
Abstract
Study Design
Retrospective Cohort Study.
Objective
Despite innovations in minimally invasive (MI) techniques for sacroiliac joint fusion (SIJF), trends in utilization and associated costs remain unclear. In this study, we assessed these trends and costs in a database of privately insured patients.
Methods
Records of open and MI SIJFs were queried from the 2007-2021 MarketScan Databases with CPT codes. Net payments made by insurance carriers were identified, as were out-of-pocket payments made by patients for each encounter. Regression was used to model utilization, payments, and costs.
Results
4124 SIJFs were identified, 1626 (39.4%) of which were MI SIJF. SIJF utilization increased by 1176.2% throughout the study period (P < .001). However, open SIJF utilization peaked in 2012. Open SIJF utilization was not significantly associated with time (P = .18). By contrast, the peak utilization for MI procedures occurred in 2021. Spine surgeons’ volume of MI SIJF increased by 258% over the study period (P < .001), while nonsurgeon volume of MI SIJF increased by 990.9% (P < .001).
Conclusion
Privately insured patients have increasingly utilized SIJF over the past several years. This is predominantly due to the adoption of MI techniques by spine surgeons and nonsurgeons.
Introduction
Sacroiliac joint pain comprises approximately 10-30% of all mechanical lower back pain.1,2 Sacroiliac joint fusion (SIJF) is a potential solution for those who have not found relief through conservative measures.3,4 Recent advances in the field have introduced minimally invasive (MI) techniques, offering patients the potential benefits of reduced recovery times and minimal tissue disruption compared to traditional open procedures.5-12 Alongside these developments, a recent report noted that non-spine surgeon providers are increasingly providing MI SIJF, adding additional complexity to the landscape of SIJF treatment. 13
Despite the dynamic environment surrounding SIJF, little is known about the current trends in MI and open SIJF within the privately insured population. While recent studies have described MI SIJF procedural utilization trends in the Medicare population, the costs and utilization of both open and MI SIJF in privately insured patients remain undescribed. 13 As a result, there is a need to characterize the trends in SIJF procedure utilization in privately insured patients, and to subsequently identify associated costs, the different types of providers involved, and the characteristics of the patients undergoing this treatment.
This report aims to present the trends in procedural utilization for both open and MI SIJF within the privately insured population by leveraging data from a 15-year sample of a nationally representative longitudinal claims database. Additionally, we sought to define and elucidate the financial costs faced by patients, insurers, and the healthcare system, contributing to a more comprehensive understanding of the economic implications of open and MI SIJF procedures in the context of private insurance.
Methods
Database
We performed a retrospective cohort study using deidentified data from IBM’s MarketScan databases. 14 MarketScan provides longitudinal data derived from insurance claims and enrollments. In total, it contains records for over 273 million unique individuals by aggregating more than 32 billion claims. Specifically, we queried records from the Inpatient and Outpatient Services databases. These repositories contain cost information and medical record details described by International Classification of Diseases (ICD) and Common Procedural Terminology (CPT) codes. These databases assign each patient a unique identification number, enabling longitudinal analysis and linkage between data sets. The Stanford Institutional Review Board approved this study under protocol #40974.
Cohort Construction and Variables
The study period was from 2007 to 2021. First, patient enrollments with procedures corresponding to open and minimally invasive SI joint fusion were identified with the CPT codes 27279 and 27280 from the inpatient and outpatient services tables. Simultaneously, provider specialty was determined via medical and surgical specialty codes inherent to MarketScan. These codes were then used to bin providers into one of two categories: spine surgeon or non-spine surgeon. Similarly, each patient’s age, sex, comorbidities, procedure date, geographic region, and year of insurance enrollment were identified. Comorbidities were defined by constructing the Elixhauser Comorbidity Index for each patient using ICD9 and ICD10 codes recorded at any time points at or before their SI joint fusion procedure. Next, the payments made by patients and insurers for each SIJF were identified. Patients out-of-pocket (OOP) expenses were comprised of any required copayments, coinsurance, and deductibles. Net payments made by insurers included any fees for the SIJF encounter that were not covered by the patient’s OOP expenses.
