
Abstract
Study Design
Prospective cohort study.
Objective
The sacroiliac joint (SIJ) is an important cause of lower back pain. The degree to which minimally invasive surgical fusion of the SIJ improves health state utility has not been previously documented.
Methods
Health state utility values were calculated using the EuroQOL-5D (EQ-5D) and Short Form-36 (SF-36) at baseline and 6 and 12 months after SIJ fusion surgery in subjects participating in a prospective, multicenter clinical trial (n = 172). Values were compared with individuals who participated in a nationally representative cross-sectional survey (National Health Measurement Study [NHMS], n = 3,844). Health utility values in the SIJ cohort were compared with those of the NMHS participants using both weighted linear regression and calculation of “health quantile” (i.e., percentile of health normalized to the NHMS cohort adjusted for age and gender).
Results
Baseline health state utility was significantly depressed in SIJ patients compared with normal subjects (SF-6D 0.509 versus 0.789, SF-36 physical component summary 31.7 versus 49.2, SF-36 mental component summary 8.5 versus 53.8, EQ-5D 0.433 versus 0.868; all p < 0.0001 after adjustment for age and gender). In the SIJ cohort, all the measures improved by 6 months postoperatively, and improvements were sustained at 12 months. Baseline health quantile was low (fifth percentile) in the SIJ cohort and improved significantly at follow-up.
Conclusions
Quality of life is markedly impaired in patients with SIJ pain compared with age- and gender-matched cohorts. SIJ fusion in this cohort resulted in a substantial improvement in health state utility, bringing the population back toward the expected levels of overall health. The quantile approach helps to explain the degree to which health is improved compared with age- and gender-matched cohorts.
Keywords
Introduction
The burden of chronic lower back pain in modern society is high, with an annual loss of ∼83 million healthy life-years. 1 Rating higher than cancer and chronic obstructive pulmonary disease, lower back pain is the sixth most common cause of loss of global disability-adjusted life-years. 2
Many patients who present with chronic lower back pain have sacroiliac joint (SIJ) disorders as a source of pain. In fact, the SIJ was determined to be the source of the lower back pain in 14 to 22% of patients presenting for back pain evaluation. 3 , 4 The SIJ is even more commonly (up to 40%) suspected as a source of lower back pain in patients with prior lumbar fusion. 5 , 6 Currently available treatment options include physical therapy,7 SIJ steroid injections, 8 , 9 radiofrequency ablation of the SIJ, 10 , 11 and open or minimally invasive SIJ fusion. 12 , 13 , 14 , 15 , 16 , 17 , 18
Clinical trials of orthopedic surgical interventions are challenging, especially when comparing surgical to nonsurgical treatments. Although orthopedic surgery trials typically focus on improvements in pain and disability, few have reported improvements in overall quality of life. Moreover, few have put observed improvements into perspective by comparison to other health conditions or age-matched cohorts. It is reasonable to expect that surgery could restore a portion of lost health in an older person; however, it is not reasonable to expect restoration to perfect health. Adjustment for the chronic health conditions of the target population could help to put observed improvements after any intervention into perspective. This report (1) compares depression of health state utility in a cohort of patients with SIJ disorders participating in a prospective clinical trial to age- and gender-matched cohorts, (2) documents the improvement in health state utility after surgery, and (3) proposes methods to put the restoration of health after surgery into perspective by direct comparison to a normal cohort matched for age and gender.
