
Abstract
Study Design/Setting
Retrospective cohort analysis
Objectives
This study evaluates utilization and demographic trends for sacroiliac joint (SIJ) fusions across the United States (US).
Methods
Patients who underwent SIJ fusion from 2010-2021 were identified within the PearlDiver national database using International Classification of Disease (ICD-9, ICD-10) and Current Procedural Terminology (CPT) codes. Indications for trauma, malignancy, or infection were excluded. Demographic, clinical, and procedure characteristics were recorded along with annual utilization rates. Annual percent change (APC) was calculated to identify increasing or decreasing utilization from prior years. Negative binomial regression was performed to project subsequent utilization for 2022-2028. Chi-squared analysis followed by post-hoc comparisons were used to compare differences in diagnostic indications and clinical features associated with SIJ fusion across regions. Bonferroni adjustments were applied to P-values for pairwise analyses.
Results
Overall, 18 032 patients (69.8% female, mean age = 51.0
Conclusion
As SIJ fusion is increasingly utilized to treat refractory SIJ-based pain, establishing evidence-based guidelines, improving diagnostic strategies, and defining indications are imperative to support growing applications within clinical practice.
Introduction
Chronic back pain remains a significant challenge, imparting substantial economic and clinical burden, globally. Within the United States (US), low back pain is the leading cause of disability and represents the largest proportion of healthcare expenditures nationwide.1,2 While acute presentations carry a relatively more favorable prognosis in the ambulatory setting, chronic forms generally dispose patients to a more insidious clinical course, placing increasing restrictions on daily function, cognitive well-being, and patient quality of life. 3 Sacroiliac joint (SIJ) dysfunction is one such source of refractory low back pain, accounting for up to 30% of cases.4,5
Deriving SIJ-based causes of chronic low back pain is associated with significant diagnostic challenges stemming from non-specific clinical and radiographic presentations and multifactorial pathogenesis.6,7 Patients commonly present with combinations of pain involving the lumbar region, gluteal muscles, groin, and hips, which can further obscure an accurate diagnosis of the underlying etiology. 7 As a result, pain sourced from SIJ pathologies is often overlooked.
Beyond diagnosis, lack of standardized clinical guidelines for assessing SIJ fusion efficacy, moreover, contributes to discrepancies in strategies to manage refractory back pain that may stem from SIJ pathology. The relative absence of well-defined diagnostic criteria and clear operative indications likely underlies differences seen in treatment strategies for SIJ-based pain across clinicians and surgeons, especially in context of definitive, operative modalities such as SIJ fusion. 8 Conventional open SIJ fusion procedures are coupled with a high risk of complications, while conservative strategies have been reported as largely inadequate in improving patient-reported outcome measures (PROMs) 9 Advances in operative techniques and technologies, however, have advanced minimally invasive (MIS) approaches to substantially improve the therapeutic efficacy of SIJ fusions for patients with intractable SIJ pain.10,11 Nonetheless, utilization remains relatively minimal compared to other spine procedures, likely owed to the sparsity of literature around SIJ fusion.
While emerging evidence to support use of MIS SIJ fusion is incipient, findings across studies remain promising. As increasing utilization of SIJ becomes a developing prospect, guidelines surrounding diagnostic strategies and indications will need to be further refined. The aim of this study is to outline national SIJ utilization trends across the US and describe current clinical applications. It is hypothesized that SIJ utilization will demonstrate an increasing trend throughout the study period, and that population characteristics of patients undergoing SIJ fusion will exhibit significant variation across geographical regions.
Methods
Patients who underwent SIJ fusion from 2010 to Q1 of 2021 (January to April 2021) were queried from the PearlDiver Mariner Database (PearlDiver Technologies, Fort Wayne, IN), which includes more than 41 billion HIPAA-compliant inpatient and outpatient records 12 across the United States (US). The database contains information on patient demographics, diagnoses, and procedures from both major private and public insurers. Patients undergoing SIJ fusion and all relevant demographic and procedural data were recorded using Current Procedural Terminology (CPT) codes and International Classification of Disease, ninth and 10th edition (ICD-9 and ICD-10) codes (Supplemental Table 1). Patients with a history of pelvic surgery and surgical indications for trauma, malignancy, or infection were excluded from this study. Informed consent and institutional review board (IRB) approval were not required as all patient data is de-identified.
