
Abstract
Study Design
Retrospective cohort study.
Objective
Decompression for the treatment of lumbar spinal stenosis (LSS) has shown excellent clinical outcomes. In patients with symptomatic single level stenosis and asymptomatic adjacent level disease, it is unknown whether decompressing only the symptomatic level is sufficient. The objective of this study is to compare outcomes between single level and dual level minimally invasive (MIS) decompression in patients with adjacent level stenosis.
Methods
The current study is a retrospective review of patients undergoing primary single or dual level MIS decompression for LSS. Radiographic stenosis severity was graded using the Schizas grading. Patients undergoing single level decompression (SLD) with moderate stenosis at the adjacent level were compared with patients undergoing dual level decompression (DLD) for multi-level LSS. Clinical outcomes, complications, and reoperations were compared. Subgroup analysis was performed on patients with the same Schizas grade at the adjacent level in the SLD group and the second surgical level in the DLD group.
Results
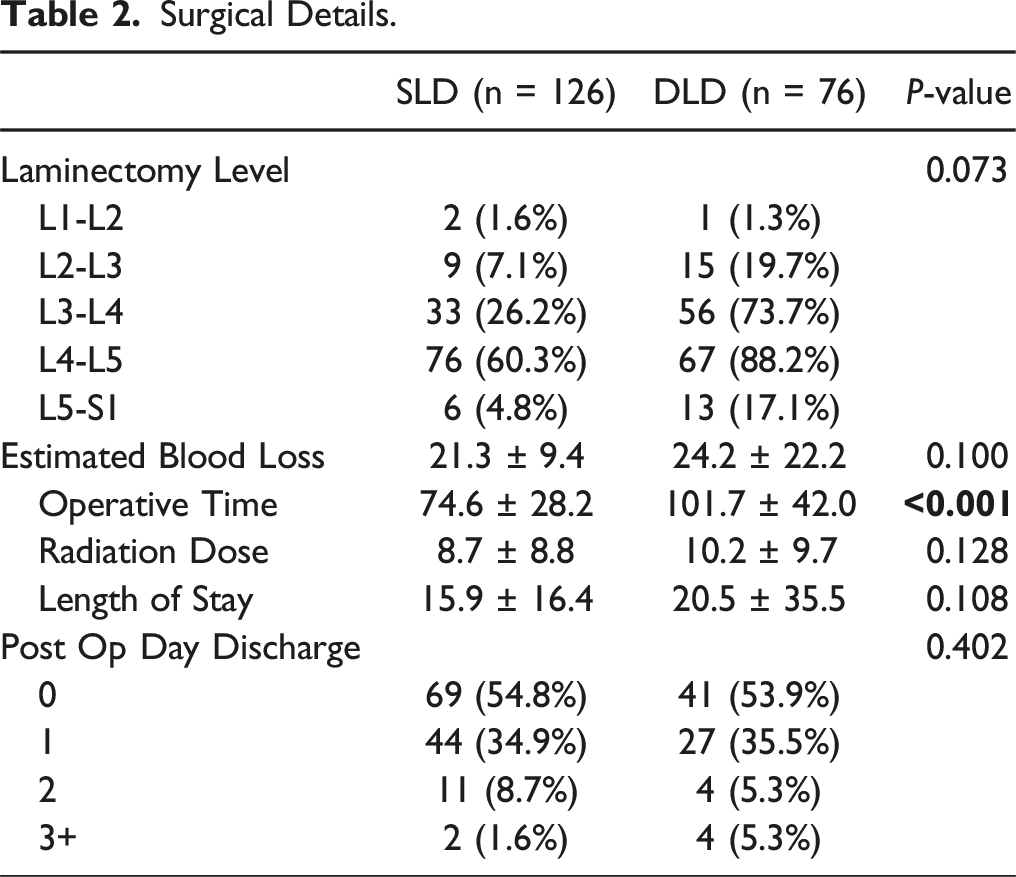
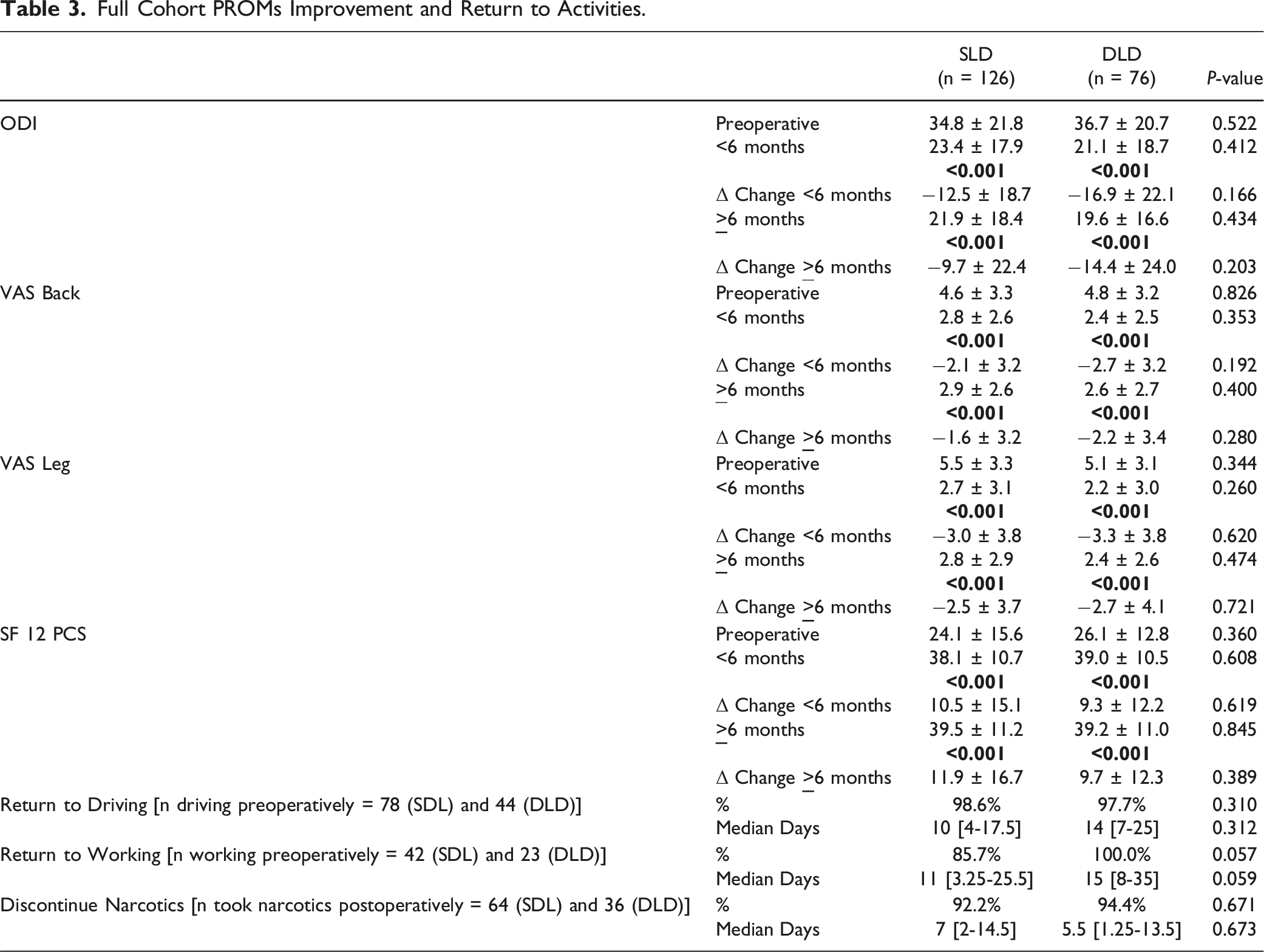
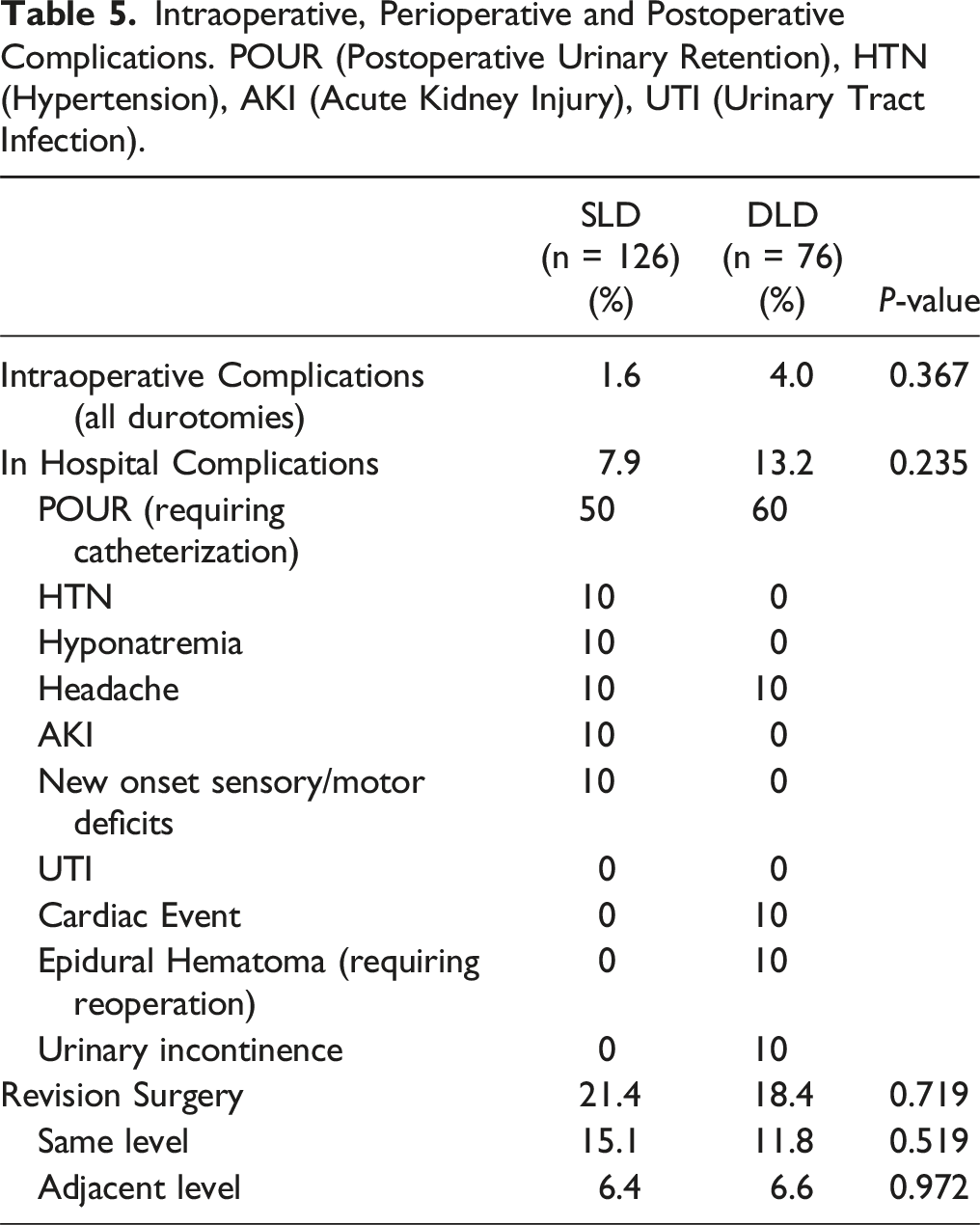
148 patients were included (126 SLD, 76 DLD). There were no significant differences in patient reported outcomes between the two groups at any timepoint up to 2 years postoperatively, including in the matched stenosis severity subgroups. Operative time was longer in the DLD cohort (P < 0.001). There were no significant differences in complications or reoperation rates.
Conclusion
