
Abstract
Objective
To evaluate clinical effects, and their correlations with preoperative computed tomography imaging parameters, in cases of lumbar spinal stenosis treated by endoscopic transforaminal decompression.
Methods
This retrospective study included orthopaedic patients who had undergone percutaneous endoscopic lumbar discectomy (PELD) for lumbar spinal stenosis. Clinical symptoms were evaluated by visual analogue scale (VAS), Oswestry Disability Index (ODI) and claudication distance. Overall clinical efficacy was evaluated by Macnab score.
Results
A total of 87 patients were included. Postoperative wound healing was good without complications. Macnab scores following PELD were ‘excellent’ in 41 cases (47.12%), ‘good’ in 30 cases (34.48%), ‘generally good’ in seven cases (8.04%), and ‘poor’ in nine cases (10.34%). The overall rate of optimal surgery was 81.60%. Postoperative pain (VAS) and ODI scores, and claudication distance, were significantly improved versus preoperative values. The soft tissue invasion ratio of the vertebral canal and invasion ratio of the nerve root canal were correlated with clinical efficacy.
Conclusion
Positive correlations were observed between clinical efficacy of endoscopic transforaminal decompression and preoperative vertebral canal soft tissue invasion ratio and nerve root canal invasion ratio in patients with lumbar spinal stenosis.
Introduction
Percutaneous endoscopic lumbar discectomy (PELD) has been widely used to treat various types of lumbar intervertebral disc herniation, with satisfactory clinical effects.1,2 The advantages of PELD include its minimally invasive nature (8-mm incision), ability to penetrate physiological channels (intervertebral bore), and minimal tissue destruction. With technological development and continuous improvement of instruments and equipment, percutaneous spinal endoscopic technology has been used by clinicians to treat lumbar spinal stenosis. A previously published study of 320 consecutive patients showed that percutaneous endoscopic technology was safe and effective in treating lumbar spinal stenosis, 3 however, the efficacy of treating lumbar spinal stenosis with PELD remains under question by surgeons who prefer traditional open techniques. Furthermore, another study reported that although PELD could be used to treat lumbar spinal stenosis disease by expanding the intervertebral foramen and removing the lateral yellow ligament, there is a relatively limited scope for this operation. 4 In patients with severe hyperplasia and serious intervertebral foramen stenosis, it is difficult to enter the intervertebral pore, which requires a drill and bone chisel and is associated with a longer operation time.
At Shanghai Provincial People’s Hospital, PELD is currently used to treat lumbar spinal stenosis in some patients. From preliminary clinical observations, most patients have achieved satisfactory postoperative clinical outcomes, however, some patients have not obtained ideal surgical outcomes. The present authors speculate that poor surgical outcomes may be due to the fact that endoscopic surgery has limited effect on relieving bone compression, which contributes to lumbar spinal stenosis. Furthermore, different proportions of bony stenosis and soft tissue stenosis in patients with lumbar spinal stenosis may lead to differences in surgical outcomes. Following a thorough and comprehensive review of the literature, the associated evidence was found to be limited. Therefore, the aim of the present study was to evaluate the relationship between preoperative imaging parameters and clinical outcome in patients with lumbar spinal stenosis who were treated using PELD.
Patients and methods
Study population
This retrospective study included data from consecutive patients with lumbar spinal stenosis who received PELD at Shanghai Provincial People’s Hospital between June 2014 and January 2016. The study was approved by the ethics committee of Shanxi Provincial People's Hospital and written informed consent for treatment and to collect data for retrospective analyses was obtained from all patients.
Inclusion criteria comprised: (1) aged 25–85 years; (2) unilateral or bilateral symptoms of nerve root with (or without) cauda equina compression performance; (3) single segment segmental stenosis symptoms; (4) neurogenic intermittent claudication; and (5) imaging findings consistent with clinical symptoms: lateral crypt and/or intervertebral pore stenosis, central vertebral canal and/or mixed spinal stenosis.
Exclusion criteria comprised: (1) intervertebral instability; (2) osseous infection; (3) tumour(s); (4) mental abnormalities and communication difficulties; (5) neurological symptoms caused by intervertebral disc herniation; (6) previous history of spinal surgery; and (7) Conservative treatment is effective for 3-6 months.