Patients were divided into one of four US geographic cohorts based on the region in which they underwent their SIJ fusion (1): West, (2) Midwest, (3) Northeast, and (4) South. States comprising each geographical region are listed in Supplemental Table 2. Demographic characteristics were recorded as mean values and proportions for continuous and categorical variables respectively. Annual procedure utilization was reported from 2010-2021, and procedures were additionally stratified into conventional open or minimally invasive (MIS) approaches, the latter which only included 2015-2021 given that CPT coding for MIS SIJ fusions were only first introduced in 2015. Diagnostic indications were categorized based on the most common operatively treated SI pathologies, which included spondyloarthropathy-induced (SpA) sacroilitis, SIJ degeneration (i.e. spondylosis), and SIJ instability. 13 Patients were included within a diagnostic category only if it was reported as the primary diagnosis at the time of their procedure. Percentages for each diagnostic indication were calculated as a proportion of total cases performed nationally. Clinical features of interest were based upon whether patients had the following prior to undergoing their SIJ fusion procedure: lumbosacral degeneration, previous lumbar fusion, and diagnostic SIJ injection. Diagnostic SIJ injections were defined by a therapeutic SIJ injection which was specifically performed and confirmed with imaging modalities (i.e. ultrasound-guided).
Statistical Methods
Annual utilization was further expressed as a percentage of the total number of cases performed throughout the study period, and APC (annual percent change) was obtained by adapting the following calculation for percent change — where positive and negative percentage values indicate growth and declining use, respectively, from the previous year
14

Following assessment of data dispersion, a negative binomial regression model was used to predict SIJ fusion utilization for subsequent years from 2022-2028.
Pearson chi-squared analysis was conducted to outline associations between diagnostic indications and clinical features of patients undergoing SIJ fusion by region, followed by post-hoc analysis to determine specific differences between regions. The Bonferroni adjustment was applied to all presented P-values for pairwise analyses to account for increases in family-wise error rates associated with multiple comparisons. All statistical analysis was conducted using Rstudio (Version 4.4.2).
Results
Demographic Characteristics
Demographic Characteristics Across Geographical Regions.
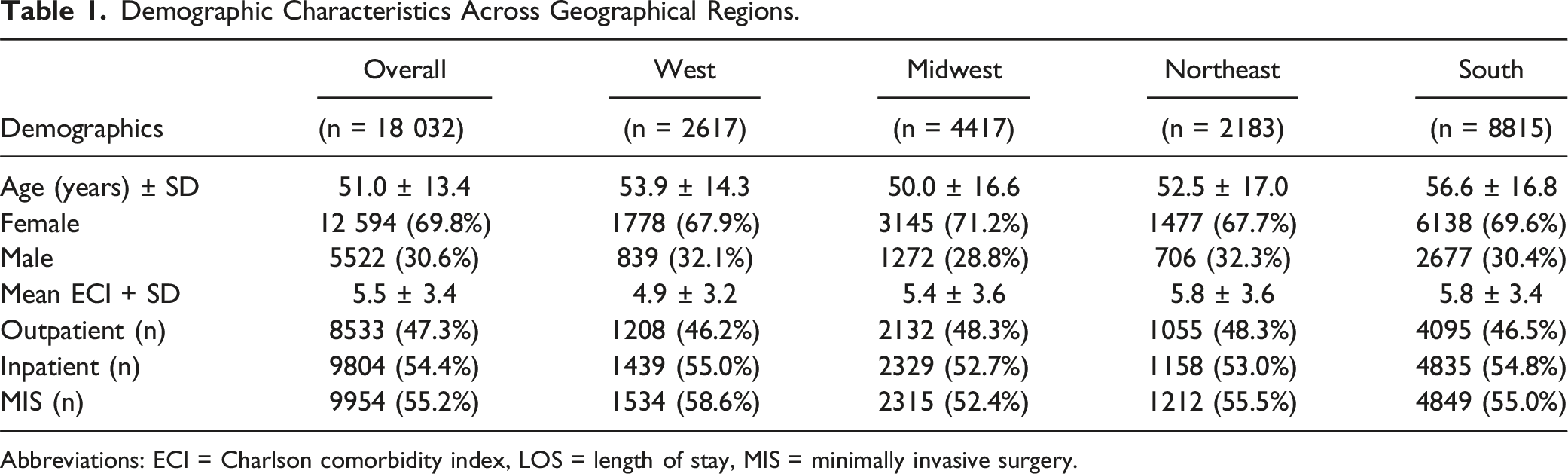
Abbreviations: ECI = Charlson comorbidity index, LOS = length of stay, MIS = minimally invasive surgery.
