
Abstract
Study Design:
Retrospective cohort study.
Objective:
To assess the effect of diabetes mellitus (DM) on clinical and radiographic outcomes in patient with degenerative spondylolisthesis undergoing posterior lumbar spinal fusion.
Methods:
Analysis of patients who underwent open posterior lumbar spinal fusion from 2011 to 2018. Patients being medically treated for DM were identified and separated from nondiabetic patients. Visual analogue scale Back/Leg pain and Oswestry Disability Index (ODI) were collected, and achievement of minimal clinically important difference was evaluated. Lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), and PI-LL difference were measured on radiographs. Rates of postoperative complications were also collected.
Results:
A total of 850 patients were included; 78 (9.20%) diabetic patients and 772 (90.80%) nondiabetic patients. Final PI-LL difference was significantly larger (P = .032) for patients with diabetes compared to no diabetes, but there were no other significant differences between radiographic measurements, operative time, or postoperative length of stay. There were no differences in clinical outcomes between the 2 groups. Diabetic patients were found to have a higher rate of discharge to a facility following surgery (P = .018). No differences were observed in reoperation or postoperative complication.
Conclusions:
While diabetic patients had more associated comorbidities compared with nondiabetic patients, they had similar patient-reported and radiographic outcomes. Similarly, there are no differences in rates of reoperation or postoperative complications. This study indicates that diabetic patients who have undergone thorough preoperative screening of related comorbidities and appropriate selection should be considered for lumbar spinal fusion.
Introduction
Diabetes mellitus (DM) is a common comorbidity for patients undergoing lumbar spinal fusion that continues to increase in prevalence. 1,2 According to the Centers for Disease Control and Prevention, in 2016 more than 29 million Americans had DM and 86 million had prediabetes. 3,4 DM has previously been established as an independent risk factor for increased adverse events and poor clinical outcomes. Specifically, majority of these studies have associated DM with increased length of hospital stay, surgical site infection, hospitalization costs, and morbidity and mortality. 1,2,5 -8 Limited number of studies address clinical outcomes in diabetic patients undergoing spinal surgery, and have largely concluded that patients with DM had poorer outcomes than those without DM. 1,2,9 -14 However, few studies have examined outcomes in patients with degenerative spondylolisthesis after an open posterior lumbar fusion. 15 -17
Given the poor outcomes that are widely attributed to diabetic patients undergoing lumbar fusion, it is prudent to examine spinopelvic parameters as a potential contributor to these outcomes; especially, in light of the direct relationship between health-related quality of outcome scores (HRQOL) and proper restoration of sagittal or spinopelvic parameters in spine fusion surgeries, and in patients with degenerative spondylolisthesis. 15,18 -24 Additionally, it is important to examine the impact of DM on sagittal parameters because studies have reported increased intervertebral disc degeneration, decreased bone matrix density, and extended fracture reunion time with DM. 25 -27 Many of these changes are normally seen with advanced age and contribute to biomechanical changes and instability of the spine. 28,29 Specifically, studies have used animal models and human disc tissue to explain the increased intervertebral disc degeneration with DM and have reported accelerated cell apoptosis in the nucleus pulposus, accumulation of advanced glycation end products in discs, and decreased microvascular density in endplates as contributing mechanisms. 25,30,31 Disc degeneration, osteoporosis or osteopenia, and improper fracture reunion can result in decreased intervertebral height accompanied by slack in supporting spinal ligaments, which alters the normal biomechanics of the spine and shifts more load-bearing to the facet joints along with increasing torsional stiffness. 26,32 Overtime the facet joints develop degenerative changes leading to spine instability and possible sagittal malalignment. 29,33 Despite the potential effect of DM on alignment, there is a lack of data examining the relationship between DM and sagittal or spinopelvic parameters following lumbar spinal fusion surgery.
In this study, we compared both the clinical and radiographical outcomes of DM in patients who had an open lumbar spinal fusion surgery utilizing a cohort from a single academic institution. We hypothesize that the patients with DM will have worse clinical outcomes, fusion rates, radiographic sagittal parameters, and reoperation rates compared to patients without DM. This study can be utilized for preoperative surgical planning and postoperative management of patients with DM.
Materials and Methods
Study Design
A retrospective cohort study was conducted of consecutive patients who were indicated for elective open posterior lumbar spinal fusion after failure of conservative treatment to address radiculopathy and neurogenic claudication at a single academic institution between January 2011 and January 2018. Exclusion criteria included the following: less than 18 years of age at the time of surgery, had a lumbar fracture, tumor, or infection, fusions involving the thoracic spine, high-grade spondylolisthesis, or concomitant deformity.
Demographic, Clinical, and Radiographic Measurement Analysis
Demographic information collected for all patients included: age, sex, body mass index (BMI), smoking status, psychiatric condition, preoperative opiate use, and American Society of Anesthesiologists (ASA) class. Patients being medically treated for DM were identified and separated from non-diabetic patients. The diagnosis of diabetes was made if the patient had fasting glucose levels of >126 mg/dL on 2 separate tests as well as hemoglobin A1c levels of >6.5% on 2 separate tests.