Surgical technique
The segment of interest for decompression was identified according to the patient’s preoperative computed tomography (CT) and magnetic resonance imaging (MRI) parameters, and their clinical symptoms. All PELD surgeries were performed by a senior spine surgeon (LL) to ensure the completion of sufficient decompression during surgery. Fluoroscopically guided lateral percutaneous puncture was performed to the apex of the superior articular process of the lower vertebral body of the lesion segment. The guide wire was inserted and expanded step by step. According to different dilated pipelines, the bone in the ventral side of the superior articular process was removed by ring saw to the outer boundary of the vertebral canal. The working pipe was placed, followed by endoscopic resection of the lateral fibrous ring and the posterior yellow ligament to explore the nerve roots. Under endoscopic monitoring, the tube was pushed again into the vertebral canal at the nerve root ventral side. The posterior edge of the lower vertebral body was blocked, and part of the vertebral body was removed by circular saw, under microscopic guidance, to expand the visual field and operating range. Nucleus pulposus was removed and dorsal yellow ligament was dissected for decompression. The nerve roots were probed throughout to ensure complete decompression. A fine drainage tube was then inserted, the working pipe was removed and the wound was sutured. Postoperative dehydration and neuro-nutrition were administrated. At one day following surgery, the drainage tube was removed and a waist support was worn to limit movement. Representative imaging data, collected before and after surgical decompression, are shown in Figure 1 and 2.

Representative radiographic images showing that the passageway can be placed: (a) in the rear or (b) in front of the dura capsule to reach the midline.

Representative endoscopic and computed tomography (CT) images, showing: (a) a pre-decompression endoscopy image; (b) a post-decompression endoscopy image; (c) coronary plane CT showing decompression of the nerve root canal and the central vertebral canal; and (d) sagittal plane CT showing decompression of the root canal.
Data collection
Functional assessment
Clinical symptoms were assessed using the following: a visual analogue scale (VAS) for pain,5,6 measured on a scale of 0–100, with higher scores equating to more pain; the Oswestry Disability Index (ODI),7,8 scored on a scale of 0–100%, with higher scores equating to higher levels of disability; and claudication distance. These factors were evaluated independently by two orthopaedic surgeons (LL, JS) during the preoperative period and at 3 and 6 months postoperatively. Overall clinical efficacy was assessed using Macnab scores of patient satisfaction, with patients categorised as ‘excellent’, ‘good’, ‘fair/generally good’, or ‘poor’. 9
Imaging parameter measurements
Patients were evaluated by CT using a Siemens 64-layer spiral CT scanner (Siemens Healthcare GmbH, Erlangen, Germany). The following indicators were measured by two imaging doctors (CX, JY) who were blinded to the patient's condition, and 64-layer spiral CT analysis software (Siemens Healthcare GmbH) was used to calculate the mean values of various parameters (Figure 3), including the bony vertebral canal area (C) (Figure 4), real spinal canal area (D) (Figure 4), nerve root canal bony area (E) (Figure 5), and the nerve root canal real area (F) (Figure 5). A further two parameters were calculated using the above measurements: the soft tissue invasion ratio of the vertebral canal (I), which was calculated as bony vertebral canal area (C) – the real spinal canal area (D)/bony vertebral canal area (C); and the invasion ratio of the nerve root canal (J), which was calculated as nerve root canal bony area (E) – nerve root canal real area (F)/nerve root canal bony area (E).