In patients with single level symptomatic LSS and adjacent level stenosis, decompression of only the symptomatic level provided equivalent clinical outcomes compared to dual level decompression. The additional operative time and potential incremental risk of dual level surgery may not be justified.
Introduction
Lumbar spinal stenosis (LSS) represents a very common pathology. Patient presentations may range from asymptomatic incidental findings to severe debilitating pain with radiculopathy and neurogenic claudication. 1 Surgical treatment is typically reserved for symptomatic patients who have often failed to respond to conservative treatment in the form of physical therapy or steroid injections.2-4 Minimally invasive (MIS) decompression is a frequently employed surgical approach for the treatment of stenosis in the lumbar spine. Surgical treatment opens the space available for neural elements and has largely demonstrated good outcomes in appropriately selected patients. 5
Previous studies correlating patient symptoms to preoperative MRI radiographs have largely demonstrated no reliable concordance between the two,6,7 suggesting an ambiguous relationship between the space available for the cord and disability. In deciding the best surgical approach and operative levels, isolated MRI findings may not be fully reliable, especially considering many patients demonstrate multi-level LSS on MRI. 8 In these patients with multi-level stenosis there remains a question whether or not decompressing additional levels with no specific localizing symptoms is valuable. Few previous studies have attempted to answer this question. Most recently, Tronstad et al published in a cohort of LSS patients finding no significant differences in patient-reported outcome measures (PROMs), complications, or reoperations between single or dual level decompression in patients with adjacent level stenosis. 9 Importantly however, this cohort remained heterogeneous as the proportion of patients with Schizas grade C at the adjacent level was 4 fold greater in the dual level group making it difficult to conclude equivalent clinical outcomes.
The purpose of the present study was to compare outcomes in patients who underwent single or dual-level minimally invasive (MIS) decompression with adjacent-level for the treatment of LSS. Specifically, we aimed to answer (1) Should surgeons decompress the second level in the absence of localizing symptoms? and (2) What is the added “cost” of decompressing the second level, considering factors such as increased operative time and heightened risk of complications?
Methods
Study Design and Patient Cohort
The present study was conducted after approval by the Institutional Review Board (IRB 2018-1142). After appropriate informed consent, patients who underwent primary minimally invasive lumbar decompression (unilateral laminotomy for bilateral decompression, ULBD) for stenosis of the lumbar spine between February 2017 and June 2022 with a minimum of 1 year follow-up were queried from a prospectively maintained multi-surgeon registry. All surgeries were performed by three fellowship-trained spine surgeons at a single academic institution as previously described in the literature. 10 The side of the ULBD was decided based on the laterality of the symptoms and the relevant anatomy in terms of docking of the tubular retractor.