Utilization Trends
Nationally, utilization of SIJ fusions on average increased 58.6% annually from 2010-2013, transiently decreased 11.7% from 2013-2014, then increased again by 28.2% annually from the start of 2014 to 2020. From 2020-2021, nationwide use of SIJ fusion fell precipitously, decreasing by -61.7%. The greatest APC was seen from 2010-2011 and 2014-2015, wherein SIJ fusion use increased 196% and 81% respectively. Throughout the entirety of 2010-2021, utilization of SIJ fusion increased on average by 33.5% annually, and 709% overall. When excluding 2021, the average APC was 53.3% and 2015% overall for 2010-2020. (Figure 1). Annual utilization trends in SIJ fusion procedures nationally and by geographical region from 2010-2021.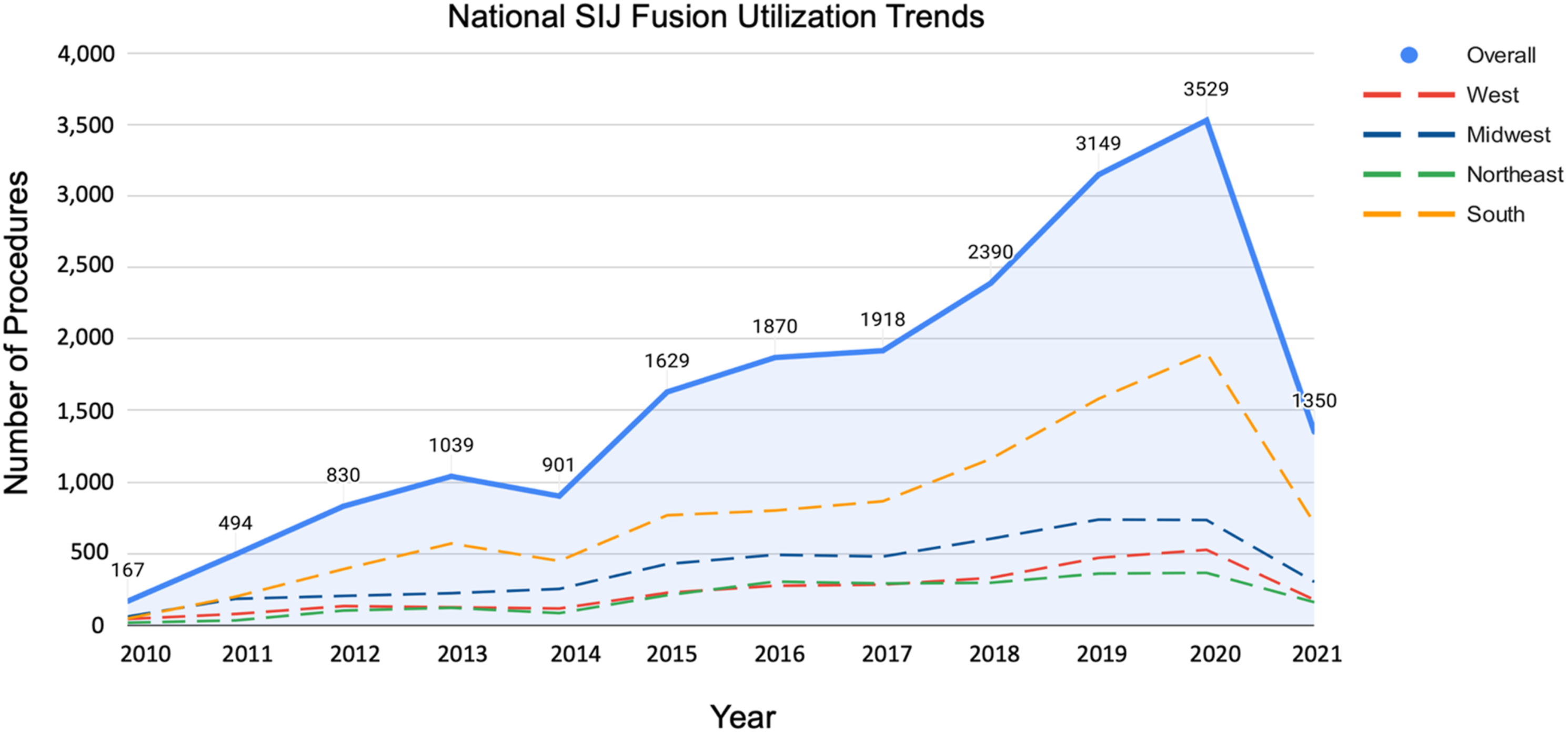
Within regions, the Northeast was the only region to undergo a period of decreased MIS utilization throughout 2015-2020, decreasing by -8% in 2017. Remaining geographical regions sustained uniform growth in utilization up until the beginning of 2021, with the largest annual percent increase for MIS procedures occurring in 2019 for the West (41.6%), Midwest (50.1%), and South (52.2%), reaching a record number of procedures for all regions by end of 2020.
