
Abstract
Study Design
Systematic review, expert opinion and Delphi technique, and validity and reliability studies.
Objective
We developed Jakarta Instability Score (JIS) to identify spinal instability and the need of fusion in degenerative lumbar spinal stenosis (LSS).
Methods
This study consisted of systematic review to find predictors of spinal instability, expert opinion and modified Delphi technique to develop JIS, and validity and reliability studies of the newly developed JIS.
Results
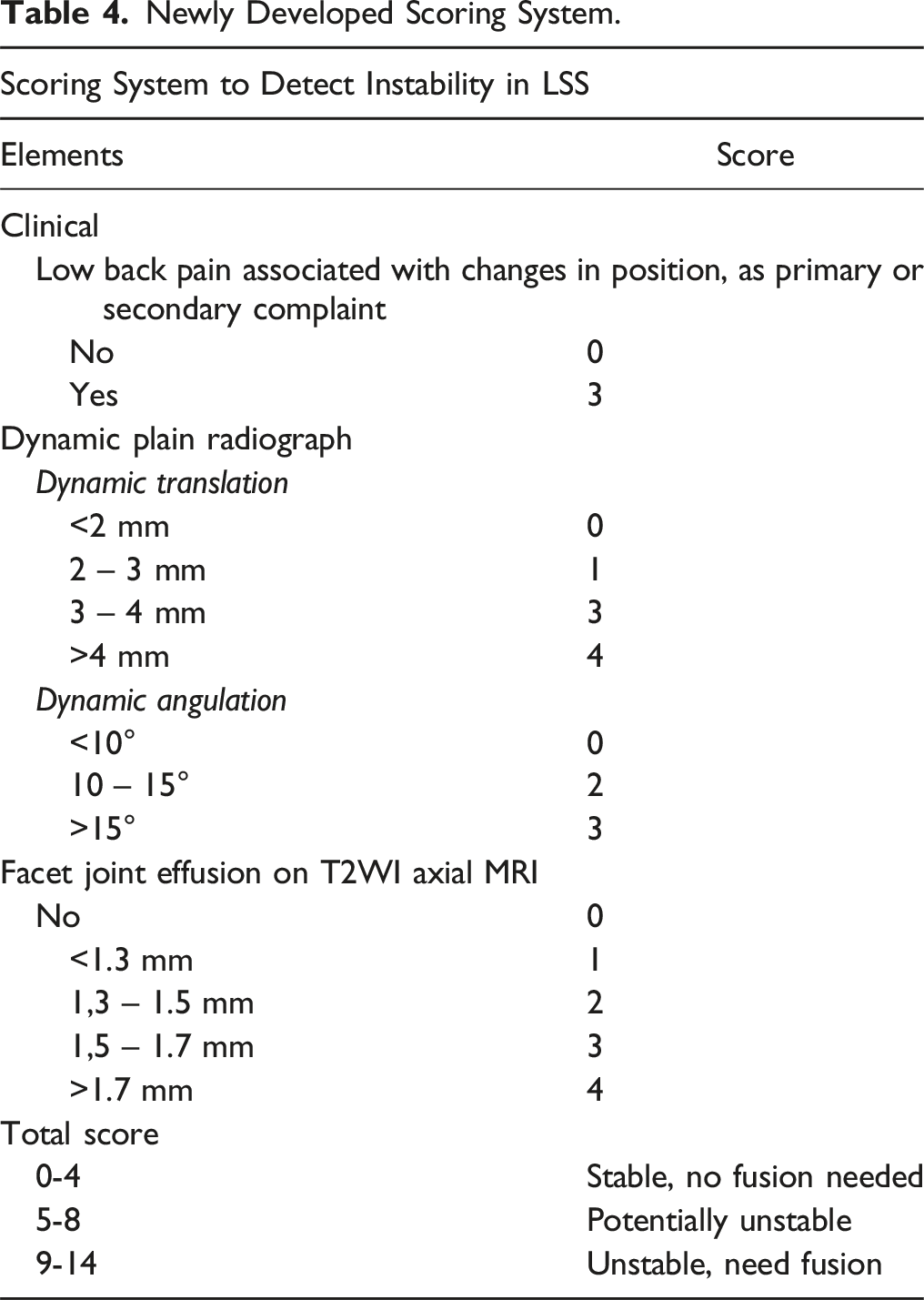
A total of 54 studies were included in the systematic reviews to obtain predictors of spinal instability. Through expert opinion and modified Delphi technique, JIS was developed and consisted of the clinical component (back pain), dynamic radiograph component (dynamic translation and angulation), and MRI component (facet joint effusion), each of the component would be scored, and the total scoring would be from 0 to 14. The final scoring would classify patients into three groups: stable group (score of 0 to 4) in which the fusion is not needed, potentially unstable group (score of 5 to 8) in which the decision of fusion is based on surgeon’s clinical judgment, and unstable group (score of 9 to 14) in which the fusion is needed. Final step of study concluded that this JIS had a high validity and reliability.
Conclusion
The newly developed JIS was a valid and reliable scoring system that could help to identify the presence of instability in LSS and can be used as a guideline to decide whether spinal fusion will be needed.
