohort (TLIF = 20.9%/PLIF = 12.6%; P = .03252). In primary interventions, the surgical technique did not correlate with the complication rate (TLIF = 12.4%/PLIF = 11.7%). There were no significant differences regarding severity of complications.
Conclusions
An important component of this work is the complication recording according to a uniform classification system (SAVES V2). In contrast to previous literature, we could demonstrate that there is not a significant difference between the two surgical techniques.
Keywords
Introduction
In particular, PLIF and TLIF are widely used and established procedures for the surgical management of degenerative instabilities and deformities of the lumbar spine.1,2
A significant increase (138%) in lumbar fusion surgeries was seen in those over 65 years of age in the United States between 2004 and 2015. Patients with degenerative spondylolisthesis made up the majority of the patient population (45.2% in 2015) and had the largest increase since 2004 (111%). 3
Although TLIF and PLIF are already compared in the literature, limitations often exist.4-6 Case numbers are predominantly small and complications are not evaluated according to an uniform scoring scheme.7,8 The inhomogeneous complication recording of many studies limits the comparability of the respective complications.
To date, only conventional PLIF techniques and not the less invasive PLIF techniques have been compared to the TLIF technique. With comparable clinical outcomes, the TLIF technique was considered the less complicated procedure compared to the PLIF technique. In 2017, De Kunder et al published the first systematic review and meta-analysis comparing PLIF and TLIF procedures in the treatment of degenerative spondylolisthesis. The PLIF complication rate of 17% was twice the TLIF complication rate of 8.7%, and neurologic complications in particular were significantly PLIF-associated. 4
Some studies have shown that TLIF patients generally benefit from shorter operative time, reduced blood loss, and shortened length of stay.7,9,10 Since the comparable clinical outcome does not support the clear superiority of either procedure, experience and surgeon preference determine the choice of surgical technique. 4
The aim of this study was to compare two cohorts of patients using retrospective registry data and to determine whether the higher complication rate reported in the literature for PLIF surgery compared to the TLIF technique is also confirmed for the more modern and less invasive, so-called mini-open PLIF technique.
Material and Methods
Patient Population and Clinical Data Collection
Patients from two spine centers were compared in a registry study. All patients with a fusion of 1 to 3 motion segments due to degenerative disc disease were included. Within an observation period of 3.5 years, a total of 1303 patients could be detected. All patients were prospectively recorded in a spine registry. Due to an additional anterior approach for interbody fusion, 161 patients were excluded, so that the data of 1142 patients could be evaluated.
The following perioperative parameters were retrospectively analyzed: Date of surgery, age at time of surgery, sex, ASA score, length of inpatient stay, surgical site, number of decompressed segments, number of fused segments, type and grade of spondylolisthesis grade, presence of central stenosis, presence of neuroforaminal stenosis, secondary diagnoses, primary/revision surgery, surgical technique (PLIF/TLIF), incision-suture time, radiographic duration, administration of blood transfusions, implant type (screw-rod system and cage), last outpatient readmission after index surgery, 30-day readmission rate.
In addition, all complications were recorded and evaluated according to the SAVES criteria (Spine Adverse Event Severity System by Rampersaud et al 11 ). Complications were recorded intraoperatively, during the inpatient stay and postoperatively during the outpatient follow-up.
All registered patients have given informed consent. The ethics vote from “Medical Association Hamburg” underlying this study has the number MC-108/16.
Complication Recording
SAVES-V2 Severity Grades (Rampersaud et al 11 ).
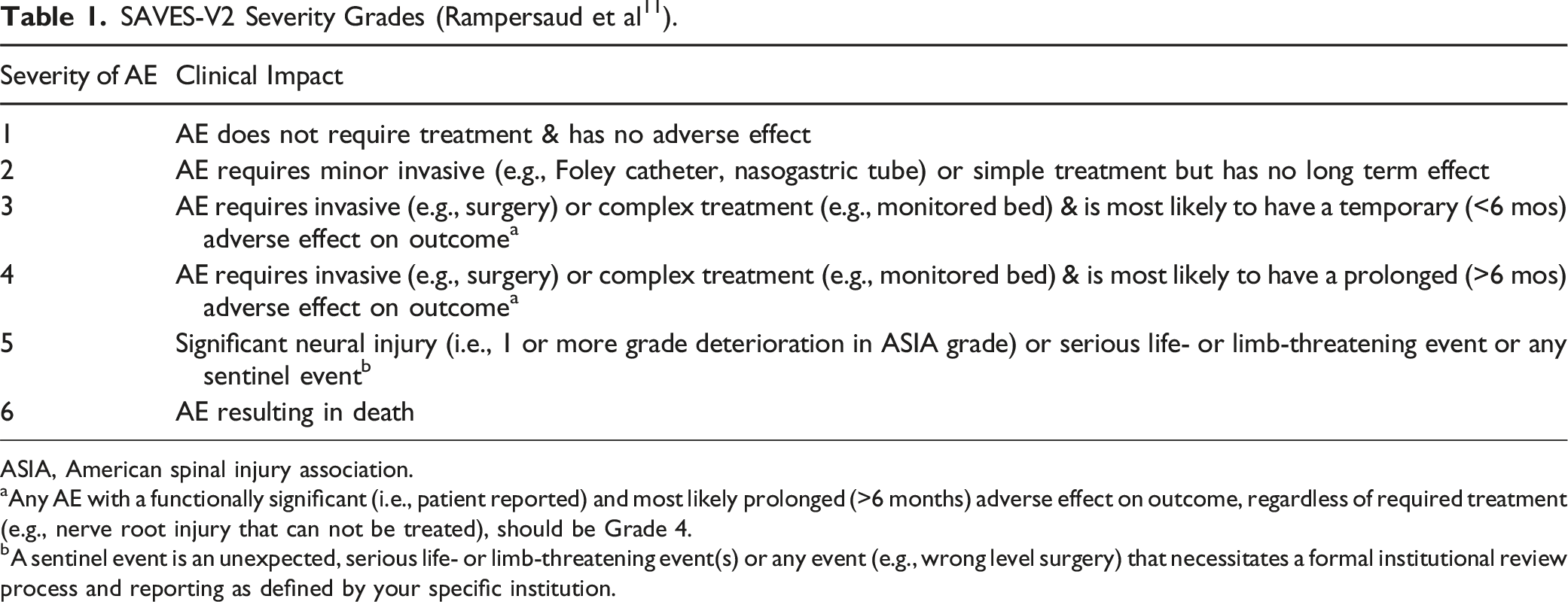
ASIA, American spinal injury association.
aAny AE with a functionally significant (i.e., patient reported) and most likely prolonged (>6 months) adverse effect on outcome, regardless of required treatment (e.g., nerve root injury that can not be treated), should be Grade 4.
bA sentinel event is an unexpected, serious life- or limb-threatening event(s) or any event (e.g., wrong level surgery) that necessitates a formal institutional review process and reporting as defined by your specific institution.