Data Collection
Data was collected and managed using REDCap (Research Electronic Data Capture)11,12 hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384. The following data was collected and analyzed: 1. Demographics: age, gender, race, body mass index (BMI), smoking status, diabetes, depression, anxiety, age-adjusted Charlson Comorbidity Index (CCI), and American Society of Anesthesiologists (ASA) Classification 2. Preoperative X-ray Measurements: Spondylolisthesis at the operated level, spondylolisthesis instability (when applicable), total lumbar lordosis (LL), proximal lordosis (PL), distal lordosis (DL), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS). PI-LL was additionally calculated. 3. Preoperative MRI Measurements: At all lumbar levels, the Pfirrmann grade, Schizas grade, and dural sac cross-sectional area (DSCSA in mm2) were all evaluated as previously described in the literature.
5
Muscle health was assessed using the psoas cross-sectional area and Goutallier grading at L3-L4. The presence of a facet cyst or effusion at the operated level was additionally recorded. 4. Preoperative CT Measurements: Bone quality was assessed with Hounsfield units using elliptical regions of interest, calculating a mean at the mid-axial level at each lumbar levels. 5. Surgical characteristics and outcomes: number of levels operated, specific operated levels, estimated blood loss (EBL), radiation dose, operative time, and operative complications were recorded. Postoperative length of stay (LOS), perioperative complications and reoperations were also collected through the patient’s latest follow-up. 6. PROMs: Oswestry Disability Index (ODI) Visual Analog Scale, (VAS) back and leg, 12-Item Short Form Survey Physical Component Score (SF-12 PCS), and global rating change (GRC) were collected at 2 weeks, 6 weeks, 12 weeks, 6 months, 1 year, and 2 years after the surgery. Two postoperative timepoints - early (<6 months) and late (>6 months) - were defined for analyses.13-16 7. Return to activities: Patients completed a return to activities survey as part of their standard of care. Patients who were driving and working preoperatively were asked if they had begun driving and working again at every follow-up visit until they returned to that activity. Patients who took opioids postoperatively were asked the date of cessation if applicable.
Single and Dual Level Decompression Cohorts
Two groups of patients were separated for the purpose of this analysis. Single-level decompression (SLD) patients all underwent single level surgery with demonstrated Schizas grade B or greater at an adjacent level on preoperative MRI. Dual-level decompression (DLD) patients all underwent two-level surgery for multi-level LSS. The decision for SLD vs DLD was based on the surgeon’s clinical judgment. In general, SLD was performed when symptoms and exam findings correlated with a one-level stenosis regardless of the degree of adjacent level stenosis. DLD was performed if symptoms of neurogenic claudication and/or radiculopathy were thought to either (1) stem from two levels based on a combination of symptoms, physical exam, MRI findings, and response to targeted steroid injections or (2) if the adjacent level had a Schizas grade B or higher and a prophylactic decompression was clinically thought to provide a longer-term benefit. To more accurately control for LSS, subgroup analysis was conducted to specifically compare patients with similar preoperative MRIs. SLD patients with adjacent level Schizas B and C were compared with DLD patients with second level Schizas B and C respectively. The adjacent level in the DLD group was defined as the level with the same or lower Schizas grade.
PROMs Analysis
VAS-back, VAS-leg, ODI, and SF-12 PCS were assessed for improvement. Changes in PROMs from their preoperative baseline were assessed at both the early and late timepoints. Additionally, the percentage of patients achieving minimal clinically important difference (MCID) for each PROMs at the late time points were calculated. MCID achievement was defined as a decrease in ODI by 12.8, VAS-back by 1.2, VAS-leg by 1.6, and SF-12 PCS by 4.1 as previously defined by Copay et al. 17 Since preoperative baseline affects the utility of MCID in predicting patient improvement, patients with preoperative ODI <15, VAS-back/leg < 2.5, and SF-12 PCS > 92.1 were excluded from MCID achievement calculations.18-20
Statistical Analysis
Statistical analyses were conducted to compare differences between the two defined groups. Normally distributed continuous variables between groups were compared with a 2-tailed independent sample t test when appropriate. Non-normally distributed variables were compared between groups with a Mann-Whitney U test as appropriate. Continuous variables were reported as mean ± standard deviation (SD) or as median [interquartile range (IQR)] when non-normally distributed. Categorical variables were compared between groups with a χ2 test or a Fisher exact test when the number of subjects was less than 10. Categorical variables are reported as sample size (%). Statistical significance was taken at P < 0.05. Analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS) version 25 (IBM Corp., Armonk, NY).
Results
Cohort Demographics and Preoperative Radiographic Parameters.