Methods
Cohorts
Methods used in this study were similar to those previously reported. 19 Two cohorts were used. The SIJ cohort consisted of 172 patients enrolled in an ongoing, prospective, multicenter clinical trial of minimally invasive SIJ fusion (NCT01640353). The study was sponsored by the device manufacturer (SI-BONE, Inc., San Jose, California, United States). All clinical trial sites obtained Institutional Review Board approval prior to enrollment in this study. To qualify for the study, adult patients between ages 21 and 70 had to have carefully diagnosed chronic SIJ pain due to degenerative sacroiliitis or SIJ disruptions as outlined in Table 1. All eligible subjects underwent minimally invasive SIJ fusion as described below. All subjects completed the Short Form-36 (SF-36) v2 and EuroQOL-5D (EQ-5D)'s health-related quality-of-life (HRQoL) questionnaires at baseline and at 6 and 12 months after surgery.20,21 Six-month follow-up was available in 163 SIJ subjects (95%). As the SIJ study is ongoing, 12-month follow-up is currently available in 63 (37%). The normal cohort consisted of respondents from the United States National Health Measurement Study (NHMS). Designed to compare commonly used preference-based HRQoL instruments (SF-36, SF-6D, 22 EQ-5D,21 and other surveys) in an oversampled cross-sectional sample of 3,844 U.S. adults, the publicly available data has been analyzed for population norms. 23
Key eligibility criteria for SIJ pain and participation in clinical trial of SIJ fusion a
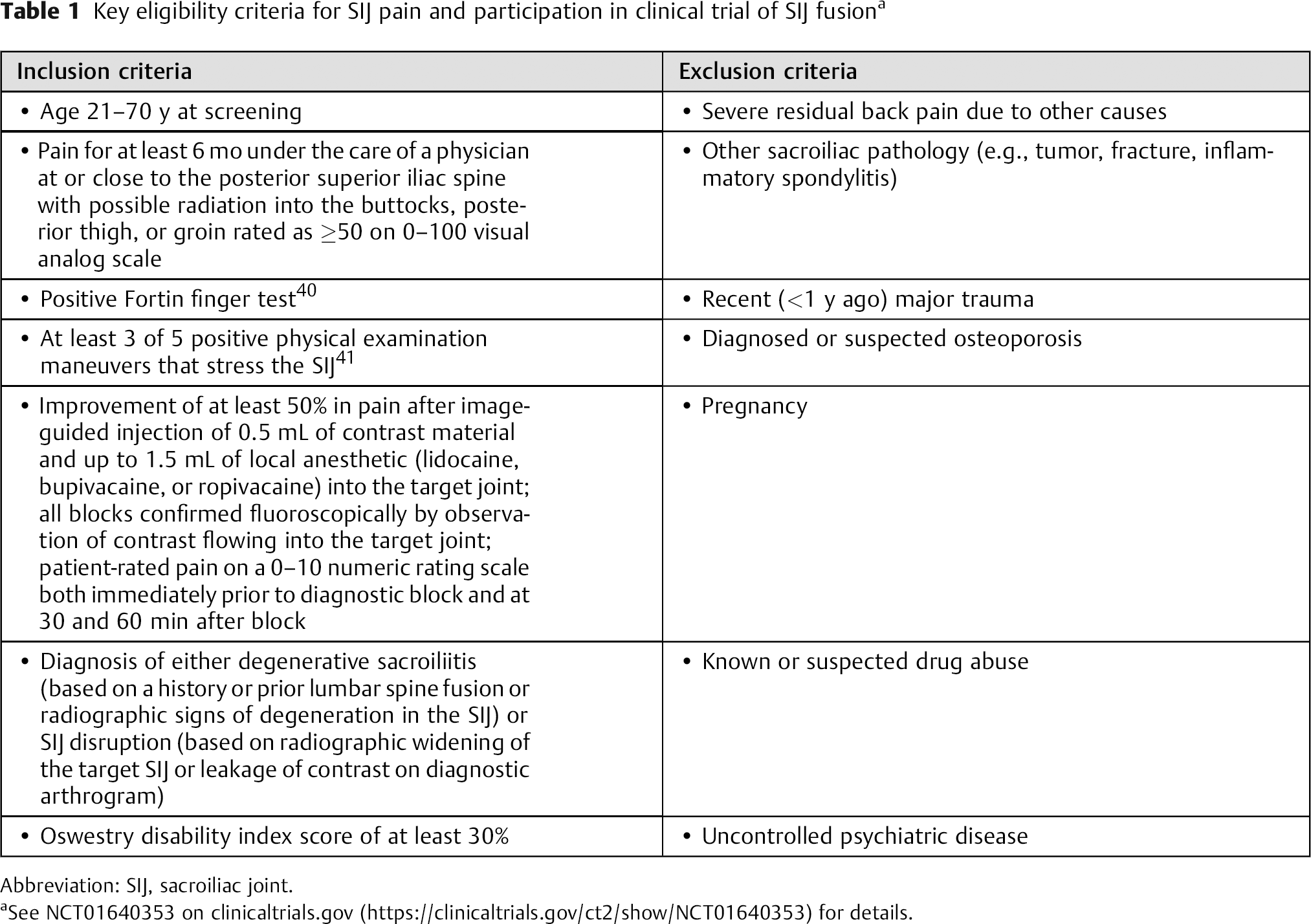
Abbreviation: SIJ, sacroiliac joint.
