
Abstract
Study Design
Retrospective Cohort Study.
Objective
To identify risk factors for sacroiliac (SI) joint fusion after instrumented spinal fusion.
Methods
Patients were identified from the PearlDiver BiscayneBay database. Patients who underwent 1 level (CPT: 22840), 3-6 vertebral segment (22842), and 7+ vertebral segment spinal fusions (22843 and 22844) were identified. Patients were separated based on whether they received an SI joint fusion (27280 and 27279) after their spinal fusion. A univariate analysis and multivariate logistic regression was performed to evaluate the associations between patient factors and incidence of SI joint fusion.
Results
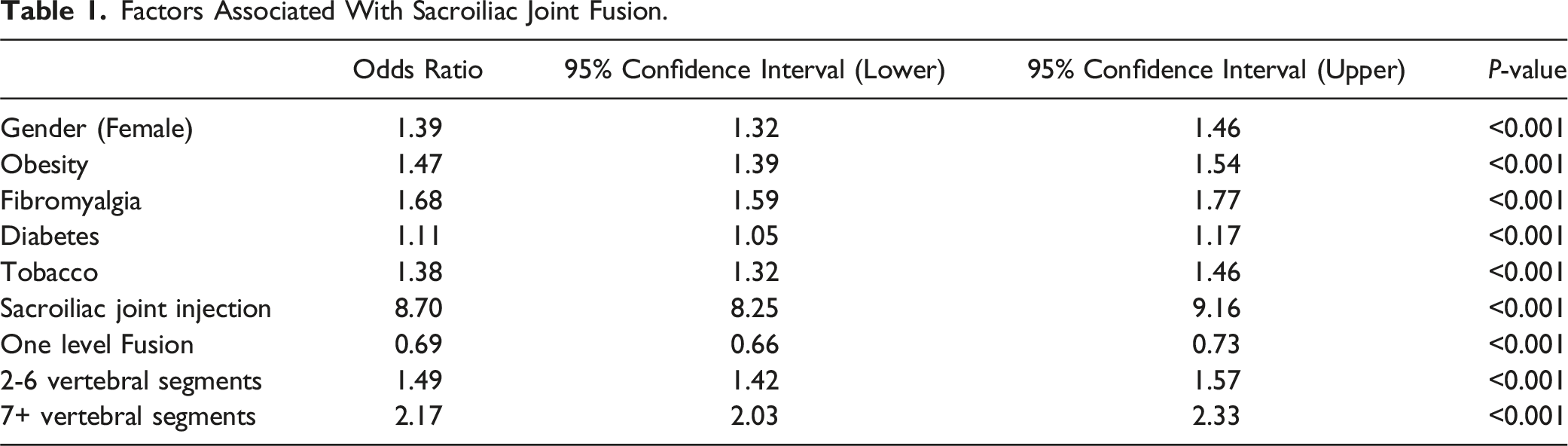
549,625 patients who underwent posterior spinal fusions were identified, 6068 of whom underwent subsequent SI joint fusion (1.1%). Factors associated with future SI joint fusion included female gender, patients with obesity, fibromyalgia, diabetes, tobacco use, increased construct length, and prior SI joint injection. Prior SI joint injection had the highest odds ratio (OR: 8.70; 95% CI: 8.25-9.16; P < 0.001), followed by 7+ vertebral segment (OR: 2.17; 95% CI: 2.03-2.33; P < 0.001) and 3-6 vertebral segment fusion (OR: 1.49; 95% CI: 1.42-1.57; P < 0.001).
Conclusions
The highest predictor of requiring subsequent SI joint fusion is a prior SI joint injection. We also found that longer fusion constructs are associated with increased risk for future SI joint fusion.
Introduction
Posterior spinal fusion is often used as treatment for many different spinal pathologies ranging from single level unstable spondylolisthesis to adult spinal deformity. Correspondingly, there has been a general increase in the incidence of spinal decompression and fusion surgery.1,2 There are numerous complications that can occur after a spinal fusion including but not limited to nerve injury, dural tears, infection, instrumentation failure, deep vein thrombosis/pulmonary embolism, pseudarthrosis, adjacent segment disease, and continued low back pain. 3 The incidence of low back pain after surgery ranges from 5%–30%. 4 The reasons for post-operative low back pain are multifactorial but 1 common cause is adjacent segment disease. The proposed mechanism is that abnormal mechanical loading and increased motion through the adjacent segment leads to accelerated degeneration of the proximal or distal adjacent segment. 5 One specific joint seeing increased attention to degeneration and as a potential source of post-operative back pain is the sacroiliac (SI) joint.