Projected Utilization
Utilization trends were projected to 2022 to 2028 premised on historical data from 2010 to 2021. Based on the negative binomial regression model, utilization of SIJ fusion procedures is projected to continue increasing over the years 2022 to 2028. The number of procedures is expected to demonstrate an average APC of 63.8% from 1350 cases at the end of 2021 to 16 195 in 2028, attaining an overall increase of 1100% through this time period. In excluding 2021, the average APC decreases to 31.1%, with an overall percent increase of 230.3% from 2022-2028 (P = .001). The model equation and corresponding regression line for projected SIJ fusion utilization are displayed in Figure 2. Negative binomial regression model for SIJ fusion procedures based on historical utilization from 2010-2021. The model equation used to calculate predicted values for SIJ fusion utilization from 2022-2028 are presented. Model significance was p=<.001.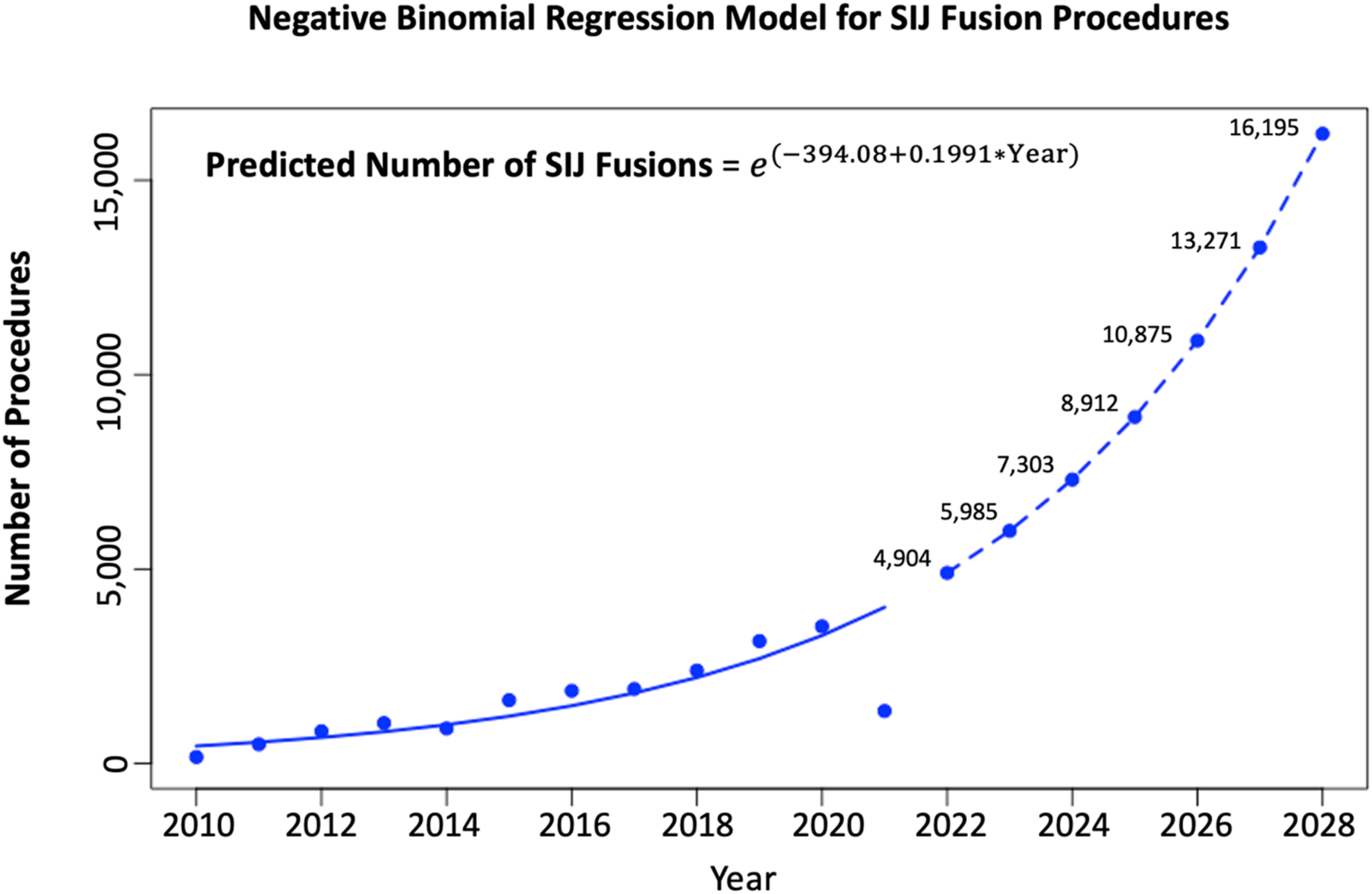
Diagnostic Indications and Clinical Features
Amongst patients undergoing SIJ fusion, SpA-induced sacroiliitis was by far the most prevalent diagnosis category, accounting for 51% (n = 9826) of cases nationally. Prevalence varied widely across regions, with the South having a statistically significant higher percentage compared to all other regions (60%; all P < .001), and West having the lowest proportion of cases (45%). SIJ instability was the second most common diagnostic indication, comprising 20% (n = 3853) of total cases, with the highest proportions in the Midwest (25.9%; all P < .001). A smaller fraction of procedures were indicated for SIJ degeneration at 13% (n = 2505) nationally, with the Northeast performing the highest percentage of cases (17.7%; all P < .001). National percentages for diagnostic indications are depicted in Figure 3. Diagnostic categories of patients undergoing SIJ fusions across the US. Categories were based on the most common SIJ pathologies indicated for operative treatment. Patients were categorized based on the primary diagnosis recorded at the time of their procedure such that they were only included in one of three diagnostic categories. Error bars represent a 10% standard error.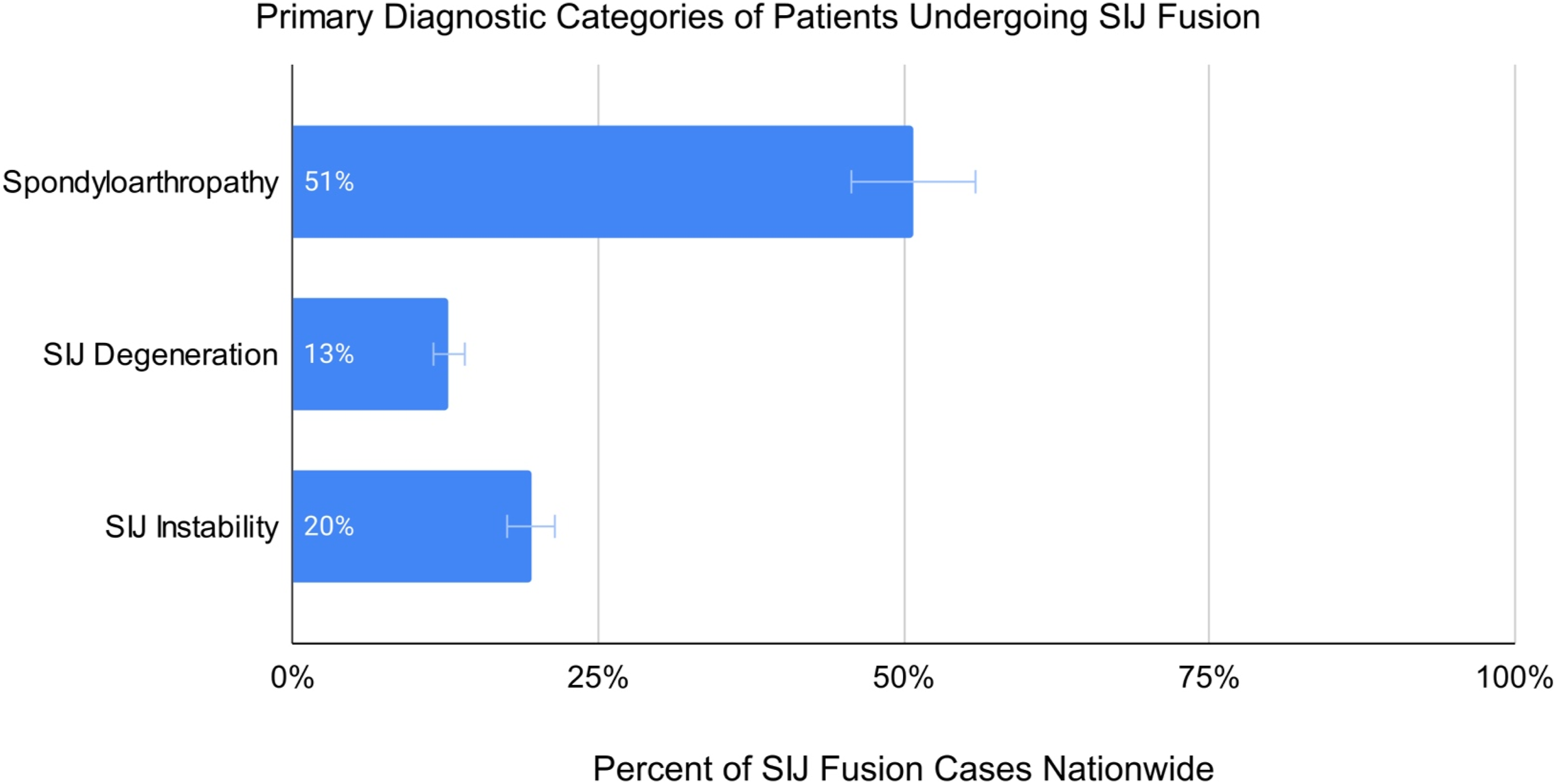
