
Abstract
Study Design
Retrospective Cohort Study
Objective
Spinal fusion, specifically constructs connected to pelvic bones, has been consistently reported as a predisposing factor to sacroiliac joint (SIJ) pain. The aim of this study is to compare SIJ outcomes in patients with constructs to the pelvis following instrumentation vs instrumentation plus fusion of the SIJ.
Methods
Data of study subjects was extracted from a prospectively maintained database as well as retrospectively collected from records at a tertiary academic medical center in the United States between 2018 and 2020.
Results
A cohort of 103 patients was divided into 2 groups: 65 in Group 1 [S2AI screw without fusion device] and 38 in Group 2 [S2AI screw with fusion device]. None of the patients in Group 2 developed postoperative SIJ pain compared to 44.6% in Group 1. Sacroiliac joint fusion occurred in all Group 2 but none of Group 1 patients. The postoperative Visual Analogue Scale (VAS) for lower extremity (LE) pain (.8 vs .5; P = .03) and postoperative Oswestry Disability Index (ODI) (18.7 vs 14.2; P < .01) were significantly higher in Group 1. The rate of distal junctional break, failure, and/or kyphosis (DJBFK) and time to DJBFK were not significantly different between the two groups, and the rate of DJBFK did not change in the presence of multiple covariates.
Conclusion
The SIJs carry the heavy load of long lumbosacral fusion constructs extending to the pelvis. Simultaneous SIJ instrumentation and fusion decreases the risk of disability, prevents the development of postoperative SIJ pain, and may also protect the S2AI screw from loosening and failure.
Introduction
The sacroiliac joint (SIJ) is a relatively large, diarthrodial joint connected by a strong fibrous, synovial fluid-containing capsule and spans a mean surface area of 17.5 cm2. 1 Generation of SIJ pain may be intra-articular (e.g.,, arthritis) or extra-articular in nature, the latter of which is related to injuries to the adjoining ligaments, tendons, and muscles. Risk factors include pregnancy, scoliosis, leg length discrepancies, and spine surgery, among others.2-4 Spinal fusion, specifically constructs connected to pelvic bones, has been consistently reported as a predisposing factor to SIJ pain.5-8 The most likely mechanism is significant axial loading combined with rotational shearing forces from a fixed/fused block of the vertebral column following spinal fusion, subsequently generating SIJ pain. Biomechanical studies studying motion across the normal and/or fused SIJ are now shedding light on this previously ambiguous topic.9,10
The aim of this study is to compare SIJ outcomes in patients with constructs to the pelvis following instrumentation vs instrumentation plus fusion of the SIJ. Based on clinical experience that we previously reported,11,12 we hypothesize that (1) concurrent instrumentation and fusion of the SIJ is associated with improved SIJ outcomes in patients with long lumbosacral constructs to the pelvis, and (2) the use of a fusion device, as opposed to instrumentation alone, is essential to ensure SIJ fusion and protect the base of the construct, which is the S2AI screw.