Using Opal Viztek-RAD, PPX Imaging, Inc, several radiographic parameters were measured preoperatively, immediately postoperatively (standing radiographs performed on postoperative day 1), and at the most recent follow-up: lumbar lordosis (LL), pelvic tilt (PT), and pelvic incidence (PI) (Figures 1 and 2). The PI-LL difference was calculated. PT was identified as the angle between a line through the midpoint of the superior sacral endplate to the center of the femoral heads and a vertical reference line. PI was obtained as the resultant angle of a line through the midpoint of the superior sacral endplate to the center of the femoral heads and the line perpendicular to the midpoint of the superior sacral endplate. LL defined as the resultant angle of the L1 superior endplate and the S1 superior endplate. As part of the preoperative planning, the surgeons assessed the lumbar spine sagittal parameters on plain radiographs. The amount of sagittal balance correction was based on their individualized evaluation. Generally speaking, if sagittal imbalance correction was deemed necessary, the goal of the correction was to obtain a PI-LL mismatch of 9° or less. Finally, fusion assessment was performed on plain radiographs. Fusion was determined to be present if bone bridging was present between transverse processes and/or facets at the fusion level on both anteroposterior and lateral plain radiograph views. If flexion and extension lateral lumbar plain radiographs were obtained, fusion was deemed present if there was no visible motion between the vertebral body and fusion adjunct.
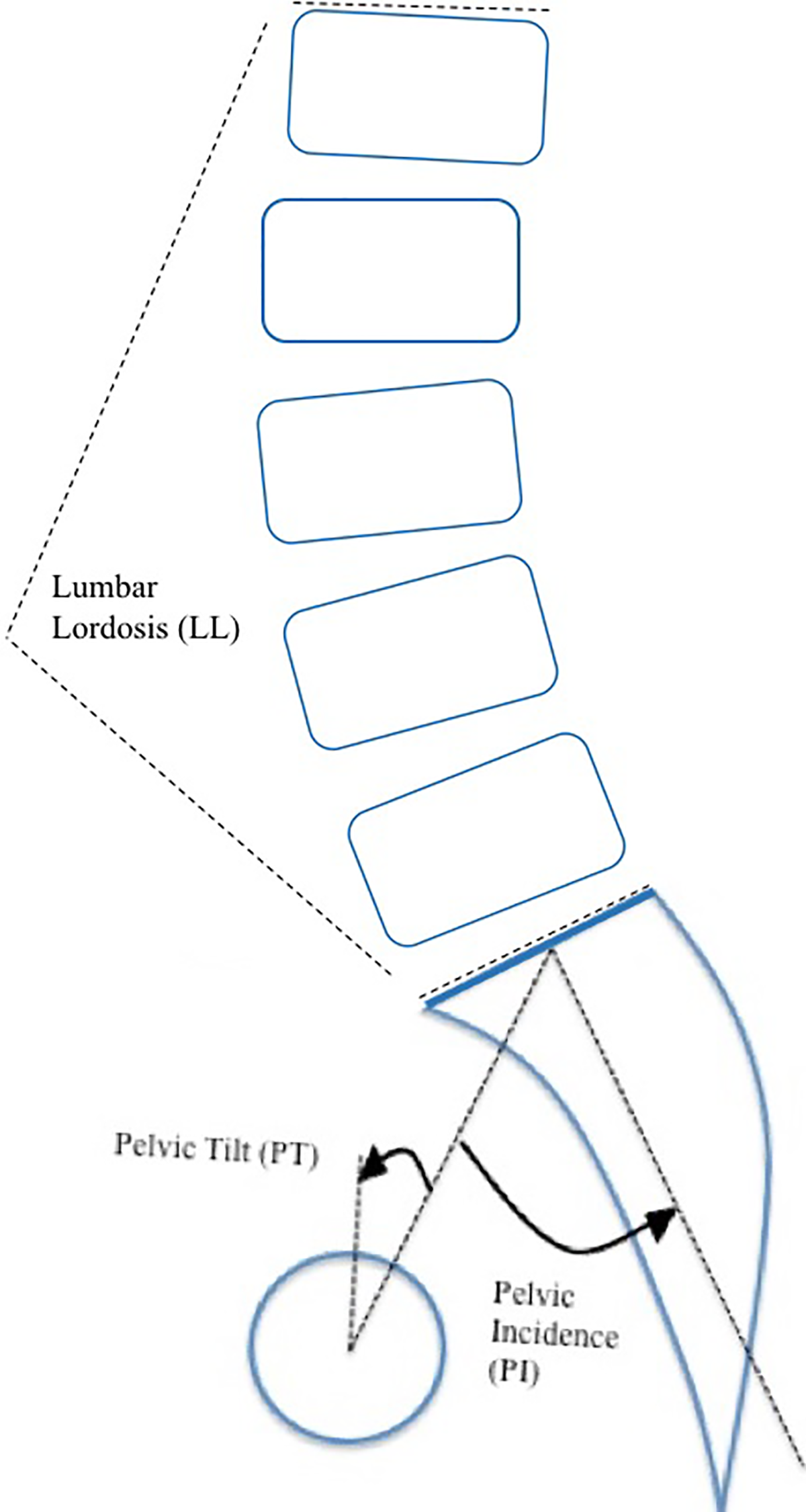
Schematic of radiographic measurements.