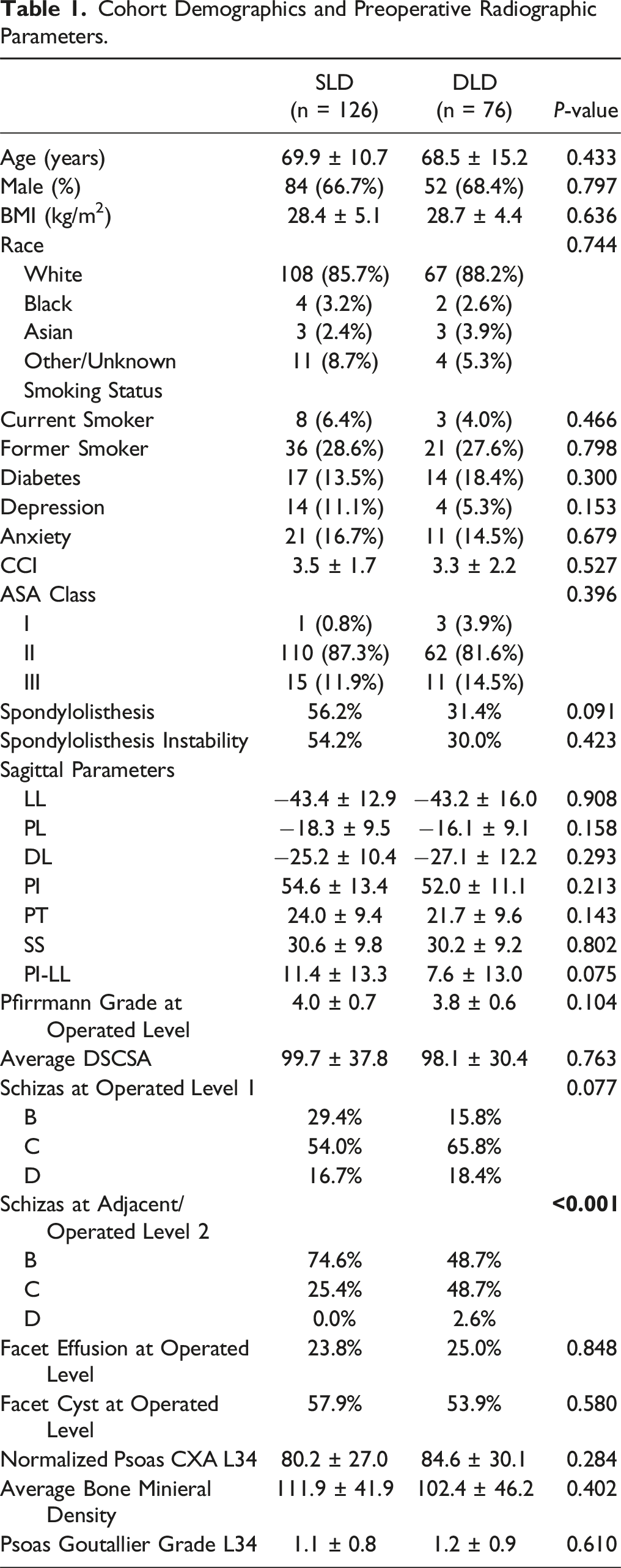
Preoperative radiographic parameters including sagittal alignment, disc health, muscle health, bone mineral density, and facet cyst/effusion, were similar between the two groups (P > 0.05 for all, Table 1). In the overall cohort, a greater proportion of patients exhibited a higher grade second-level compression in the DLD cohort based on Schizas grading (P < 0.001).
Surgical Details.
Full Cohort PROMs Improvement and Return to Activities.
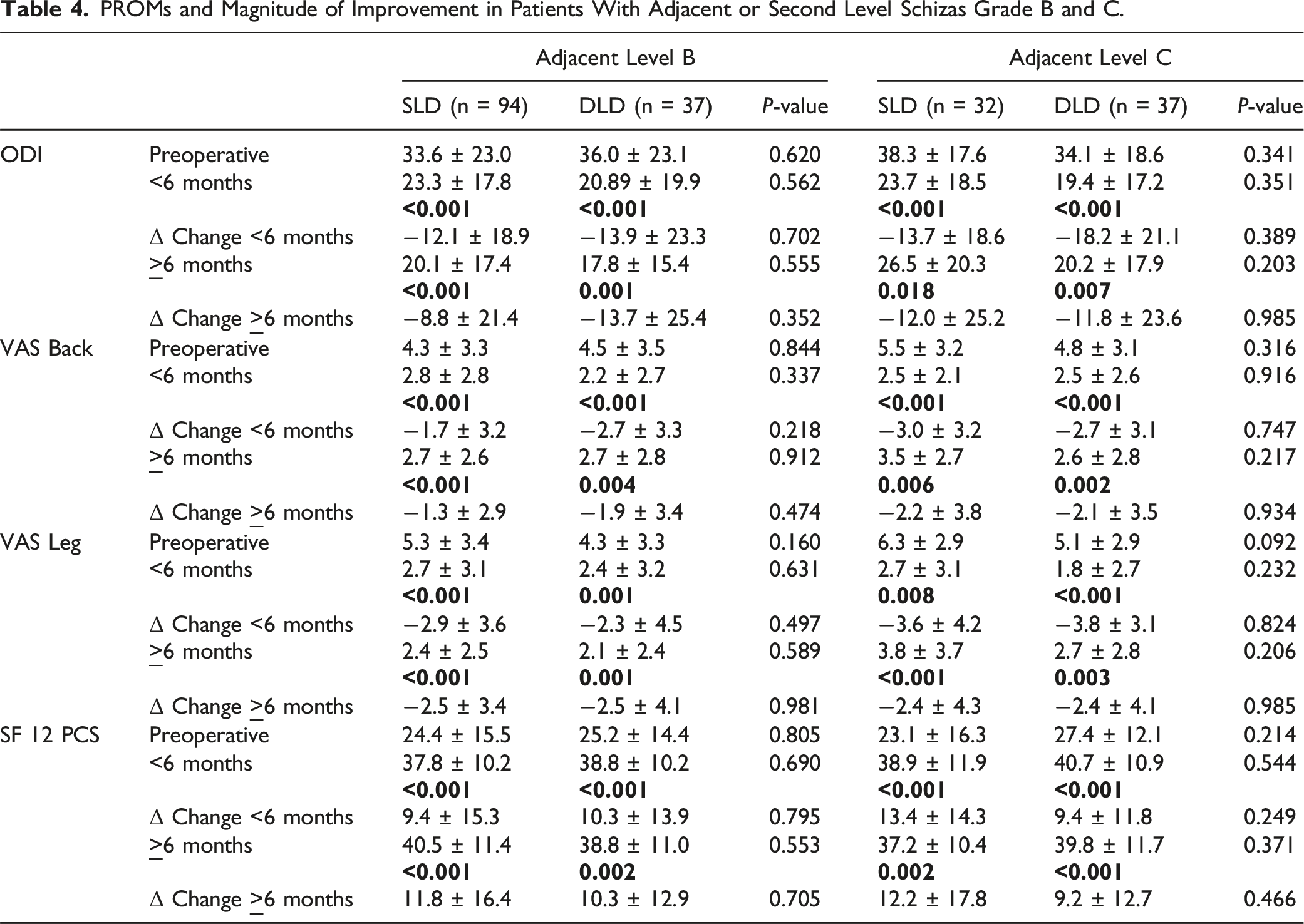
PROMs and Magnitude of Improvement in Patients With Adjacent or Second Level Schizas Grade B and C.
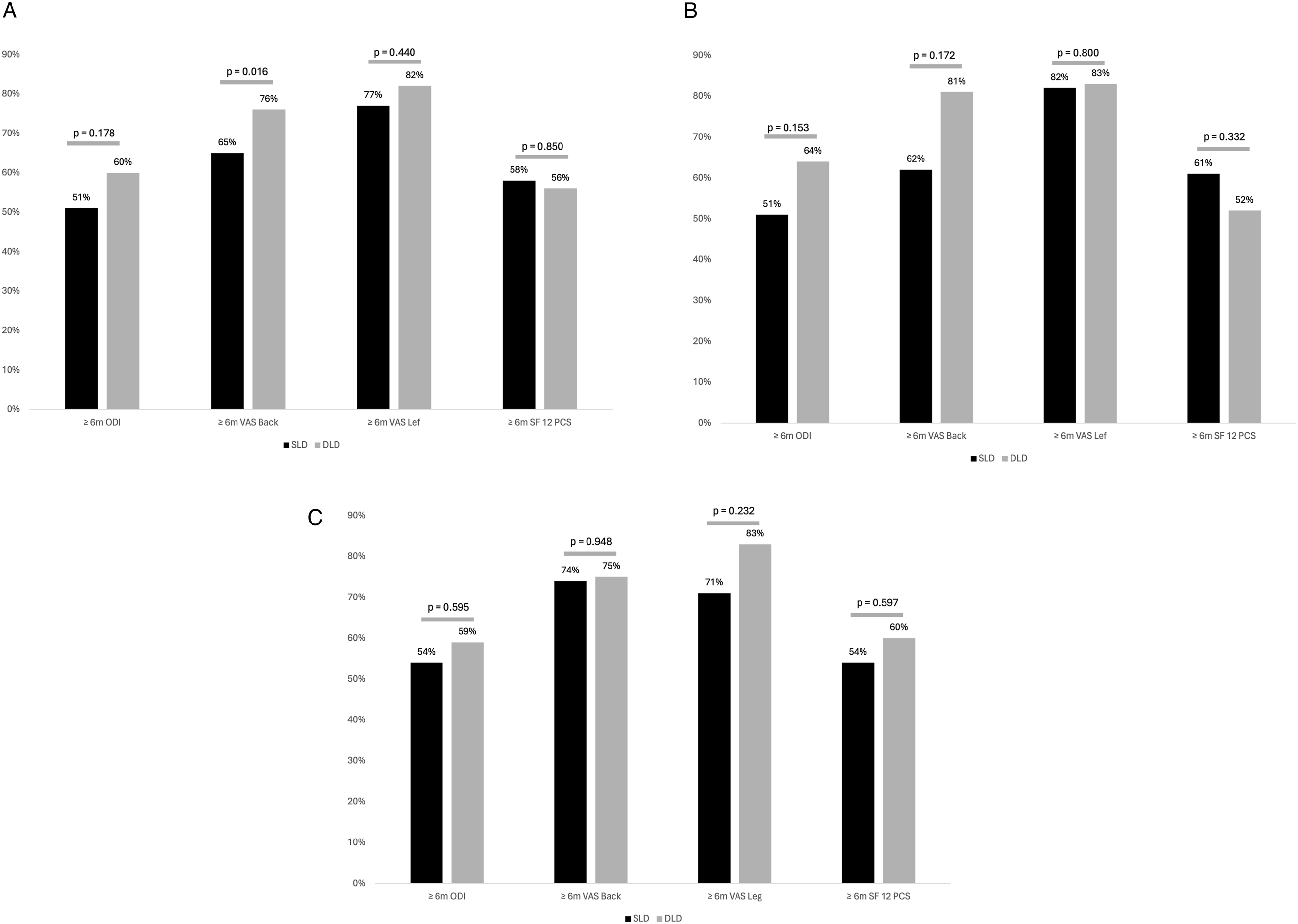
MCID achievement (A) for the entire cohort, (B) in patients with adjacent or second level Schizas grade (B and C) in patients with adjacent or second level Schizas grade (C).
Intraoperative, Perioperative and Postoperative Complications. POUR (Postoperative Urinary Retention), HTN (Hypertension), AKI (Acute Kidney Injury), UTI (Urinary Tract Infection).
Discussion
Lumbar spinal stenosis represents is a common pathology that oftentimes requires surgical intervention to improve the associated disability and decreased quality of life. In many patients with multi-level spondylosis, identifying operative levels can be a clinical and surgical conundrum. Since MRI identified stenosis oftentimes does not correlate clinically with patient symptoms, there exists a need for homogenous data regarding outcomes in patients with adjacent