Materials and Methods
Patient Population & Study Design
Data of study subjects was extracted from a prospectively maintained database as well as retrospectively collected from records at a tertiary academic medical center in the United States between 2018 and 2020. A cohort of all consecutive patients who underwent bilateral SIJ instrumentation with S2AI screws, with and without a fusion device (SiCure® System, Alevio Spine, Birmingham, AL, USA), were included in this study. Patients with preoperative SIJ pain, patients who underwent pelvic instrumentation techniques other than S2AIs, patients who underwent unilateral pelvic instrumentation and/or fusion, and patients with less than 3 months of follow-up were excluded from this study (Figure 1). In all subjects, the diagnosis of postoperative SIJ pain was achieved using a combination of (1) at least 3 positive validated clinical/provocative tests—namely, pelvic compression, pelvic distraction or gapping, pelvic torsion or Gaenslen’s, thigh thrust or posterior shear, Faber or Patrick’s, Fortin finger, and sacral thrust,13-16 and (2) complete relief or significant reduction of SIJ pain following local anesthetic injections under fluoroscopic guidance.17-19 Computed tomography (CT) scans obtained after a minimum of 3 months of follow-up were used to document the presence or absence of SIJ fusion. The study protocol (Pro00023643) was approved by the institutional review board (IRB) prior to data collection, which included demographic, preoperative, perioperative, and postoperative patients’ variables. Sacroiliac joint outcomes of interest consisted of occurrence and progression of SIJ pain, evidence of SIJ arthropathy on imaging studies, and documented SIJ fusion on CT scans at follow-up. Obtaining patient consent was waived by the IRB due to the retrospective nature of the study. Flowchart of patients included in the study.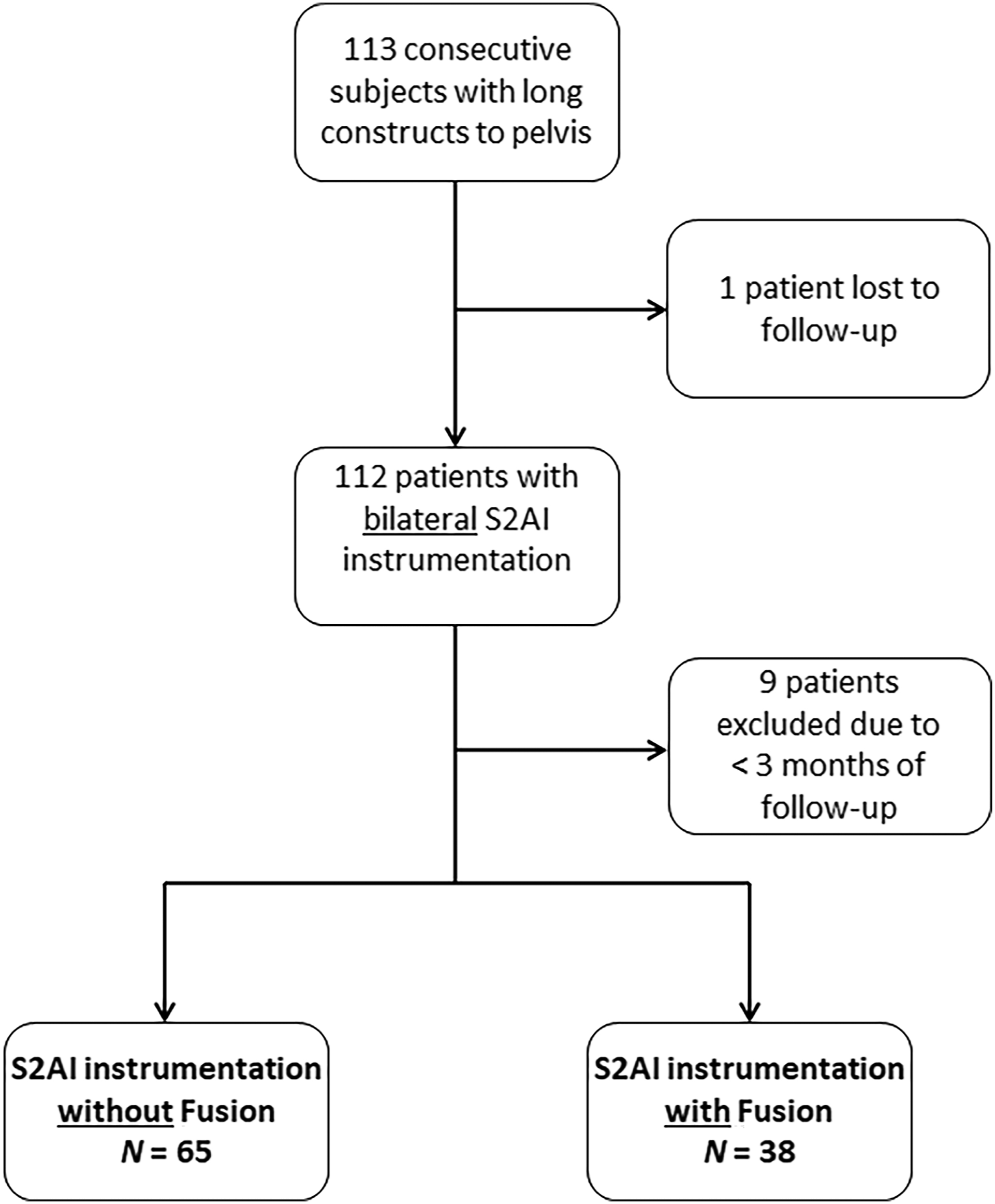
Statistical Analysis
Frequency counts and percentages were used to report categorical variables, whereas continuous variables were reported with means and standard deviations (SD). The association between categorical variables was assessed using the chi-square test or Fischer’s exact test with the continuity correction. The differences in distribution of continuous variables (e.g., age, body mass index [BMI], etc.) across the categorical variables (e.g., Group 1 [S2AI without Fusion] vs Group 2 [S2AI with Fusion device]) was investigated via the Mann–Whitney U test. Multivariate binary logistic regression analysis was conducted to assess the significance of a group (Group 1 vs Group 2) coefficient in the presence of a covariate. A repeated-measures Analysis of Variance (ANOVA) test was used to assess the differences in pre-vs post-procedure values of continuous variables across groups (Group 1 vs Group 2). A P-value of less than .05 was considered significant. Statistical analyses were performed using IBM SPSS Statistics Version 26 (IBM Corp., Armonk, NY, USA).