With regard to clinical features, lumbosacral degeneration was only found amongst 6.2% (n = 1156) of cases nationwide, with negligible regional variation across patients undergoing SIJ fusion. Prior history of lumbar fusion was a relatively common feature of SIJ fusion patients, with 18% (n = 3468) patients overall. Nationally, diagnostic SIJ injections were administered in less than the majority of patients undergoing SIJ fusion and varied by region, with only 45% (n = 8670) overall having received a diagnostic injection preoperatively. The lowest rate of preoperative diagnostic SIJ injections was found within the West at 41.5% (all P < .001) and was significantly lower than all other regions (Figure 4). Clinical features of patients undergoing SIJ fusions across the US. Error bars represent a 10% standard error.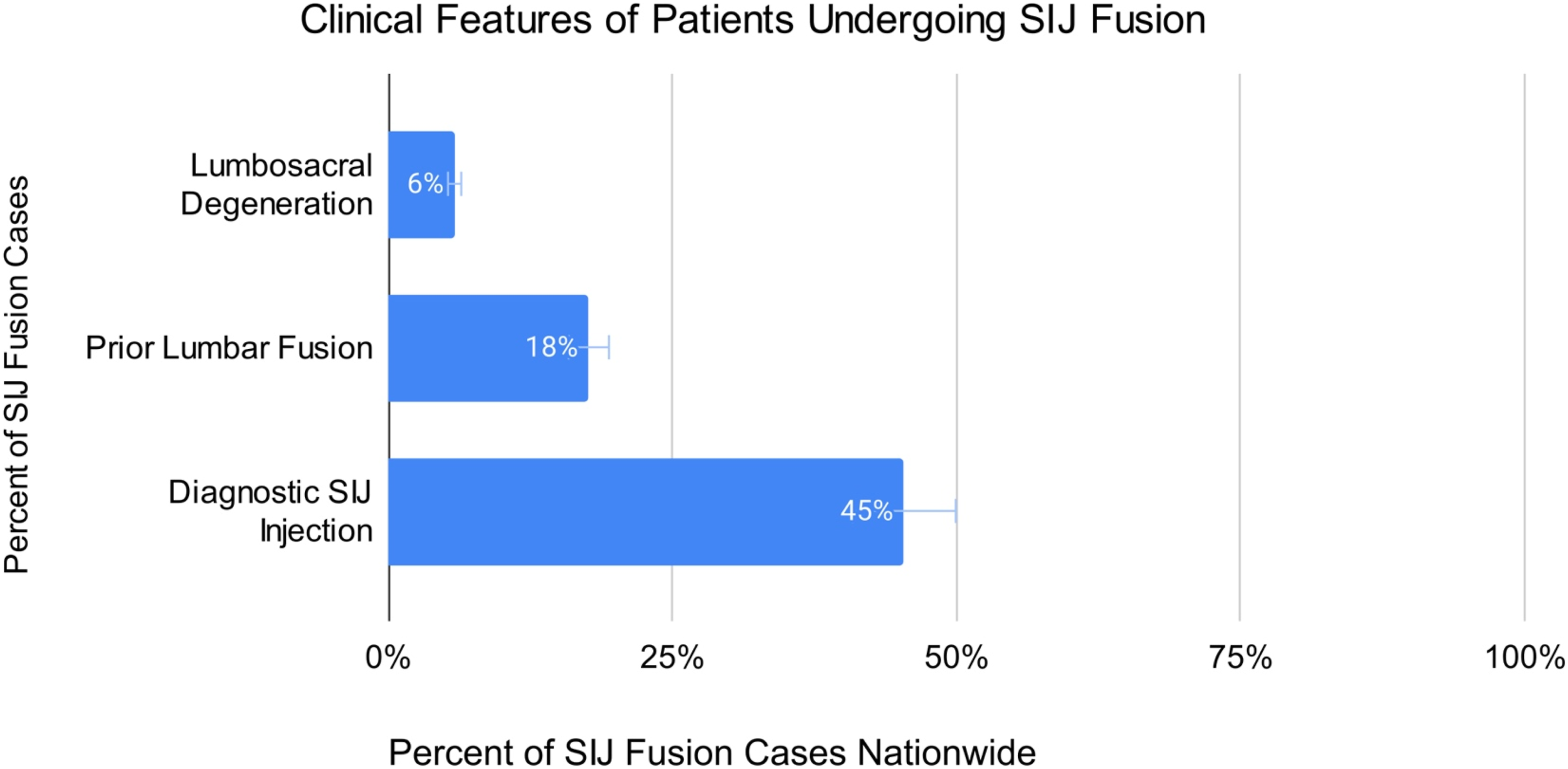
Discussion
The findings from this study herein describe nationwide trends in sacroiliac joint (SIJ) fusion utilization from 2010 to 2021, highlighting an overall, increasing trajectory in the volume of procedures performed nationally. Despite the expanded time frame in which open SIJ fusions were reviewed, MIS procedures were more commonly utilized both on a national scale, and across all geographical regions. This growing preference for MIS procedures is a product of advancements in surgical techniques and technologies, which have made MIS approaches an increasingly accessible, effective, and safer alternative to conventional open approaches. In comparison to continued conservative treatments, further evidence suggests greater improvements in economic, clinical and patient-reported outcome measures (PROMs). 15 This sentiment is moreover reflected by the transient decrease in utilization of SIJ fusion by end of 2014, with recovery of marked growth in 2015 — immediately upon introduction of CPT coding for MIS procedures. 16