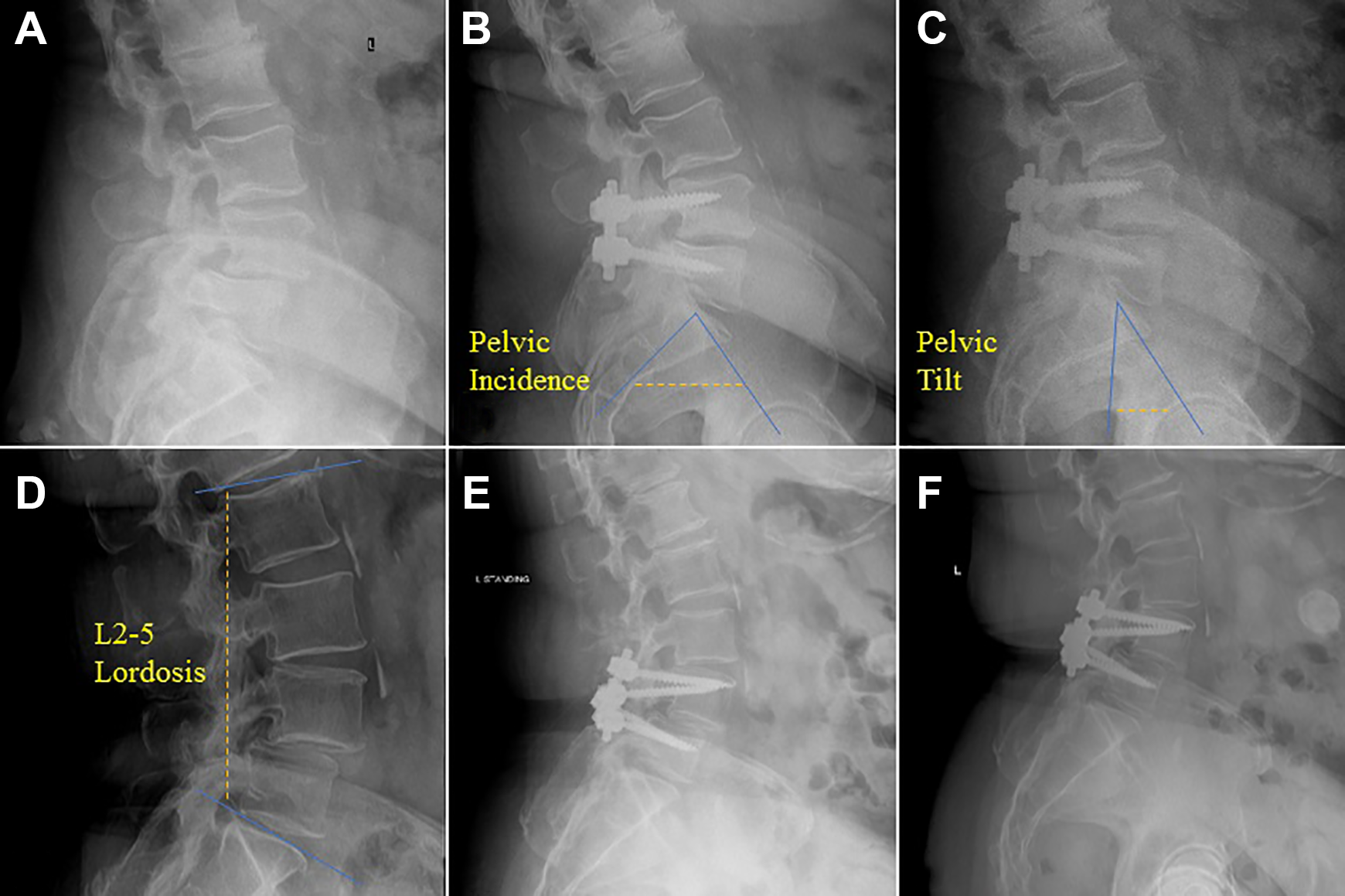
Lateral neutral x-ray of diabetic patient prior to posterior lumbar spinal fusion (A), following fusion (B), and at final follow-up (C). Lateral neutral x-ray of nondiabetic patient prior to posterior lumbar spinal fusion (D), following fusion (E), and at final follow-up (F).
Preoperative and final patient-reported outcomes were obtained in the form of visual analogue scale (VAS)–back pain, VAS–leg pain, and Oswestry Disability Index (ODI). Additionally, the rates of dural tear, postoperative complications (aspiration, urinary tract infection, acute renal failure, epidural hematoma, altered mental status, deep vein thrombosis/pulmonary embolism, stroke, myocardial infarction, pneumonia, pleural effusion, urinary incontinence, neurological deficit, or hardware complications), postdischarge destination, reoperation, pseudoarthrosis, as well as operative time and postoperative length of stay were recorded. The following operative characteristics were also recorded: number of levels fused, the use of an interbody cage, and if intraoperative neuromonitoring was employed. Minimal clinically important difference (MCID) thresholds were as follows: ODI 14.9, VAS–back pain 2.1, VAS–leg pain 2.8, which is based on previous thresholds reported in the literature for posterior lumbar fusion. 34
Statistical Analysis
Analysis was conducted using Stata version 13.1 (StataCorp LP, College Station, TX). Binary outcome variables were compared between diabetic and nondiabetic groups with multivariate logistic regression for categorical variables, and continuous outcome variables were compared using multivariate linear regression. Baseline patient and operative characteristics were compared using chi-square analysis and t tests for categorical and continuous data, respectively. Multivariate analyses controlled for baseline patient and operative characteristics, such as age, smoking status, and BMI. The threshold for statistical significance was set at P < .05.