Results
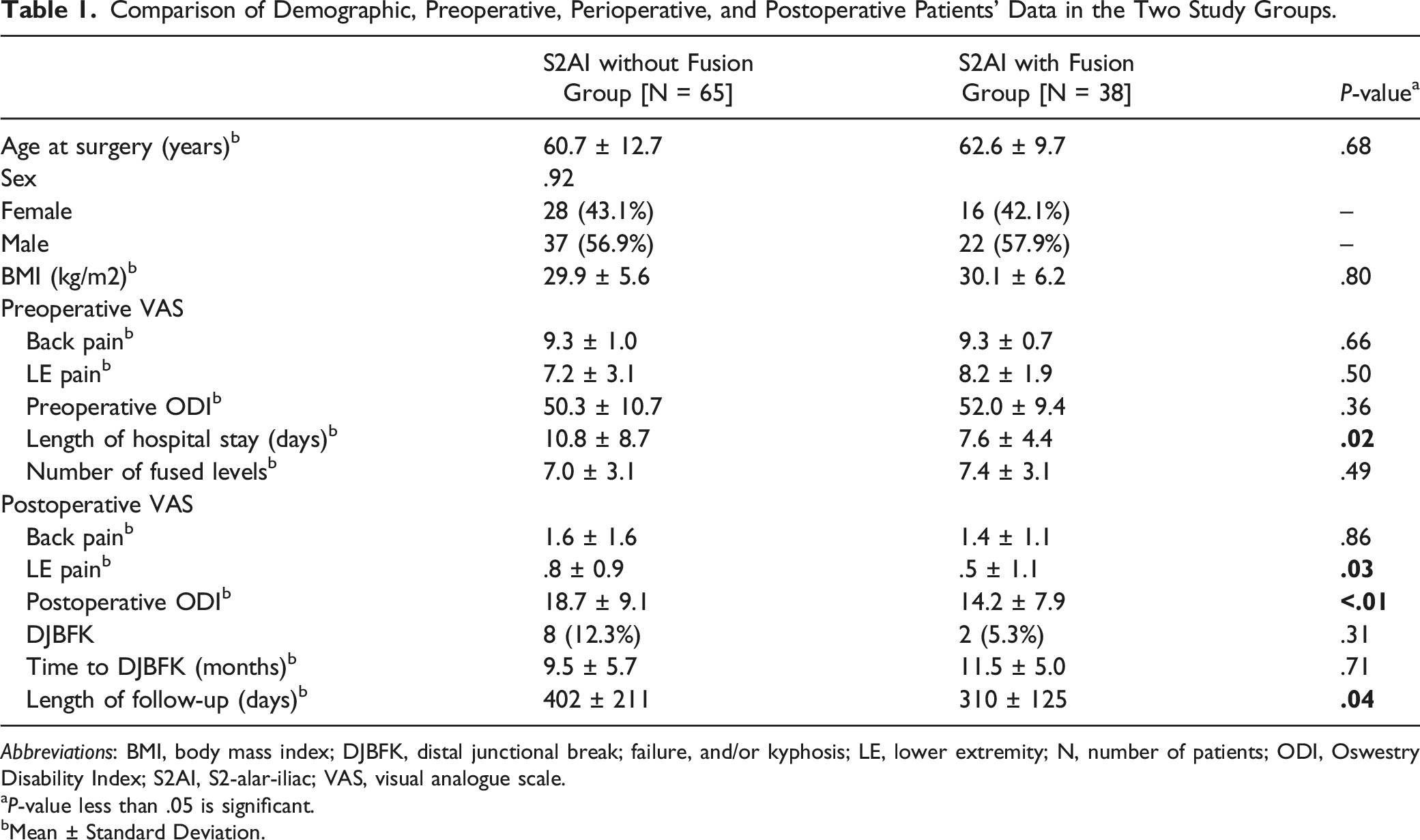
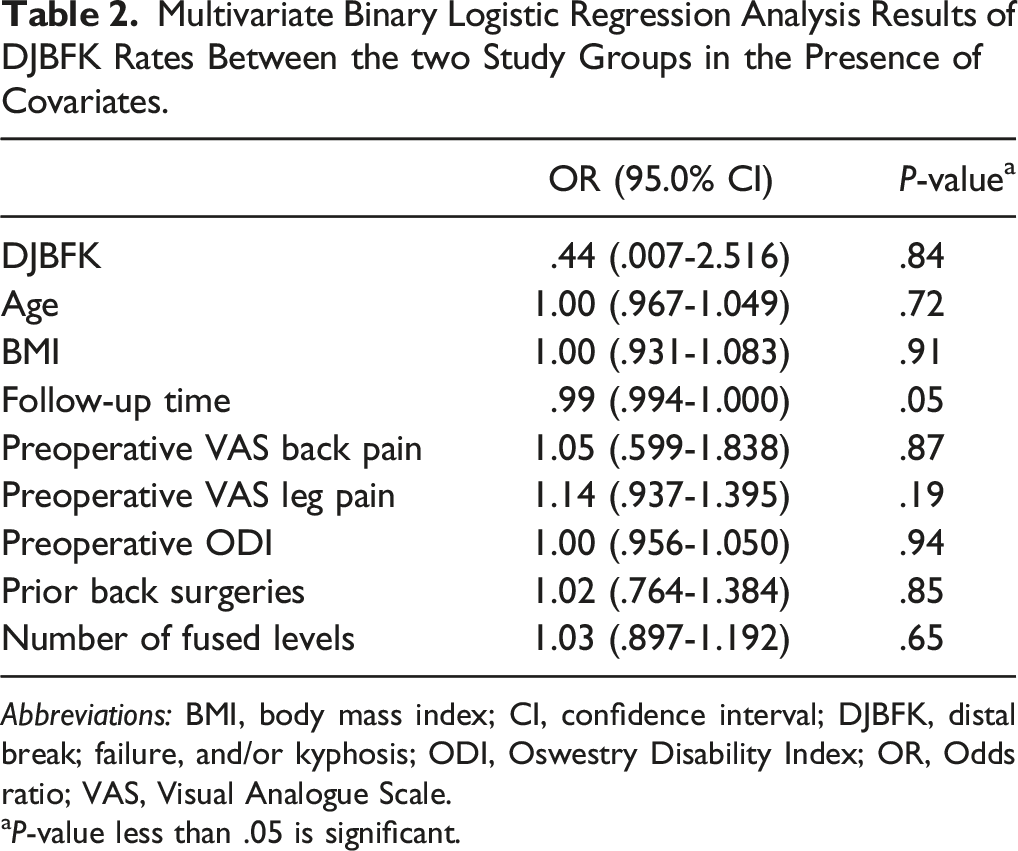
The study cohort consisted of 103 patients with long spinal constructs who underwent S2AI instrumentation, of whom 38 had concomitant fusion with an SIJ fusion device (Figure 2). There were no differences between Group 1 [S2AI without fusion device] and Group 2 [S2AI with fusion device] in terms of age, sex, BMI, preoperative Visual Analogue Scale (VAS) for back and lower extremity (LE) pain, preoperative Oswestry Disability Index (ODI), and number of fused levels (Table 1). The length of hospital stay (10.8 vs 7.6 days; P = .02) and length of follow-up (402 vs 310 days; P = .04) were significantly higher for Group 1. Both the postoperative VAS for LE pain (.8 vs .5; P = .03) and postoperative ODI (18.7 vs 14.2; P < .01) were also significantly