Trajectories in the ensuing years support this notion, with consistently positive APCs to indicate growth in procedure utilization until the end of 2020. Compared to other geographical regions, the South interestingly reported the highest utilization of SIJ fusions; this likely a consequence of being the most highly populated region within the United States (38.7%) https://www.census.gov/popclock/data_tables.php?component=growth. alongside a higher prevalence of modifiable risk factors, such as obesity and smoking, 17 which are strongly associated with chronic low back pain. 18 Significant declines in procedure utilization were similarly seen. however, across all regions through 2021, and is likely attributable to nationwide restrictions on elective procedures enforced at the onset of the COVID-19 public health emergency, wherein all elective case volumes plunged nationally. 19 On account of 2021 being an established outlier for case volume, peak utilization seen by end of 2020 alludes to an increasing trajectory and moreover supports the prediction posited by our negative binomial regression model.
Furthermore, the study found regional variations in diagnostic indications and preoperative clinical characteristics in patients indicated for SIJ fusion. Sacroilitis secondary to seronegative spondyloarthropathies comprised the majority of cases nationally (51%), but exhibited significant regional variance, with the South (60%) having the highest proportion of procedures for SpA-related sacroiliitis, and the West having the lowest (45%). Indications for SIJ instability (20%) and degenerative SIJ (13%) pathologies represented a substantially lower proportion of cases nationally, but still demonstrated statistical significance with regional comparisons. The high proportion