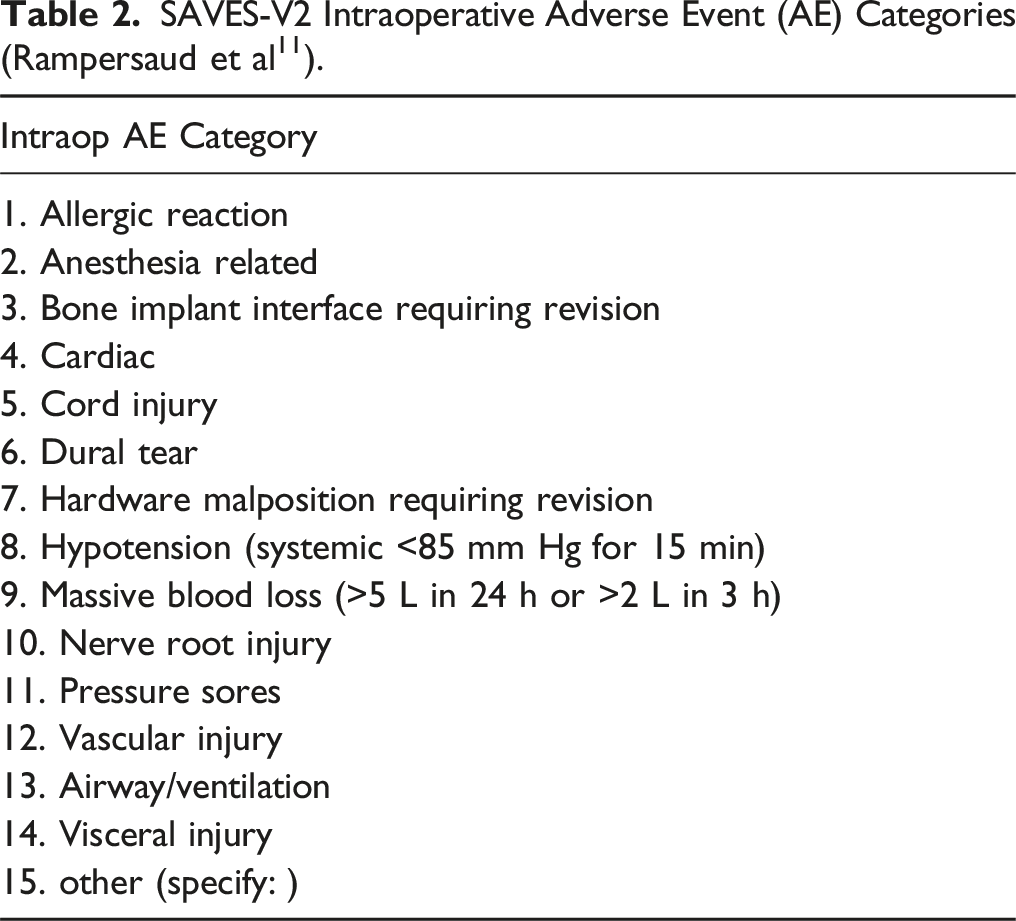
SAVES-V2 Intraoperative Adverse Event (AE) Categories (Rampersaud et al 11 ).
SAVES-V2 Postoperative Adverse Event (AE) Categories (Rampersaud et al 11 ).
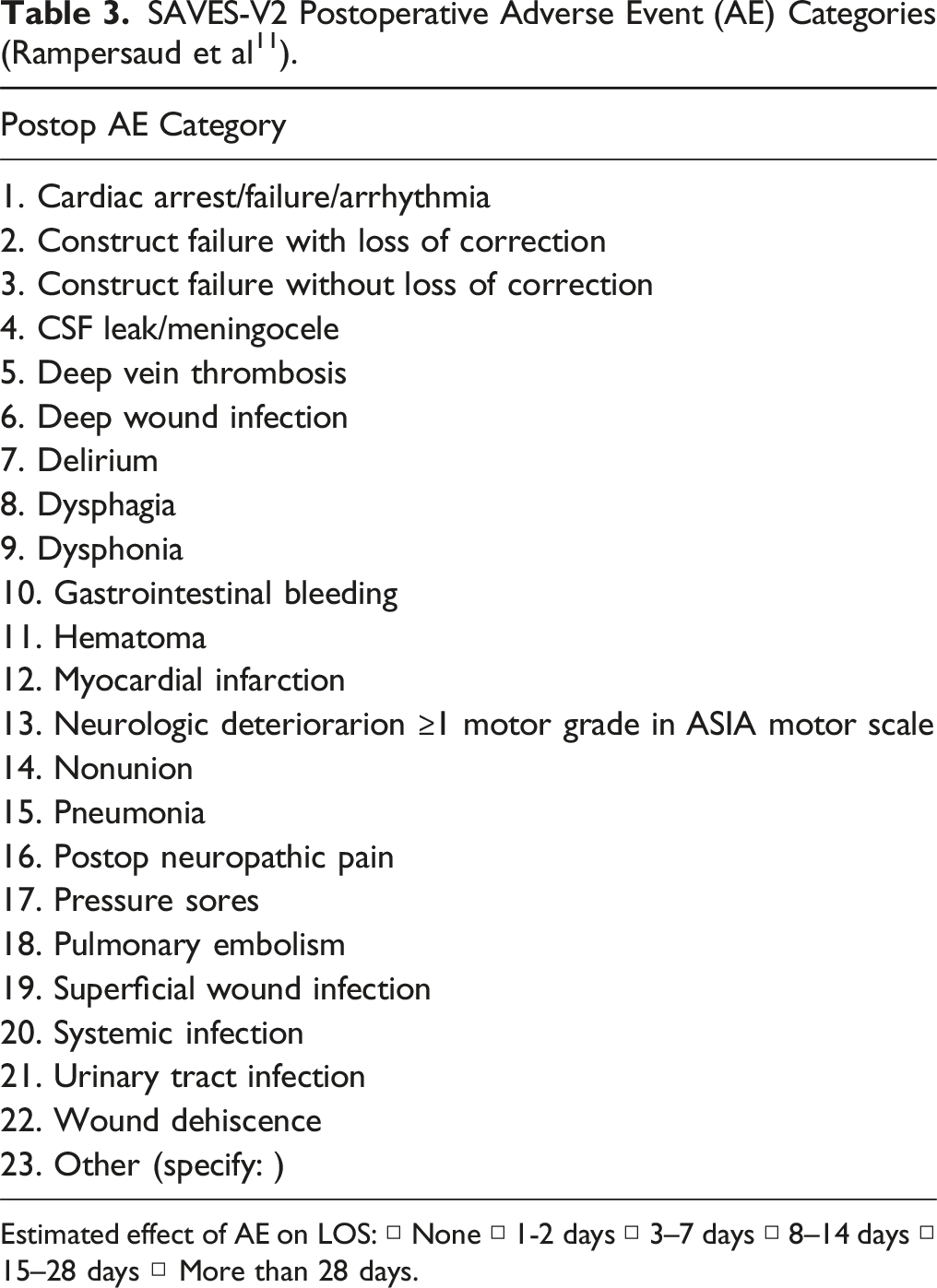
Estimated effect of AE on LOS: □ None □ 1-2 days □ 3–7 days □ 8–14 days □ 15–28 days □ More than 28 days.
Statistical Methods
Statistical data analysis was performed using the statistical program R for Mac (version 3.6.3). We used 5% as the significance level within the hypothesis tests, i.e., there was statistical significance as soon as the P-value was below .05. Descriptive data were presented using absolute and relative frequency, median, mean, standard deviation (SD), and range. A boxplot was used to graphically represent the distribution of results. As upper/lower whisker we defined a quartile + - 1.5x IQR (inter-quartile range).
For metric variables (e.g., ODI), we used the t-test to clarify whether differences in the mean were statistically significant. For binary variables (e.g., complication/no complication), we used Fisher’s exact test. For correlation analyses, Pearson’s correlation coefficient was calculated.
Surgical Techniques and Intervertebral Implants
Both surgical techniques were performed in standardized procedures. In the PLIF technique, a bilateral laminotomy with flavectomy and partial facet-joint resection was performed and two titanium-coated PEEK cages were inserted intervertebrally under flouroscopic control, which were filled with autologous bone chips. All surgical steps of preparation and cage