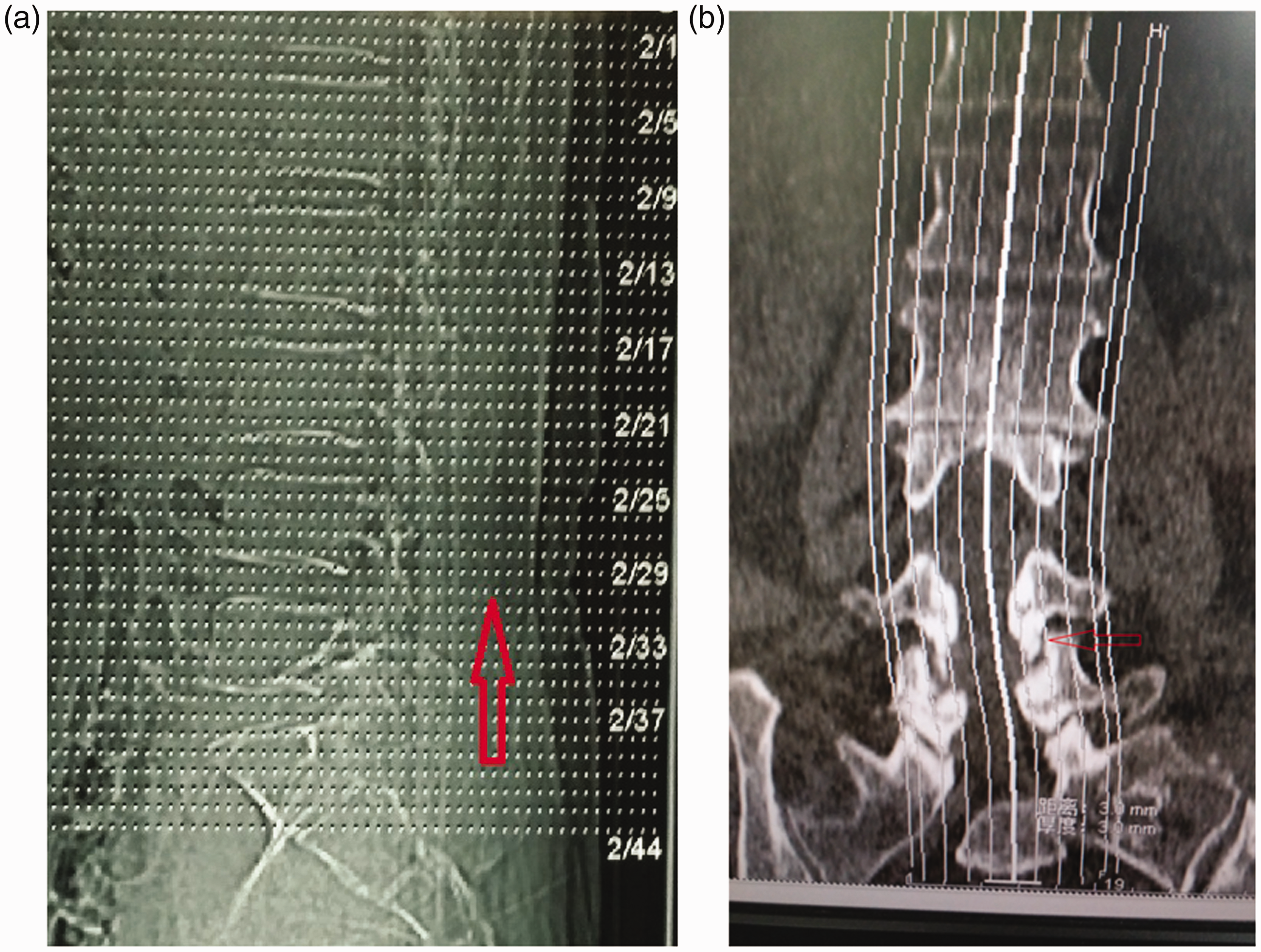
Representative images showing analysis of computed tomography (CT) scan results: (a) sagittal plane CT of the cross-sectional area of the vertebral canal (arrow shows scanning results of the middle of the interstitial three layers); and (b) CT of the area of the intervertebral pore (arrow shows scanning results of the joint interarticulation).

Representative computed tomography images, showing: (a) measurement of the bony vertebral canal area (designated ‘C’ for calculations); and (b) measurement of the real spinal canal area (designated ‘D’ for calculations).

Representative computed tomography images, showing: (a) measurement of the nerve root canal bony area (designated ‘E’ for calculations); and (b) measurement of the nerve root canal real area (designated ‘F’ for calculations).
Statistical analyses
Patients were divided into groups according to change in claudication distance between preoperative and 6-month postoperative assessment: group 1 (excellent, ≥1000 m), group 2 (good, 500–1000 m), group 3 (generally good, 250–500 m), and group 4 (poor, < 250 m). Variables are presented as mean ± SD, and statistical analyses were performed using SPSS software, version 18.0 (IBM Corporation, Armonk, NY, USA). Differences in VAS and ODI scores, and claudication distance, between the pre-operative period and 3 and 6 months after surgery were analysed using an F test. Correlations between preoperative CT imaging variables, calculated parameters and clinical outcome variables (VAS and ODI scores, and claudication distance) were evaluated using Pearson’s correlation coefficient (presented as Pearson’s r). A P value < 0.05 was considered to be statistically significant.