Results
A total of 850 patients were included; 78 (9.20%) diabetic patients and 772 (90.80%) nondiabetic patients. The average length of clinical follow-up was 22.99 ± 18.50 months (range: 6-83 months) and average length radiological follow-up was 15.47 ± 12.41 months (range: 6-83 months). For diabetic patients, the average hemoglobin A1c was 7.20% ± 1.18% (range: 5.10%-10.70%). On bivariate analysis, diabetic patients were older (P < .001), had higher body mass index (P < .001), greater ASA scores (P < .001), and higher prevalence of grade 1 spondylolisthesis (P < .001), while nondiabetic patients were more likely to have had an interbody used (P = .024, Table 1). A total of 203 patients (23.88%) had prior lumbar surgeries, which included 68 (33.50%) patients with prior lumbar fusions and 135 (66.55%) patients with decompression alone (isolated laminectomy and discectomy). In this group, 149 (73.40%) patients had prior lumbar spine surgery at the same level, and of these, 32 (21.48%) were lumbar fusions. Indications for lumbar fusion after a prior lumbar spine surgery included lack of symptomatic relief, iatrogenic instability, and recurrence of herniation of the nucleus pulposus and/or stenosis.
Baseline Patient/Operative Characteristics.
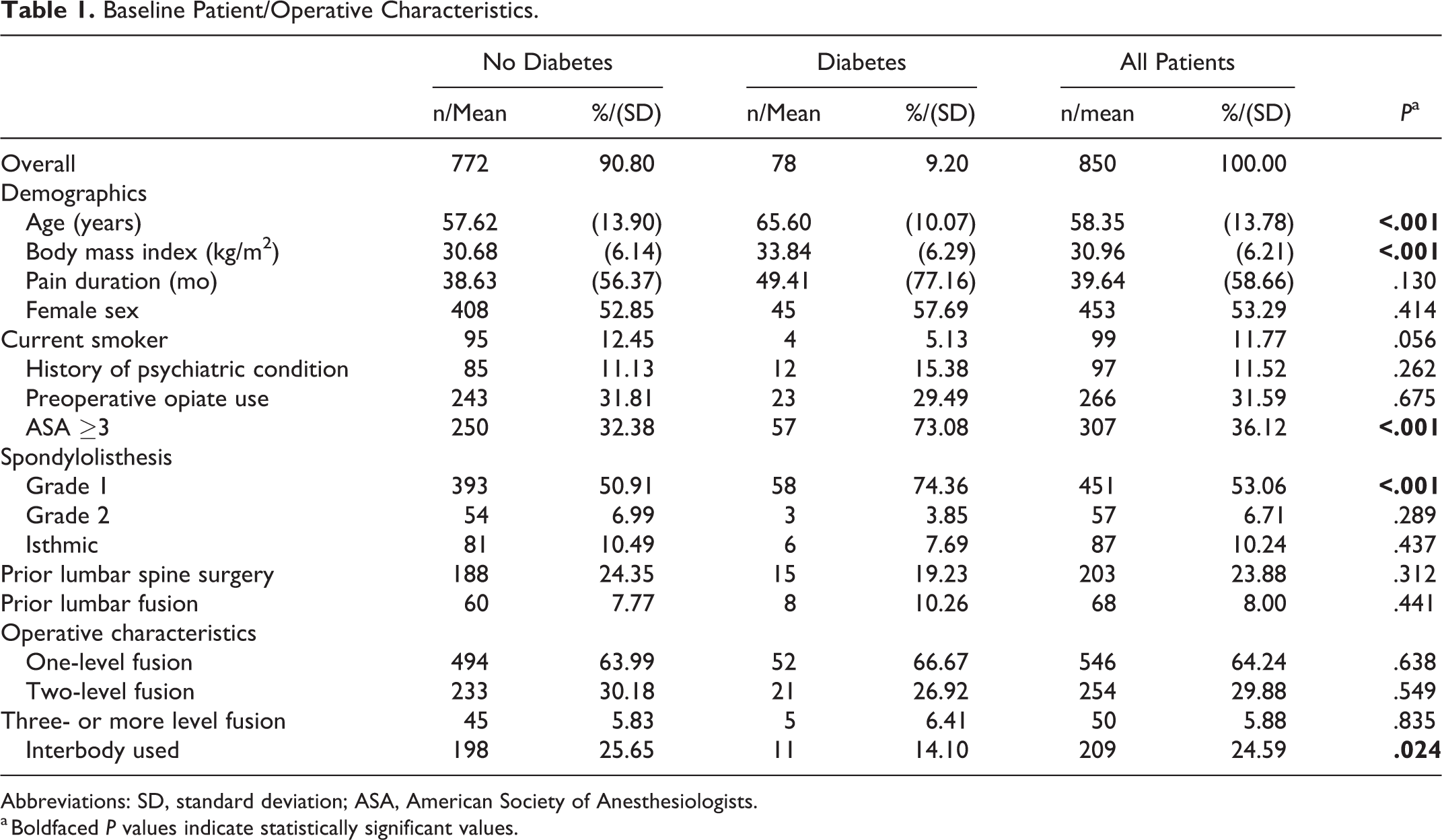
Abbreviations: SD, standard deviation; ASA, American Society of Anesthesiologists.
a Boldfaced P values indicate statistically significant values.