The SI joint is a diarthrodial joint that connects the axial skeleton to the lower extremities. 6 The joint helps absorb the stresses from axial compression and rotational stresses 6 and can see upwards of 4800N in shear force. 7 What is unique about the SI joint is that it sees relatively little motion, with approximately 4° of rotation and 1.6 mm of translation. 8 Despite minimal motion, the SI joint is thought to be a source of low back pain in upwards of 15%–30% of patients.4,6,9,10 One specific factor that has been linked to accelerated SI joint deterioration and SI joint pain is prior lumbar fusion, with multi-level fusions and fusions to the sacrum being noted to be risk factors for SI joint pain.4,11 However, most of the studies looking at SI joint pain after a prior lumbar spinal fusion are either retrospective in nature11-13 or systematic reviews,6,14 with few prospective studies.7,15 In addition, many of these studies do not examine which of these patients end up progressing to require an SI joint fusion. Also, there has been no large-scale database study to date examining this issue. The purpose of our study was to perform a large-scale database study looking at the risk factors for SI joint fusion after previous spinal fusion.
Materials and Methods
Study Database
We performed a retrospective cross-sectional review of patients identified from the PearlDiver BiscayneBay Patient Claims database (Colorado Springs, CO, USA). The PearlDiver database includes de-identified medical record claims data from 161 million individual patients from all payer types including commercial Medicare, Medicaid, government, and cash payers except Kaiser and Tricare. Institutional review board (IRB) approval and patient consent was not required as the database is de-identified and data is aggregated.
Patient Cohort
The study population was defined as patients greater than the age of 18 who underwent posterior spinal fusions and those that underwent posterior spinal fusions and subsequent SI joint fusions. Posterior spinal fusion patients were categorized by Current Procedural Terminology (CPT) codes into single interspace (CPT: 22840), 3-6 vertebral segments (22842), 7-12 vertebral segments (22843), and 13+ vertebral segment posterior spinal instrumentation (22844), excluding patients with fusions solely in the cervical spine (22595 and 22600). We grouped patients with 7-12 and 13+ vertebral segments together to increase the number of patients in that cohort. Patients were separated based on whether they received an SI joint fusion after their spinal fusion (27280 and 27279). There was no specific restriction on the time frame between the initial spinal fusion and the SI joint fusion, only that the SI joint fusion occurred after the initial spinal fusion. The following patient factors and their association with future SI joint fusion were evaluated: age, gender, obesity, fibromyalgia, diabetes, tobacco use, SI joint injection prior to initial spinal fusion, and spinal fusion length. Patients receiving SI joint injection were identified by CPT codes 27096 or G0260.
Data Analysis
Univariate chi-squared analysis was used to analyze the associations between patient factors and the need for subsequent SI fusions and are reported as odds ratios (OR) with 95% confidence intervals (CI). A multivariable logistic regression method to control for confounding factors was used to analyze the independent effect of each patient factor and are reported as adjusted OR and 97.5% CI. Statistical significance was defined as P < 0.05. All statistical analysis was conducted using the R statistical software integrated within PearlDiver.
Results
A total of 549,625 patients who underwent posterior spinal fusions were identified, 6068 of whom underwent subsequent SI joint fusion (1.1%). There was a total of 315,212 females (57%) and 234,413 males, of whom 3946 (65%) females and 2122 (35%) males who underwent subsequent SI joint fusion. The average age, in years, of patients who underwent posterior spinal fusions was 58.8 vs 59.7 in patients who had subsequent SI joint fusion.
Univariate Analysis
Factors Associated With Sacroiliac Joint Fusion.