of cases which were indicated for SpA-related sacroilitis was likely attributable to various spondyloarthopathy subtypes, including non-radiographic axial spondyloarthritis (nr-axSpA), which exhibits clinical features similar to that of ankylosing spondylitis (AS), however, without conventional radiographic markers. 20 Therefore, nr-axSpA is sometimes viewed as a preclusive manifestation of AS, given that symptoms of SIJ dysfunction can persist for years before radiographic findings maniest, at which point it becomes recognized as AS.20,21 Progression to AS, however, has only been reported in 10-40% across studies, 22 leaving the majority of these cases to subsist indefinitely. As such, patients with nr-axSpA are likely to meet diagnostic criteria for SIJ-based pain while exhibiting symptoms for prolonged periods without alternatively identified pain sources, and may therefore comprise a large percentage of cases performed within the SpA-related diagnostic cohort within our study. Regional variations seen with all diagnostic indication cohorts are likely owed to discordant clinical guidelines and practices across the US due to a lack of uniform diagnostic criteria.23,24
Difficulties inherent in diagnosing SIJ pathologies further stem from overlapping presentations with other etiologies for low back pain. Lumbar pathologies and history of lumbar fusion have been described as possible differential pain generators in suspected SIJ pathology. 25 Incidence of new onset SI pain following lumbar fusion, however, has been widely documented, and further postulated as a driver of subsequent SIJ degeneration from increased intraarticular stress. 26 Our study found an overall prevalence of 18% for history of lumbar fusion amongst patients who underwent SIJ fusion, consistent with reports ranging from 13-32% across the literature.27,28 Findings within our study are on the lower range, however, given that our study population was based solely on operatively treated cases.