On multivariate linear regression, final PI-LL difference was significantly larger (P = .032) for patients with diabetes compared with those without diabetes, but there were no other significant differences between radiographic measurements, or operative time (Table 2). Pain control, drain output, physical therapy clearance, discharge to facility, and postoperative complications, such as urinary tract infection or epidural hematoma, were among the reasons for a delay in discharge; however, the postoperative length of stay was similar for both cohorts. There was no difference in VAS-back, VAS-leg, and ODI scores between the 2 groups (Table 3).
Radiographic measurements, degenerative diagnosis used as reference.
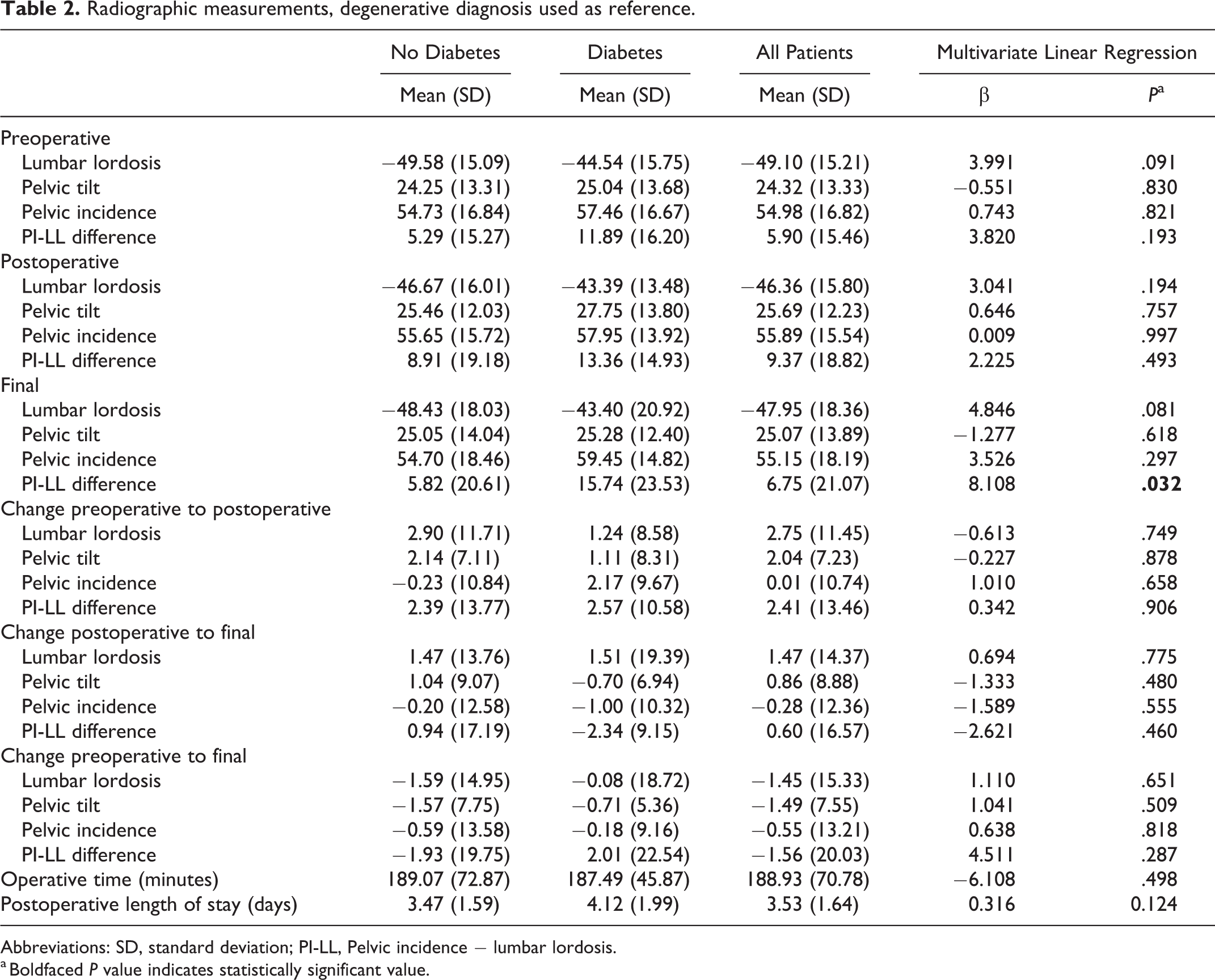
Abbreviations: SD, standard deviation; PI-LL, Pelvic incidence − lumbar lordosis.
a Boldfaced P value indicates statistically significant value.
Patient-Reported Outcomes.