higher in Group 1 but not the postoperative VAS for back pain (Table 1). Moreover, the rate of distal junctional break, failure, and/or kyphosis (DJBFK) and time to DJBFK were not significantly different between the 2 groups. Of note, the rate of DJBFK did not change in the presence of multiple covariates, including age, BMI, follow-up time, preoperative VAS for both back and LE pain, preoperative ODI, number of prior back surgeries, and number of fused levels (Table 2). Illustration showing the S2AI screw and SIJ fusion device in place. The presence of 2 parallel of lines of support inside the same joint likely prevents rotational micro-motion around the S2AI screw, and the fusion device provides an environment for bone growth between the sacral and iliac surfaces of the SIJ. (a) 2021 globalmedicalillustrations.com. Used with permission. Comparison of Demographic, Preoperative, Perioperative, and Postoperative Patients’ Data in the Two Study Groups. Abbreviations: BMI, body mass index; DJBFK, distal junctional break; failure, and/or kyphosis; LE, lower extremity; N, number of patients; ODI, Oswestry Disability Index; S2AI, S2-alar-iliac; VAS, visual analogue scale. aP-value less than .05 is significant. bMean ± Standard Deviation. Multivariate Binary Logistic Regression Analysis Results of DJBFK Rates Between the two Study Groups in the Presence of Covariates. Abbreviations: BMI, body mass index; CI, confidence interval; DJBFK, distal break; failure, and/or kyphosis; ODI, Oswestry Disability Index; OR, Odds ratio; VAS, Visual Analogue Scale. aP-value less than .05 is significant.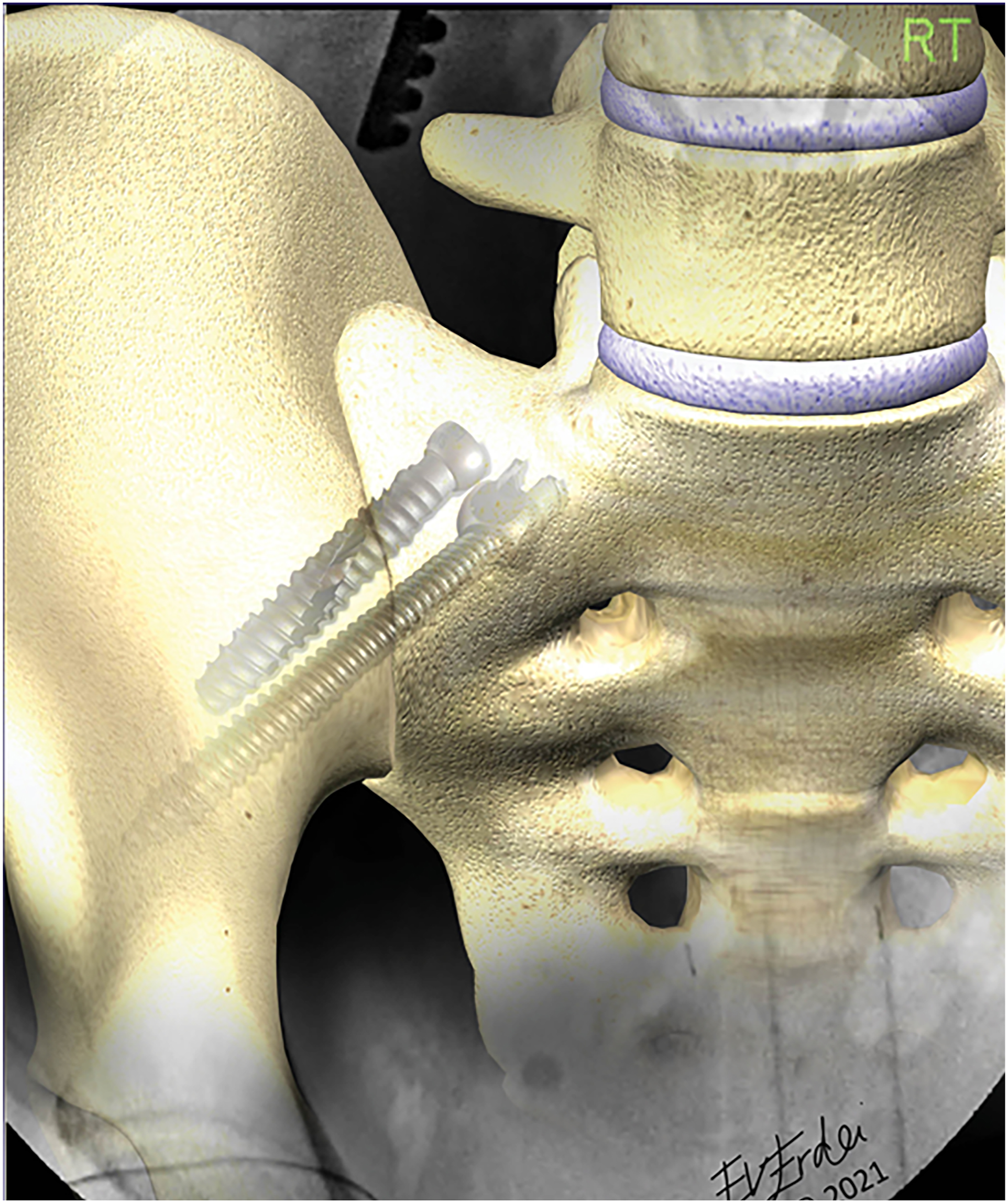
Comparison of SIJ Outcomes in the two Study Groups.