Introduction
Degenerative lumbar spinal stenosis (LSS) is defined as degenerative, pathological condition characterized by narrowing of the spinal canal, foramen, or lateral recess. This pathological condition can cause a clinical entity called as neurogenic claudication. 1 In mild and moderate cases, the main treatment is non operative. Surgical treatment by decompression is indicated in cases with persistent symptoms even after non operative treatment or in cases with severe stenosis. Beside decompression, fusion or arthrodesis of the vertebra is needed if the stenosis is associated with spinal instability. 2 Spinal stability is defined as the ability of the spine to maintain its degree of motion while simultaneously preventing pain, neurologic deficit, and abnormal angulation. 3 Traditionally, spinal instability was diagnosed based on finding of segmental translation in sagittal plane of 4.5 mm or more. 4 This finding is seen in plain radiograph of lumbar vertebral in lateral view in flexion and extension positions. 5
Several studies reported that beside decompression, addition of fusion in LSS associated with instability provided significantly better improvement of low back pain and leg pain compared to decompression alone. 6 For that reason, it is important to accurately identify patients with LSS who are also suffer from spinal instability. 5 Literatures showed that clinical and radiological assessment of instability in cases of degenerative LSS is still difficult to be performed because instability in cases of degenerative LSS was not only seen in flexion and extension plain radiographs. 7 Several findings in plain radiograph and magnetic resonance imaging (MRI) other than segmental translation can identify the presence of spinal instability. 5
According to the literature, specific scoring system to asses spinal instability had been available for cases of malignancy (Spinal Instability Scoring System – SINS) 8 and infection (Spinal Instability Spondylodiscitis Score – SISS and Spinal Infection Treatment Evaluation Score – SITE Score).9,10 Up until now, there is no available scoring system which clinically and radiologically are able to detect spinal instability in degenerative LSS.11,12 Due to lack of guideline, spine surgeons relied on clinical experience and dynamic or flexion and extension plain radiographs to detect the presence of instability and to assess whether fusion is indicated.
The development of simple scoring system containing clinical and radiological elements which is easy to apply will aid a proper communication and referral between spine surgeons and radiologists, in order to ensure that optimal surgical planning can be given to the patients. Moreover, the scoring system will be able to achieve a more consistent therapeutic approach between spine surgeons and will also be helpful in education and research fields. The aim of this study was to use evidence-based medical process which combine the best studies yielded from systematic literature review, expert opinion, and Delphi technique to develop a new instrument or scoring system that are able to detect instability and the need of fusion in degenerative LSS. This study also assess the validity and reliability of this newly developed scoring system in our institutional hospital. This new scoring system is identified as Jakarta Instability Score (JIS).
Materials and Methods
This study consisted of three stages: systematic literature review to obtain clinical and radiological indicators of spinal instability in LSS; expert opinion and modified Delphi technique to develop the scoring system; and validity and reliability study of the newly developed scoring system.
Systematic Literature Review
The first stage of research was a systematic literature review following the guidelines of The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020. 13 The systematic literature review aimed to find clinical and radiological indicators related to spinal instability in LSS based on evidence-based literature review. The indicators obtained from the systematic literature review would later be assessed through expert opinion and modified Delphi technique.
The systematic literature review began with the formulation of research questions based on the PICO framework (patient/population/problem, comparison, intervention, and outcome). After asking questions, the next step was to determine a library search plan. A literature search was carried out using keywords, index terms (including MeSH/Medical Subject Headings), and Boolean operators on the Medline/Pubmed and Google Scholar databases. Bibliographies of articles included in the observations were also added individually. By using this method, authors would get a sentence that will be used in library searches on Internet search engines. The inclusion criteria for the literature were English literatures that defined spinal instability, study performed in human, available in full article, published within 10 years from 2013 to 2023, with the keywords “spinal stenosis [mh] AND instability”. The exclusion criteria were systematic review or meta-analysis study, animal study, and article published in a language other than English.
The methodological quality of each study obtained from literature review was assessed using the level of evidence in medicine criteria. 14 Studies were also assessed for risk of bias using the criteria presented in the Cochrane handbook. Assessment of quality and risk of bias in RCT studies has been carried out using domain-based evaluation while assessment for non-RCT studies has been carried out using the Newcastle-Ottawa Scale, as recommended by The Collaboration. 15
Expert Opinion and Modified Delphi Technique
The second stage of research is expert opinion and modified Delphi technique to see the experts’ assessments of instability indicators obtained from the literature review. The second stage research sample was Orthopaedic spine surgeons in Indonesia who had completed formal spine sub-specialist education in Indonesia, with clinical experience of more than 10 years, who worked in an Orthopaedic educational institution and had been selected based on discussions with the supervisor, and taking into consideration that the experts in their daily practice as an Orthopaedic spine surgeon who handle many spine cases. Expert opinion is one of the key components in evidence-based medical science which is used later in building consensus. 16
The modified Delphi technique is a communication technique between individuals in a group who are geographically separated. This technique allows a group to solve problems or tasks systematically.