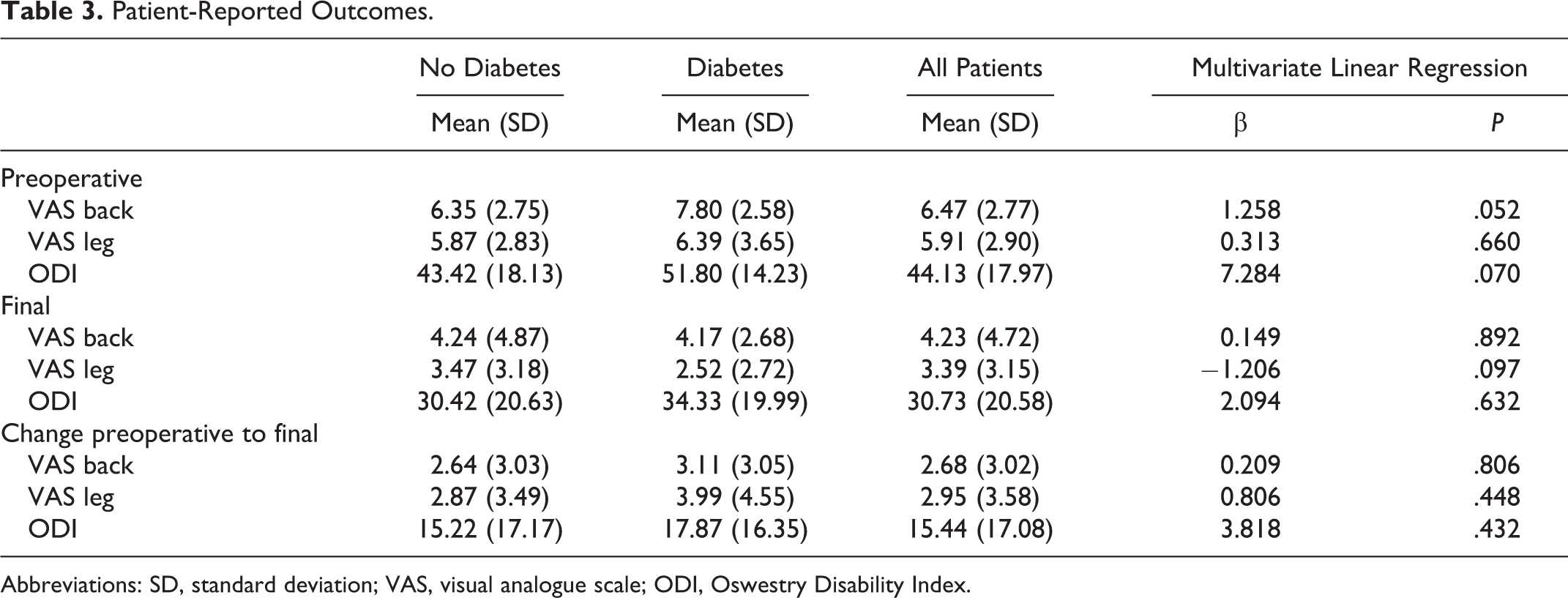
Abbreviations: SD, standard deviation; VAS, visual analogue scale; ODI, Oswestry Disability Index.
Furthermore, diabetic patients were found to have a higher rate of discharge to a facility following surgery (P = .018, Table 4). There was no difference in rate of dural tear, reoperation, postoperative complication, pseudoarthrosis, or early adjacent segment degeneration. The pseudoarthrosis rate for patients without diabetes was 6.06% and 8.20% for patients with diabetes while the reoperation rate was 6.05% for nondiabetic patients and 12.50% for diabetic patients. No difference in achievement of MCID for VAS-back, VAS-leg, or ODI scores was found between diabetics and nondiabetic patients.
Postoperative Complications and Reoperation.
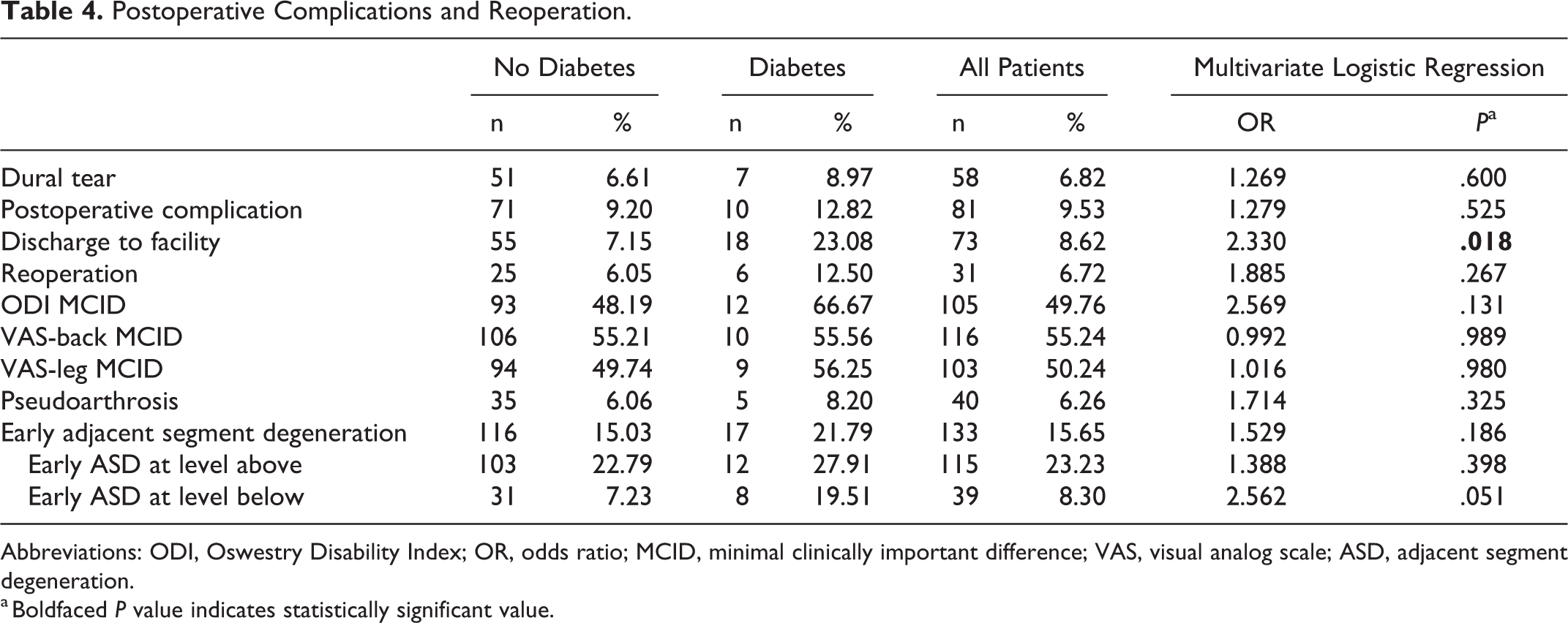
Abbreviations: ODI, Oswestry Disability Index; OR, odds ratio; MCID, minimal clinically important difference; VAS, visual analog scale; ASD, adjacent segment degeneration.
a Boldfaced P value indicates statistically significant value.
Discussion
Prevalence of DM continues to increase in the United States and accordingly the number of diabetic patients undergoing lumbar fusions continues to rise. 3,4 While many studies have assessed complications and clinical outcomes for diabetic patients after undergoing spinal surgery, 1,2,5 -8 there is little in the literature regarding effect of diabetes on sagittal or spinopelvic parameters. It is important to examine the impact of DM on sagittal parameters because increased disc degeneration, osteoporosis or osteopenia, and improper fracture reunion associated with DM can contribute to instability and, subsequent, sagittal malalignment in patients. 25 -29 The present study assessed 850 diabetic and nondiabetic patients and found overall similar radiographic and clinical outcomes. The final PI-LL difference was significantly larger for patients with diabetes versus those without diabetes but there were no other significant differences between radiographic measurements, operative time, postoperative length of stay, VAS-back, VAS-leg, and ODI scores, or MCID achievement between the 2 groups. Furthermore, diabetic patients had higher rates of discharge to a facility despite comparable reoperation, postoperative complication, and pseudoarthrosis rates compared with nondiabetic patients.