See NCT01640353 on clinicaltrials.gov (https://clinicaltrials.gov/ct2/show/NCT01640353) for details.
SIJ Fusion
The SIJ was fused during a minimally invasive surgical procedure under general anesthesia with fluoroscopic guidance. Briefly, the patient is placed in the prone position on a radiolucent table, a 3- to 5-cm lateral incision is made into the buttock region, and the gluteal fascia is bluntly dissected to reach the outer table of the ilium. A guide pin is passed through the ilium across the SIJ to the center of the sacrum lateral to the neural foramen. A drill is used, followed by a triangular broach, to create a pathway into the sacrum into which a titanium rod is impacted. Typically, three implants are placed at various locations across the SIJ. The incision is irrigated and the tissue layers sequentially closed. The implants and delivery system are manufactured by SI-BONE, Inc. Subjects requiring surgery on both SIJs could undergo either bilateral same-day surgery or staged surgery. Postoperatively, subjects underwent rehabilitative therapy for up to 6 weeks tailored to individual needs.
Transformations
Key measures in this study were the SF-36 physical component summary (PCS) and mental component summary (MCS), SF-6D, and EQ-5D. The EQ-5D in the SIJ cohort was transformed into health state utility using EuroQOL tables, and the SF-6D was calculated using published formulae. 24 , 25
Statistical Evaluation
All statistical evaluation was performed using R. 26 The NHMS and SIJ cohorts were combined with an additional grouping variable representing cohort (SIJ cohort or NHMS). Weighted means and other statistical measures were calculated across NHMS age and gender groups and gender using weighted approaches. Weighted regression, which controlled for age and gender and took into account oversampling at various strata in NHMA, was performed with the R “survey” package. 27 Hypotheses with p values less than 0.05 were deemed statistically significant.
An alternative approach to estimating health impact was investigated by calculating each SIJ patient's percentile for a selected index using the NHMS cohort as a reference standard. That is, empirical cumulative distribution functions for each assessment of interest in NHMS (SF-6D, SF-36 PCS and MCS, and EQ-5D time trade-off index) were calculated by age group (by 10-year groupings) and gender, taking into account survey sampling weights. Weighted regression showed statistically significant differences in the reference population by gender and age groupings. Locally weighted smoothing for each empirical cumulative distribution function was determined, which allows estimation of the exact quantile of health given any input value for each age/gender subcohort. Then, for each SIJ subject, the corresponding quantile normalized to the NHMS reference population was determined at baseline and at 6 and 12 months after surgery. Any given percentile for an SIJ cohort participant indicates HRQoL with SIJ pain as compared with an age- and gender-matched reference standard. A value of 5% means that the quality of life for the SIJ patient is in the fifth percentile compared with age- and gender-matched peers.
Results
In all, 172 patients were enrolled in the SIJ surgery study and 3,844 people participated in the NHMS normal cohort. Compared with the NHMS normal cohort, the clinical trial subjects with diagnosed SIJ pain were somewhat younger and more likely to be women (Table 2). For each measure of interest (SF-36 PCS and MCS, SF-6D, and EQ-5D TTO [time trade-off index]), values in the SIJ cohort at baseline were substantially depressed compared with the NHMS cohort. After adjustment for differences in age and gender and accounting for oversampling, the differences were −18 and −15 points for the SF-36 PCS and MCS, respectively, and −0.28 and −0.43 points for the SF-6D and EQ-5D (Table 3, all p < 0.0001). At 6 and 12 months of follow-up, scores improved from baseline by ∼8 and 9 points for the SF-36 PCS and MCS, respectively, and by ∼0.12 and 0.25 points for the SF-6D and EQ-5D TTO, respectively (all p < 0.0001).
Age and gender distributions by cohort

Abbreviations: SE, standard error; SIJ, sacroiliac joint; NHMS, National Health Measurement Study.