8
The group referred here was Orthopaedic spine surgeons in Indonesia with criteria as mentioned before. The task in question here was the question of how to determine spinal instability in cases of LSS. The Delphi technique was used to collect and filter the knowledge obtained from the experts by providing a questionnaire form to be filled in. The modified Delphi technique process was explained as follows: 1. The first process in the modified Delphi technique was to ask each of Orthopaedic spine surgeons about what factors or findings are associated with or indicate spinal instability in LSS. The results of the experts’ answers were then compiled and combined with the results of the systematic literature review. 2. A questionnaire form was then prepared to assess the experts’ opinions regarding each indicator found, to see how important this factor is in indicating spinal instability in LSS. The indicators assessed were the results obtained from stage 1 of the research. These indicators were arranged in a questionnaire and divided into three groups, namely clinical factors, static (AP and lateral) and dynamic (flexion and extension) plain radiographs and MRI. Experts were asked to give a value from 0 to 10 for each indicator, with a value of 0 indicating that the indicator has no relevance or relationship to spinal instability, and a value of 10 indicating that the indicator had absolute importance in the presence of spinal instability in LSS. This first process was called as the first round. 3. The results of the assessments from the experts were then combined and grouped into 3 groups. Factors with a value of ≥7 were categorized as factors with high relevance, factors with a value of 4 – < 7 were included as factors with medium relevance, and factors with a value <4 were included as factors with low relevance. 4. Second questionnaire was then prepared, which contained repeated questions like the questions in the first round. This process was called as the second round. The second round was carried out 3 to 5 days from the second round. The answers from the experts were then compared with the answers from the first round and compared statistically. If there were no significant differences, then the study proceeded. 5. A new assessment system was developed to assess instability and the need for spinal fusion in cases of degenerative LSS, namely the Jakarta Instability Score – JIS, where the components were composed of the results of expert opinion and the first and second rounds of the Delphi technique. 6. The new assessment system that has been prepared will be given back to the experts to see whether the experts agreed with the new assessment system.
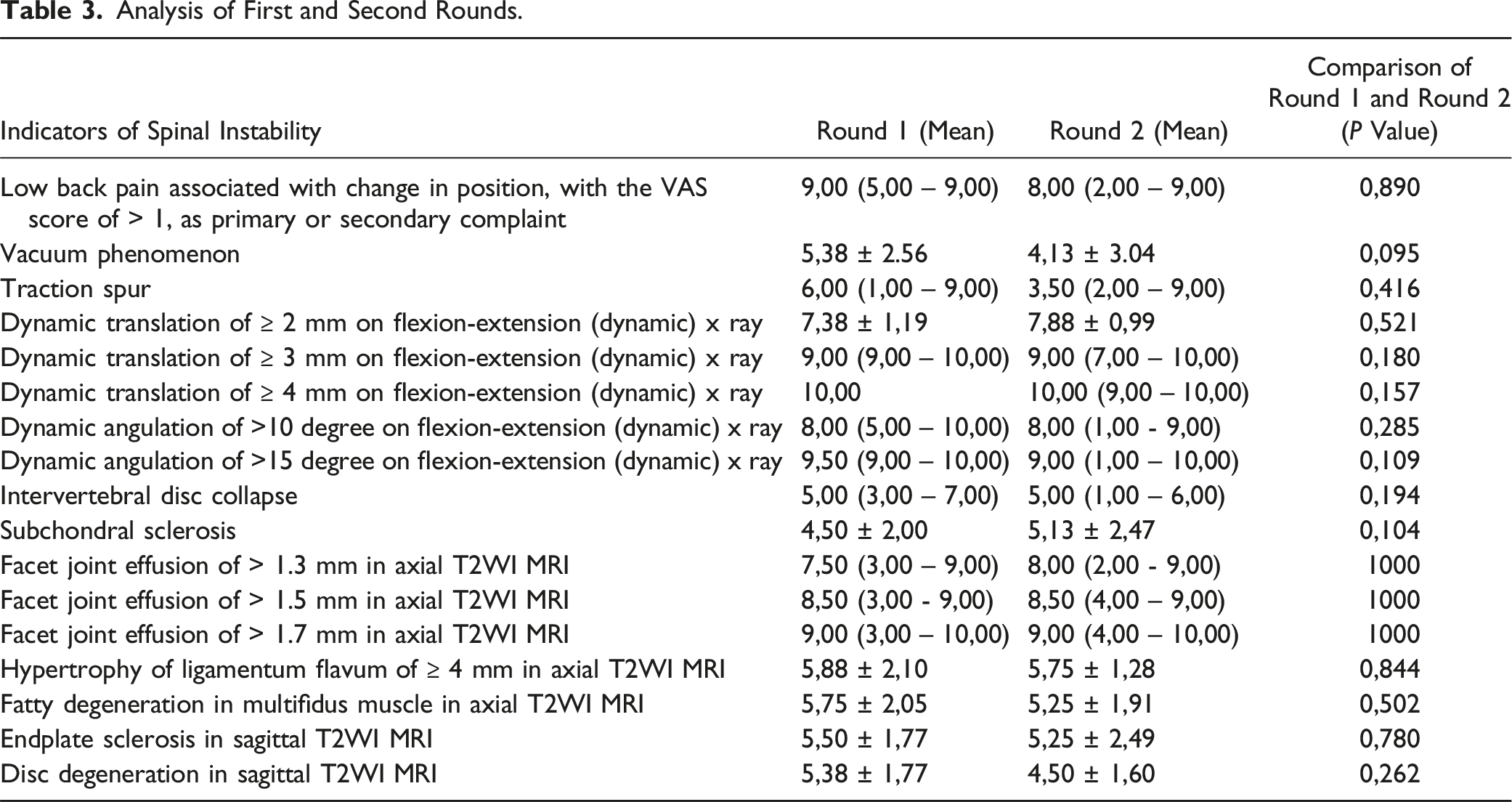
For the analysis, the paired t test was carried out to assess the differences between the experts’ answers to the questionnaire in first round and second round. This test was used to see whether discussion or rethinking in second round changed the experts’ opinions about the instability indicators. Analysis was carried out using SPSS software, with a P value < .05 considered as statistically significant with a confidence interval of 95%.