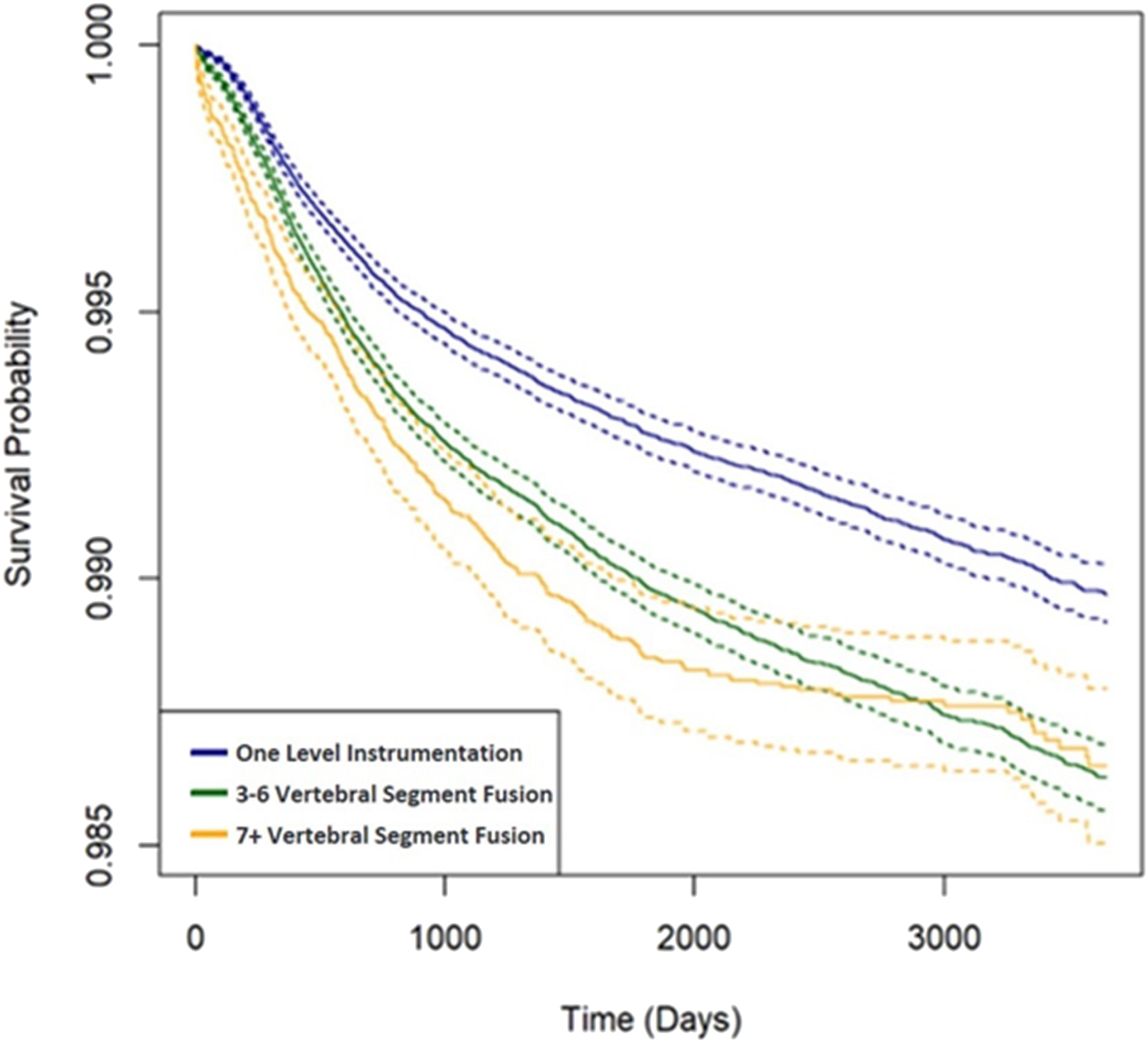
Kaplan-Meier Survival Curve comparing fusion construct length and future sacroiliac joint fusion. Solid line represents survival probability, dashed lines represent standard deviations.
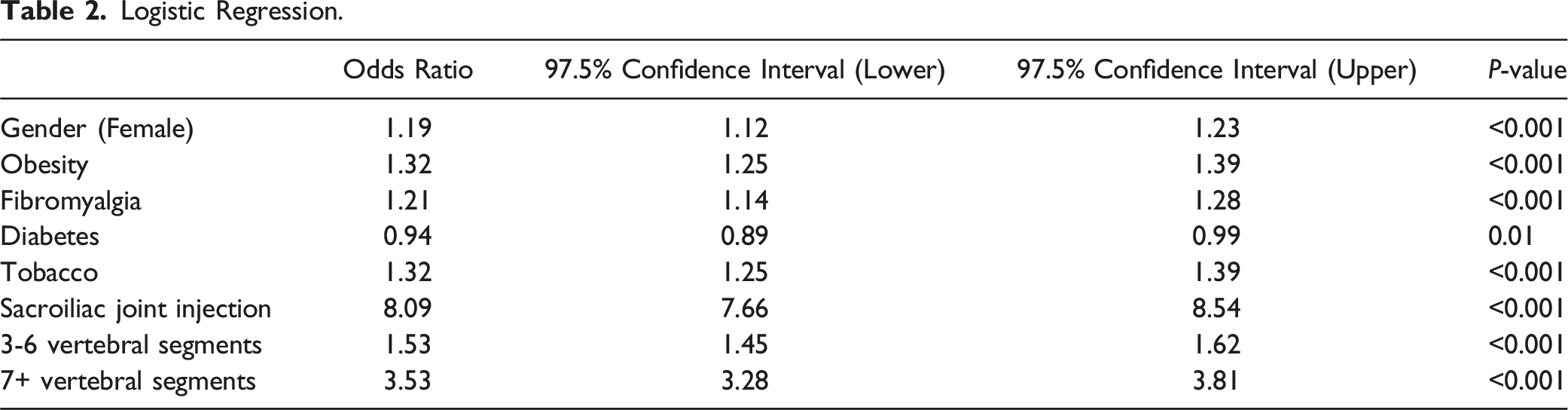
Logistic Regression Analysis
Logistic Regression.