Mean (95% CI) HRQoL, decrement in quality of life, and improvement values by group
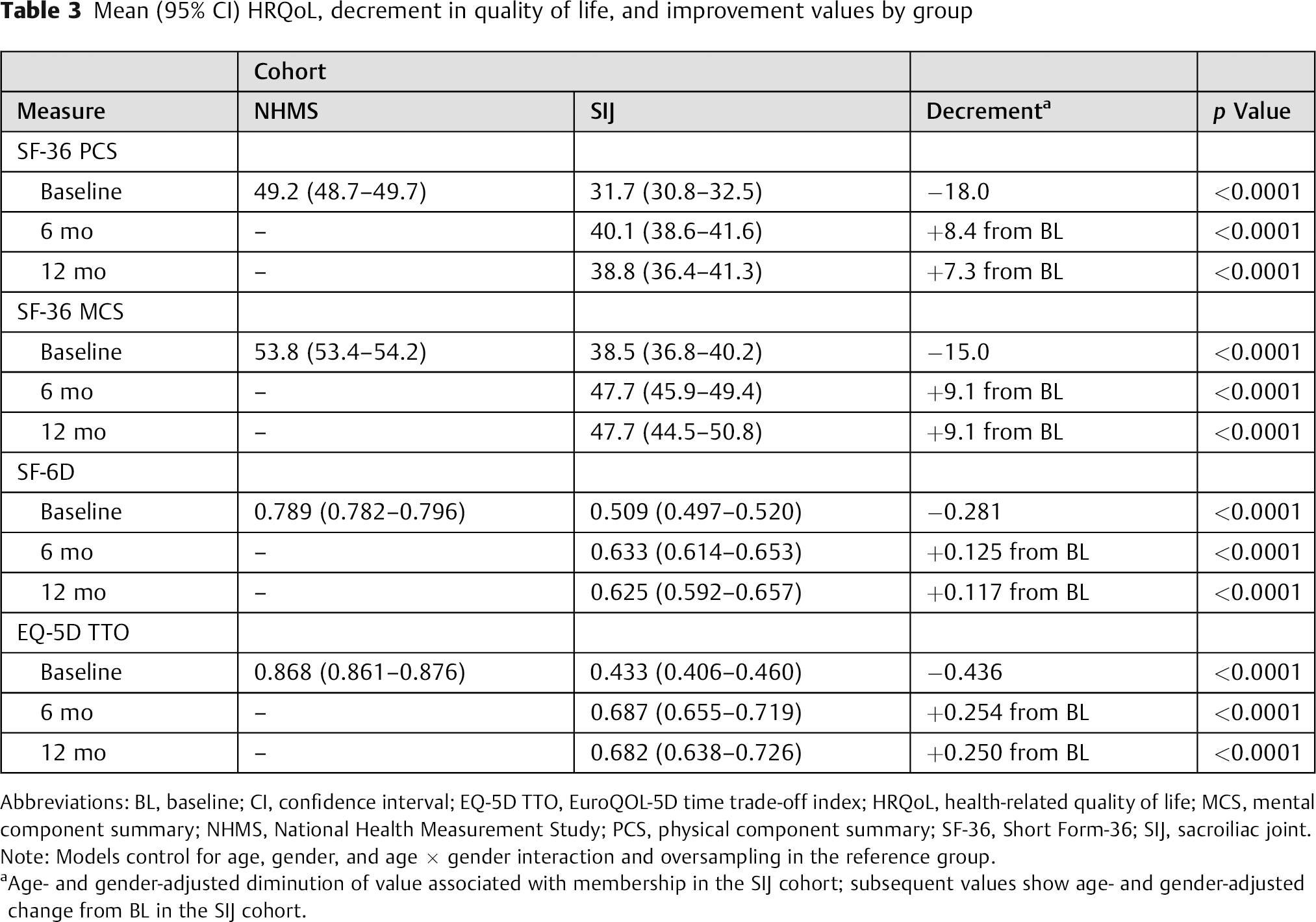
Abbreviations: BL, baseline; CI, confidence interval; EQ-5D TTO, EuroQOL-5D time trade-off index; HRQoL, health-related quality of life; MCS, mental component summary; NHMS, National Health Measurement Study; PCS, physical component summary; SF-36, Short Form-36; SIJ, sacroiliac joint.
Note: Models control for age, gender, and age × gender interaction and oversampling in the reference group.
Age- and gender-adjusted diminution of value associated with membership in the SIJ cohort; subsequent values show age- and gender-adjusted change from BL in the SIJ cohort.