Validity and Reliability Study
Cohen’s k Value.
Results
Systematic Literature Review
After applying inclusion and exclusion criteria, a total of 54 articles were extracted. The literature search is presented in Figure 1. Literature search chart through systematic literature review.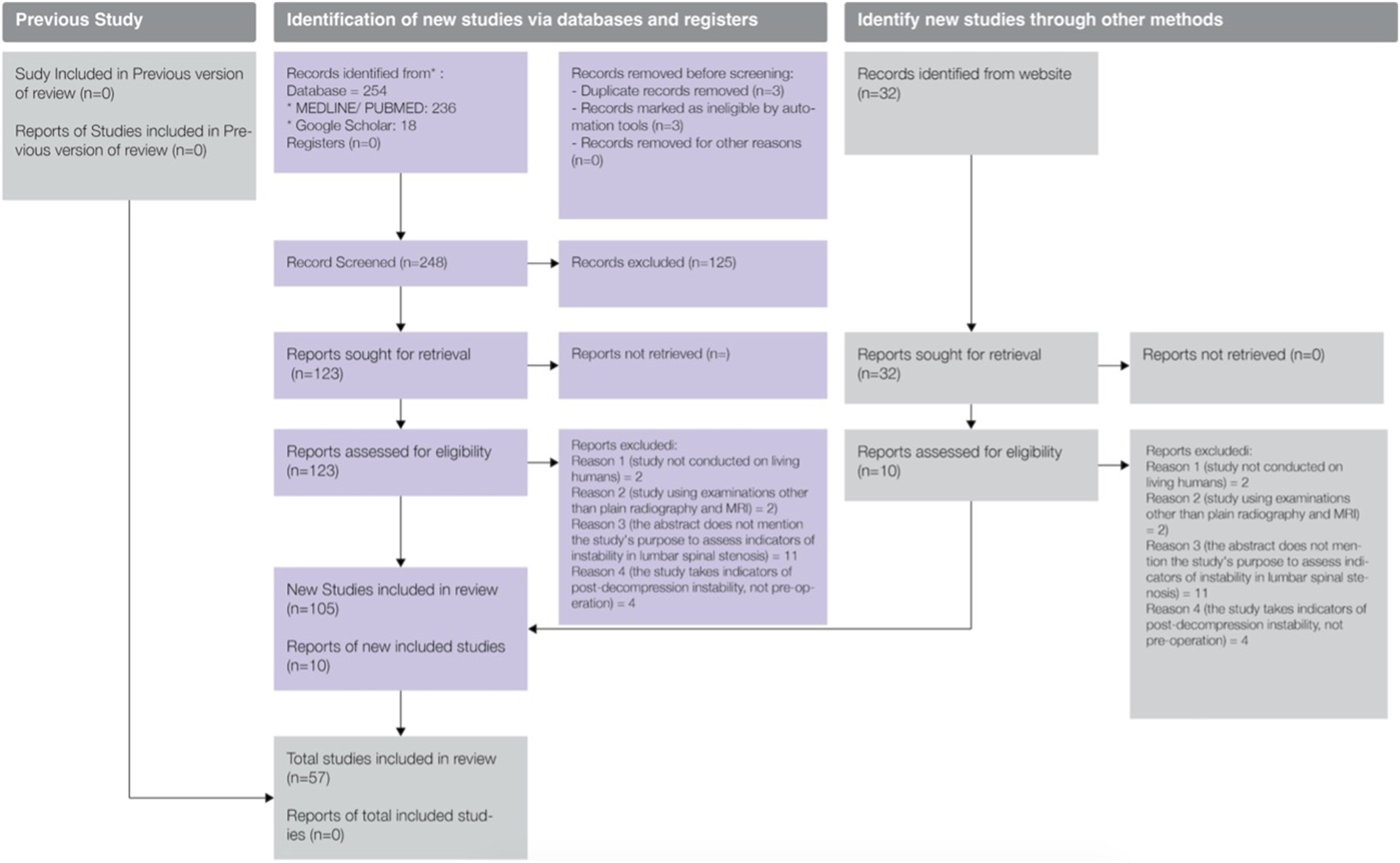
There were 3 randomized controlled trial (RCT) studies included in the literature review. The assessment of the research methods of these studies was carried out using domain-based evaluation. The results of the methodological evaluation showed that all studies had the potential to have bias from other sources and only one study from Farrokhi et al
23
which has the potential to have selective bias. The results of the study methodology assessment for RCT were listed in Figure 2. Quality assessment of non-RCT studies was carried out using the Newcastle-Ottawa Scale.