insertion were carried out with the aid of a surgical microscope. Great attention was paid to the retraction of the muscles with Langenbeck hooks in order to avoid tissue damage in the access area. In the TLIF group, the facet joint was completely resected on one side and the decompression was completed contralaterally in a cross-over technique under microsurgical conditions as well. A “banana” titanium cage filled with autologous bone material was inserted centered in the ventral third intervertebrally and compressed dorsally via screw-rod instrumentation for lordosis in both techniques.
With regard to the first postoperative mobilization, the same standard of procedure was used in both groups. In principle, mobilization was permitted immediately after the anaesthetic had worn off. Mobilization under physiotherapeutic guidance was routinely performed within the first 24 h postoperatively. Only in case of the occurrence of a complication in the sense of a dural injury, prolonged postoperative bed rest required.
Results
Patient Cohort and Perioperative Measures
At the first center 702 patients were operated on using the PLIF technique and at the other center 440 patients using the TLIF technique. Of these, 297 (42%) were male and 405 (58%) were female in the PLIF collective and 193 (44%) were male and 247 (56%) were female in the TLIF collective. 745 patients (65.23%) had a first procedure (PLIF: n = 520: 74%/TLIF: n = 225: 51%). 397 patients (34.76%) were operated already (PLIF: n = 182: 26%/TLIF: n = 215: 49%).
Data-Basis of the Total Study Population.