To put both baseline decrements and subsequent follow-up improvements into perspective, Figs. 1,2 to 3 show the distribution of raw utility values in the SIJ cohort compared with the NHMS normal cohort as well as age- and gender-adjusted quantile of health when compared with the NHMS reference standard. Table 4 shows summaries of the distribution of health quantile. At baseline, the mean quantile of health utility in the SIJ cohort was very low, and the distribution of utilities was concentrated in the lowest “decade.” These results suggest a marked depression of health in the SIJ cohort compared with unselected age- and gender-matched peers. At 6 and 12 months of follow-up, substantial improvement in health state utility was seen for both raw values as well as the distribution of health quantiles. For the SF-36 PCS, SF-6D, and EQ-5D, health quantiles improved from approximately the 5th percentile to the 20th to 25th percentiles. If the SIJ population were restored to health equivalent to that of the reference standard, then the distribution of quantiles would be flat across the quantile spectrum. Flattening of the quantile distribution is evident in each utility measurement. Quantile of health as assessed by the EQ-5D and SF-6D were moderately correlated (Pearson R = 0.78).
Quantile of health in SIJ cohort by study visit and gender
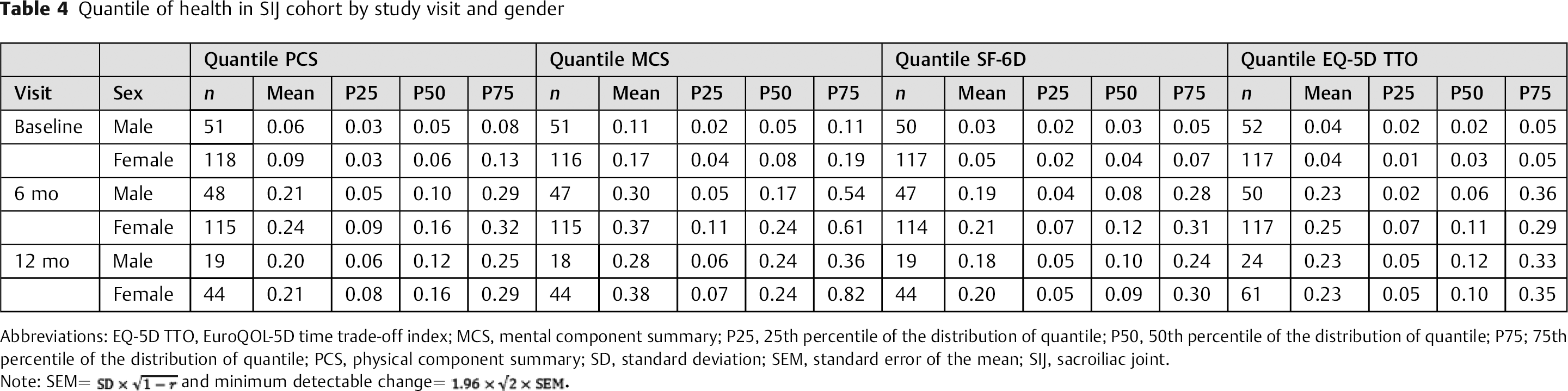
Abbreviations: EQ-5D TTO, EuroQOL-5D time trade-off index; MCS, mental component summary; P25, 25th percentile of the distribution of quantile; P50, 50th percentile of the distribution of quantile; P75; 75th percentile of the distribution of quantile; PCS, physical component summary; SD, standard deviation; SEM, standard error of the mean; SIJ, sacroiliac joint.