level stenosis. In the present study we found patients who underwent SLD with adjacent level stenosis demonstrated similar PROMs, complication rates, and reoperation rates compared with patients who underwent two DLD with similar Schizas graded compression. The added “cost” of the second level likely comes in the form of a longer operative time and a potentially greater risk of operative and perioperative complications. This suggests that even in the presence of significant adjacent level stenosis, decompressing the second level may not provide additional benefit if that level is not a significant contributor to the patient’s symptom profile.
At both early and longer-term follow-up, PROMs for ODI, VAS-Back, VAS-Leg, and SF12-PCS were similar between the single and dual level cohorts. These findings are in line with the recent study by Tronstad et al which similarly found no differences in PROMs, complications, or revisions between 1 and 2-level decompression. 9 A key limitation of the Tronstad et al study was a difference in the severity of adjacent level stenosis between the two groups. In their DLD cohort, 61 patients had Schizas grade C compression vs only 16 in their SLD group, adding significant bias to the analysis. Without performing a subgroup analysis, our patient cohort also demonstrated that a greater proportion of patients exhibited a higher grade second-level compression in the DLD group compared to the SLD group. This difference is inherent to the retrospective nature of the study as SLD or DLD is performed based on the surgeon’s clinical judgment, with patients exhibiting higher grade adjacent level stenosis being likely to be indicated for a DLD.
In order to address this, our study also performed a subgroup analysis, where we compared cohorts of patients with similar levels of second level compression. On this subgroup analysis, patients demonstrated similar pain score outcomes. By demonstrating similar findings in a cohort with comparable adjacent-level MRI findings classified according to a validated system, our study lends further credence to the notion that the radiologic appearance of stenosis does not necessitate surgical intervention in the absence of convincing clinical symptoms. This concept has been supported by several studies showing a lack of correlation between MRI findings and symptom severity in lumbar stenosis.6,7 A sub-analysis of the SPORT study published by Park et al demonstrated the number of levels treated was not predictive of outcomes in multilevel LSS. 21 External validity of these results has been demonstrated by Ulrich et al, Yoshikane et al, Adilay et al, and Yamamoto et al, who all demonstrated equal or greater pain score outcomes in single-level decompression for patients with multilevel LSS.22-25 Taken together, multilevel LSS likely represents a condition poorly correlated with symptomatology and surgical decision making should focus on addressing symptoms specifically for optimal outcomes.