24
There were 51 non-RCT studies included in the systematic literature review. A total of 45 studies were studies of good quality and 6 studies were studies of medium quality. RCT study assessment chart based on domain-based evaluation.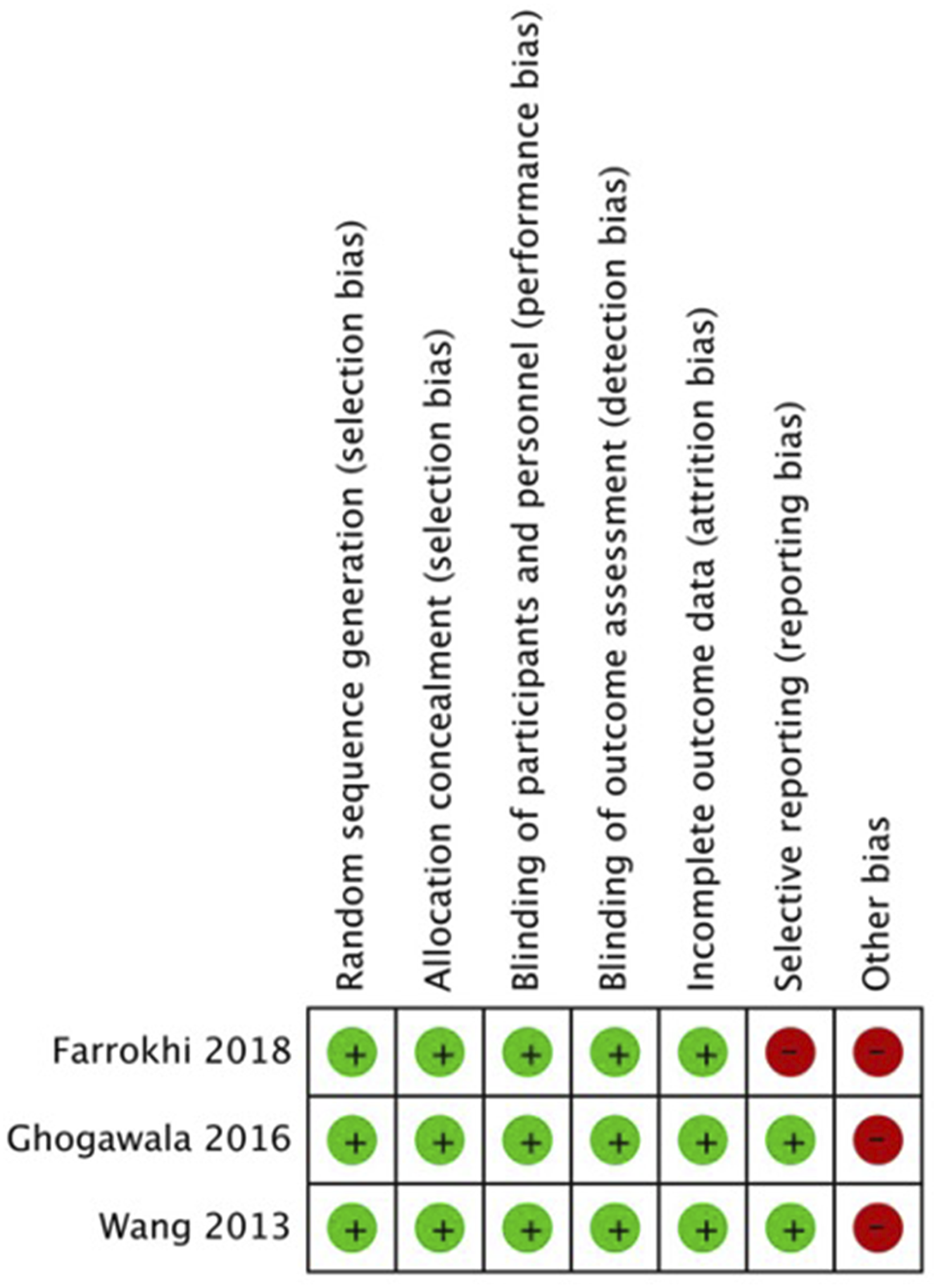
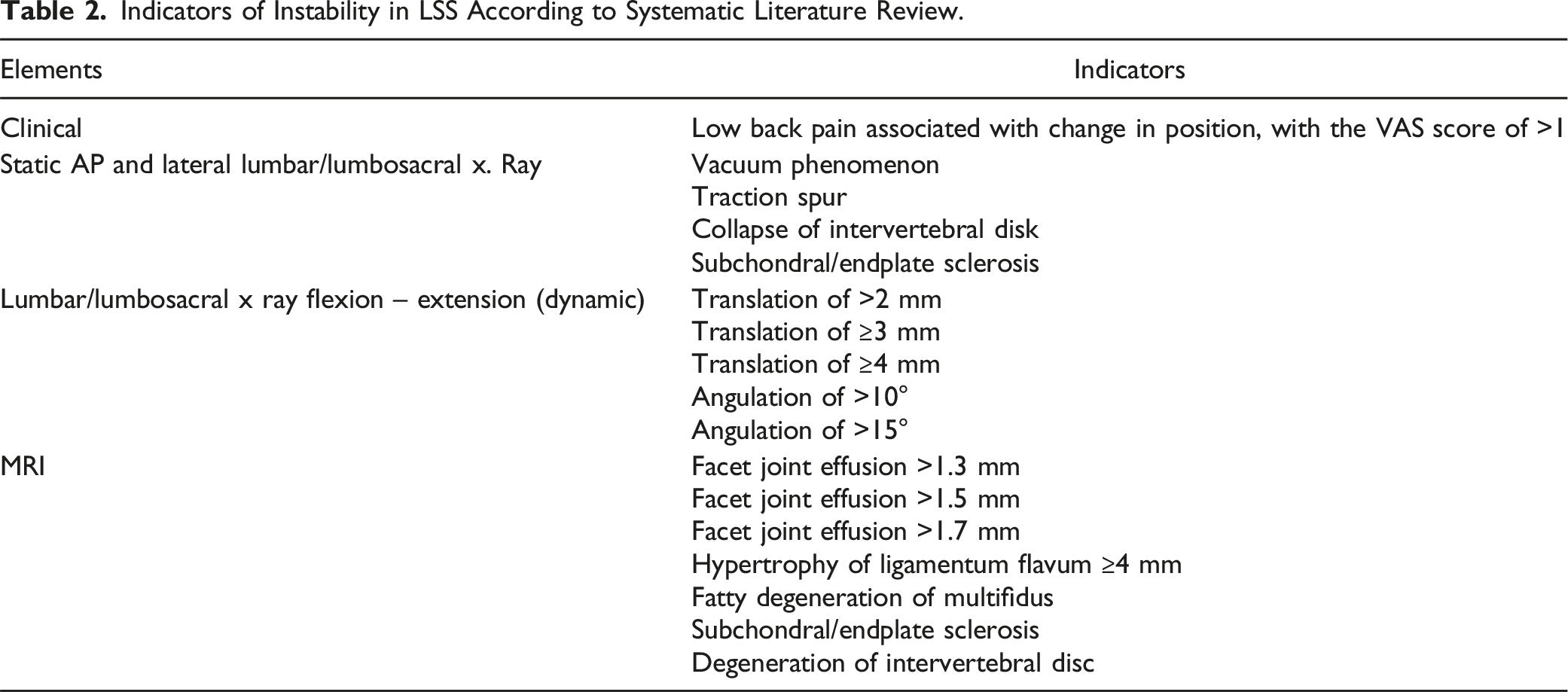
Indicators of Instability in LSS According to Systematic Literature Review.
Expert Opinion and Modified Delphi Technique
Analysis of First and Second Rounds.
Newly Developed Scoring System.
Validity and Reliability
The third stage of the research was carried out at our institutional hospital, with 40 patients for validity testing and 20 patients for reliability testing. Most patients were female with the majority of stenosis occurring at the L4-5 level, followed by L5-S1 then L3-4. The average age was 53 years with an age range of 52 – 70 years. History taking and physical examination were carried out on the patient, as well as radiological data. The radiological examination in the validity test was carried out by one Orthopaedic surgeon while the reliability test was carried out by one Orthopaedic surgeon and one Radiologist. Examples of patient radiological examination results were shown in Figure 3. Radiological examination results.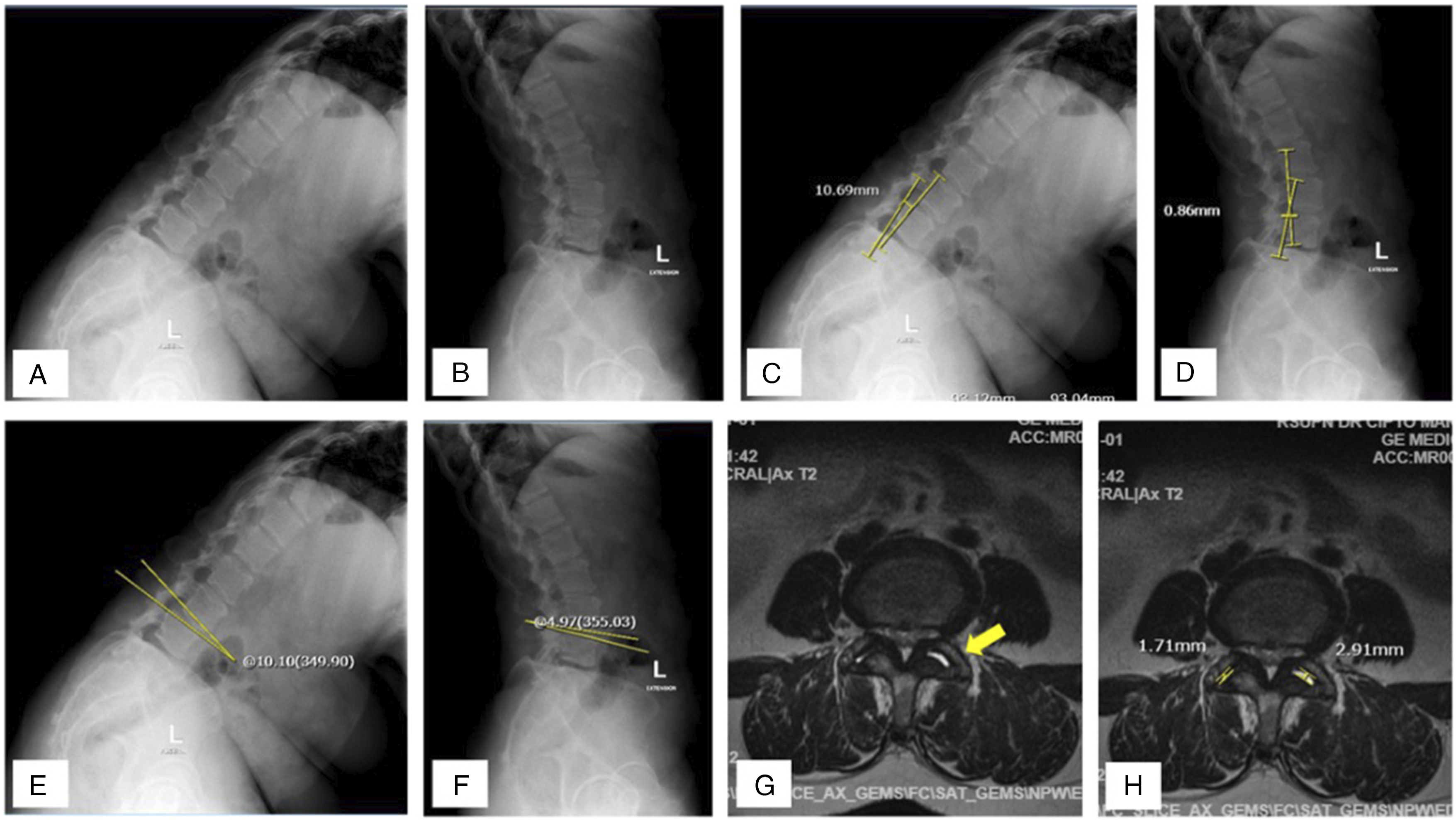
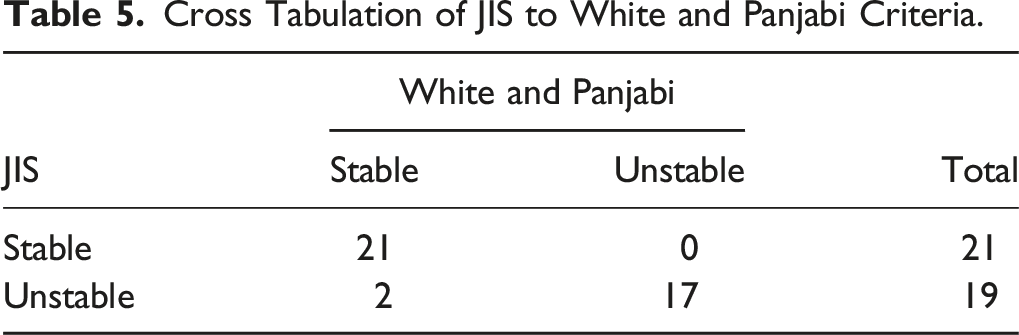
Cross Tabulation of JIS to White and Panjabi Criteria.
Discussion
A motion segment is defined as the smallest segment of the spine having biomechanical characteristics similar to that of the entire spine. Each motion segment, or functional unit of the spine, consists of two adjacent vertebral bodies, intervening intervertebral disc, and the interconnecting ligaments. A spinal motion segment can undergo two kinds of motion, namely translatory and rotatory motions. Segmental instability occurs when a force produces displacement of part of a motion segment exceeding that found in a normal spine. The most widely accepted thresholds for diagnosing instability have been put forward by Panjabi and White 17 as 4 mm of sagittal plane translation anteriorly or 2 mm sagittal plane translation posteriorly for translational instability