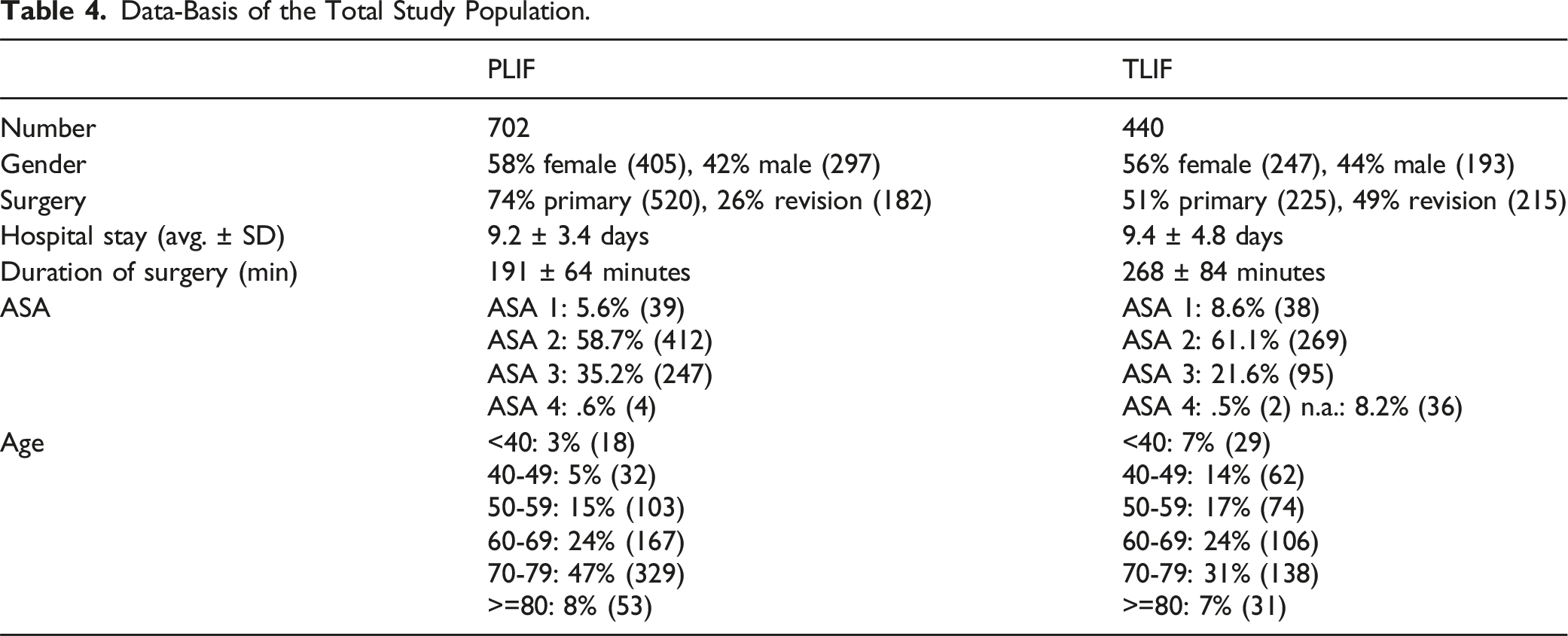
The number of decompressed segments ranged from 1 to 5 and averaged 1.42 in the entire study population (PLIF 1.40 levels/TLIF 1.45 levels). The number of fused segments ranged from 1 to 3 and averaged 1.25 in the entire study collective (PLIF 1.29 levels/TLIF 1.17 levels).
Duration of surgery was statistically significantly shorter in PLIF patients than in TLIF patients (191 min vs 268 min, P < .0001).
40 patients (3.50%) needed blood transfusions without differences between the two groups (PLIF: n = 20: 2.84%/TLIF: n = 20: 4.54%; P = .1387).
The median inpatient stay was 7.8 days for the PLIF group and 7.9 days for the TLIF group.
A graphical illustration is shown in Figure 1. Graphic illustration of the length of stay for the PLIF and TLIF procedure.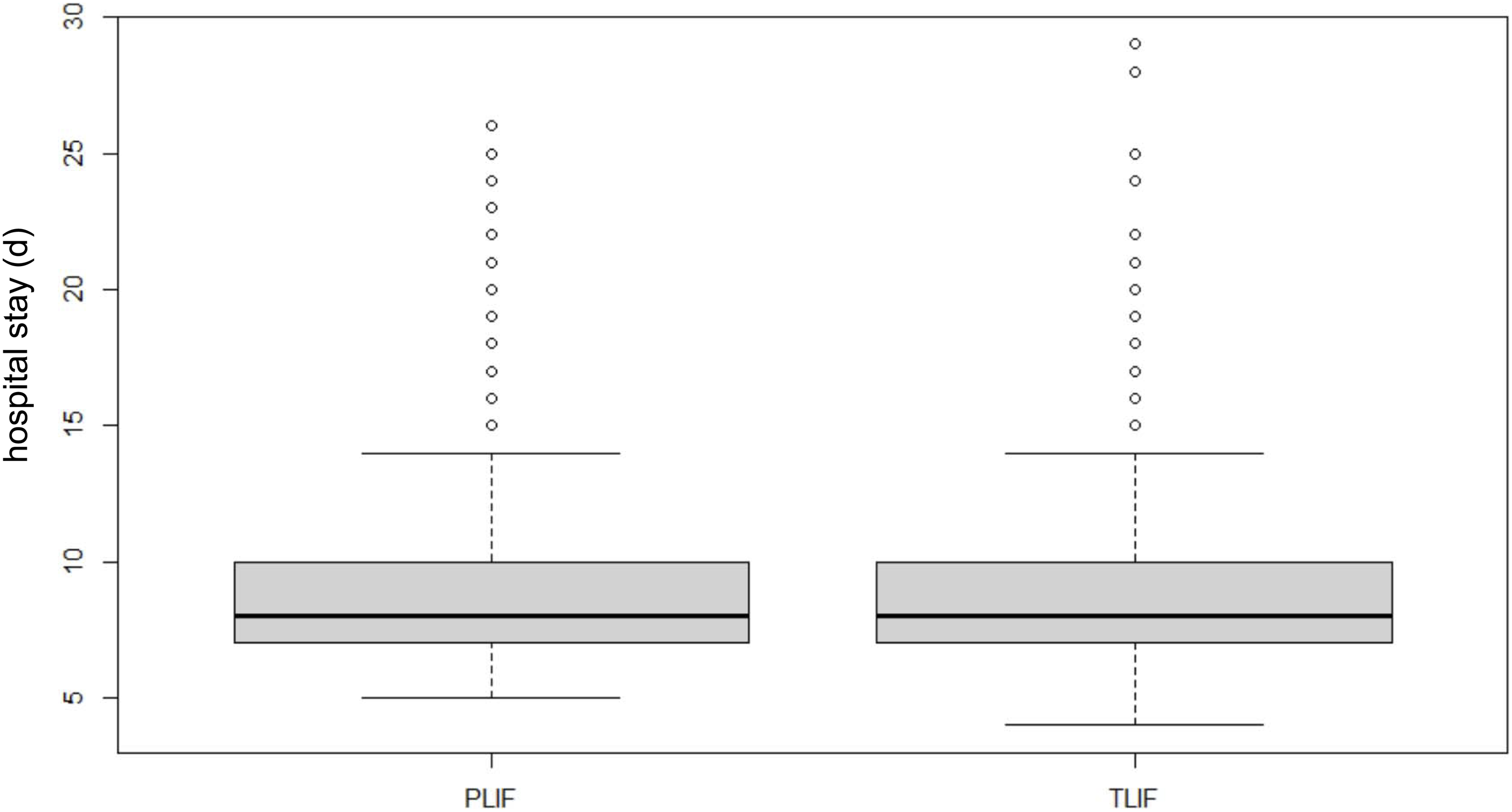
The overall 30-day readmission rate was 2.88% (n = 33) and was significantly higher in the TLIF collective than in the PLIF collective (PLIF: n = 12: 1.70%/TLIF: n = 21: 4.77%; P = .003419).