Results
A total of 87 patients were enrolled in the study, comprising 45 male patients (51.72%) and 42 female patients (48.28%) with a mean age of 55.14 years (range 25–81 years). Patients were affected in the following lumbar regions: L3/4 (eight patients), L4/5 (61 patients) and L5/S1 (18 patients). Postoperative wound healing was good without complications, defined as healing without inflammation or secretions.
After categorizing patients according to change in claudication distance, there were 78, four, three and two patients in the ‘excellent’, ‘good’, ‘generally good’, and ‘poor’ groups, respectively (change in claudication distance: 1391.85 ±119.10 m, 657.75 ± 193.59 m, 370.17 ±104.96 m, and 215.50 ± 0.71 m for each group, respectively). The distribution of Macnab scores following PELD were as follows: ‘excellent’ in 41 cases (47.12%), ‘good’ in 30 cases (34.48%), ‘generally good’ in seven cases (8.04%), and poor in nine cases (10.34%). The overall rate of optimal surgical treatment (excellent/good Macnab scores) was 81.60%. Preoperative, and 3- and 6-month postoperative values for VAS, ODI and claudication distance were as follows: VAS, 63.88 ± 8.56 versus 13.22 ± 8.24 and 6.83 ± 9.43; ODI, 59.96 ±12.60 versus 9.08 ± 10.55 and 5.64 ± 6.84; and claudication distance, 114.55 ± 150.22 versus 1363.97 ± 321.44 and 1410.39 ±306.71. Postoperative VAS, ODI and claudication distance at 3 months and 6 months were significantly improved compared with preoperative values (P < 0.01; Table 1).
Overall clinical effect, at 6 months postoperatively, of treatment with endoscopic transforaminal decompression in 87 patients with lumbar spinal stenosis.

VAS, visual analogue scale; ODI, Oswestry Disability Index; SS, standard deviation squared; MS, mean square.
Correlation analyses showed that soft tissue invasion ratio of the vertebral canal (I) and invasion ratio of the nerve root canal (J) were positively correlated with improvements in VAS and ODI scores, and claudication distance at 6 months postoperatively versus preoperative values (Table 2, Figure 6 and Figure 7).
Pearson’s correlation coefficient analyses of the association between preoperative computed tomography imaging parameters and clinical efficacy at 6 months following treatment with endoscopic transforaminal decompression in 87 patients with lumbar spinal stenosis.

CT, computed tomography; VAS, visual analogue scale; ODI, Oswestry Disability Index; C, bony vertebral canal area; D, real spinal canal area; E, nerve root canal bony area; F, nerve root canal real area; I, soft tissue invasion ratio of the vertebral canal; J, invasion ratio of the nerve root canal.
NS, no statistically significant correlation (P > 0.05; Pearson’s correlation coefficient).

Scatter plots showing a positive correlation between preoperative soft tissue invasion ratio of the vertebral canal (I) and improvements in the following clinical efficacy measures at 6 months postoperatively versus preoperative values: (a) pain measured by visual analogue scale (VAS); (b) Oswestry Disability Index (ODI); and (c) claudication distance. (a and b) y-axes represent preoperative minus postoperative scores; and (c) y-axis represents postoperative minus preoperative distance.

Scatter plots showing a positive correlation between preoperative invasion ratio of the nerve root canal (J) and improvements in the following clinical efficacy measures at 6 months postoperatively: (a) pain measured by visual analogue scale (VAS); (b) Oswestry Disability Index (ODI); and (c) claudication distance. (a and b) y-axes represent preoperative minus postoperative scores; and (c) y-axis represents postoperative minus preoperative distance.