and for rotational instability as >15° at L1-L4, >20° at L4-L5 and >25° at L5-S1. More than 10° angulation in the sagittal plane has also been widely accepted.25,26 Dynamic radiograph, defined as flexion and extension lateral views, is taken with patient in upright position and a dorsal support placed at the level of the sacrum. Patient is asked to flex or extend the spine actively as much as possible without flexing the hips. The X-ray beam is centered at the iliac crest and radiographs were taken with a tube-film distance of 1.5 m. Measurement of instability was done using the method of Dupuis et al, 27 which is the most commonly used one. Sagittal translatory instability is diagnosed when the translation is 4 mm or more. The criterion for diagnosing sagittal angular instability is when the sagittal angulation is more than 10°.
The presence of instability in patients with degenerative LSS is an important thing to determine because it will help in determining patient management, especially surgical treatment. The surgical treatment of patients with stenosis is decompression. The literature stated that in patients with LSS with instability, fusion in addition to decompression will provide better clinical outcomes. 28 Leschke et al 12 previously conducted a systematic literature review on five RCT studies to look for a definition of spinal instability requiring fusion, they found that there were many indicators of spinal instability but there was no clear consensus on their definition. These indicators were segmental translation and angulation on dynamic flexion and extension x ray; facet joint effusion on MRI; changes in spinal alignment; and lower back or lower back pain related to positioning. They stated that there are still many confounding factors in the accuracy of measuring these indicators. Hasegawa et al 29 conducting research on the probability of spinal instability. They found that if the lumbar spine had degenerative spondylolisthesis, grade III and IV disc degeneration on MRI, facet joint effusion, without subchondral sclerosis, the probability of spinal instability was 91.6%. If there is no degenerative spondylolisthesis, grade V disc degeneration on MRI, without facet joint effusion, and with subchondral sclerosis, the probability of spinal instability is only 4.2%. 29