Patients returned to driving, working, and discontinued narcotics at similar rates regardless of the number of levels. To the best of our knowledge, no comprehensive data has been reported regarding differences in returning to activities following SLD vs DLD. So, the question remains, what is the “cost” of the second level of surgery with regards to operative time and perioperative complications? Why not decompress the adjacent level? While differences in patient outcomes were minimal, there was a notable disparity in operative time between the SLD and DLD cohorts. There was also an approximately 2-fold increase in rates of intraoperative and perioperative complications in the DLD group though we were likely underpowered to find statistical significance. These findings are similar to results published by Adilay et al who reported a 10.4% compilation rate for single level surgery compared with 18.8% for multilevel surgery. 24 Urich et al demonstrated a 9.1% complication rate for single level vs 18.5% for multilevel surgery. 22 Importantly neither of these results were statistically significant. It is possible the current set of published cohorts are underpowered to show significance, and a pooled analysis is necessary. Regardless, this highlights the importance of considering the incremental risks of more “invasive” procedures, even if the absolute differences are small for any individual patient.
Reoperation rates were similar between our SLD and DLD cohorts, both at the index level and at adjacent segments. This argues against routinely decompressing asymptomatic stenotic levels to prevent revision surgery. Nolte et al and Yamamoto et al both compared single-level decompression vs multilevel surgery in both cases finding single-level decompressions were revised at similar rates.25,26
Thus, our findings combined with prior data suggest that patients presenting with symptomatic LSS with an adjacent level stenosis of Schizas B or C will equally benefit from either a SLD or a DLD. A caveat to this finding, however, is applying this concept for patients presenting with symptomatic LSS with two levels of equivalent grades of stenosis, particularly when the primary symptoms are neurogenic claudication. As previously described, it is especially difficult to define the “most symptomatic level” among patients with multilevel LSS presenting with neurogenic claudication.21,25 Therefore, patients presenting with symptoms of LSS with equivalent compression grade at two levels may benefit from a DLD over an SLD to ensure proper symptomatic resolution.
We acknowledge several limitations to our study. The retrospective methodology introduces the possibility of selection bias, as surgeons may have been more likely to perform dual level decompressions on patients with more severe symptoms or greater disability. Although baseline PROMs were comparable between groups, subtle differences in presentation could have influenced decision-making. The cohort size, particularly in the DLD group and radiographic subgroup analysis, limits the power of the study to detect small differences that may still be clinically relevant. Longer term follow-up would be helpful to ensure the durability of our findings, as some patients with untreated stenosis could develop recurrent symptoms over time. Additionally, our results are not necessarily generalizable to patients with different radiographic profiles than those included here. More expansive prospective studies, ideally with randomization, are needed to validate our findings and guide management across a range of clinical scenarios. Finally, the present study was not equipped to study the financial implications associated with SLD and DLD which may be necessary in the effort for optimal value-based care.
Conclusion
SLD and DLD provided equivalent outcomes among patients presenting with symptomatic LSS with two levels of Schizas B or C stenosis. There were no clear protective benefits of adjacent level surgery with regards to PROMs, complications, or reoperation rates at minimum 1-year follow-up. Surgeons should weigh the potential benefits of addressing radiologic abnormalities against the added time and small incremental risk associated with more levels of surgery. Shared decision making with patients should emphasize the primacy of their presenting complaints. Larger prospective studies with longer-term follow-ups are needed to clarify the optimal management of this common clinical scenario. Additionally, financial cost effectiveness studies comparing SLD and DLD procedural cost and costs of perioperative complications/reoperations may be helpful to better quantify the tradeoffs involved.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: State: HS2, LLC Ownership/Equity/Investment Innovasis Research Support (either personally or through HSS) Globus Medical, Inc. Speakers’ Bureau Intrinsic Therapeutics Inc. Other Bioventus Consulting HSS AND ASC Development Network Ownership/Equity/Investment. Sheeraz Qureshi has the following disclosures: AMOpportunities: Other financial or material support; Annals of Translational Medicine: Editorial or governing board; Association of Bone and Joint Surgeons: Board or committee member; Cervical Spine Research Society: Board or committee member; Contemporary Spine Surgery: Editorial or governing board; Globus Medical: IP royalties; Paid consultant; Paid presenter or speaker; Hospital Special Surgery Journal: Editorial or governing board; HS2, LLC: Stock or stock Options; International Society for the Advancement of Spine Surgery (ISASS) - Program Committee member: Board or committee member; Lifelink.com: Other financial or material support; Lumbar Spine Research Society: Board or committee member; Minimally Invasive Spine Study Group: Board or committee member; North American Spine Society: Board or committee member; Simplify Medical, Inc.: Other financial or material support; Society of Minimally Invasive Spine Surgery (SMISS) - Program Committee member: Board or committee member; Spinal Simplicity: Other financial or material support; SpineGuard, Inc.: Paid consultant; Stryker: IP royalties; Paid consultant; Surgalign: Paid consultant; Tissue Differentiation Intelligence: Stock or stock Options; Viseon, Inc.: Paid consultant; Research support. Sravisht Iyer has the following disclosures: Globus Medical: Paid presenter or speaker; Stryker: Paid presenter or speaker; Vertebral Columns/International Society for the Advancement of Spine Surgery (ISASS): Editorial or governing board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.