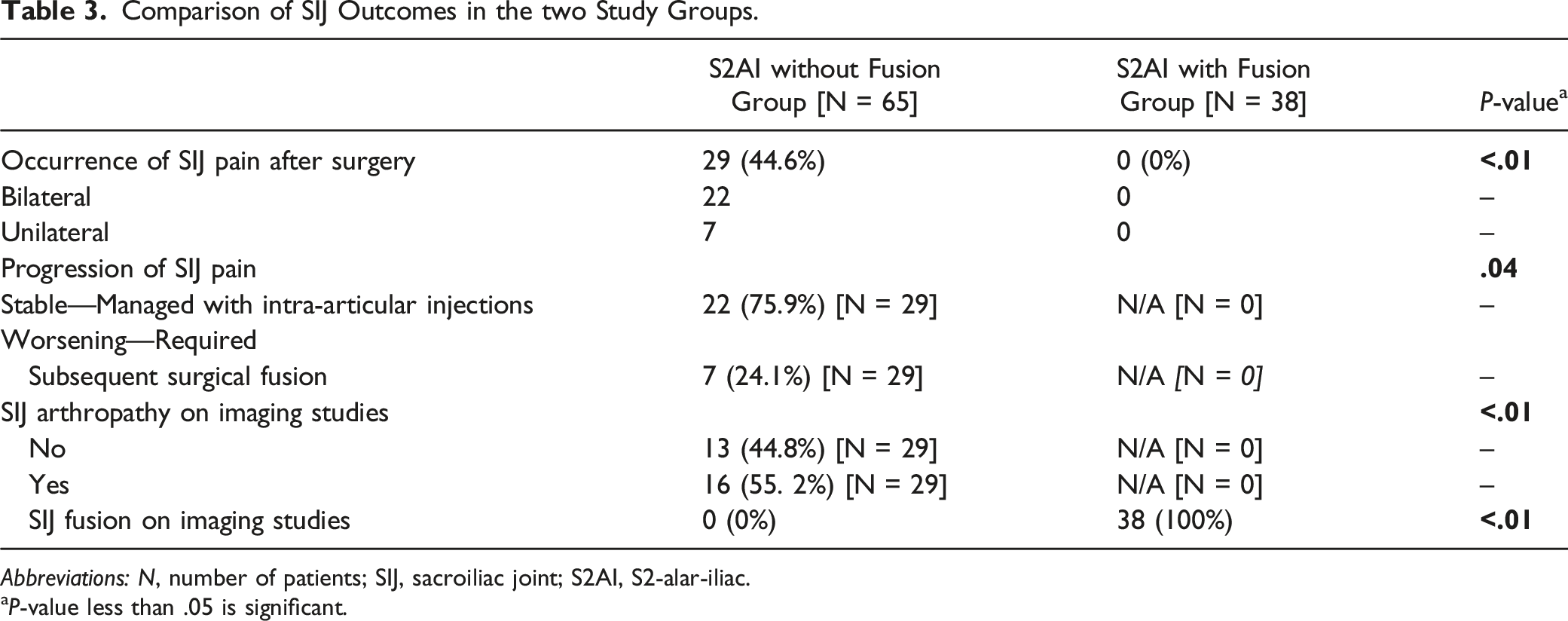
Abbreviations: N, number of patients; SIJ, sacroiliac joint; S2AI, S2-alar-iliac.
aP-value less than .05 is significant.