Note:
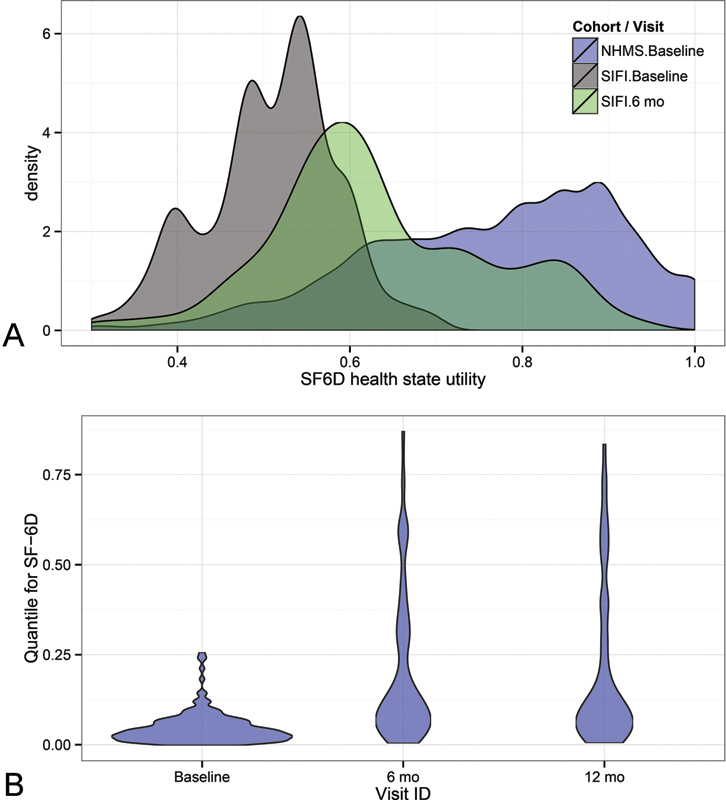
(A) Distribution of SF-6D in NHMS (reference cohort, blue) and SIJ subjects at baseline (gray) and 6 months of follow-up (green). Twelve-month results are nearly superimposable with 6-month results and are not plotted. (B) “Violin plot” distribution of SF-6D by study visit in SIJ cohort only expressed as quantiles using NHMS as a reference standard and adjusting for age and gender. The width of the violin is proportion to the point density. Abbreviations: SIFI, sacroiliac fusion investigation; SIJ, sacroiliac joint; NHMS, National Health Measurement Study.
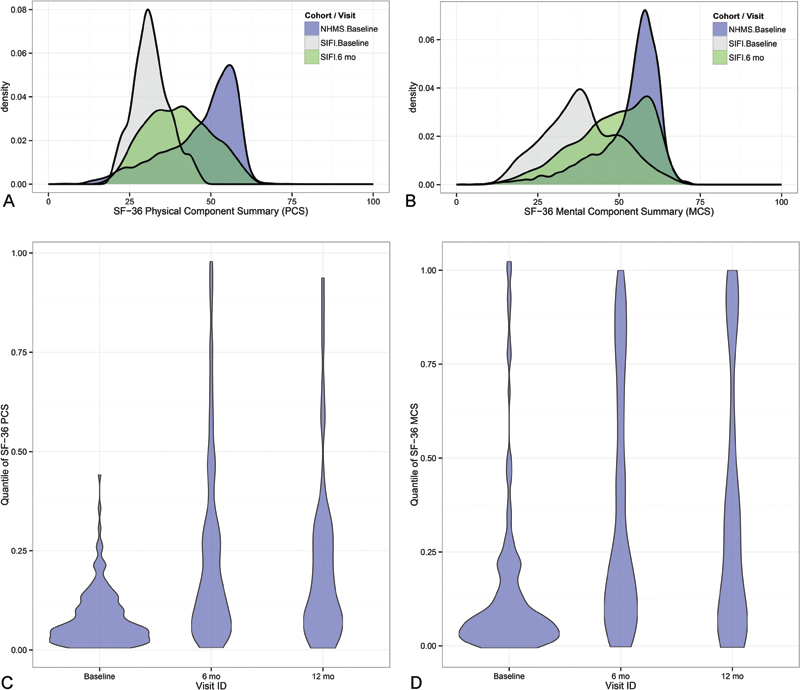
Distribution of SF-36 PCS (A) and MCS (B) in reference group (blue) and SIJ study subjects by study visit (baseline = gray, 6-month follow-up = green). (In the SIJ cohort, the 12-month results are nearly identical to 6-month results and are therefore not shown.) Quantiles of PCS (C) and MCS (D) in SIJ cohort by study visit when normalized to NHMS reference group by age and gender. Abbreviations: PCS, physical component summary; MCS, mental component summary; SF-36, Short Form-36; SIFI, sacroiliac fusion investigation; NHMS, National Health Measurement Study.