Patients with degenerative spondylolisthesis have significantly larger facet joint effusions, with the size of the effusion being directly proportional to the size of the anterolisthesis. Vertebral translation or listhesis may not be detected on x-ray or MRI examination, especially in the supine position. 7 However, the finding of a large facet joint effusion (>1.5 mm) has a high predictive value for degenerative spondylolisthesis, which indicates spinal instability. Facet joint effusion was defined as a curvilinear hyperintense signal within the facet joint with the same appearance as cerebrospinal fluid on T2W MRI. Measurement of the size of the facet joint effusion was done by drawing a line perpendicular to the joint line, and the size of the effusion is the largest line size obtained from the measurement. 30
The clinical component of JIS was low back pain associated with changes in position (appearing or improving with extension and disappearing or improving with flexion). Mentioned by Panjabi 17 that low back pain is a clinical sign of instability in the spine. Derman et al 4 mentioned that in their practice, fusion is not performed in patients who have stenosis secondary to spondylosis unless they exhibit a significant component of low back pain. Clinical spinal instability assumes a relationship between abnormal intervertebral motion and low back pain, and with decrease in the intervertebral motion in patient with low back pain, the pain will reduce. According to study by Panjabi, 17 this is the basis of low back pain treatment involving surgical fusion. Furthermore, Fritz et al 31 found that the presence of low back pain related to a high likelihood of lumbar instability. Herkowitz et al 32 also found that in patients with stenosis and spondylolisthesis, fusion provided better improvement in the back pain. These retrospective studies supported the involvement of low back pain as the component of consideration for fusion. Further prospective studies using this newly developed scoring system are awaited.