Discussion
Our study found multiple risk factors that were associated with requiring subsequent SI joint fusion: female gender, obesity, fibromyalgia, diabetes, tobacco use, SI joint injections prior to spinal fusion, 3-6 vertebral segment fusions, and 7+ vertebral segment fusions. Prior SI joint injections, 7+ vertebral segment fusions, and 3-6 vertebral segment fusions had the highest odds ratios of requiring a future SI joint fusion. Interestingly, with a multivariable analysis, diabetes is a slightly protective co-morbidity. This could be because surgeons are more hesitant to re-operate on a patient with diabetes due to concerns over post-operative complications.
Patients who undergo spinal fusions are at risk for adjacent segment disease and SI joint pain. A retrospective study by Ha et al 7 found that 75% of patients in the spinal fusion group showed evidence of SI joint degeneration compared to 38% in the control group. However, that study focused on radiographic SI joint degeneration. The rates of SI joint pain after spinal fusions vary between 3%–90%.4,16-19
It is thought that after fusion of the spine the SI joint sees altered forces and compensatory hypermobility which can lead to accelerated degeneration and be a potential pain generator. A finite element study by Ivanov et al 20 found that lumbar fusion increased the magnitude of sacral angular motion and stresses across the SI joint. They also found that a two-level L4-S1 fusion experienced greater sacral angular motions and stresses across the SI joint compared to single level L4-5 or L5-S1 fusions. A L4-S1 fusion increased stress across the SI joint by up to 6 times an intact model. A similar finite element study by Yao et al 21 found that an L5-S1 fusion increased maximum contact pressure and stress to upwards of 676% and 424% respectively. Baria et al 22 performed a cadaveric study looking at SI joint motion and found a 67% increase in SI joint vertical translation during flexion-extension loading following L4-L5 instrumentation, and a 77% increase following L4-S1 instrumentation. Unoki et al 4 found that as the number of fused segments increased, so did the incidence of SI joint pain. They found that 1 fused segment had an incidence of SI joint pain of 5.8% compared to 22.5% for at least 4 segments. Guan et al 11 also found that SI joint pain occurred more frequently in patients with multiple operative segments. This agrees with our study, which found that longer fusion construct lengths increased the odds of requiring a future SI joint fusion. Interestingly our study found that although constructs of 7+ vertebral segments failed (requiring SI joint fusion) at a higher rate initially, the survival curves eventually evened out with constructs of 3-6 vertebral segments (Figure 1). This could be because longer constructs place more stress initially on the SI joint causing accelerated degeneration and all SI joints that were going to degenerate, degenerate quicker and get an earlier fusion. Meanwhile, shorter constructs, because they place less stress on the SI joints, degenerate at a slower rate and are fused at a slower rate. However, the ultimate incidence of SI joints requiring fusion could be similar despite varying construct lengths.
In addition to construct length, there is thought that fusing to the sacrum increases the rate of SI joint pain as well. Although Maigne et al 9 did not find a statistically significant difference, they found that patients with an L5-S1 fusion had an increased frequency of positive SI joint blocks. Unoki et al 23 found that patients with fixed fusion to the sacrum experienced significantly higher rates of SI joint pain (32/1%) compared to those without fusion to the sacrum (12/7%). They also found that patients with fixed fusion to the sacrum have a shorter mean time of onset of SI joint pain (3.78 months vs 8.63 months). Similarly, Ha et al 7 found that patients with fusion to the sacrum had significantly higher rates of SI joint degeneration (100% vs 64%). However, this study is slightly limited by the small number of patients in each cohort. The higher rates of SI joint pain after fusion to the sacrum is thought to be because the distal adjacent non-fused joint would be the SI joint compared to a fusion that ends at the L5 vertebral body where the L5-S1 joint would be the distal adjacent joint. Therefore, the SI joint would be expected to see larger forces with a fusion that extends to the sacrum as opposed to the L5 vertebral body.