Patient-reported clinical outcomes were comparable between diabetic and nondiabetic patients. Our results contrast with multiple studies that have shown that patients with DM have worse clinical outcomes with increased morbidity compared to patients without DM. 1,2,9 -14,19 -21 Armaghani et al 14 studied clinical outcomes in 1005 diabetic and nondiabetic patients undergoing spine surgery, and noted significantly worse outcomes for diabetics compared with nondiabetic patients despite improvement in both groups from preoperative scores. More specifically, Freedman et al 1 examined patient-reported clinical outcomes in 594 diabetic and nondiabetic patients with degenerative spondylolisthesis treated with open lumbar fusion. This study found that patients with diabetic patients had worse outcomes than nondiabetics. 1 Contrarily, Bendo et al 19 evaluated 32 diabetic patients undergoing open posterior lumbar fusion and reported comparable clinical outcomes. Our results reflect specific patient-reported outcomes for diabetic patients with degenerative spondylolisthesis in isolation as we controlled for all of the associated comorbidity; thus, the diagnosis of diabetes independently may not cause worse outcomes. However, our results may also be explained by the vigorous preoperative medical clearance and careful selection of patients with moderately controlled diabetes and proper surgical indications. Majority of our patients may have been non–insulin-dependent diabetics with moderately controlled blood glucose levels and hemoglobin A1c and without progression of DM late stage with neuropathy, which would favor clinical outcomes similar to nondiabetic patients. Diabetic patients were also counseled about the potential for worse outcomes after surgery that can influence patient expectations and perceived improvement of symptoms.
Even though the clinical outcomes between diabetic and nondiabetic patients were comparable, diabetic patients were older with higher prevalence of obesity and ASA ≥3 compared with nondiabetic patients. The literature largely supports these results although some studies have found similar age and BMI between the 2 cohorts. 1,2,9 Appaduray et al 2 concluded that patients with DM were older and had more associated comorbidities than those without DM after evaluating 902 patients who underwent lumbar decompression and/or spinal fusion. There was also a higher likelihood of discharge to facility for diabetic patients compared with nondiabetics, which is an interesting finding given that the 2 cohorts had comparable postoperative complications. However, DM has been noted as an independent predictor of discharge to facility by few previous studies. 7,35,36 Aldebeyan et al 35 analyzed discharge destination of 15 092 patients and identified DM as predictor of discharge to facility. With the advent of bundled-care reimbursement systems for many procedures, the increased rate of discharge to facilities for diabetics must be accounted for in order to maintain appropriate access of these patients to these interventions.