Statistical Analysis
The primary outcome of this study was the volume of SI joint fusions per calendar year across the study period, which was further stratified into the volume of MIS and open procedures. Secondary outcomes were net OOP expenses and net insurance payments for each procedure. For graphical analysis, minimally invasive and open procedure counts and associated costs were grouped by provider specialty and the calendar year. No imputation of missing data (less than 1%) was performed at any point throughout this study. Finally, no patients were excluded from this analysis, as the primary aims of this study were to identify the frequencies at which patients underwent SI joint fusion of any form.
All statistical analyses were conducted in the R Environment for Statistical Computing (Vienna, Austria). Summary statistics for the relevant variables in the study cohort were computed and reported via the TableOne package. Univariate analysis was performed to compare study variables stratified by whether an encounter’s SI joint fusion was minimally invasive or open. Multivariable linear regressions assessed the associations between costs and patient age, sex, comorbidities, geographic region, year of insurance enrollment, insurance plan type, and provider type. Next, a multivariable Poisson regression (count model) was fit to assess the impact of calendar year, provider type, and procedure type (MI or open) on the number of annual SI joint fusions. No additional variables were constructed or used in regression analysis. Poisson regression coefficients were reported as incidence rate ratios (IRR). Coefficient estimates are accompanied by their 95% confidence intervals (CI). The threshold used to assess statistical significance throughout all analyses was P < .05.
Results
Cohort Characteristics
Cohort Characteristics.
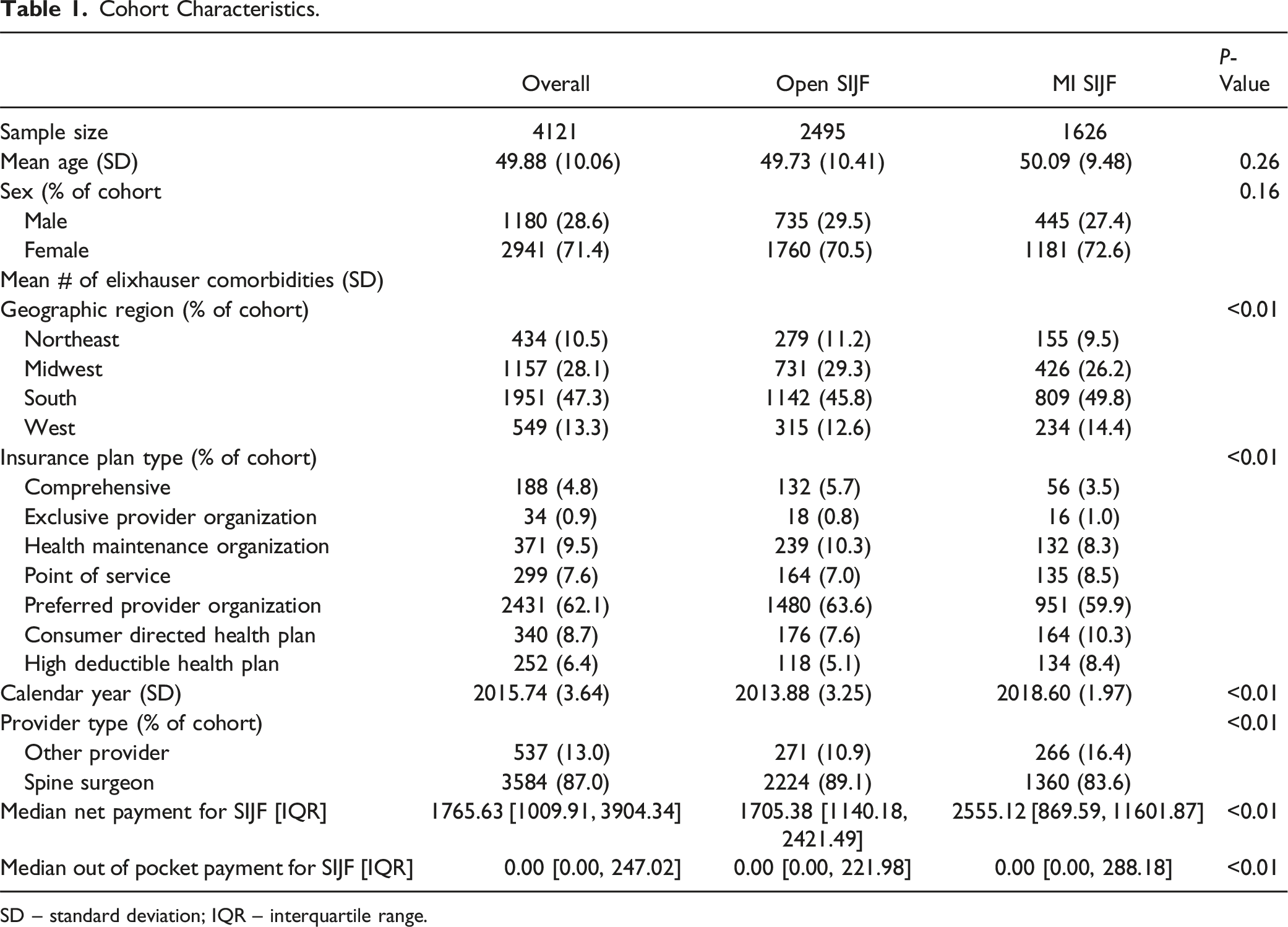
SD – standard deviation; IQR – interquartile range.