As evidenced, accurately identifying the pain source in suspected sacroiliac joint pathology is critical for determining the most appropriate treatment strategy. Accurate diagnosis of SIJ pathologies is confounded by the lack of pathognomonic features and non-specific symptomatology — namely low back pain, as a cardinal symptom of SI pathology.29,30 Current imaging modalities, in isolation, provide limited insight without further context, often demonstrating non-specific inflammatory changes, or in some cases, without appreciable radiographic changes. 31 At present, diagnostic SIJ injections are considered the most reliable diagnostic tool in confirming SIJ-based pain.5,32 Nonetheless, our findings revealed that only 45% of patients undergoing SIJ fusion received diagnostic preoperative injections overall, ranging from 51.6% in the Northwest to 41.5% in the West. With such large regional variation in both diagnostic and management strategies for SIJ-based pathologies, these findings emphasize the need to establish standardized guidelines using consistent, evidence-based approaches to parallel the increasing use of SIJ fusions. With continued discrepancies in management strategies and diagnostic challenges associated with SIJ pathologies, uniform guidelines must be developed to drive standardized adherence. Notwithstanding, emerging evidence to support the efficacy of SIJ fusions for intractable cases of low back pain from SIJ pathology yields substantial promise for widespread adoption of this approach, which provides a potential solution to a long-standing global burden.
Limitations
Several limitations should be considered for this study. It should first be noted that our study excluded operative indications for urgent/emergent indications for SIJ fusion such as malignancy, neoplasm, and infection and therefore reflects procedure utilization to treat chronic SI pathologies. Given that the PearlDiver national database uses ICD and CPT coding, the granularity of our analysis was limited by the binary nature of the available data. For example. Although our study includes SIJ instability as a diagnostic indication, we were unable to assess whether instability was accurately detected based on provocative physical exam maneuvers commonly utilized to evaluate instability. 33 The binary nature of our dataset furthermore precludes assessment of patient-reported outcomes, which are important metrics in determining whether SIJ fusion offers a pragmatic treatment alternative to conservative management. For that reason, we sought to center the current study’s objectives around national trends rather than at the individual patient level to appropriately utilize the capabilities of a large-scale national database. Moreover, the use of medical billing codes to characterize our diagnosis and procedure categories relies on accurate medical coding. While the classification systems were designed to be standardized, individual practices may vary across institutions and are liable to human error. Reliance on CPT codes furthermore limited inclusion of MIS procedures which were likely performed prior to 2015 given that corresponding codes were only introduced that year. Finally, the difficulty inherent in accurately identifying the SIJ as a source for low back pain may also skew our results relative to the true incidence of SIJ-based pathologies. Despite these limitations, this is the largest study to characterize national trends in SIJ fusion and the variability of diagnostic indications and relevant clinical features in patients undergoing SIJ fusion across the US.
Conclusion
Our study highlights utilization trends and variability in operative indications and demographic features within the patient population undergoing SIJ fusion across geographical regions of the US. As SIJ fusion is increasingly utilized, it is crucial to establish evidence-based guidelines to improve diagnostic modalities for SIJ pathologies and clarify indications for SIJ fusion. Our study provides a foundation for future research therein, and calls for collaborative efforts among clinicians, researchers, and policymakers to develop standardized guidelines that optimize patient outcomes while minimizing the economic and clinical burden associated with the high prevalence of chronic, refractory low back pain across the US.
Supplemental Material
Supplemental Material - Nationwide Analysis of Sacroiliac Joint Fusion Trends: Regional Variations in Utilization and Population Characteristics
Supplemental Material for Nationwide Analysis of Sacroiliac Joint Fusion Trends: Regional Variations in Utilization and Population Characteristics by Andy Ton, Kevin Mertz, Marc Abdou, Nicole Hang, Emily S. Mills, Raymond J. Hah, Ram K. Alluri and Jeffrey C. Wang in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the North American Spine Society to attend meetings. Ram K. Alluri, M.D. discloses has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccentrial Robotics for lectures and presentations. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes.
Informed Consent
Informed consent was waived due to the retrospective nature of the study and institutional review board (IRB) approval was not required as the database is de-identified.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.