The MRI component of JIS is the presence and magnitude of facet joint effusion. Literature review and meta-analysis study by Aggarwal et al 33 found that facet joint effusion is an indicator of spinal instability, and in patients with facet joint effusion >1 mm, the risk of spinal instability increases to 8 times. The presence of facet joint effusion has a positive predictive value for instability. This was also conveyed by Singh et al. 34 Singh et al 34 mentioned that facet joint effusion was a reliable sign of spinal instability.
From the analysis, the correlation coefficient for JIS is .795. According to Munro et al, 18 The correlation coefficient value is included in the high correlation coefficient. From the analysis, it was found that the Cohen kappa value for agreement between the JIS results and the radiological criteria by White and Panjabi was .899. In accordance with Landis’ criteria, the agreement value is near-perfect. This shows that JIS had a close correlation with the White and Panjabi radiological criteria as a standard reference, and showed that JIS was a valid tool for detecting instability in LSS. Reliability was measured by one Orthopaedic surgeon and one Radiologist, and according to Landis’ criteria, the agreement value was near-perfect. This showed that the JIS had very good inter-rater reliability. The results of the reliability test showed that JIS total score had an almost perfect level of agreement, which showed that the results of examinations by Orthopaedic surgeon and Radiologist were comparable.
The sensitivity of JIS in detecting instability was 91% with a specificity of 100%. The positive predictive value of JIS in detecting instability was 100% with a negative predictive value of 89%. This showed that JIS was a specific assessment tool with a high positive predictive value in detecting instability in LSS, in other words, JIS was able to correctly detect instability. JIS was quite sensitive with a fairly high negative predictive value in detecting instability.
The validity examination in this study compared the JIS with White and Panjabi’ instability criteria. The White and Panjabi criteria are radiological criteria that are well known and used as a reference for Orthopaedic spine surgeon. In the White and Panjabi radiological criteria component, there is a translation of 4.5 mm in static and dynamic plain radiographs, which indicates instability. In Indonesia, especially in the center where this research was conducted, traditionally a translation of 4.5 mm in dynamic plain radiograph is the limit for determining the presence of instability in the spine. For these reasons, the White and Panjabi criteria were considered appropriate standards as a reference in assessing validity.
The high reliability value showed that the JIS was a reliable measure of spinal instability in degenerative LSS. The results of examinations from Orthopaedic surgeon and Radiologist had a strong level of agreement, this had important benefits in cases of degenerative LSS, because the Radiologist is the doctor who may be the first to read the patient’s condition and the Orthopaedic surgeon is the determining doctor for patient management.
With good validity and reliability test results, this research has clinical and research implications. In terms of clinical implications, the JIS is expected to help spine surgeon in considering the direction of patient management and the type of surgery. It is recommended that JIS can be a tool and guide in determining instability and the need for spinal fusion in degenerative LSS, however, it is not as an absolute decision tool in decision making, because the absolute decision in determining the patient’s surgical treatment will also depend on the clinical judgment of the surgeon. JIS is used as a supporting tool in making decisions about the type of surgery in patients with degenerative LSS. This is especially true in classifying patient stability against the total JIS value in a patient. In terms of research implications, further studies can be performed particularly to see the functional and radiological outcomes of patients with degenerative LSS treated with the guidance of JIS.
Conclusion
It has been previously mentioned that the classification of the total JIS value is divided into stable, potentially unstable, and unstable spine. In stable spines, research suggests that no fusion is necessary, therefore the decompression performed is aimed not to cause post-operative instability. For an unstable spine, fusion is recommended in addition to decompression because the spine clearly shows signs of instability. If the total JIS value is classified as potentially unstable, the decision to perform fusion or not will depend on the clinical assessment of the surgeon. It is recommended that JIS can be a tool and guide in determining instability and the need for spinal fusion in degenerative LSS. Meanwhile this newly developed scoring system is a valid and reliable scoring system to define spinal instability and the need of fusion in degenerative lumbar spinal stenosis, retrospective and prospective studies are awaited to further validate its use.
Footnotes
Acknowledgments
Authors would like to say gratitude for the experts who participated in this study, they are Ifran Saleh, Dohar AL Tobing, Rahyussalim, Luthfi Gatam, Didik Librianto, Fachrisal, Zairin Noor, Agus Hadian Rahim, R Andhi Prijosedjati, and Rendra Leonas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.