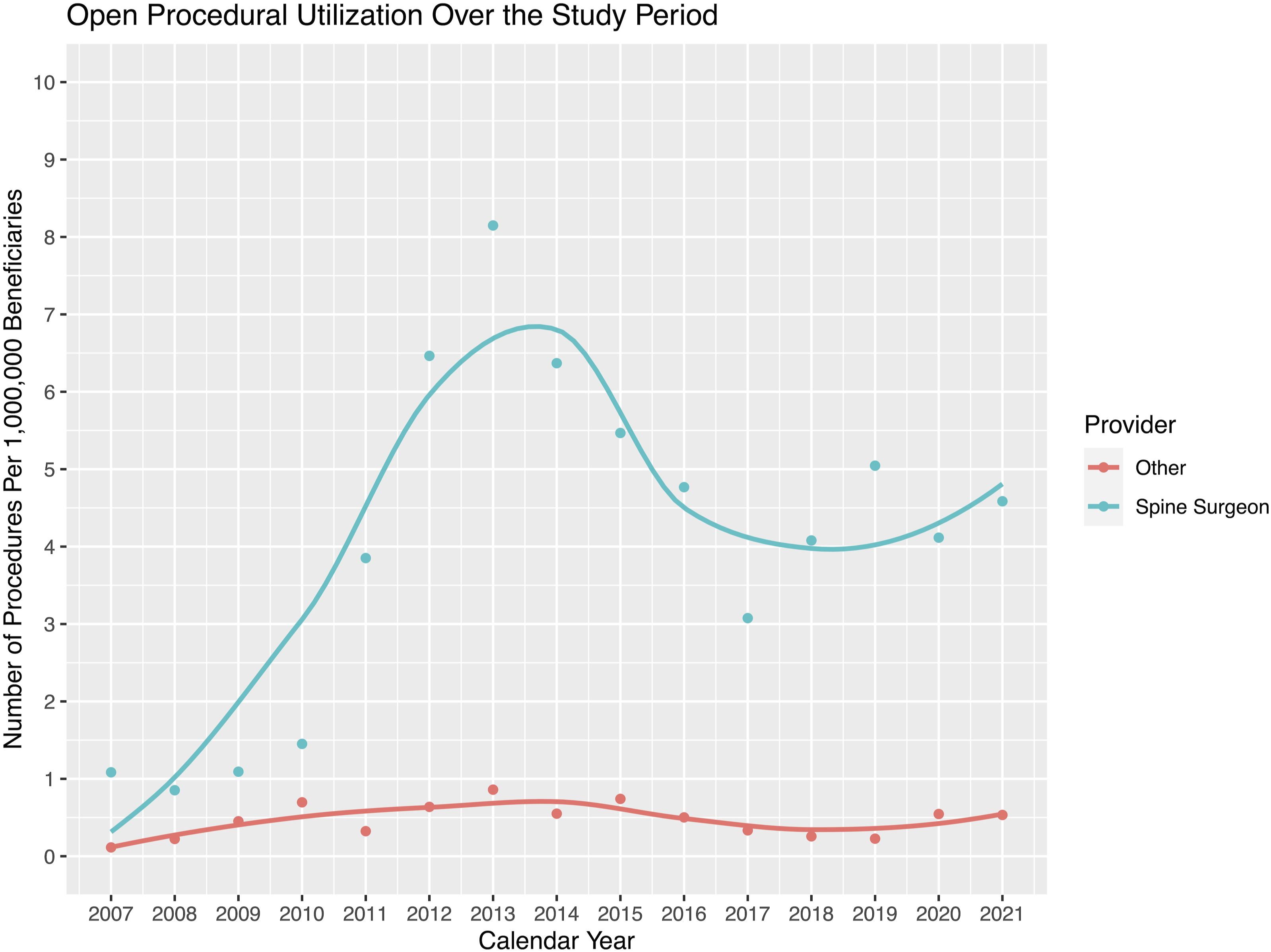
Procedural Utilization
SIJF utilization increased by 1176.2% over the course of the study period (P < .001), and the calendar year was a significant predictor of increased procedural utilization (IRR: 1.10 95% CI: 1.09-1.11 P < .001). This was driven primarily by an increase in MI SIJF volume (IRR: 1.17, 95% CI: 1.14-1.20, P < .001), as open SIJF utilization peaked in the year 2012. Moreover, open SIJF utilization in 2007-2011 was similar to that in 2017-2021 (104.0 vs 109.6 procedures per year). Unlike MI SIJF, open SIJF utilization was not significantly associated with time (IRR: 0.99, 95% CI: 0.98-1.01, P = .18). By contrast, the peak utilization for MI procedures occurred in 2021. Spine surgeons’ volume of MI SIJF increased by 258% over the study period (P < .001), while non-spine surgeon volume of MI SIJF increased by 990.9% (P < .001). Use of MI SIJF has experienced exponential growth since 2019 (Figures 1 and 2). Procedural utilization for MI SIJF throughout the study period. The y-axis depicts cases per 1,000,000 MarketScan beneficiaries, while the x-axis shows the time by calendar year since the