Final PI-LL differences were significantly larger in diabetic patients compared with nondiabetic patients, which is the first time such an association has been noted in literature. In fact, PI-LL difference of diabetic patients remained >10° and larger than nondiabetic patients from preoperative to final evaluation although these differences were not statistically significant. Regardless, PI-LL difference of >10° signifies global sagittal malalignment, and is compensated by larger PT and smaller LL; however, these compensations were lacking in the diabetic patients. 37,38 Kim et al 15 examined clinical and sagittal parameters in 18 patients with degenerative spondylolisthesis after undergoing posterior interbody fusion, and reported that sagittal parameters influence clinical outcomes and should be addressed in fusion to promote sagittal balance. Several other studies have also addressed the importance of sagittal balance for achieving good clinical outcomes in patients with degenerative spondylolisthesis. 16,17 These studies did not consider the presence or absence of diabetes, thus postulating an explanation for the PI-LL difference between the diabetic and nondiabetic patients must rely on animal model studies. Studies have shown increased intervertebral disc degeneration, decreased bone matrix density, and extended fracture reunion time found in animal model and human tissue with DM, which may decrease the ability to compensate for sagittal malalignment. 25 -27 These studies elucidate a difference in the biological components of the spine in a patient with diabetes, which may contribute to the PI-LL mismatch. Higher BMI in diabetic patients was controlled for in the multivariate analysis and, thus, cannot be used to explain the PI-LL mismatch noted in patients with diabetes. However, there may be little relevance of these results given that PI-LL is an important consideration in deformity correction surgeries which were not included in our study cohorts. Additionally, the association between sagittal parameters and clinical outcomes noted in many studies was not observed in this study as there was no difference in clinical outcomes between the 2 cohorts. Park et al 39 reported similar findings after examination of 223 patients with adult spinal deformity undergoing minimally invasive or hybrid correction surgery. 39 They found that achievement of spinopelvic parameter was not predictive of improvement in minimal clinical important difference or substantial clinical difference in clinical outcomes. As mentioned previously, this lack of difference in clinical outcomes may be due to the focused nature of our study cohort that included only diabetic patients with degenerative spondylolisthesis. Further clinical and biochemical studies may be beneficial to understand the large PI-LL mismatch and lack of compensation for spinopelvic malalignment in diabetic versus nondiabetic patients.
The present study does have several limitations. Selection bias is a potential concern as a retrospective cohort study. Furthermore, the level of diabetic control was difficult to ascertain from this retrospective analysis, and adjustment for this can be difficult given the wide variety of medical treatments available. Majority of the diabetic patients in this study were moderately controlled, which limits the generalizability of the results to patients with uncontrolled diabetes. In addition, data regarding the rate of readmission was limited because it was outside the scope of this study and patients that may have been readmitted at an outside hospital could not be captured. The study is further limited due to the lack of long-term follow-up for all our patients although the average clinical follow-up was approximately 23 months. However, this is the first study to explore possible associations between sagittal parameters and DM which creates an avenue for future discussion and investigation, specifically for stratifying hemoglobin A1c levels and DM type. Although, we cannot comment on the global malalignment because full-length spine plain radiographs were not obtained for all patients (as per surgeon protocol). Additionally, there were baseline differences between diabetic patients and non-diabetics. In an effort to increase clinical applicability and reduce selection bias, multivariate analyses controlled for baseline demographics and preoperative characteristics between groups. Finally, another limit to the generalization of these results is that the data reflects the work of only 3 surgeons at a single academic center. However, this study provides support for individualized evaluation of diabetic patients indicated for lumbar fusion surgery rather than avoiding the consideration of surgery due to the worry of insufficient improvement of symptoms and radiographic parameters due to associated comorbidities and risk of complications.
Conclusion
Diabetic patients have a higher likelihood of associated comorbidities compared with nondiabetic patients. However, patients with DM have similar patient-reported and radiographic outcome, except for a larger final PI-LL difference following an open posterior lumbar fusion. Similarly, there were no differences in reoperation rates and postoperative complications. This study indicates that open lumbar spinal fusion can be safe and effective for diabetic patients after vigorous preoperative medical clearance and careful selection of patients with well-controlled diabetes and proper surgical indications. Future studies are necessary to understand the biomechanical impact of DM on the ability to restore and maintain lumbosacral sagittal balance following lumbar fusion surgery.
Supplemental Material
Supplemental Material, Suppl_1_GSJ - Do Clinical Outcomes and Sagittal Parameters Differ Between Diabetics and Nondiabetics for Degenerative Spondylolisthesis Undergoing Lumbar Fusion?
Supplemental Material, Suppl_1_GSJ for Do Clinical Outcomes and Sagittal Parameters Differ Between Diabetics and Nondiabetics for Degenerative Spondylolisthesis Undergoing Lumbar Fusion? by Jannat M. Khan, Joseph Michalski, Bryce A. Basques, Philip K. Louie, Oscar Chen, Zayd Hayani, Chaim Kalish, Islam Elboghdady, Matthew Colman and Howard An in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.