Complications
Timing of Different Complications for PLIF and TLIF Technique in Primary and Revision Cases.
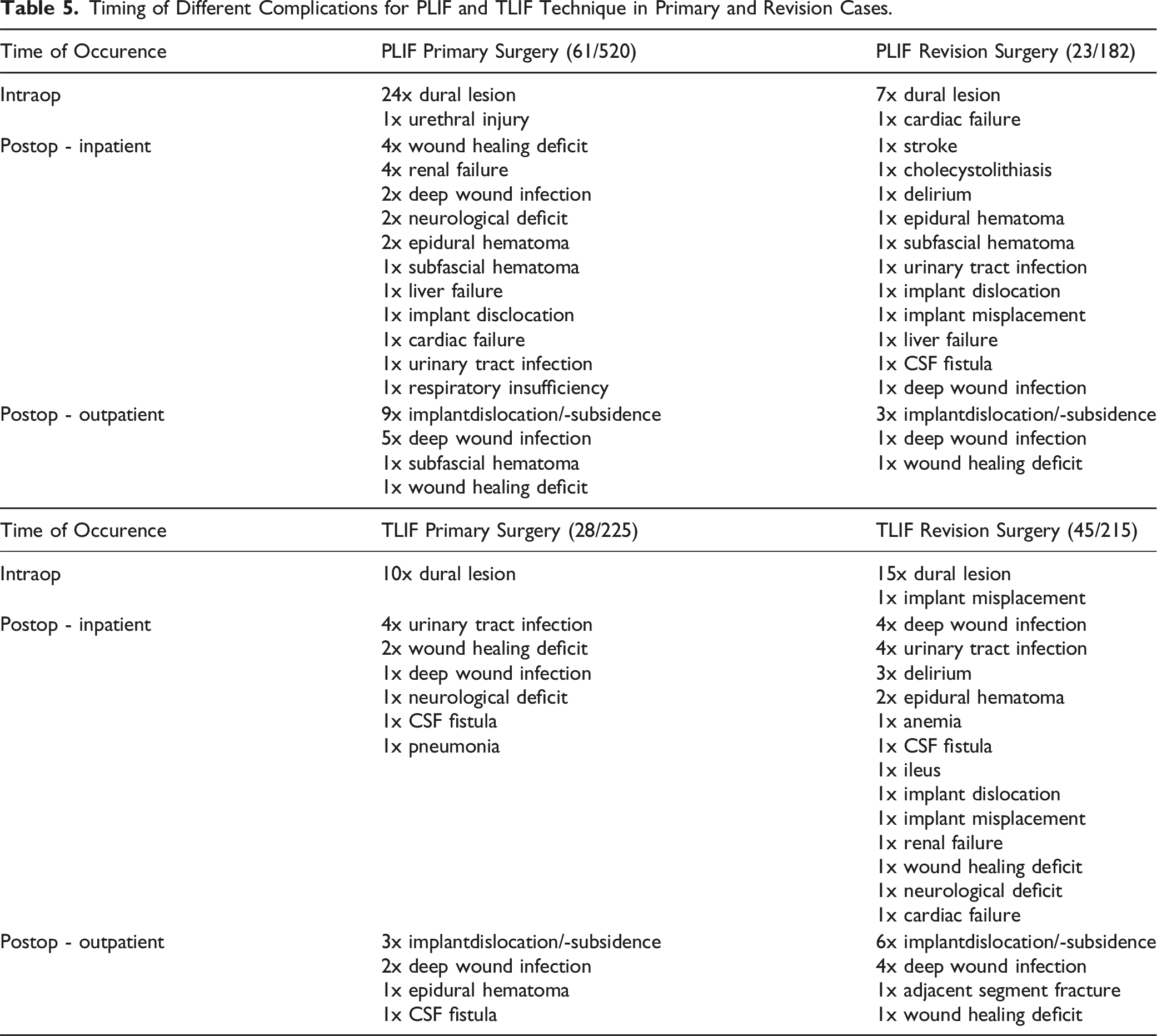
Most complications in the PLIF collective occurred intraoperatively (4.7%), and in the TLIF collective postoperatively during the inpatient course (7.5%). Intraoperatively, dural lesions were most common in both collectives (n = 56: 4.9%; PLIF: n = 31: 4.41%/TLIF: n = 25: 5.68%). In primary surgeries, the rate of dural lesions was comparable in both cohorts (PLIF: n = 24: 4.61%/TLIF: n = 10: 4.44%, P = 1). In revision surgeries, dural lesions were more common in TLIF patients than in PLIF patients (PLIF: n = 7: 3.84%/TLIF: n = 15: 6.97%), but the difference was not statistically significant (P = .19).
During the hospital stay wound healing disorders and renal insufficiencies were most common in the PLIF collective (n = 4: .56%), and urinary tract infections were most common in the TLIF collective (n = 8: 1.81%). After discharge, implant dislocations were most common in the PLIF collective (n = 12: 1.70%) and the TLIF collective (n = 9: 2.04%). Deep wound infections occurred with similar frequency (PLIF n = 3: .42%/TLIF n = 6: 1.36%).
Complications were divided into surgery-specific and general complications. PLIF and TLIF did not differ for surgery-specific complications.