CPT code for MI SIJF was created in 2015 until the end of the study period in 2021. A polynomial trendline is fit to the data. Procedural utilization for open SIJF throughout the study period. The y-axis depicts cases per 1,000,000 MarketScan beneficiaries, while the x-axis shows the time by calendar year throughout the study period (2007-2021). A polynomial trendline is fit to the data.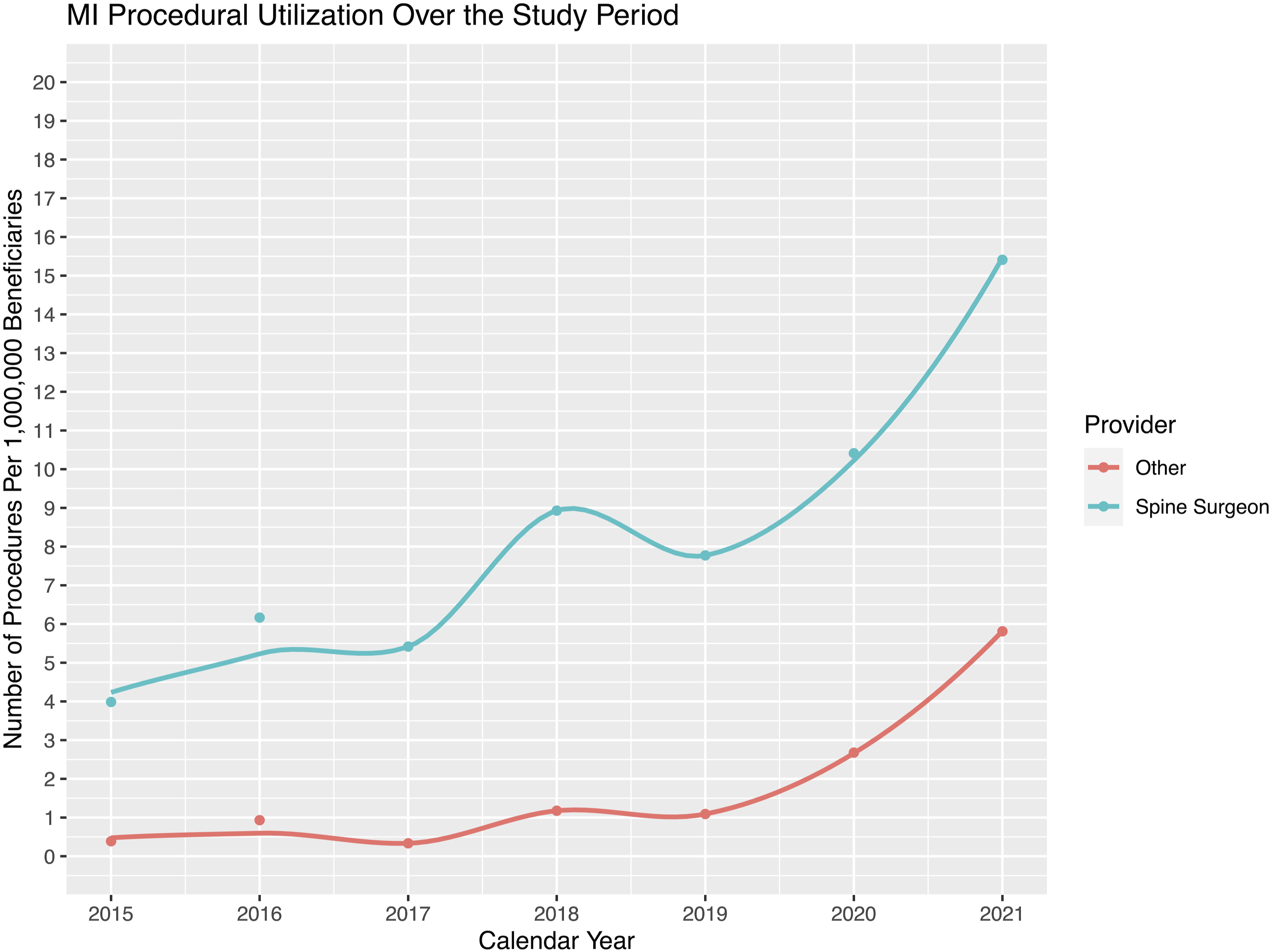
Costs
Patients paid a mean of $285 OOP for each SIJF (SD: $777, IQR: $0-242). Similarly, mean net payments made to the healthcare system by insurers per SIJF were $4780 (SD: $8,518, IQR: $1009-3904). Net payments made by insurers to the healthcare system for SIJF were significantly greater as the calendar year increased (Coefficient: $261, 95% CI: $167-355, P < .001), when a nonsurgeon conducted the procedure (Coefficient: $1,031, 95% CI: $255-1,807, P = .009), when the SIJF was MI (Coefficient: $3,923, 95% CI: $3243-4,604, P < .001), and when the patient was insured by a consumer-directed health plan (Coefficient: $1,740, 95% CI: $254-3,225, P < .001). Lastly, OOP payments made by patients for SIJF were also significantly greater if a patient underwent MI SIJF (Coefficient: $123, 95% CI: $59-188, P < .001), as well as if they were insured by a consumer-directed health plan (Coefficient: $176, 95% CI: $35-318, P = .014) or high-deductible health plan (Coefficient: $206, 95% CI: $56-357, P = .007).
Discussion
This report provides insights into the increasing utilization of SIJF procedures, both open and MI, within the privately insured population. Importantly, this manuscript is the first to comprehensively characterize trends in both open and MI SIJF costs and utilization within the context of a privately insured population. Notably, the research highlights a substantial surge in SIJF procedures, with a remarkable 1176.2% increase over the 15-year study period. This growth is predominantly attributed to the rise of MI SIJF, indicating a paradigm shift towards less invasive techniques. The study sheds light on the evolving landscape of SIJF interventions, with both spine surgeons and non-spine surgeons actively participating. Furthermore, the findings characterize the costs associated with SIJF procedures, emphasizing the economic implications of this treatment.