Discussion
At present, there is no uniform worldwide standard of surgical indications for treating lumbar spinal stenosis, and opinions vary regarding the treatment of lumbar spinal stenosis with percutaneous endoscopic technology. In a study of patients who received decompression of the lumbar lateral recess using a suprapedicular foraminal endoscopic approach, the combined excellent and good rate was 84.62%, and the technique was shown to be safe and effective with satisfactory outcomes, particularly for elderly patients with complicated underlying diseases. 10 The authors commented, however, that there is more blood loss when treating lateral recess stenosis using transforaminal endoscopic surgery. 10 A study of microscope-guided treatment of lumbar spinal stenosis disease through the intervertebral foramen reported that the operation time for this type of surgery was short, haemorrhage was minimal, and operative and postoperative complications were slightly more than those of conventional surgery. 3 Thus, the authors concluded that this approach was safe and effective for lumbar spinal stenosis. 3 A summary of the surgical techniques for treating lumbar vertebral stenosis through a percutaneous intervertebral foramen approach highlighted both the advantages and disadvantages of selecting the laminae or foramen in different parts of the lumbar vertebrae. 11 Another review of relevant information on the treatment of lumbar spinal stenosis in multiple hospitals, using a percutaneous intervertebral foramen technique, showed that all patients had good clinical effects without significant differences compared with conventional surgery. 12 The advantages of the technique in terms of safety and treatment cost were compared, and the authors concluded that percutaneous intervertebral foramen mirror technology may effectively resolve most cases of lumbar spinal stenosis, even if it was difficult to reach these areas during surgery, but it may not be sufficient to relieve the stress. 12 Clinicians should balance the advantages and disadvantages when blind decompression has the potential to increase the risks associated with surgery. Surgical indications for treating lumbar spinal stenosis with percutaneous endoscopic technology, and comparisons with conventional open surgery, remain unclear, and further evidence is required.
Imaging measurement in cases of lumbar spinal stenosis is an auxiliary and indispensable examination that can be performed to provide diagnosis. CT imaging has been reported to enable accurate delineation of the lumbar spinal stenosis area boundary, and measurements of the area, angle and segment length using measurement software were found to be more accurate and reasonable than previous measurement techniques. 13 In a 1982 study, measurement of the bones of 100 corpses found the spinal canal diameter in L4 was 15.31 ± 2.23 mm and in L5 was 15.98 ± 2.58 mm. Measurement of the bones of 100 corpses in a 1983 study showed that the spinal canal diameter in L4 was 15.43 mm and in L5 was 16.68 mm. 13,14 Guo et al. 15 reported that the diameter of the L5 vertebral canal was 16.61 ± 2.42 mm. Spinal canal diameters measured by CT imaging have been reported to be 15.44 ± 3.06 mm in L4 and 16.18 ± 2.29 mm in L5, 13 which is very similar to those of the above cadaver measurements, indicating that results of CT imaging to measure vertebral canal diameters are close to physical specimen measurement.
A total of 87 cases of lumbar spinal stenosis treated with percutaneous endoscopic technology were analysed in the present study, and postoperative wound healing was found to be good, without complications. The VAS and ODI scores, and claudication distance were significantly improved following treatment compared with preoperative values, and the overall rate of optimal surgery was 81.60%. Although percutaneous endoscopic decompression surgery may have good clinical efficacy and unique minimally invasive advantages in the treatment of degeneration in spinal canal stenosis,16–19 the present study still found that treatment was less effective in over 10% of the patients. There are several factors that may contribute to the relatively low overall rate of optimal surgery in the present study, and may limit the present results, including small sample size, short follow-up time, and broad patient selection. Choice of surgical indications depends on a good preoperative evaluation, since lumbar spinal stenosis remains a greater challenge than lumbar disc herniation. It is also important to focus on the complications of surgery, such as injury to the dural sac, nerve injury and radiation exposure.20–22
Correlation analysis of preoperative imaging parameters and post-treatment effect revealed positive correlations between clinical efficacy and the preoperative soft tissue invasion ratio of the vertebral canal (I) and invasion ratio of the nerve root canal (J). Thus, the results suggest that spinal stenosis caused by soft tissue may have better postoperative efficacy, possibly due to the characteristics of this particular treatment technique, which may remove too much bony structure and increase the risk of intervertebral instability.
In conclusion, the present study demonstrated that treatment of lumbar spinal stenosis by endoscopic transforaminal decompression may achieve good clinical results. There was a positive correlation between clinical treatment effect and preoperative soft tissue invasion ratio of the vertebral canal (I) and invasion ratio of the nerve root canal (J). The results of this study have a clear guiding significance for the clinical application of intervertebral endoscopy in the treatment of lumbar spinal stenosis, however, they should be viewed cautiously due to the limited amount of clinical data collected and limited follow-up time. Further studies are required to verify the present findings.