Because of the high rates of SI joint pain after spinal fusions, some surgeons advocate for simultaneous SI joint fusion at the time of spinal fusion. However, there is still the question of how much instrumentation of the SI joint is required. Unoki et al 24 found that fixation to the pelvis with S2 alar iliac (S2AI) screws reduced postoperative rates of SI joint pain to 4.2%, compared to 16.7% in patients fused to L5 and 26.1% in patients fused to the sacrum. On the other hand, Finger et al 13 found that there was no difference in rates of SI joint pain between patients with fusion to the sacrum or with sacropelvic fixation. In fact, they found that 34.5% of patients with sacropelvic fixation had worsening/new onset of SI joint pain post-operatively. This is similar to findings by Noureldine et al 12 who found that S2AI screws did not lead to SI joint fusion at long term follow-up and 43% of patients with S2AI instrumentation experienced post-operative SI joint pain. Interestingly though they found that fixation with fully threaded S2AI screws had lower rates of post-operative SI joint pain compared to partially threaded S2AI screws (32% vs 52.5%). While S2A1 screws in isolation do not reduce rates of post-operative SI joint pain, it is possible that a formal SI joint fusion procedure at the time of index spinal fusion could reduce post-operative SI joint pain. Another study by Noureldine et al 25 found that no patients with simultaneous SI joint fusion with a fusion device developed post-operative SI joint pain while 44.6% with just S2AI screw fixation without a fusion device developed post-operative SI joint pain. Their hypothesis is that the addition of the fusion device prevents rotational micro-motion around a single S2AI screw and provides an enhanced environment for bony fusion of the SI joint. In a cost-utility analysis, Ackerman et al 26 found that simultaneous SI joint fusion in multi-level lumbar fusion patients, compared to multi-level lumbar fusions to the sacrum, leads to an additional 5-year cost of $2421 and a gain of 0.14 quality adjusted life years, resulting in an incremental cost-effectiveness ratio of $17,293 which is similar to a total knee arthroplasty. They found that fusing the SI joint appears to be cost-effective over a 5-year timeline if the incidence of SI joint pain after multi-level lumbar fusion to the sacrum exceeds 25%. This is thought to be because despite the higher initial upfront cost, the cost offsets over time mostly due to subsequent treatment for SI joint pain in patients who did not undergo initial SI joint fusion. However, it is not clear which patients are at high risk for developing post-operative SI joint pain and which specific patients may benefit from a simultaneous SI joint fusion.
Strengths and Limitations
This study does have a few limitations. First, this is a retrospective large database review and depends on correct documentation of all patients’ co-morbidities and procedures. Therefore, incorrect or incomplete documentation could potentially lead to under- or over-estimation of the impact of certain co-morbidities. Secondly, because all patient co-morbidities are based on diagnostic coding and not laboratory values, we are not able to determine the severity of the patient co-morbidity and how it relates to outcomes. Third, because we utilized CPT codes to identify patients that underwent spinal fusion, we are unable to determine exactly which levels were fused and if those levels included the sacrum. In addition, different surgeons can code the same procedures differently. Similarly, we are unable to control for surgical technique and the degree of soft tissue injury, instrumentation used, or post-operative spinal alignment. However, this study to the best of our knowledge is the first large database study looking at risk factors for SI joint fusion after a spinal fusion. A large population is required to have sufficient power as the incidence of future SI joint fusion after a spinal fusion is relatively low at 1.1%., and we were able to examine over 500,000 patients who underwent spinal fusions.
Conclusions
In conclusion, our study found that the highest risk factor for requiring a subsequent SI joint fusion after a spinal fusion is a prior SI joint injection. We also found that constructs of longer length were associated with increased risk for future SI joint fusions, although the overall incidence tended to converge over the long term.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Clifford Lin: Grants/Contracts: AO Spine North America, Medtronic. Consulting: Depuy. Meeting/Travel Support: North American Spine Society Biologics Committee. Jung U Yoo: Royalties/Licenses: Osiris Therapeutics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request.