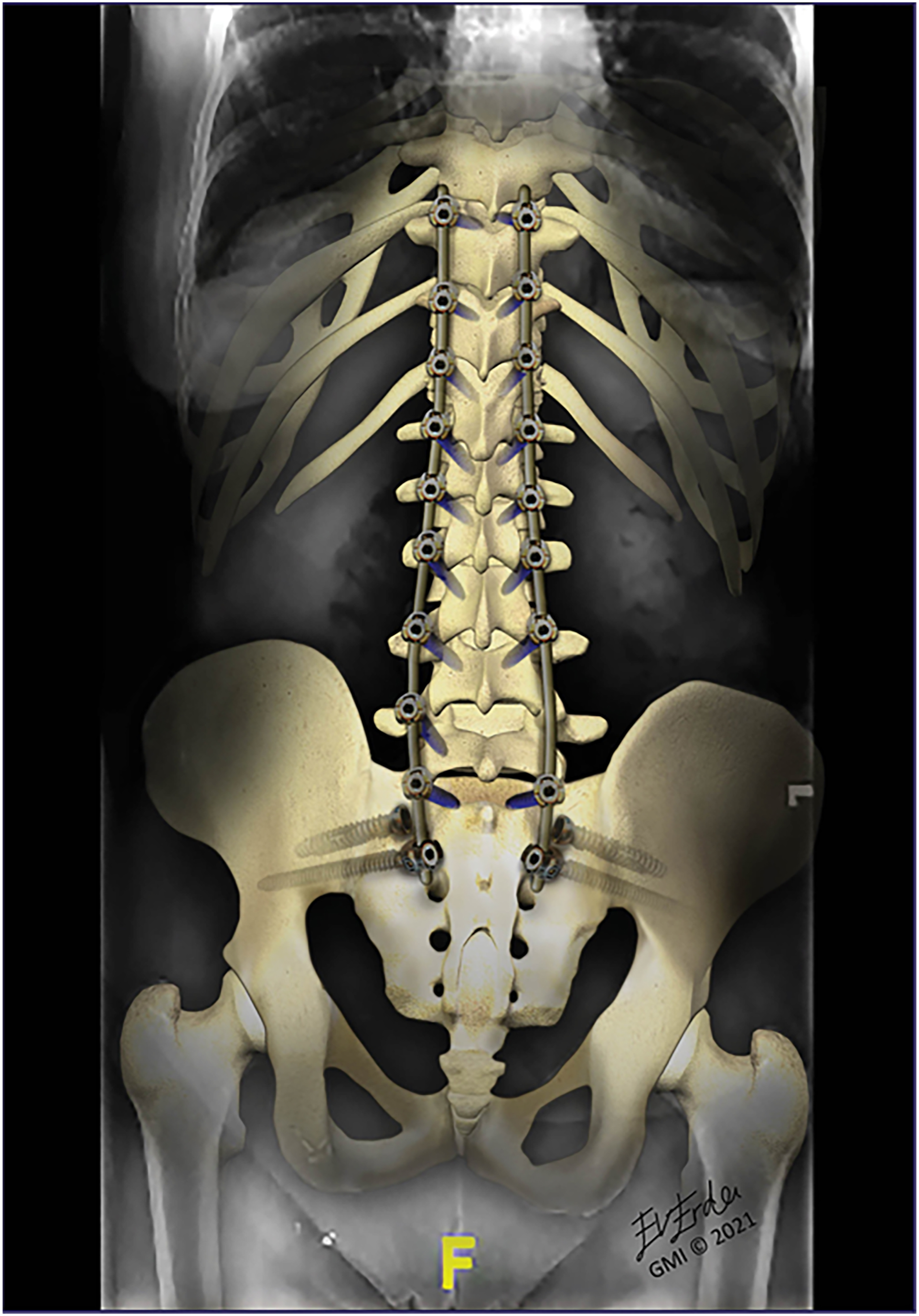
Artistic rendering of a long throaco-lumbo-scaro-pelvic construct, highlighting successful fusion of the SIJs, with the S2AI screws and fusion devices in place. (a) 2021 globalmedicalillustrations.com. Used with permission.
Discussion
The results of this study strongly concur with the clinical observation of and patient-reported better SIJ outcomes following simultaneous pelvic instrumentation and fusion compared to pelvic instrumentation alone. The two study groups were similar in terms of age, sex, BMI, preoperative VAS for back and LE pain, preoperative ODI, and number of fused levels (Table 1), providing a less confounded platform for comparison and analysis of the SIJ outcomes. The follow-up time was longer in Group 1 (Table 1), mainly because we shifted our practice to concurrent fusion in almost all our patients over the last year after observing improved SIJ outcomes, which was the catalyst for conducting this comparative study.