There were no significant differences between PLIF and TLIF in complication severity, weighted by SAVES V2 severity. For revisions, both PLIF and TLIF patients had a greater proportion of SAVES 3 rather than SAVES 2 severity scores as shown in Figure 2. Distribution of SAVES V2 severity in primary and revision surgery.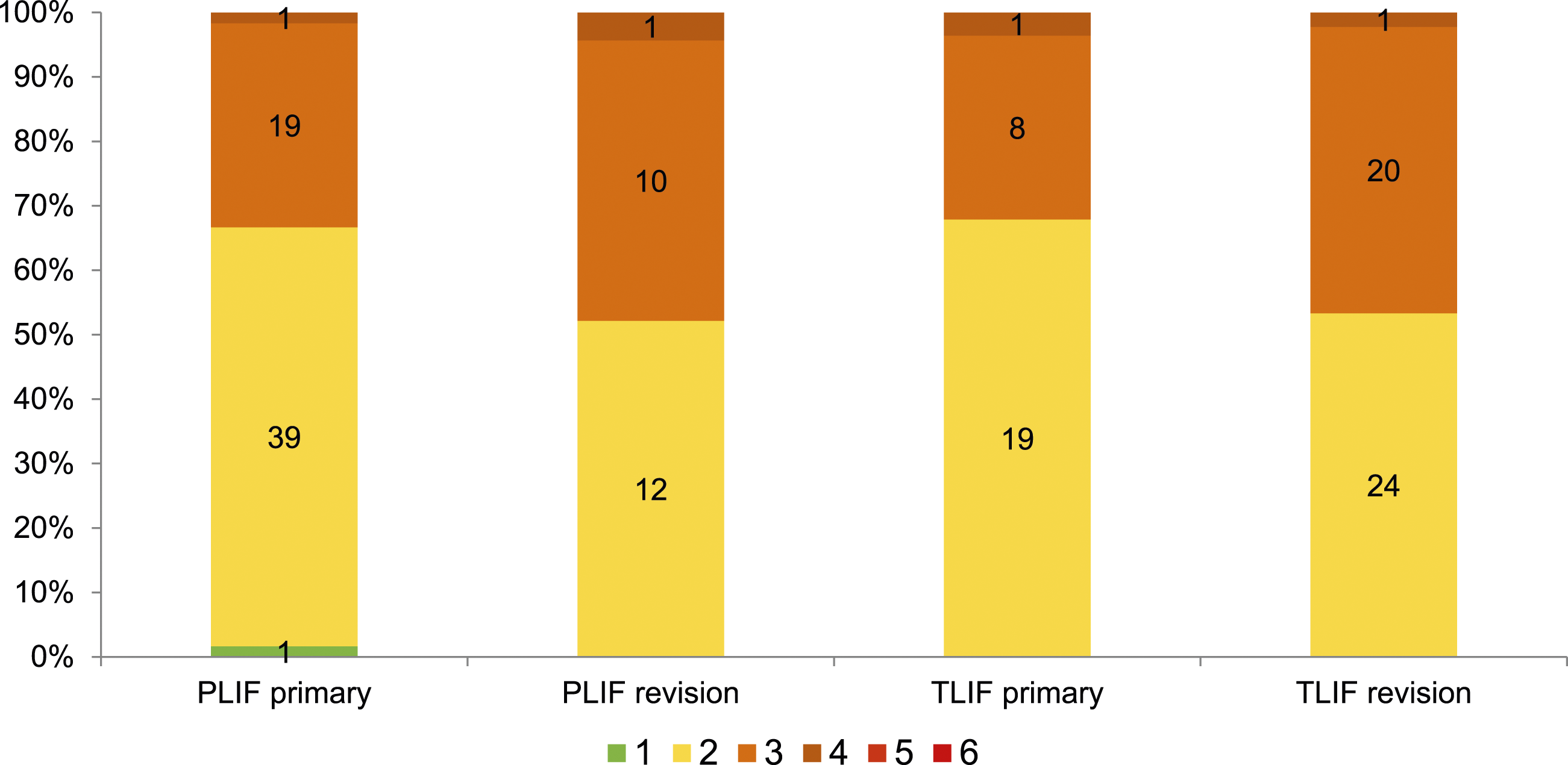
There was a correlation between the rate of complications and the duration of surgery. If complications occurred intraoperatively, the incision-suture time was prolonged. A correlation between incision-suture time and postoperative complications could also be demonstrated as outlined in Figure 3. The longer the surgery-time, the more frequently intraoperative or postoperative complications occurred. Correlation between duration of surgery and incidence of intraop resp. postop complications.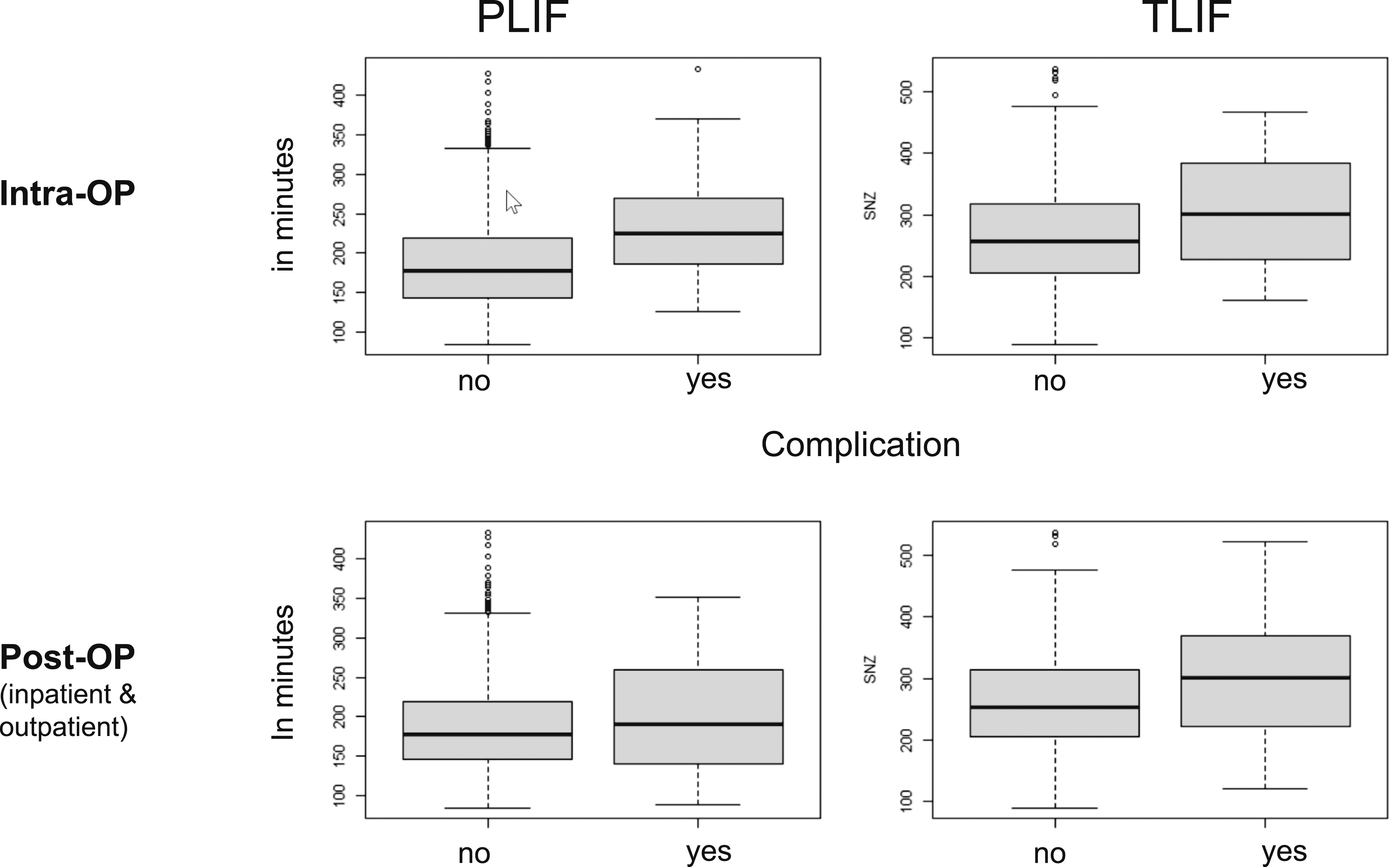
Discussion
Aim of this retrospective registry study was to compare the occurrence of complications between the surgical techniques PLIF and TLIF in two highly specialized spine centers. For the first time, complications were recorded and evaluated according to a uniform classification system. Instead of the conventional PLIF technique, a less invasive PLIF technique (mini open) was compared with the conventional TLIF technique.
To our knowledge, there is no comparable study with a comparably high number of patients. An important component of this work is the complication recording according to a unified classification system (SAVES V2). Until now, complication recording was often not performed uniformly and showed large differences between the respective studies. For example, early/late complications, transient/permanent complications, and major/minor complications were differentiated4,13,14 or only certain complications such as leg paralysis, dural tear, and postoperative back pain were recorded. This study is the first PLIF- and TLIF-comparative work in which all complications were uniformly recorded and classified according to their severity. Due to the standardized preoperative recording of the initial health status and postoperative outcome recording of the patients with uniform FU questionnaires, homogeneous data were available in this study. This increased comparability between the two study centers and provided better data quality compared with previous studies with often inhomogeneous evaluation parameters.
The SAVES V2 system, whose validity and reliability have been previously demonstrated11,12 was used for complication recording and analysis. The clear complication definition avoids terms such as “major”/“minor” “early”/“late”-“complications”, which offer much room for interpretation and are subject to the subjective interpretation of the surgeon. The different complication severity grades, which are based on the clinical effects, allow the complication severity to be classified more precisely.
The complication rate was influenced by many different factors (age, ASA, pathology, etc.,) in our study. The average age of the entire study cohort (n = 1142) at the time of surgery was 66 years. In both collectives, PLIF patients were slightly older on average than TLIF patients. The mean age was significantly higher than that from de Kunder et al study (52.5 years) 4 and Oezel et al work (59.9 years). 15 In the literature, the older age of patients is described as a clear perioperative risk factor for the occurrence of complications.16,17