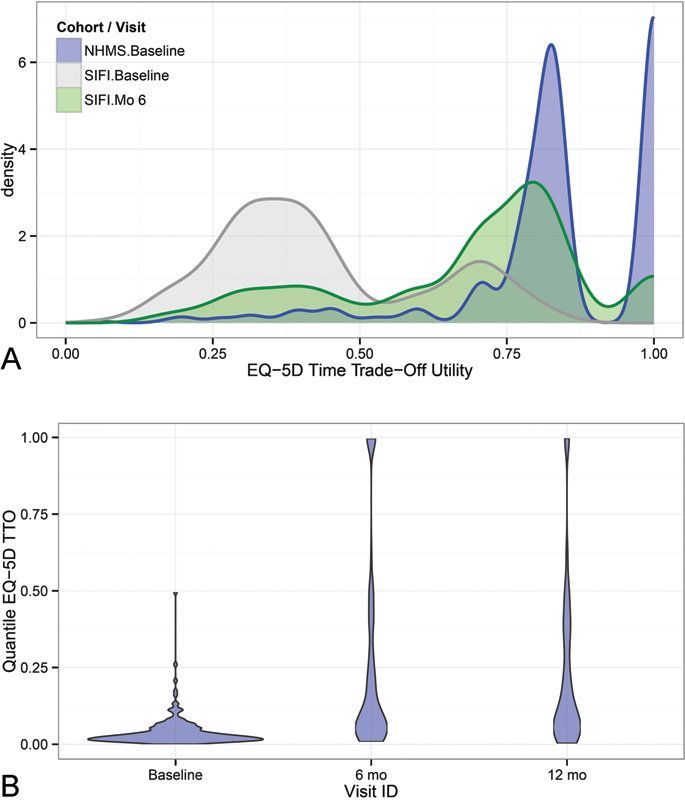
(A) Distribution of EQ-5D time trade-off utility (top) in reference group (blue) and SIJ study subjects by study visit (baseline = gray, month 6 = green). Twelve-month SIJ cohort values, which were nearly identical to 6-month results, are hidden. (B) Quantiles of EQ-5D TTO in SIJ cohort by study visit when normalized to NHMS reference group by age and gender. The bimodal distribution for EQ-5D TTO in normal subjects is typical. Abbreviations: EQ-5D TTO, EuroQOL-5D time trade-off index; SIFI, sacroiliac fusion investigation; NHMS, National Health Measurement Study.
Discussion
This study extends the findings of a previous report of the same cohort that patients with SIJ disorders severe enough to consider surgery have very poor health state utility values. 19 The prior report compared the disutility associated with SIJ pain to other medical conditions as well as to orthopedic conditions commonly treated surgically. The disutility associated with SIJ pain was equivalent to or worse than that from hip osteoarthritis, knee osteoarthritis, degenerative spondylolisthesis, and spinal stenosis.
We report herein that patients participating in a prospective trial, all of whom underwent minimally invasive SIJ fusion, saw substantial improvements in health state utility, with increases of 0.12 for the SF-6D and 0.25 points for the EQ-5D. The SF-6D changes are similar to 1-year changes reported in a registry study of lumbar diskectomy and single-level fusion for spondylolisthesis. 28
More commonly reported are changes in the SF-36 PCS after a surgical intervention. In our cohort, these measures improved by 7 to 9 points. These changes are similar to those seen in the INTER FIX investigational device exemption clinical trial, 29 which had a fusion control group (31 at baseline to 40 at 5 years) in a prospective randomized control study of total disk replacement versus single-level circumferential arthrodesis for single-level degenerative disease, as well as other randomized trials (e.g., a Canadian study of decompression with or without fusion for degenerative lumbar spondylolisthesis and a European randomized trial of posterior lumbar interbody fusion using autograft with or without platelet-rich plasma). 30 , 31 , 32 The changes seen in the SIJ cohort are somewhat larger than those reported in a prospective study specifically used to look at minimally clinically important differences in measures such as PCS. 33 The changes are also very similar to those seen in patients in multiple clinical trials who underwent total knee arthroplasty and just slightly smaller than those undergoing hip arthroplasty. 34 The improvement of PCS in the SIJ cohort was above the minimum detectable change as reviewed by Copay and exceeds one-half the standard deviation of the mean, 33 a value shown to generally represent the minimally important difference. 35 The observed improvement in the EQ-5D TTO health index in our cohort (0.25 units) was similar to that observed in patients undergoing a variety of orthopedic surgical procedures. 36 Though not the focus of the current report, improvements in HRQoL measures were paralleled by improvements in SIJ-specific pain and disability. Taken together, these results confirm those from several prior cohort and comparative studies including a 5-year follow-up study demonstrating the value of minimally invasive SIJ fusion. 13 , 14 , 15 , 16 , 17 , 18 , 37 , 38 , 39
Although improvements in pain are easy to interpret, improvements in quality of life and utility estimates are harder to put into perspective. Most HRQoL studies use the 0 to 1 scale, where 0 represents death and 1 represents perfect health. When considering the risk associated with treatments, there is an implicit presumption that treatment should restore as many patients as possible back to 1 (i.e., perfect health). With increasing longevity, however, patients are affected by an increasing number of chronic health conditions and achieving perfect health is therefore not a realistic goal.