The literature is rich in studies reporting biomechanical and hardware-related complications in patients with long lumbosacral constructs, including new/persistent back pain, pelvic stress fractures, infections, distal and/or proximal adjacent level disease, instrumentation failure (rod break, screw loosening/break, etc.), and pseudarthrosis.20-24 Although the definition of a long fusion construct is not standardized yet (L2 or higher vs thoracolumbar junction or higher), pelvic fixation is nowadays universally utilized to decrease the rates of caudal instrumentation failure and pseudarthrosis. 25 In this study, we included only patients who underwent pelvic fixation with S2AI screws due to its superior or at least equivalent outcomes compared to traditional pelvic instrumentation techniques.26-29 Nevertheless, instrumentation failure and sacral fractures also occur with S2AI instrumentation, as demonstrated in recent studies. In a series of 156 patients with S2AI fixation, Hyun et al. (2021) reported a peri-screw lucency (>2 mm) in 2.2%, screw head dislodgement in 2.2%, screw fracture in 1.9%, distal device breakage in 3.2%, and sacral fractures in 1.9% 30 ; SIJ pain was described in 6.4% of their cohort, 80% of whom improved following SIJ injections. 30 We recently reported our experience with different types of S2AI screws, where the fully threaded type was associated with better observed and patient-reported SIJ outcomes compared to the partially threaded type. 12 The rates of SIJ pain were relatively higher than those reported in the literature (32–52.5% vs 3.2–8.8%).12,26,27,30,31 The rate of SIJ pain in Group 1 of this study (44.2%) is comparable to that of our previous study (Table 3). One explanation of our higher SIJ pain rates following S2AI instrumentation compared to the literature could be that every patient with a long spinal construct returning to clinic with low back and/or LE pain is screened for SIJ pain using the standard provocative tests, and the diagnosis is confirmed with pain relief following local injections.13-19
Interestingly, none of the patients with either S2AI screw types had SIJ fusion on imaging in our previous study, 12 an observation that was noted again in patients with S2AI instrumentation alone of this study (Table 3). It seems that the addition of a fusion device is integral to ensure SIJ fusion, likely by (1) preventing rotational micro-motion around the S2AI screw due to the presence of 2 parallel lines of support inside the same joint, and (2) by providing an environment for bone growth between the sacral and iliac surfaces of the SIJ (Figure 2); these hypotheses require validation via future biomechanical studies, however.
The concurrent S2AI instrumentation/fusion group was also associated with significantly improved postoperative VAS for LE pain and ODI (Table 1). The lower pain and disability scores could be directly related to the fact that none of the patients in Group 2 developed SIJ pain during the follow-up period, compared to 44.6% of patients in the S2AI instrumentation alone group (Table 3). The most plausible explanation is the occurrence of SIJ fusion in Group 2, which was documented on imaging studies of Group 2 patients at follow-up (Table 3). These findings, however, should be substantiated with forthcoming controlled trials. It is noteworthy, however, that the .3 cm (ie, 3 points) and 4.5 points difference in postoperative VAS for LE pain and postoperative ODI, respectively, in our cohort did not exceed the minimum clinically important difference (MCID) of VAS for leg pain at 5 points 32 and ODI at 12.8 points 33 as reported in the literature.
We speculated whether the addition of an SIJ fusion device would influence the rate of DJBFK. Although the rate of DJBFK was higher in Group 1 (12.3% vs 5.3%), our results showed no significant difference in the rate of DJBFK between the 2 groups, which did not change in the presence of other covariates (Table 2). In a standing/sitting position, the SIJ is constantly suffering from micro-traumatic injuries incurred by rotational shear forces of a heavy, fused vertebral block over a relatively immovable SIJ, which is the immediate next caudal joint. 1 We believe that patients with long constructs to the pelvis and concomitant SIJ fusion will most likely develop hip arthropathy in the intermediate- and long-term follow-up period, given that the hip is the following caudal joint that will suffer from the overwhelming shear forces of a heavy proximal construct. Indeed, some of the patients in Group 2 did report new onset hip pain, which is worthwhile investigating in future studies.
Conclusion
The SIJs carry the heavy load of long lumbosacral fusion constructs extending to the pelvis. Simultaneous SIJ instrumentation and fusion decreases the risk of disability, prevents the development of postoperative SIJ pain, and may also protect the S2AI screw (i.e., the distal junction and base of the construct) from loosening and failure. Future studies are needed to address the effect of long constructs on the next non-instrumented caudal joint, the hip, which will inevitably suffer from the overwhelming forces of a long proximal construct with fused SIJs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.