The ASA score was similarly distributed in both collectives. No ASA scores have been documented in previous comparative work. Oezel et al 15 had reported an increase in ASA scores of 3 or >3 in a sample of PLIF and TLIF patients between 2015-2019 compared with 2009-2013. The sample reflects the current trend toward increasingly older and multimorbid patients.
More primary than revision surgeries were performed in the PLIF collective, and the ratio was balanced in the TLIF collective. Interestingly, no explicit statement in this regard can be found in the literature. Only Yang et al indicated revision surgery as an exclusion criteria. 10
Unlike the majority of previous studies, in which the OR time for PLIF was often longer9,18,19 the OR time for PLIF in this study was significantly shorter. This is probably due to the fact that PLIF surgeries in the first center were mainly performed by a few very experienced surgeons. TLIF surgeries in the other center were also performed by younger surgeons with less clinical experience. An exact recording of the clinical experience of the surgeons was not part of this work and should be documented in the future. Chi et al 20 criticized the mostly missing information about the clinical experience of the surgeons.
The lower blood loss reported in the majority of the literature for TLIF compared to PLIF4,19 was not confirmed. Both techniques had similar transfusion rates. The reason could be the extensive use of the surgical microscope and less soft tissue trauma with the less invasive PLIF technique. Teng et al 6 and Lan et al 21 attributed the increased blood loss and prolonged OR time with the conventional PLIF technique compared with the TLIF technique to the more extensive dissection of the paravertebral musculature and more extensive bony resection with the bilateral PLIF approach.
The increased complication rate often reported in the literature for conventional PLIF compared to conventional TLIF was not confirmed with the less invasive PLIF technique. TLIF patients had a statistically significant higher complication rate compared to PLIF patients for revision cases. This is due to the increased rate of dural lesions and above-mentioned complications in TLIF revisions. The main reason for this could be the necessary more extensive preparation of the scar tissue in the spinal canal in order to be able to insert the significantly larger TLIF cage (banana cage) unilaterally. In primary procedures, both techniques had comparable complication rates. No clear data regarding primary or revision surgeries can be found in the literature.
The intraoperative complication rate of both study groups was comparable. Intraoperatively, dural lesions were most common, with comparable incidence in both cohorts for primary surgeries and increased incidence in the TLIF collective for revision surgeries.
According to the literature, a problematic aspect of the PLIF technique is excessive retraction of the root and dural sac during access to the disc space.7,9,13,18 Consequently, the risk of complications increases, especially nerve-related complications such as dura or nerve injuries.