In the SIJ cohort studied, the presurgical health level averaged in the third to fifth percentiles using the SF-6D and EQ-5D TTO index, and the sixth to ninth percentile for the SF-36 PCS. These values indicate severe baseline disability. At 6 and 12 months, the mean quantile had increased to the 20th to 25th percentile for all measures, indicating a substantial restoration of overall health with a single surgical procedure. A substantial number of patients were restored to health levels above the 50th percentile. Thus, although postintervention health states were still impaired in many patients, significant improvements should be acknowledged. The concept of improvement toward the age- and sex-matched health state gives a new perspective to the value of the intervention.
Extending these findings further, we believe that the value of any health intervention should be interpreted in light of both the preintervention health utility value as well as reasonable expectations for health given the population's age and gender distribution. Some interventions are aimed at populations whose overall health state utility is not severely depressed. These interventions may have limited ability to improve overall health. In contrast, as evidenced by the baseline quantile values in the SIJ cohort, SIJ pain was associated with severely impaired overall health. The improvement in health seen after SIJ fusion potentially translates into a larger overall public health impact given the marked depression of the baseline health. For example, an improvement from the 3rd percentile of health to the 20th to 25th percentile represents an increase of 1 to 1.2 standard deviations. In contrast, a similar improvement of 17 to 22 quantile points when starting at the median level of health constitutes a change of less than half a standard deviation.
Using this approach, the threshold for what constitutes a meaningful improvement might be different in the groups with varying degrees of diminution of presurgery health. Further exploration of the value of the approach described herein is warranted. Of special interest is whether the cost-effectiveness calculations could or should be affected by comparison to age- and gender-matched normal cohorts.
The improvements in health state utility were somewhat different across the two utility measures: +0.12 and +0.25 points on the SF-6D and EQ-5D TTO indices, respectively. The EQ-5D utility measure showed more depression at baseline than the SF-6D (0.43 versus 0.51 points) as well as greater improvement (+0.25 versus +0.12 points). The EQ-5D TTO also demonstrated a ceiling affect. Possibly because it has fewer response categories (three per question) and fewer questions (five) than the SF-36, the EQ-5D may have less resolution than the SF-6D. Interestingly, the two values were moderately correlated and the baseline and postsurgery quantile measurements associated with these two measures agreed closely, suggesting that both instruments measure a valid aspect of overall health state utility.
This study has several strengths. First, we compared a relatively large number of patients from a carefully selected and homogeneous population (i.e., participants in a prospective multicenter clinical trial) to an unselected age- and gender-matched cohort from a nationally representative health survey. The same questionnaires used to assess HRQoL at baseline were repeated at predetermined follow-up intervals, allowing an accurate assessment of response to the intervention. Finally, the large number of subjects in the reference population allowed precise estimation of health quantiles by gender and age categories. A potential limitation is that because the reference standard focused on individuals of all ages who were able to participate in surveys, it may overestimate health in normal people by excluding persons with poor health who could not participate.
Conclusions
SIJ pain due to degenerative sacroiliitis and SIJ disruptions was associated with marked decreases in quality of life and health state utility, corresponding to the third to fifth percentiles of health compared with free-living age- and gender-matched individuals. SIJ fusion in this cohort resulted in a substantial improvement in health state utility, bringing the population back toward expected levels of overall health.
Disclosures
Daniel J. Cher, employee: SI-BONE
David W. Polly, none
Financial Support
The study from which data analyzed in this report is derived was sponsored by SI-BONE.