MI SIJF is gaining popularity for the treatment of chronic sacroiliac joint pain in multiple key patient populations. A recent report by Hersh et al. examining SIJF utilization in Medicare beneficiaries also highlighted a substantial increase in the popularity of MI SIJF procedures in recent years. 13 Our study complements and expands this prior work by providing insights into utilization trends in privately insured patients, who constitute a younger and healthier subset of the population. Additionally, this study characterizes a concomitant decline in open SIJFs since the introduction of MI SIJF as a discrete, billable procedure, highlighting that MIS and open procedures are economic substitutes for one another in certain instances. This has potential economic consequences for spine surgeons, who perform a significant majority of open SIJFs. Hersh’s study also demonstrates that non-spine surgeons are performing a significant share of MI SIJFs. In fact, in the Medicare population, non-spine surgeon utilization of MI SIJF surpassed that of spine surgeons in the years 2019 and 2020. The present study provides a second angle: in the privately insured population captured by MarketScan, spine surgeons still provide the majority of both MI and open SIJF, though non-spine surgeons have recently begun to perform a significant portion of these procedures. While the adoption of these procedures by non-spine surgeons may increase procedural accessibility, reduce costs, and allow practitioners with different training backgrounds to collaborate and collectively improve care, it remains to be seen whether this will be borne out in outcomes data.
However, neither the use of MI SIJF nor the presence of non-spine surgeon practitioners was found to be associated with decreased net payments from insurers to healthcare systems or out-of-pocket payments made by patients for their procedures. Therefore, despite the introduction of new techniques into the landscape of SIJF treatment, these costs associated with care are unchanging, if not increasing. This intriguing finding challenges the conventional notion in spine surgery and other fields that that less invasive procedures translate to reduced economic burden by virtue of reduced recovery times and postoperative lengths of stay.15-18 Moreover, this study highlights that the adoption of SIJF by non-spine surgeons, a phenomenon observed primarily in MI procedures, is not associated with decreased costs. This adds nuance to the economic landscape, suggesting that the involvement of non-spine surgeons in SIJF procedures may not lead to substantial cost savings, despite the potential advantages of increased procedural accessibility and collaboration among practitioners with diverse training backgrounds. As SIJF procedures and their utilization continue to change, ongoing research is warranted to unravel the intricate relationship between procedural techniques, provider specialties, and the associated economic outcomes.
The rapid increase in SIJF procedural utilization observed in this study may be partially related to changes in reimbursement rates and economic factors. It is likely that favorable reimbursement policies have influenced this trend, especially given the similar findings in the Medicare population, where MI SIJF saw a 382.8% increase from 2015 to 2020. 19 From 2010 to 2020, surgeon reimbursements for both open and MI SIJF procedures increased (20% and 44.9% inflation-adjusted, respectively), which may have contributed to the rise in procedural volumes. 19 The Medicare data demonstrate that procedural reimbursement remains a critical factor, even as overall payments to surgeons have trended downward in other orthopedic procedures like joint arthroplasty and spinal fusions. 20 The introduction of MI SIJF as a distinct procedure code in 2015 enabled surgeons and non-surgeon providers to bill independently, which may have contributed to increased procedural adoption. However, it is important to recognize that while reimbursement rates for surgeons have increased, hospital costs have also risen significantly across various orthopedic procedures. This discrepancy between increasing hospital payments and decreasing physician reimbursements has been observed in other fields. 20
Despite its contributions, this study has limitations. The analysis relies on retrospective data from a claims database, subject to inherent biases and coding inaccuracies. However, analysis of a longitudinal, multicenter, national claims database is also an optimal format for examining costs of care. Additionally, the focus on privately insured patients may limit the generalizability of findings to other populations. Despite this, previous studies have examined procedural utilization trends in other populations such as Medicare beneficiaries, which place this study’s findings in context. Furthermore, the study’s observational nature prevents the establishment of causal relationships. Next, granular data such as the number of implants, types of implants, and approach type for each SIJF are not available in the MarketScan databases. This prohibits evaluation of costs and utilization according to these factors. Moreover, this study does not have the capability to adequately report on complications following SIJF, as the coding present for complications following SIJF is largely nonspecific. Also, this study evaluated procedural utilization and costs from a time periods that bridges a change in ICD-coding for complications, further limiting the ability to draw accurate conclusions about postoperative complication rates. Future research should address these limitations, considering prospective designs and alternative patient cohorts to enhance the robustness and applicability of findings.
Conclusion
Privately insured patients have increasingly utilized SIJF over the past several years. This is predominantly due to the adoption of MI techniques by spine surgeons and non-spine surgeons alike.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Previous Presentations
This work was presented at the 2024 Spine Section Meeting.