In 2017, de Kunder et al published the first systematic review and meta-analysis on TLIF and PLIF in degenerative spondylolisthesis. 4 Of note, the overall complication rate for PLIF was twice that for TLIF (17% vs 8.7%). Nerve root injuries and dural lesions were significantly PLIF-associated. This is consistent with the results of Lan et al 21 systematic review and meta-analysis, which also showed a PLIF complication rate twice that of TLIF (23.85% vs 11.33%), especially nerve-related complications such as dura and nerve injuries. The increased rate of dural lesions often associated with PLIF procedures was not confirmed in our study. Both techniques had comparable rates of dural lesions in primary surgeries. In revision surgeries, dural lesions were more common with TLIF, although not significantly so. De Kunder et al 4 (PLIF 6.1% vs TLIF 3.33%), Lan et al 21 (PLIF 8.98% vs TLIF 3.42%) and Ohrt-Nissen et al 22 (PLIF 9.5% vs TLIF 1.9%) reported increased dural lesions with PLIF. In most studies, decompression was performed without a microscope.9,10,19 It is possible that the more extensive use of the surgical microscope in the “mini open” PLIF technique compared to the conventional PLIF technique favors sparing of nerve structures and thus reduces the risk of nerve complications, especially incisional dura injuries.
A few papers reported comparable complication rates for both techniques. In Yang et al 10 randomized controlled trial, the complication rate was 11.8% for PLIF and 9.4% for TLIF. De Kunder et al 23 also reported comparable complication rates in their retrospective case series (PLIF 23% vs TLIF 25%). Blood loss was slightly, but not significantly, lower with TLIF. Limiting factors in all three studies were the small numbers of patients included.
While there are many comparisons between minimally invasive and conventional TLIF techniques,24-26 less or minimally invasive PLIF techniques are sparsely described and inconsistently defined. Tsutsunimoto et al 27 compared the effects of the “mini open” PLIF technique (paramedian, bilateral Wiltse approach) and conventional PLIF technique on paravertebral muscle damage and radiological parameters. The “mini open” PLIF provided less atrophy of the back muscles (multifidus muscle) and less postoperative analgesia requirements on MRI than the conventional approach. Limiting factors were the small collective size (n = 20) and lack of validated outcome parameters (VAS, ODI).
The influence of the invasiveness of the approach - posterior minimally invasive surgery (MIS) compared with open transforaminal or posterior lumbar interbody fusion (TLIF/PLIF) – was examined by Goldstein et al 28 within a meta-analysis and systematic review. There was no significant difference in surgical adverse events, but MIS cases were significantly less likely to experience medical adverse events (risk ratio [MIS vs open] = .39, P = .001). Nevertheless, this meta-analysis of adverse event data suggests equivalent rates of surgical complications with lower rates of medical complications in patients undergoing minimally invasive TLIF/PLIF compared with open surgery which can be recognized in accordance with these results.
Gala et al 29 came to a similar conclusion in comparison of different fusion techniques (PSF, TLIF, ALIF and AP fusion). In this large registry study the findings suggest that “patient/surgeon preference should be considered to determine the best surgical technique for the select patients with the given diagnosis who are considered for lumbar fusion”.
Inpatient, wound healing disorders and renal insufficiencies (n = 4 = .56%) were most common in the PLIF collective, and urinary tract infections (n = 8 = 1.81%) were most common in the TLIF collective, with no significant difference between the two collectives. There was no relevant difference in deep wound infections during the inpatient course (PLIF n = 3 = .42%, TLIF n = 5 = 1.13%). According to the literature, the general infection rate ranges from 0%-9%,4,13,30 although the time of infection is not explicitly mentioned.
Postoperatively, implant dislocations were most common in the PLIF collective (n = 12 = 1.70%) and the TLIF collective (n = 9 = 2.04%), as in Lan et al work 21 with no significant difference between the two collectives.
The incidence of surgery-specific complications as well as complication severity were comparable for both techniques. For revisions, there were more severity 3 complications than 2 complications for both techniques. Comparative values from the literature are not available for first-time use of the SAVES V2 system in this subject.
Chen et al 31 (Chen et al, 2017) studied the SAVES V2 system in elective spine surgery. They reported a significantly higher AE rate of independent reviewers after SAVES V2 use compared with the AE rate of surgeons (44% vs 13%). AEs of severity level 1 or 2 were most common, and the smaller (“minor”) AEs in particular were captured by the SAVES V2 system. The most common AEs were wound secretion and neuropathic pain. Severity 3 AEs were rare compared with this study. Chen et al 31 and Street et al 32 emphasized the importance of “minor” AEs, which would be increasingly captured by the SAVES system. Although usually without serious consequence to the patient and not individually costly, they cumulatively account for more than half of the total cost of AEs.33,34 The importance of smaller AEs will increase significantly in the future in an increasingly economized work environment. Further studies with SAVES application are needed to examine AEs in more detail.
Limitations
It is well known that retrospective longitudinal studies have a lower level of evidence than prospective ones. The data quality of complication recording decreases in case of a retrospective survey and also the complication rate may differ in this case compared to a prospectively collected complication rate. Ideally, AEs should be recorded immediately intraoperatively, within the hospital stay and even after discharge of the patient using SAVES V2 scheme.
Another limitation of the present study is that one of the two surgical techniques compared was performed in each of the two centers. In principle, this could represent a risk of bias; on the other hand, this offers the advantage of “high-volume surgery.” The lack of detailed recording of the clinical experience of the surgeons should also be mentioned as a weak point of this study.
Conclusion
An important component of this work is the complication recording according to a uniform classification system (SAVES V2). Until now, complication recording was often not performed uniformly and showed large differences between the respective studies. This study is the first PLIF- and TLIF-comparative work in which all complications were recorded uniformly and classified according to their respective severity.
In contrast to previous literature, we could demonstrate that there is not a significant difference between the two surgical techniques. A less invasive PLIF technique can be performed by an experienced spine surgeon with intraoperative and postoperative complication rates comparable to the TLIF technique.
Randomized clinical trials on this topic are needed to verify the results and correlations. It is also necessary to take a look at the long-term follow-up, especially with regard to the fusion rates, in order to be able to make a conclusive assessment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.